
Abstract
Background:
Compassion is seen as a core professional value in nursing and as essential in the effort of relieving suffering and promoting well-being in palliative care patients. Despite the advances in modern healthcare systems, there is a growing clinical and scientific concern that the value of compassion in palliative care is being less emphasised.
Objective:
This study aimed to explore nurses’ experiences of compassion when caring for palliative patients in home nursing care.
Design and participants:
A secondary qualitative analysis inspired by hermeneutic circling was performed on narrative interviews with 10 registered nurses recruited from municipal home nursing care facilities in Mid-Norway.
Ethical considerations:
The Norwegian Social Science Data Services granted permission for the study (No. 34299) and the re-use of the data.
Findings:
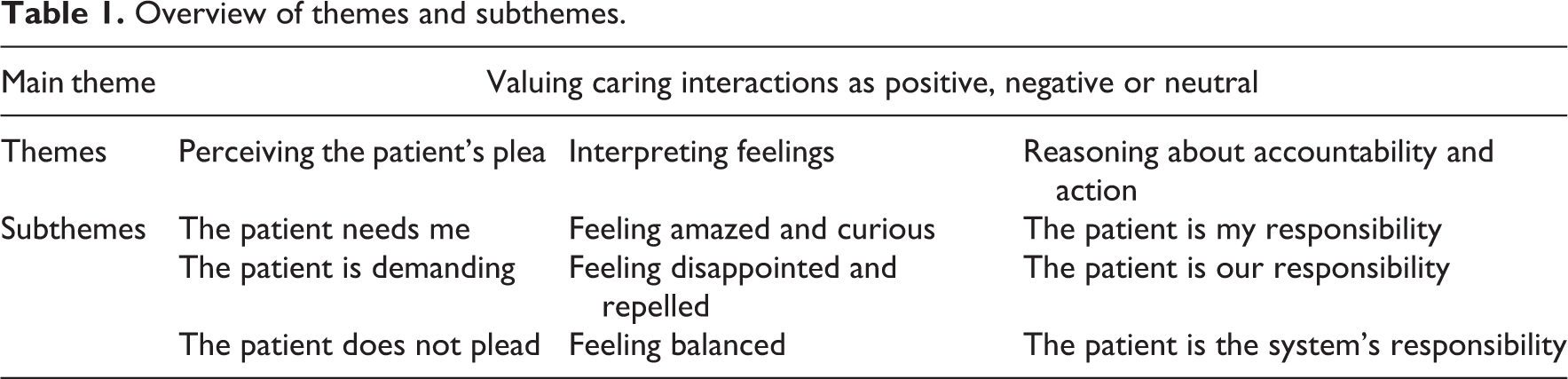
The compassionate experience was illuminated by one overarching theme: valuing caring interactions as positive, negative or neutral, which entailed three themes: (1) perceiving the patient’s plea, (2) interpreting feelings and (3) reasoning about accountability and action, with subsequent subthemes.
Discussion:
In contrast to most studies on compassion, our results highlight that a lack of compassion entails experiences of both negative and neutral content.
Conclusion:
The phenomenon of neutral caring interactions and lack of compassion demands further explorations from both a patient – and a nurse perspective.
Keywords
Introduction
Compassion is seen as a core professional value in nursing 1 and has long been a hallmark in the effort of relieving suffering and promoting well-being in palliative care patients. 2 Caring for palliative patients is perceived as both professionally and personally rewarding. 3 Palliative nursing care frequently necessitates being simultaneously exposed to ethical issues, psychological challenges and emotional distress when encountering patients facing the end of life. 4,5 Given that the quality of care and the emotional well-being of nurses have been proven to be interdependent, 6 knowledge about nurses’ experiences and caring abilities, especially regarding providing compassionate care, has become a matter of urgency. 6,7
While the nurses’ abilities to compassionately care may be implicit, stories from patients often disclaim that belief. Patients have reported being neglected, mistreated and not cared for in a compassionate way, both in hospital settings 8 –11 and community care settings. 12,13 Poor communication and condescending behaviour from health professionals violate patients’ dignity and may increase their burden and vulnerability when relief should be expected. 14,15 There is a growing clinical and scientific concern that compassion as a value in palliative care is being less emphasised. 7,16 –18
Background
As much as it may be self-evident, the concept of compassion remains largely theoretical and anecdotal, 19 and its usefulness is subjected to ongoing debates. 20 Several authors have called for a more profound exploration of the concept 20,21 that also incorporates the empirical understanding of the parties involved. 19 While, the research focus on compassion in healthcare has centred upon nurses’ skills, behaviours and attitudes, 22,23 the actual experience of compassion and what might foster it seem to be missing. Although nurses are urged to be friendly, courteous, interested, concerned, nurturing, ministering, diplomatic and authentic, 24,25 guiding frameworks that integrate compassion in practical nursing care are mostly lacking. 26 Dewar 27 described compassion as the way in which one relates to human beings, as defined by the people who give and receive it. Others have described compassion as characterised by two main components: the affective feeling of caring for one who is suffering and the motivation to reveal that suffering. 19,28 Compassion has also been described as a modality that is intentional and targeted but coincidental because it involves action and choice. 18,19 Present investigation lends on the review by Kanov et al. 29 that incorporate the aforementioned elements and regards compassion as a dynamic process entailing three facets that could be operationalised in practice: ‘noticing’, ‘feeling’ and ‘responding’. Since compassion seems to require both emotion and action on the part of the respondent, caring behaviours may be viewed as reflections of compassion – compassionate behaviours. 18,19
In Løgstrup’s philosophy, 30 compassion is seen as something that is ‘already there’, a characteristic that is present prior to the ethical demand. In his opinion, one cannot encounter others without being confronted with the radical demand to concern oneself with their lives; being responsible for one another is seen as a feature of human existence.
Accordingly, by reviewing the literature on compassionate care, interactional, emotional and ethical aspects were derived as gateways for our exploration. The aim of this research was to explore and interpret nurses’ experiences of compassion when caring for palliative patients in home nursing care. To enter these experiences and to possibly trace compassion in nurses’ ‘noticing, feeling and responding,’ we utilised narratives about patient meetings that had affected nurses emotionally. This study constitutes a secondary analysis of narratives that were primary collected for the purpose of illuminating and interpreting the meaning of nurses’ lived experience when meeting severely ill and palliative patients in home nursing care.
Method
Design
This study was designed as a secondary qualitative analysis of data that had been previously collected and investigated. 4 It is classified as a supplementary analysis that involves a more in-depth investigation of an emergent issue or aspect of the data that was not fully addressed in the previous study. 31 According to Gadamer, 32 understanding cannot be reduced to a method in a narrow sense. As the world is always met with prejudice and preconceived expectations of it based on prior experience, understanding takes place when a fusion of horizons from the past and present ensues. 32 The analysis of the interview texts was performed by four cyclic steps, described by Flemming et al. 33 that are in line with the hermeneutic circling.
Participants and data collection
A total of 10 registered nurses (RNs) were recruited from four community healthcare districts in a municipality in Mid-Norway. Inclusion criteria were as follows: workplace in patients’ homes and experience with caring for seriously ill and palliative patients. Six women and four men aged 29–63 years consented to participate. Their work experience ranged from 4 to 36 years. Half of the nurses were specialist nurses within geriatric, cancer or psychiatric nursing, whereas the other half were RNs with bachelor degrees.
The first author (S.A.D.) conducted the interviews with each RN in a preferred place chosen by the participants. The interviews lasted about 46–100 minutes.
Narrative interviews 34 were carried out, and the researcher asked the participants to narrate their lived experience of meetings with palliative patients who had emotionally moved them. The questions asked were: ‘Can you please tell me about a patient meeting in which you were positively touched?’ and the opposite: ‘Can you please tell me about a meeting that awoke negative feelings?’ To clarify and to encourage further reflections, subsequent questions were asked, such as ‘How did you feel?’ ‘What happened?’ and ‘Could you please tell me more?’. The first author transcribed the audiotaped interviews verbatim.
Ethical consideration
The informants received oral and written information about the study and gave their written consent to participate. The Norwegian Social Science Data Services (NSD) granted permission for the study (No. 34299). The data had no identifying information at the point of the secondary analysis, and the NSD approved the re-use of the data (spring 2017).
Analysis
Gadamer 32 argued that prejudice must be provoked to be understandable; 33 therefore, negativity is productive because one can accumulate more comprehensive knowledge. 34 We utilised this approach by questioning our initial understanding from the primary study and returning to a new and critical dialogue with the interview texts. The analysis was inspired by a systematic development of understanding explained in four phases by Flemming et al. 33 First, all interview texts were examined to find expressions that reflected the fundamental meaning of the text as a whole. At this stage, the first author formulated a fundamental meaning of the nurses’ experiences of their caring interactions. This content was shared and discussed by all authors and formed our starting point of understanding. The fundamental meaning of the nurses’ experiences could be seen along three dimensions – positive caring interactions, negative caring interactions and neutral caring interactions. The positive and negative dimensions were expected dimensions based on the questions in the interview guide, but the neutral dimension was added by the participants.
In the second phase, the texts were scrutinised, unit by unit, to identify the meaning of the subject matter (i.e. caring interactions). The identified meaning units were reflected upon and interpreted to represent themes, that in turn, were challenged by the initial fundamental meaning that we had found in the first phase. The first author presented meaning units and pertaining themes for all authors to contemplate.
Third, in light of the initial overall understanding, the themes and subthemes were seen in a comprehensive understanding that covered commonalities and differences found in the interviews as a whole. At this stage of the analysis, the hermeneutical circle was experienced when the meaning of the parts widened and expanded our understanding of the whole text. 32
The fourth phase involved identification of passages that could represent a shared understanding between the participants and the researchers. When the authors agreed on a reasonable understanding, the circle was closed, although it cannot be absolute in the hermeneutic. 35
Results
The results are presented in one main theme: valuing caring interactions as positive, negative or neutral, which entailed three themes: (1) perceiving the patient’s plea, (2) interpreting feelings and (3) reasoning about accountability and action, with subsequent subthemes (Table 1). The main theme was seen as a horizontal pattern transcending the three themes and the subthemes.
Overview of themes and subthemes.
Valuing caring interactions as positive, negative or neutral
The nurses’ narratives revealed various experiences related to compassion when encountering and caring for palliative patients living at home. The fundamental meaning of these experiences reflected their categorisation of caring interactions as positive, negative or neutral. The positive interactions are understood as giving rise to compassionate feelings, while the negative interactions create feelings of dislike towards the patient. In neutral interactions, the nurses seem indifferent towards the patient. One of the nurses compared these interactions with meetings of different people in everyday life: As otherwise, in life, you meet new people, and some…they just pass by…While others, they make a stronger impression that affects you. It happens to me all the time. Yet, we are only humans, and even as professionals we have to admit that we are humans working with humans and such relationships are deemed to involve both positive and negative experiences. It just comes along with the care we provide…
Perceiving the patient’s plea
The first theme reflects what the nurses recognise as making a plea in their meetings and caring interactions with their patients. Most of the patients appearing in the nurses’ stories are old, have advanced cancer, have distressed symptoms, both physically and mentally, and demonstrate obvious caring needs. Although, the nurses observe and affirm the patients’ situations on a rational level, they explain how they comprehend and attend to each patient differently.
The patient needs me
Feelings of sympathy or compassion might arise easily and immediately when the nurses perceive patients as weak or distressed. Sometimes, these signals are urgently visible conveyed by the patient’s physical appearance. Other times, direct observations are coupled with contextual information about the patients, for example, their living circumstances, social connections, case history or prognosis of disease. One of the nurses talked about an older female patient who was in her palliative stage of cancer: It did something to me…to see how lonely and lost she was, ate almost nothing. She was so shy, and did so little for herself…it just felt good to be there for her. It is easier to feel good about patients the less they request for themselves, you know. Patients who do not ask for more than your presence…It is easier to give, then…
The patient is demanding
While, the nurses perceived that some patients presented an unprejudiced wish for care, other patients are understood to be presumptuous and demanding. One of the nurses explained, Some just have this mentality: ‘I am entitled to it’ – or ‘Society owes me this’. I really dislike this attitude, and I’m afraid we are heading in that direction as we are increasingly dealing with customers.
The patient does not plead
Coincidentally, the nurses find that some patients have neither demands nor silent pleas. In these cases, the nurses classify their caring interaction as neutral. One of the nurses said, I think some of the patients have just stopped expecting anything. In a way, they have got used to nurses dropping by…having no time to sit down…and some of the patients just want the ‘mission completed’, neither more nor less.
Interpreting feelings
The nurses also alluded to the awakening of different emotions. Incidents when feelings are activated seem to be provoked by a disturbance of their inner balance, featured by elements of surprise in either positive or negative directions.
Feeling amazed and curious
In positive interactions, encountering unexpected or unfamiliar expressions seem to arouse the nurses’ curiosity. The nurse might feel impressed or touched by the patient’s courage: It caught me off guard…I had never witnessed that before…this man’s hope for and strong will to die in his own home. No signs of fear – he was just so determined. His housing conditions were really bad…dirt and trash all over, but the man was so reflective and shared so many interesting details about his life at sea…He wasn’t among the popular patients, but to me, he was very interesting.
Typically, in positive interactions, the nurses perceived that the patients were full of confidence: To feel the huge trust that is given to me is really touching…almost something solemn, and it inspires respect.
Feeling disappointed and repelled
Other times, encountering unexpected reactions from the patient, like mistrust or humiliating behaviour, causes negative feelings. Therefore, the nurses were more likely to appraise such interactions as negative. Dislike often occurs when the nurses encounter patients with endless demands or those who openly express their dissatisfaction: No matter how hard I tried, it was never enough for him. I felt annoyed and helpless because I always fell short. I misjudged upon her situation…I thought she wanted to open up and talk to me, but that was not her intention at all. It made me feel disappointed…and defective. She has her favourites…and I haven’t been professional enough to handle it…I have been hurt by it, and felt sad…She may ask for certain nurses, ‘Fetch (the name of a nurse) for me, she always cheers me up’. It becomes personal, you know. She has large caring needs and is mentally unstable…but I find her to be simply manipulative.
Feeling balanced
Several nurses perceive that most interactions progress without disturbance or surprise. One of the nurses said, I feel that most of the interactions are somewhat in the middle…the patients get what they need or what has been decided…and, sometimes, you deliberately avoid getting involved because there is not enough time to deal with any struggles. As years go by, I find it much easier to observe the right things, and I have to work less with myself on interpersonal relations…In a way I feel that I am finished with this relational-part…I have it made, so to say (laughs).
Reasoning about accountability and action
The narratives revealed that the process of making meaning in each caring interaction affects the nurses’ accountability and their willingness to engage with the patients. In addition, their stories exposed that the process of grading caring interactions is not solely based on the perception of each isolated interaction, but it also depends on a comprehensive understanding of all care interactions in which they are involved. In the end, their interpretations may become the result of comparisons between completely different interactions: All his nagging and demands, he is the polar opposite to the man next door who just lies there and never asks for anything…His (the first mentioned patient) problems are real, I am well- aware of that…but when I compare him to the other man…It doesn’t feel right. In that perspective, it is difficult to feel sympathy… I wanted to be forthcoming, but I couldn’t…none of us are, all the time…Some days are very chaotic, and you just concentrate on keeping up with the tasks on your list. In stressful periods, I know that my patience and empathy are affected.
The patient is my responsibility
In positive caring interactions, the nurses make great efforts in living up to the patients’ expectations and trust. Being flexible, adapting and doing ‘the little extra’ are seen as obvious and as a pleasant performance in such cases. The actions taken seem to originate from a spontaneous and free will, and a significant commitment to the patient’s well-being. One of the nurses said, I felt like doing something extra for him…and when giving the little extra – you actually give the patient your presence…something that should be included as a part of the whole package (the care)…and not be seen as something extra.
The patient is our responsibility
When narrating about negative caring interactions, the nurses admitted that their caring activities are typically more standardised, brief and less flexible than the positive interactions. They are more inclined to regard their responsibility as a shared one, shared with the other nurses who are also visiting the patient. One of the nurses talked about a patient she strived with: His mood was so volatile…One day he could be pleasant and nice, but the other day he was angry and called me names…You never knew. Maybe he had his reasons for being angry and I heard that my colleague experienced the same. I just delivered his medicines and took the blood samples as ordered. I didn’t have to go there every day…some of the days he was on my colleague’s list.
The patient is the system’s responsibility
The neutral caring interactions are understood as effective and the least disturbing of the interactions. The nurses are occupied with accomplishing care activities that are expected and instructed, both from their patients and from their employer. Attentiveness to situational and unpredicted requirements are subjected to their time at disposal. One of the nurses explained, We are not always that touched…and it doesn’t have to be a bad thing, I hope (laughs). It has to do with the setting and the timing. In order to manage a long list of patients you can’t ask everybody how they really are…We have to take care of the tasks that are expected from us. No matter the feedback from the patient, praise or criticism, it does something to you…it activates you and makes a difference on the care you provide…we always strive to respond and please. In the neutral interactions, we may be less focused or observant, but if anything special occurred, I hope we would notice… In positive or negative interactions, the focus is so strong…in the neutral interactions…maybe we do not try that hard?
Discussion
The results of this study show that the nurses experienced both the presence and absence of compassion when caring for palliative patients living at home. Based on how they interpreted the patients’ expressions and the way they became emotionally affected, the nurses understood that their caring interactions comprised compassion, dislike and indifference.
Experiences of compassion involved awareness (of the patient’s plea), attention (to feelings) and engagement (ascribing meaning and accountability) that agree with the literature. 18,19,28,36 In line with other studies, 37 –39 our results also identified enablers and barriers for compassion. Positive relational aspects or perceptions of dependence and trust within patients could enable compassion. Barriers could be related to perceptions of unduly demanding patients, shortage of time or the nurses’ own feelings of well-being in the moment. Possible barriers or enablers of compassion are recently suggested to be associated with nurses’ well-being and their levels of self-compassion. 40 Interventions to promote individuals’ psychological flexibility have also been shown to enhance the perceptual, cognitive, affective and behavioural aspects of compassion. 41 Our data did not allow pursuing aspects of self-compassion, but further research is strongly recommended.
However, in contrast to most studies on compassion, our results highlight that lack of compassion entails experiences of both negative and neutral content. In addition, the fact that the nurses in this study viewed most caring interactions as neutral is quite surprising and calls for further explorations.
When encountering the patient, the nurses are exposed to a wealth of expressions that may actualise not only the patient’s vulnerability but also their own. According to Løgstrup, 30 vulnerability is a basic condition of one’s existence, as humans are reciprocally dependent on and entrusted to the care of one other. In that respect, vulnerability qualifies the nurse to enter the patient’s suffering and actually recognise his/hers plea. Vulnerability makes the nurse imperfect as she tries to protect herself from being refused or falling short of the patient’s expectations. Our findings may indicate that the nurses’ vulnerability may activate a self-defence that counteracts compassion. Somehow, the nurses seemed to be more touched and motivated to be involved if the patients’ vulnerability exceeded their own. Perhaps, patients that had the power to demand or demonstrate mistrust appeared less vulnerable than patients who posed no claims.
Struggling with compassion was often related to interactions with patients perceived as demanding and argumentative. In such interactions, compassion was not only reported as lacking, but it also turned into direct negative feelings of dislike. Singh et al. 37 also reported that patients who were deemed to behave in an unacceptable manner were less likely to receive compassionate care. Placing different values on caring interactions may have the power to divide patients into ‘deserving’ and ‘undeserving’ groups. Indirectly, the present findings may indicate that patients who are perceived as modest, trustful, impressive and noncompliant or those who impose no conditions for care seem to easily awake and deserve the nurses’ compassion, contrary to undeserving patients who are perceived to be self-assertive, suspicious and predictable, or those who pose claims or seem careless. Although the nurses never used words like deserving or undeserving when describing such patient characteristics, their impressions and responses may be associated with this taboo in healthcare. 42
However, in neutral caring interactions, the nurses typically normalised the absence of compassion and explained that time pressure or low expectations from the patients may be the cause. Moreover, neutral caring interactions do not seem to be very problematic to the nurses. We have not succeeded in retrieving any study on the phenomenon of neutral caring interactions from a nurse perspective. However, patients’ perspectives on quality of interactions with health professionals at hospital wards have been rated as positive, negative and neutral. 43,44 Both studies found that the length of interaction was not associated with quality of interaction, suggesting that both positive and negative interactions can be accomplished despite short contact time. In these studies, neutral interactions, which were defined as neither undermining nor enhancing, were either part of adequately carrying out care tasks or involved request, suggestions or information exchange without any features of positive or negative social interactions. In this respect, neutral interactions are not expected to impact the feelings of patients or their perceptions of care quality. This understanding seems to be shared by the homecare nurses in our study. However, although a slight suspicion arose concerning their ability to adequately observe and capture changes or preference for their patients, the nurses did not appear to be concerned about patients wanting or needing them to be more involved. Although the patient perspective is not provided in our study, others 38 have found patients to be very much aware of both the presence and absence of compassion. Patients experience compassion not only as an emotional resonance but also as a willingness to engage and relate to patient suffering from a place of shared humanity. 38 Our findings indicate that the nurses’ willingness to engage varies and seems to be affected by the meaning ascribed to each caring interaction. In both positive and negative interactions, the nurses seem to make efforts to achieve good relationships with their patients, though not always successfully. On the contrary, in neutral interactions, the nurses admitted that they do not try very hard. If such efforts reflect a willingness to engage, neutral caring interactions may ultimately have an effect on patient suffering.
Tveit and Raustøl 20 have recently questioned whether compassion really is a helpful concept to understand the lack of involvement or malpractice in healthcare. Molander et al. 45 launched the idea that a potential compassion crisis may be better understood as ‘poor discretion’ and argued that healthcare today is characterised by structural measures and quality systems that may limit individual and professional discretion. On one hand, the finding of neutral interactions explained as task-oriented care on behalf of the system may call for increased attention on how professional discretion is exercised. On the other hand, the results of this study indicate that experiences of compassion extend the concept of discretion, as experiences of compassion are also expressed as a willingness to engage. Then, if willingness to engage is transitory and situational (as may be reflected in neutral interactions), it is of the utmost importance to pursue deeper explanations. The efforts made to engage in both positive and negative caring interactions may be associated with the ontological foundation of compassion. 30 However, the experiences of neutral interactions may disturb the idea of compassion as something already there. From the nurses’ perspectives, compassion appears to be ‘inactive’ in the neutral interactions. According to Martinsen and Kjerland, 46 care is more than feeling sorry for or having a liking for someone; care also involves practical participation in the patient’s suffering based on professional judgement (to see and express the patient’s plea for help). Inspired by Løgstrup, Martinsen’s philosophy rests on the assumption that human beings are interconnected and dependent on each other and, thus, compassion is seen as ontological. In light of Martinsen, the results of this study might be interpreted as compassion in practice – where recognising the patient’s plea and feeling emotional unbalance are dimensions in ‘professional judgement’, and willingness to engage is fulfilled in ‘practical participation in the patient’s suffering’. Thus, the notion of compassion as ontological is kept, but the findings of this study indicate that compassion is inactive unless under the presence of a will. Therefore, explorations should be made to increase our understanding on how this will is either strengthened or weakened by the way that nurses interpret and value different caring interactions.
Strengths and limitations of the study
The strengths of this research are the rich descriptions, personal reflections and unique experiences shared by the participants. The interview situations were based on trust and careful attention to the flow of the nurses’ stories by avoiding interruptions. Since the same researcher who performed the secondary analysis performed the initial collection of the data, contextual and interactional contexts were understood through the way they were produced. The analysis process is outlined in detail to construct a transparent logic. The findings cannot be generalised, but they can provide new insights and new questions that should be followed up. The influence of contextual factors, for example, work environment, workload or leadership was not researched in this study.
Conclusion
The nurses experienced compassion, indifference and dislike when caring for palliative patients living at home. The compassionate experience seemed to be influenced by variations in awareness, attention and engagement, situated in caring interactions characterised as positive, negative or neutral. In contrast to most studies on compassion, our results highlight that a lack of compassion entails experiences of both negative and neutral content. The phenomenon of neutral caring interactions and a lack of compassion demands further explorations from both a patient – and a nurse perspective.
Footnotes
Acknowledgements
The authors are grateful to the nurses who shared their stories.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.