
Abstract
Background:
Doctors should disclose the diagnosis to patients according to the principle of autonomy. However, not disclosing the diagnosis and prognosis to cancer patients remains common in mainland China.
Objective:
The study explored the experiences and attitudes of patients with cancer, family members, and the medical staff in truth-telling.
Research design:
A quantitative survey with three closed-ended questionnaires was conducted.
Participants:
In all, 137 patients with cancer, 134 family members caring for cancer cases, and 54 medical staff were surveyed. Descriptive statistics were used to summarize all characteristics, and the chi-square test was performed to analyze group differences in attitudes toward cancer disclosure.
Ethical considerations:
This study was approved by the Committee on Ethics of Biomedicine Research, at the Second Military Medical University (HJEC-2018-YF-001). Informed consent was obtained from all participants prior to study commencement.
Findings:
A total of 59.8% of patients were informed about their diagnosis within 1 week, and 19.7% inferred theirs. The medical staff preferred to prioritize family members in informing about patient diagnosis while 77.4% of patients preferred to be told the whole truth at the time of initial diagnosis. More patients than family members and medical staff wanted the patients to be informed about the diagnosis (p < 0.001). A significant difference was found between the patients and family members regarding who should tell the patients.
Discussion:
The willingness of patients in knowing the truth was underestimated by their family members as well as the medical staff. Guessing the truth indirectly may exert negative effects on the patients, and not telling the truth is inappropriate in patients who want to be informed.
Conclusion:
Disclosure of a cancer diagnosis is a complex process involving medical practice, as well as a range of cultural, ethical, and legal factors. The medical staff should first assess each patient’s willingness in truth-telling and inform about disease diagnosis with respect. Emotional support and comfort from family members are encouraged. Anyone in the patient’s care team, especially nurses, could be integrated in the process of truth-telling.
Introduction
The GLOBOCAN 2018 survey 1 by the International Agency for Research on Cancer estimated that one in five men, and one in six women, have cancer during their lifetimes. Worldwide data estimated that there would be 18.1 million new cancer cases, and 9.6 million associated deaths in 2018; of these, almost 24% (4.3 million) and 30% (2.9 million) of cancer cases and deaths, respectively, have occurred in China. 2 Despite advances in the treatment and control of cancer, this disease is still considered by many cultures to inevitably lead to death.
Announcing cancer diagnosis and poor prognoses to patients is one of the most challenging and stressful tasks performed by the medical staff. On one hand, it is worrisome that bad news might take away the hope of patients, make them feel more vulnerable, and shorten survival; on the other hand, not telling the truth could infringe patient’s autonomy. 3 Therefore, the medical staff often face the dilemma of whether or not to tell the truth.
In developed countries, there has been increased interest in patients’ involvement in healthcare, and doctors usually disclose information to cancer patients in a direct manner. 3 Recent studies have shown that telling the truth in an appropriate way could result in better treatment compliance, greater levels of satisfaction, and lower levels of anxiety and mood disturbances in cancer patients. 4 To promote and improve the disclosure of bad news to patients, several guidelines have been issued, such as the SPIKES protocol. 5 However, many questions remain. (1) How much disclosure is enough? (2) Can doctors cause harm by telling too much? Physicians and nurses still struggle to find the best way to tell bad news without causing undue harm to the patients. 3,6
Despite a change in attitudes, perceptions and beliefs about disclosing the truth in some regions, particularly the Middle East, Eastern Europe, and Asia, are less optimal compared with those of developed countries. 7,8 Not telling the truth to patients with poor diagnosis and prognosis in the above regions is still very common. 9 The medical staff are frequently subordinate to the power of the patient’s family with regard to truth-telling, 8 and the family members often decide whether to tell the truth or not. A substantial number of cancer patients have died without knowing their diagnosis. 10 Some of those patients wanted to know the truth but were not told. It seems to contrast the principle of respect of autonomy. Meanwhile, multiple patients do not want to know the truth. In such cases, if the medical staff tell the truth to patients, the patient’s autonomy is not respected either because the information is unwanted. Therefore, it is critical to establish the patient’s needs with regard to the truth, and to establish whether these are fulfilled in the clinical environment.
Recently, experts in mainland China have developed significant interest in this field. In 2017, scholars at Peking University 11 used interviews and surveys to explore the views of patients, family members, the public, and doctors, with regard to truth-telling; the results revealed a discrepancy between the needs of patients and medical professionals. Doctors were less willing to tell the truth than patients and family members. A more recent study 12 also found a gap between the medical staff’s clinical practice and the preferences of cancer patients and their families.
The above studies mainly compared the attitudes between patients and doctors, rather than experiences. The findings have evoked a number of pertinent questions. (1) Does the patient know his or her diagnosis and prognosis? (2) What is the role of family members in telling the truth? (3) How do the doctors tell the truth? To answer these questions, a survey was performed to investigate the experiences and attitudes of cancer patients, as well as the attitudes of family members and the medical staff engaged in the diagnosis and treatment of cancer.
Methods
Participants
Potential participants were approached within the Oncology and Gynecology Departments of two general hospitals in Shanghai and Hainan province between May and July 2019. Patients with tumors were recruited if they met the following criteria: (1) age > 18 years; (2) confirmed diagnosis of malignant tumor; (3) normal mental state, with an ability to read or answer questions; and (4) willingness to participate voluntarily in the survey. “Family members” were defined as the members of a patient’s family who were most involved in patient care. All physicians and nurses caring for cancer patients in both departments were invited to participate in this study. Physicians and patients were not paired.
Instruments
Based on a qualitative study 13 and existing literature, three self-reporting questionnaires were developed, respectively, for patients, family members, and the medical staff. The qualitative study interviewed 22 patients and their family members and 19 doctors about their attitudes and practices associated with the disclosure of cancer-related information. The resulting findings served as the conceptual framework for developing the questionnaires. Then, the questionnaires were evaluated by a panel of 10 experts, including physicians, nurses, hospital administrators, and other cancer professionals. Then, items were revised in accordance with the recommendations made by the panel of experts.
Besides the general information sheet, the questionnaire for patients included two parts: (1) patient’s experiences in truth-telling, four items, and (2) patient’s attitudes in truth-telling, six items, such as “When the patient is told the truth, how much disclosure is appropriate?” (Choices include “tell the whole story,” “tell part of the story,” and “it depends”). The questionnaire for family members contained nine items assessing their attitudes in truth-telling. The questionnaire for the medical staff mainly focused on their preferences and attitudes in truth-telling; it consisted of nine items. For example, “Will you tell the patient his or her diagnosis at the time of initial diagnosis” was used to assess the medical staff’s attitude about disclosure target at the time of initial diagnosis. All items used closed questions.
Procedure
The medical staff completed all their questionnaires. The questionnaires given to the patients and family members were completed by the respondents themselves, or assisted by the investigators. To avoid influencing the views of patients who were unaware of their diagnosis, the word “disease” was used in the patient questionnaire rather than “cancer.”
Data analysis
All data were recorded in EPIDATA3.1 and analyzed with SPSS version 19.0 (IBM Corporation, Chicago, IL, USA). Descriptive statistics were used to summarize the characteristics of the respondents included in the survey sample, and to examine the distribution of responses. The χ2 test was used to determine relationships among variables. Statistical significance was set at p < 0.05.
Results
The final analysis included 137 patients diagnosed with cancer, 134 family members taking care of these cancer patients, and 54 medical professionals. The medical staff included also took care of the participating patients. The demographics of these three groups are given in Table 1.
Demographical data of the medical staff, patients, and the family members of patients.
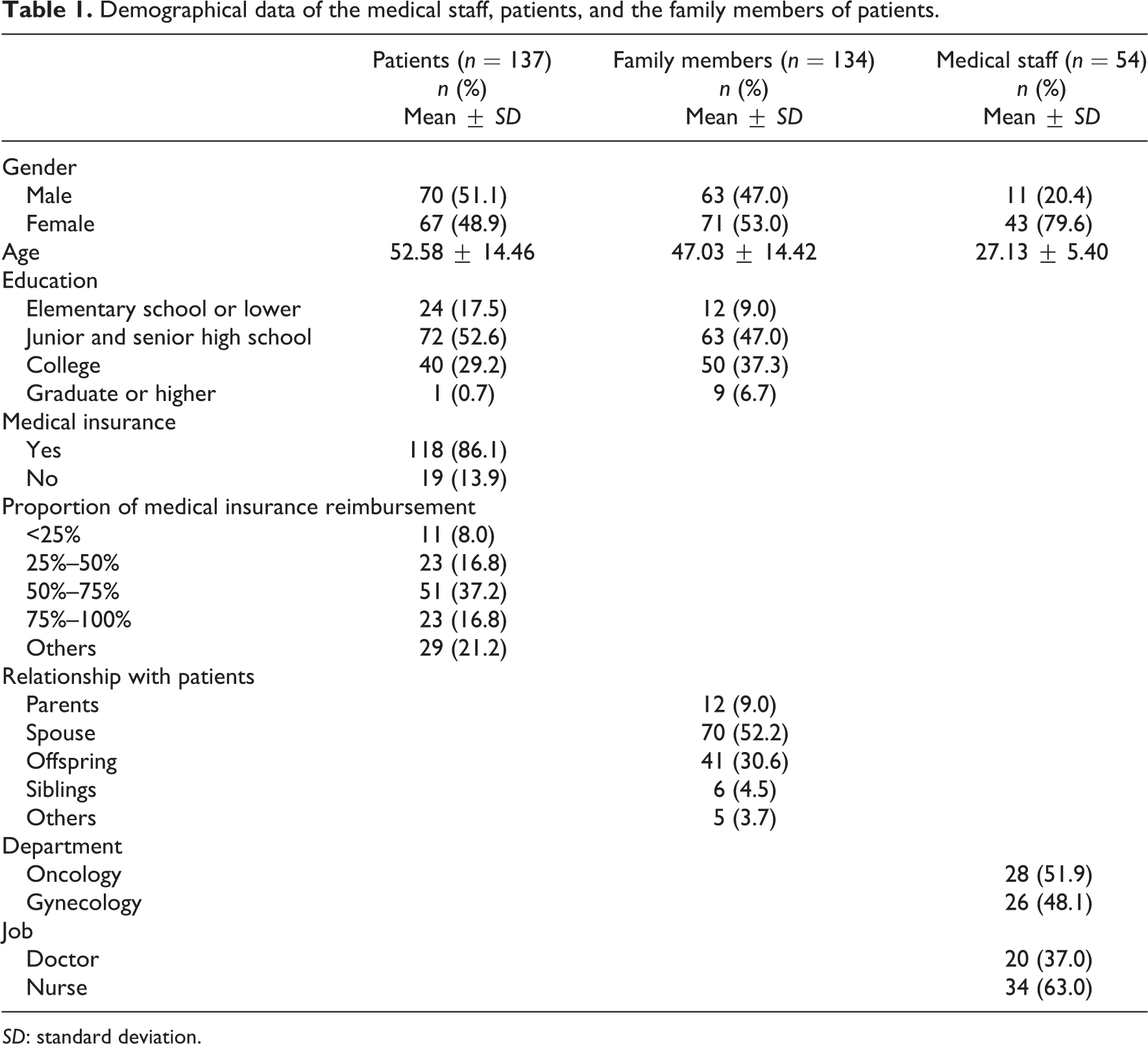
SD: standard deviation.
Experiences of cancer patients with regard to truth-telling
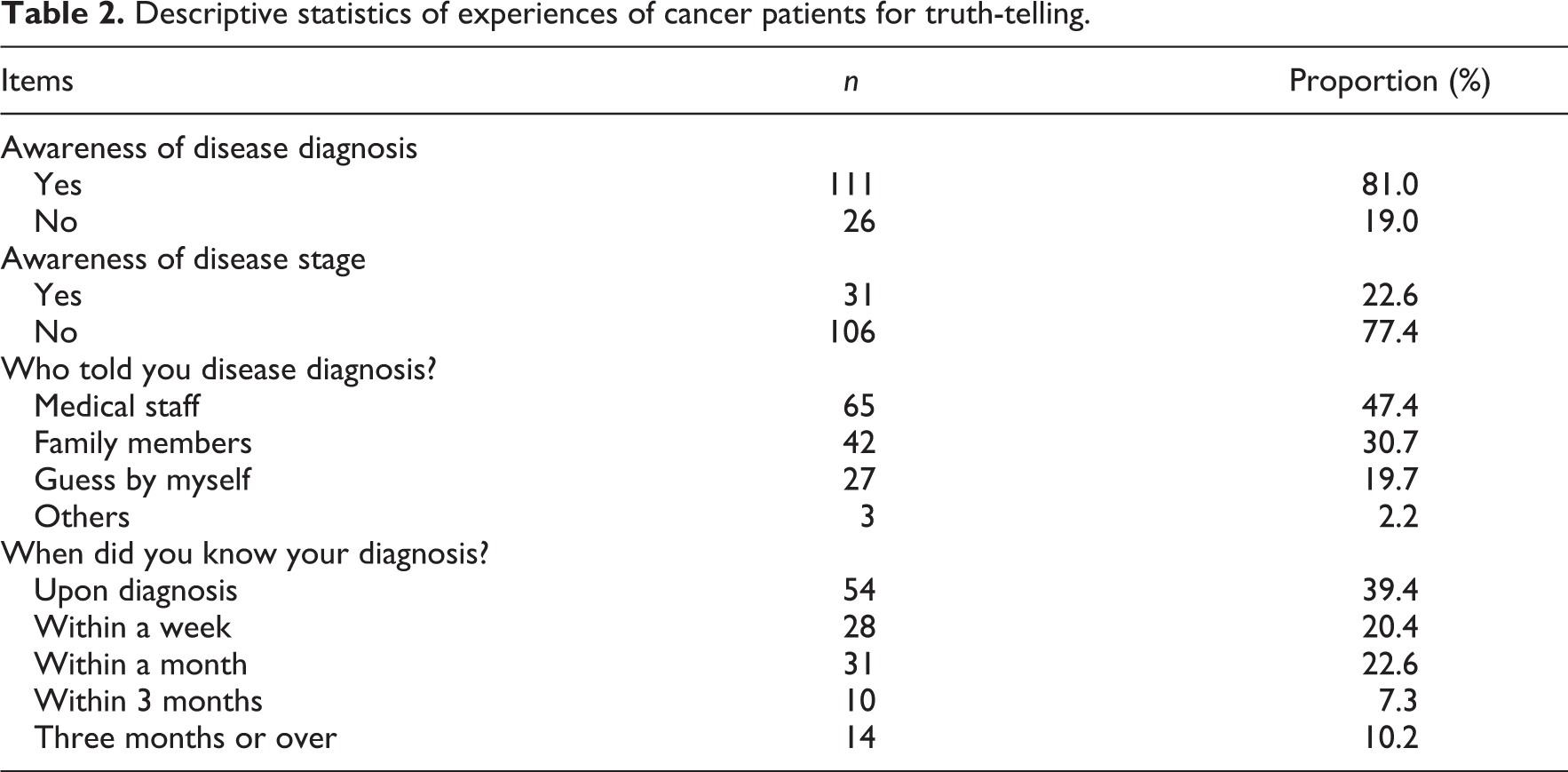
The results showed that 81% of patients reported knowing their diagnoses, with 22.6% aware of their disease stage. Almost half of the patients (47.4%) received information from doctors. Only 39.4% had such information at the time of initial diagnosis (Table 2). The percentage of patients who knew their diagnoses was significantly higher than that deemed by the family members (81.0% vs 56.0%, p < .001).
Descriptive statistics of experiences of cancer patients for truth-telling.
Attitudes of medical staff with regard to truth-telling
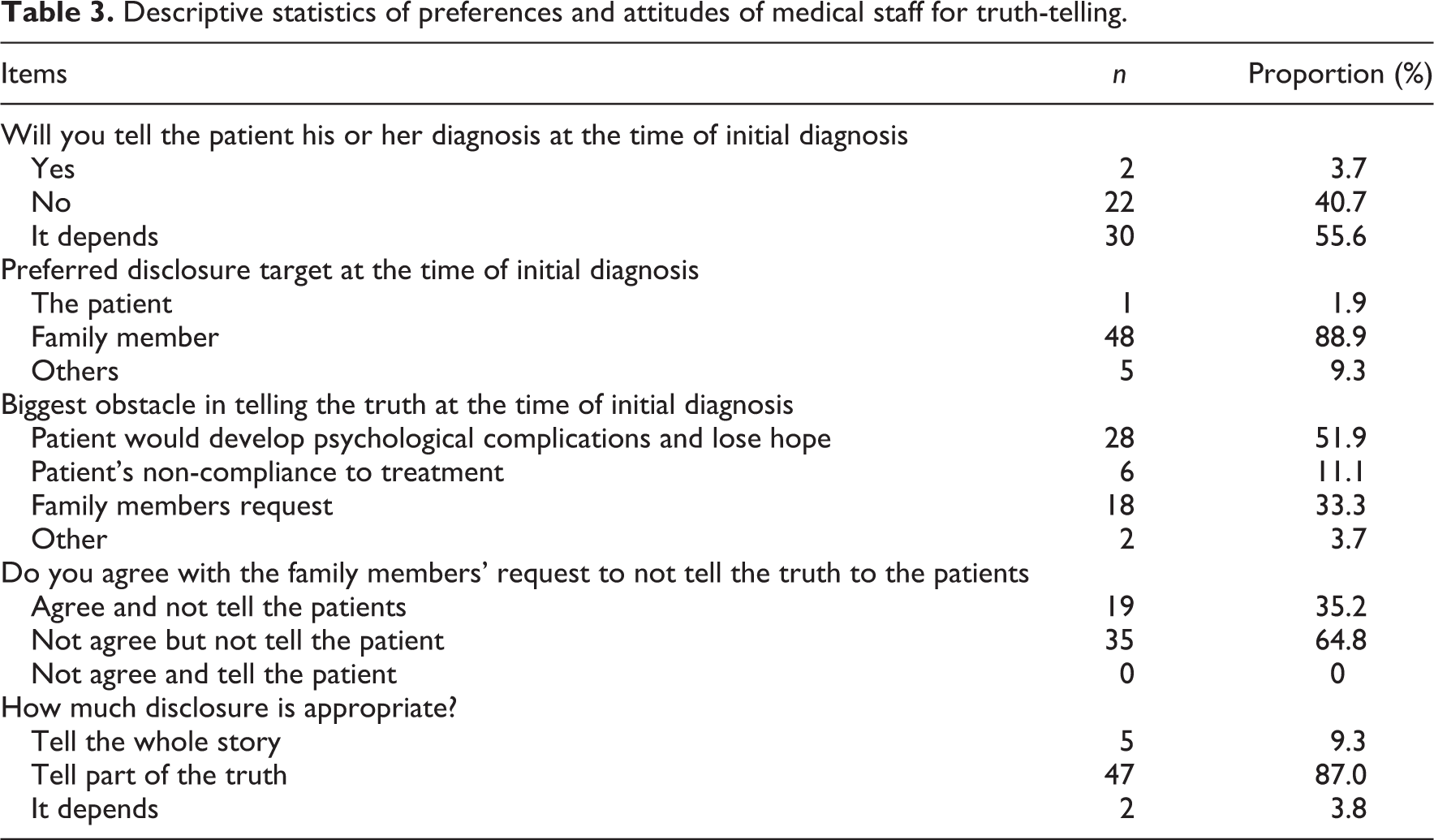
Table 3 listed the attitudes and preferences of the medical staff with regard to truth-telling. A total of 88.9% of the medical staff preferred to tell the diagnosis to patients’ family members at the time of initial diagnosis, and 64.8% did not agree with the family members’ request to not tell the truth and would not tell the truth at the time of initial diagnosis.
Descriptive statistics of preferences and attitudes of medical staff for truth-telling.
Attitudes of family members with regard to truth-telling
A total of 35.1% of the family members did not want the patients to know their diagnoses. Reasons included worrying that the patient would lose hope (62.7%), possible non-compliance of the patients to treatment (17.2%) in case they knew the truth, and others (20.1%). For patients diagnosed with terminal cancer, only 29.1% of the family members would tell the patients.
Differences in attitudes to truth-telling between patients, family members, and medical staff
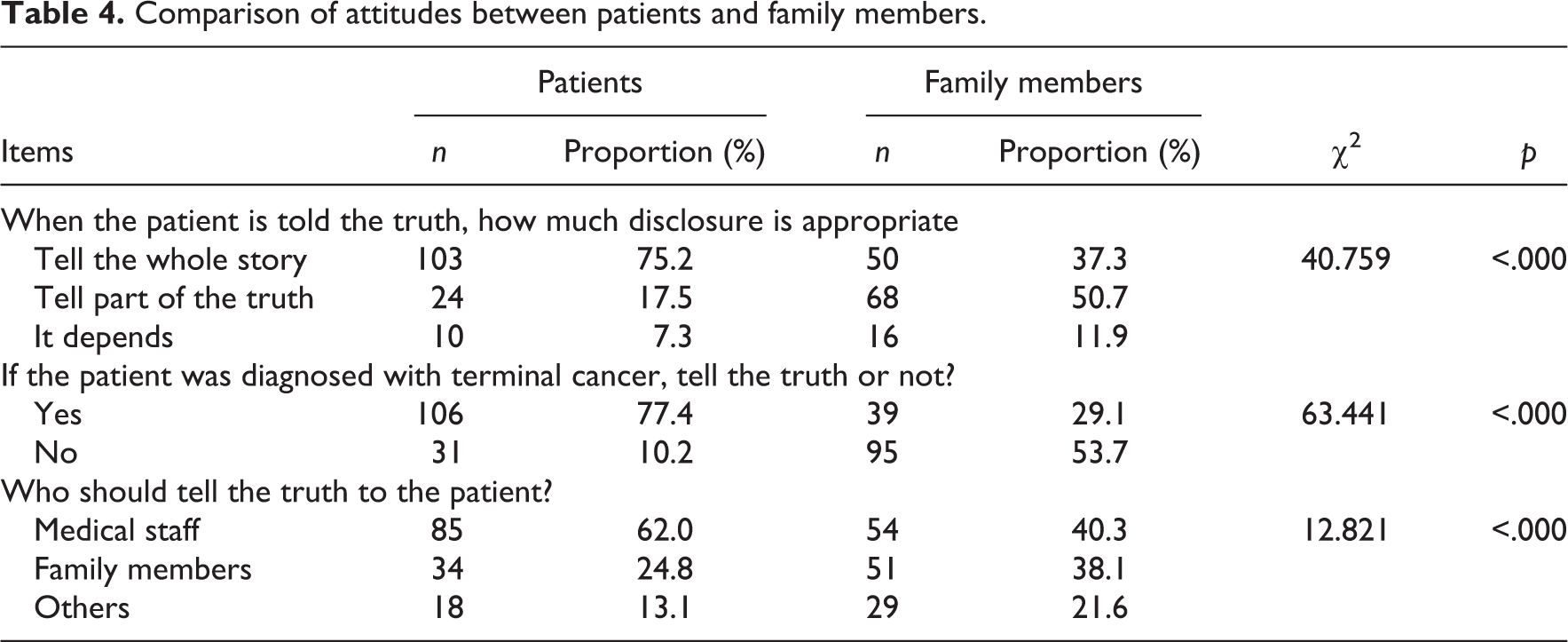
Significantly more patients wanted to know information about the diagnosis, progression, and outcomes of their disease than the family members did (77.4% vs 29.1%, p < 0.001) (Table 4). Furthermore, the proportion of patients who wanted to be told all the truth was much higher than that of the medical staff deeming the patients should be (75.2% vs 9.3%, χ2 = 80.923, p < 0.001).
Comparison of attitudes between patients and family members.
Discussion
This study investigated the preferences, attitudes, and experiences of cancer patients, their family members, and the medical staff engaged in cancer diagnosis and treatment with regard to truth-telling. The differences in the preferences and attitudes of truth-telling in these patients, their families, and medical staff were analyzed. Moreover, the differences between the experiences and preferences and attitudes of patients were assessed.
The current survey showed significant differences in the preferences and attitudes regarding whether to tell the cancer diagnosis and prognosis or not to the patient among cancer patients, family members, and medical professionals, even in the situation of terminal cancer. These results implied that the willingness of patients to know their disease diagnoses was underestimated by their family members as well as the medical staff. These findings concurred with several reports, 11,14,15 showing there were more patients than family members and medical workers who wanted the patients to be informed about the diagnosis of terminal illness. Telling the truth based on each individual patient’s willingness not on doctors’ or family members’ assumptions need to be considered in further clinical practice.
As shown above, nearly half of the patients (40.2%) were informed about their diagnoses 1 week after, and almost one in five (19.7%) of the included patients inferred their diagnoses during the follow-up treatment. Previous research showed that patients could guess their diagnoses by considering their symptoms, along with the information retrieved from the Internet. 9,16,17 During their efforts to figure out the truth, patients reported poor daily well-being, 18 more psychological morbidity and reduced trust in their families and the medical staff. 19 Concerning these negative effects, not telling the truth to patients with cancer is inappropriate for patients who want to be informed.
The above results showed that the medical staff mainly prioritized the family members in disclosing disease diagnosis at the time of initial finding. Moreover, family members preferred to tell the truth to the patients by themselves. This might be related to the following factors. First, Confucianism has a profound influence on every aspect of Chinese citizens, 20,21 including medical decisions. Family-based decision making is given first priority. Patients believe that family members will make reasonable decisions in their best interests. In addition, the involvement of family members in decision making is perceived as a reflection of love from family members to the patient. 20 Second, telling the truth to family members is legally acceptable in China. According to Article 16 of the Doctor Law of the People’s Republic of China, 22 the doctor should frankly introduce diagnosis and prognosis to the patient or his or her family members and avoid harm to the patient. In clinical practice, the patient usually voluntarily selects one of his family members as his or her representative. Then the patient, his or her representative, and the doctors sign a proxy document together attesting that they know their rights and duties. In this situation, the doctors could communicate with the representative about the patient’s issues. Third, both the medical staff and family members consider that the patients might develop psychological complications and lose hope if they were told the truth. The above results showed that the reasons for doctors and family members not to tell the truth to the patient at the time of initial diagnosis included concerns about the patients losing hope and non-compliance. They strongly desired to protect the patients. Fourth, being diagnosed with cancer would probably result in substantial stress, not only in patients but also their family. The doctors tell the truth to family members at first in order to give them time to handle the situation and prepare the patients mentally. 23 Then, the patients would probably receive emotional support and comfort from family members during truth disclosure, which will help the patients maintain hope. 24 Cao’s et al. 25 showed that patients whose diagnosis was mainly disclosed by a family member have higher levels of hope compared with those who were mainly informed by doctors. The reason might be that the family members know the patients’ emotional condition best.
We found a significant difference between the patients and family members regarding who should tell the truth to the patients. More patients preferred to be informed by doctors and nearly half of the patients reported they were told by doctors. This corroborates Zafar et al., 26 in which three in five respondents wanted a healthcare provider to give them detailed information about prognosis and life expectancy. Studies showed most patients believe that their attending doctors are the only reliable source of information. 9 Therefore, strategies to facilitate information disclosure to patients by attending doctors would help meet the patients’ needs. Besides, the process of truth-telling could be improved by taking a multidisciplinary approach. 5,27 Nurses, as the most frequently contacted professionals for patients, could play active roles in truth-telling. 28 Before telling the truth, nurses can acquire the patients’ needs and willingness in truth-telling, share with the doctors, and help doctors choose appropriate strategies for truth-telling. After telling the truth, needs of emotional and informational support can be detected by nurses as early as possible, and timely support should be provided when necessary. 9 This multidisciplinary approach might help maintain hope in the patients.
The above results indicated that most patients (77.4%) preferred to be told all the truth at the time of initial diagnosis. However, few medical workers (3.7%) were willing to do this. Besides, only 59.8% of patients knew their diagnoses within 1 week after the finding. Informing partially and gradually in truth-telling instead of telling the whole story at the time of initial diagnosis might be related to the doctor’s intention to protect the patients and maintain hope. This also indicated that the medical staff did not really understand the patients’ desires. Further research should focus on the patients’ differences in attitudes and preferences to the amount and timing of information to be disclosed as well as the associated influencing factors, to provide evidences for choosing reasonable disclosure strategies in the light of ethical principles of autonomy and beneficence.
Conclusions and clinical implications
The disclosure of cancer diagnosis is a complex process involving the medical practice, as well as a range of cultural, ethical, legal, and regulatory factors. Truth-telling should be considered as a process through which the truth is revealed progressively, sensitively, and skillfully to help the patients understand and live with their illness, while maintaining a strong sense of hope. The medical staff are considered the most trusted informers by patients, and yet should assess and respect each patient’s willingness to know the truth, such as the amount and disclosure timing.
Family members, who might be those knowing the patients’ needs, preferences, and capacities, could play an important role and should be involved in helping the medical staff better understand the patients and choose an appropriate way for informing. Emotional support and comfort from family members are encouraged during truth disclosure. Anyone in the patient’s care team, especially nurses, should be included in the process of truth-telling.
Study limitations
There were several limitations in this study. First, the sample size was relatively small, and the trial was limited to two hospitals. The patients diagnosed with cancer at the outpatient clinic were not included. Therefore, these findings may not apply to the whole oncology population because some patients might not seek treatment after being told the truth. Second, sampling bias may have had an impact on findings since participation was voluntary and anonymous. The patients who did not participate might be those who did not want to know the truth. Third, the data were not detailed enough to allow the analysis of influencing factors. More in-depth research, featuring a larger dataset, is required to explore patients’ differences in attitudes and preferences to the amount and timing of truth-telling and the associated influencing factors.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by National Natural Science Foundation of China (71904200) and Shanghai Sailing Program (18YF1429400) from Science and Technology Commission of Shanghai Municipality.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.