
Abstract
Background:
Healthcare professionals follow codes of ethics, making them responsible for providing holistic care to all disaster victims. However, this often results in ethical dilemmas due to the need to provide rapid critical care while simultaneously attending to a complex spectrum of patient needs. These dilemmas can cause negative emotions to accumulate over time and impact physiological and psychological health, which can also threaten nurse–patient relationships.
Aim:
This study aimed to understand the experience of nurses who cared for burn victims of the color-dust explosion and the meaning of ethical relationships between nurse and patient.
Research design:
A qualitative descriptive study using a phenomenological approach.
Participants and research context:
Clinical nurses who provided care to the patients of the Formosa color-dust explosion of 2015 were selected by purposive sampling (N = 12) from a medical center in Taiwan. Data were collected using individual in-depth semi-structured interviews. Audiotaped interviews were transcribed and analyzed using Colaizzi’s method.
Ethical considerations:
This study was approved by the institutional review board of the study hospital. All participants provided written informed consent.
Findings
Three main themes described the essence of the ethical dilemmas experienced by nurses who cared for the burn-injured patients: (1) the calling must be answered, (2) the calling provoked my feelings, and (3) the calling called out my strengths.
Conclusions:
Healthcare providers should recognize that nurses believed they had an ethical responsibility to care for color-dust explosion burn victims. Understanding the feelings of nurses during the care of patients and encouraging them to differentiate between the self and the other by fostering patient–nurse relationships based on intersubjectivity could help nurses increase self-care and improve patient caregiving.
Introduction
The World Health Organization (WHO) defines a disaster as an occurrence disrupting normal conditions of existence and causing a level of suffering that exceeds the capacity of adjustment of the affected people. 1 Disasters involving burns are described as burn mass casualty incidents (BMCI), in which a massive influx of patients exceeds the capacity and capability of burn centers to respond. 2 BMCI may result from not only natural disasters, such as earthquakes, volcanic eruptions, and wildfires, but also from man-made accidents, nuclear and biological attacks, and chemical explosions. 3
BMCI occur without prior warning, and the large number of patients affected makes it impossible to triage nurses according to specialty, which can be stressful for frontline nurses. 4 The infrequency of BMCI prevents medical personnel, who are likely to be the first to manage burn casualties, from acquiring the necessary experience of how to respond emergently. 5 A literature review found that although nurses play a significant role in managing care of disaster victims, there is no mandated training for emergency response. 6 A quantitative study demonstrated that a lack of training was a source of significant stress and other psychological problems when treating burn victims. 7 However, there are few qualitative studies on the emotional experiences of nurses when required to respond to a BMCI.
Nurses have little time to deal with the emotional experience of caring for burn patients, and keeping busy was reported to be a common coping strategy for avoiding self-reflection and suppression of emotional responses. 8 Emotional stability is an important component of the quality of patient care, which has been shown to be a predictor of patient safety. 9 The limited training in disaster management for nurses 10 impacts physiological, psychological, cultural, spiritual, and moral aspects of an injured patient and their families. 11 Therefore, healthcare professionals could improve emotional stability by understanding the emotional responses of nurses when caring for disaster victims.
One means of shaping interactions and relationships between patient and nurse is to focus on the “the lived body,” 12 one of four components comprising Merleau-Ponty’s concept of embodiment, which nurses use to perceive their world. 13 The concept of the lived body is based on one’s self-reflection about personal and social interactions, which includes the mind and body as individual components, and their interactions. 14 Therefore, understanding a nurse’s internal psychological stresses during a disaster and the impact on the lived body could help nurses overcome the challenges of caring for survivors as well and for improving nurse–patient interactions.
Background
A dust fire occurred in Taiwan in June 2015 when staff at a water park sprayed clouds of colored corn starch toward attendees and the dust exploded, injuring nearly 500 people. 15 Of those injured, almost 50% of the injuries involved burns, averaging 44% of total body surface area (TBSA). It was the worst BMCI in the history of Taiwan; most burn-injured patients were teenagers who needed intensive care and treatment and long hospital stays to recover. 15
Although over 2000 studies have examined aspects of the Taiwan color-dust explosion, <30 include nurses as part of their research and none are qualitative. Therefore, knowledge about the emotional responses of nurses during the color-dust explosion is limited. Tseng et al. 7 examined quantitative measures of stress, resilience, and quality of life and reported that resilience was important for coping secondary traumatic stress from the color-dust explosion. Another study examined how hospital staff adapted to the overwhelming surge in patients and workload and the concomitant shortage of clinicians, beds, and medical materials. 16 However, their findings were practical responses for mobilization, rather than emotional responses to the experience.
Healthcare professionals follow a code of ethics, making them responsible for providing holistic care to disaster victims, which involves attending to the needs of the patient’s body, mind, and spirit to the best of their ability. 17 There is a growing body of evidence that emergency preparedness should address the needs of not only the patients but also the healthcare staff to ensure outcomes for both are ethically sound. 18 In contrast, guidelines developed by the International Council of Nurses (ICN) emphasize nurses’ ethical responsibility to focus on disaster victims’ psychological and emotional stress. 19 The pressure for nurses to rapidly respond and care for a large population of disaster victims, while simultaneously attending to a broad, complex spectrum of individual patient needs can cause psychological stress. 20 However, little attention is paid to the ethical dilemma of nurses’ feelings of uncertainty when providing patient care during a catastrophic event in unfamiliar surroundings and simultaneously attempting to manage their own stress.
Disasters bring about special ethical challenges that differ from those encountered during typical clinical nursing. The lack of human resources requires an increase in workload to provide adequate care for the survivors, which adds additional stress. 21 However, nurses have an ethical obligation not only to care for the patient, but also to care for themselves. Therefore, providing holistic care requires nurses to find a balance between meeting the needs of the patient as well as their own.
Dahlberg 22 proposed that intersubjectivity is a central concept in nursing and delineates the important relationship between the patient and nurse. Merleau-Ponty 13 believed intersubjectivity was important for nurse–patient interactions, as it facilitates intersubjective meetings, in which nurses (the carers) interact with patients (the cared-for) as individuals while maintaining their own sense of worth. 22 These intersubjective meetings help nurses provide holistic care to patients, on a continuum of a caring relationship with the patient, and the therapeutic self. 21 This obligation of caring, however, can cause conflict, which is especially prominent after a disaster when nurses are required to care for critically ill or wounded patients for extended periods of time. 22
Nursing professionals cannot ignore the pressure of their caregiving responsibilities, but they also need to care for their own body, feelings, emotions, and spirituality. 23 Therefore, nurses on the frontline caring for patients during disasters need the therapeutic self to care for their own body and self. 14 During the extended care nurses provided for patients injured in the color-dust explosion, levels of conflict and discomfort were shown to increase, which generated increased psychological pressure. 7 However, there is a gap in the literature regarding the personal and emotional experiences of these nurses during the course of caring for the burn victims. Understanding the experiences of nurses who have cared for patients of BMCI, such as the burn victims of the color-dust explosion, could lay the foundation for guiding care providers in how to manage and care for burn-injured patients, as well as how to help nurses balance the lived body and self during a disaster. How nurses responding to a BMCI face the ethical dilemma of caring for burn-injured patients in an unfamiliar setting during the journey from the acute phase to recovery is worthy of exploration. Therefore, the purpose of this study was to understand the experience of nurses who cared for the burn victims after the color-dust explosion and the meaning of ethical relationships between nurse and patient.
Methods
Design
A qualitative descriptive phenomenological design with face-to-face semi-structured interviews was used to gain an understanding of the meanings and essence of the experience 24 of nurses caring for burn-injured patients after the color-dust explosion. The goal of a phenomenological enquiry is to fully describe a lived experience at a particular point in time using details provided by the persons involved, in order to develop insights about the phenomenon. Qualitative studies using Husserl’s process of phenomenological reduction can be applied as a means to get “back to the things themselves.” 25
Participants
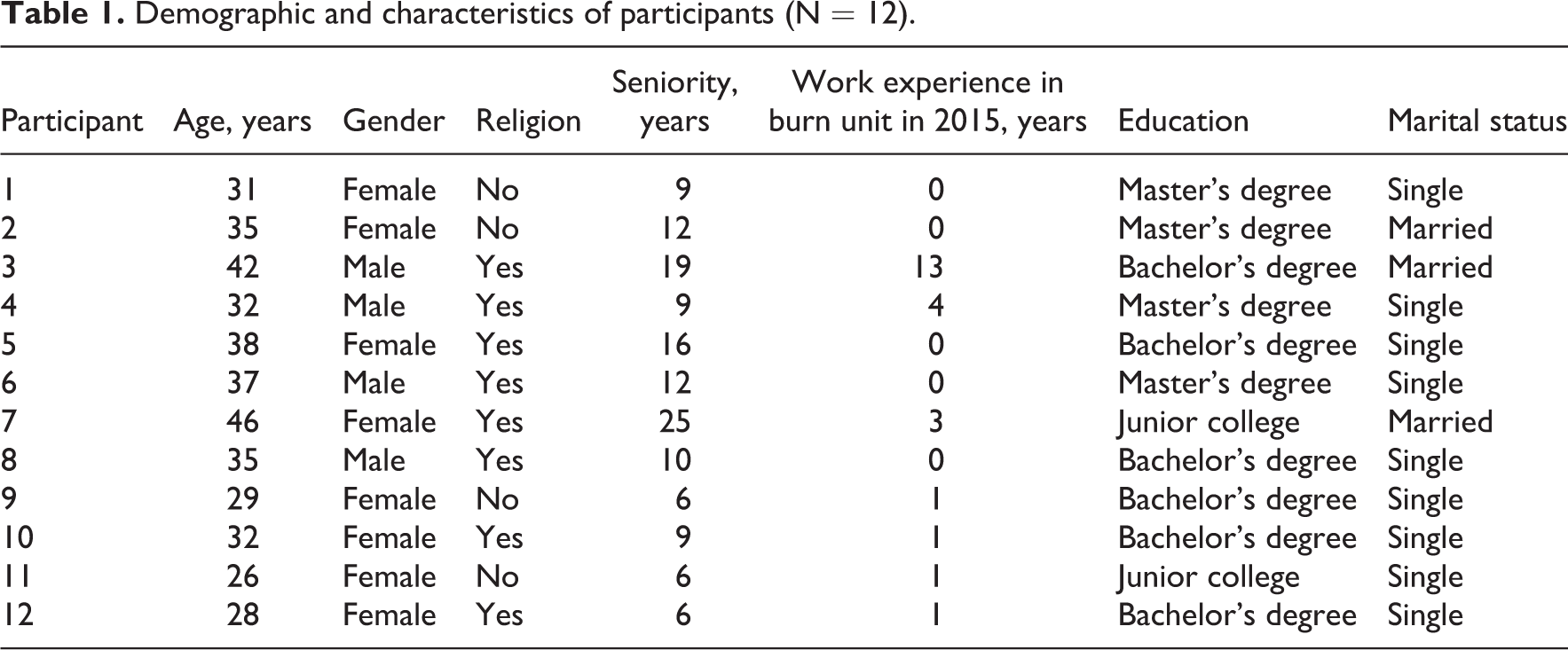
Nurses with clinical experience of providing care to burn-injured patients following the Formosa color-dust explosion were purposively sampled from a medical center in Taiwan. When the BMCI occurred, the hospital established a dedicated ward to care for the burn-injured patients from the acute to recovery phase. We posted a research flyer advertising the study to recruit nurses who had cared for burn victims in this special hospital ward. Nurses were eligible to participate in the study if they met the following inclusion criteria: (1) provided direct care to burn patients following the Formosa color-dust explosion victims for at least 2 weeks in the dedicated ward, (2) had at least 1 year of work experience in clinical nursing, and (3) willing to participate in this study. There were no exclusion criteria. A total of 12 nurses met the inclusion criteria and provided signed informed consent to participate in the interviews. Most participants were female (n = 8, 67%), the mean age was 34.6 years, the mean nursing seniority was 11.58 years, and the mean length of time with burn care experience was 2 years. Demographic characteristics of participants are shown in Table 1.
Demographic and characteristics of participants (N = 12).
Data collection
Data were collected from May to August 2020 using individual semi-structured, face-to-face, in-depth interviews. All 12 nurse participants were interviewed by the first author in a meeting room, which was a safe, quiet, and comfortable environment. The mean duration of the interviews was 58 min. Participants were asked to describe their past experiences of caring for the burn victims of the color-dust explosion by answering the following six questions: (1) What was your experience of caring for the burn victims every day? (2) What strength inspired you to continue to provide care to these burn-injured patients? (3) What was your most satisfying/proud/unforgettable/successful/experience? (4) What did the experience of caring for the burn victims mean to you? (5) Did these caregiving experiences change you in any way and how? and (6) Is there anything else you would like to share with me? All the interviews were audiotaped; the first author transcribed the audiotapes after completion of the interview. Data collection ceased when no new meanings emerged following analysis of the interview data; data saturation was reached after analysis of interview data from the 12th participant.
Ethical considerations
This study was approved by the institutional review board (IRB) of the study-site medical center (IRB number: C202005056). Following approval of the study, the first author approached the nurses who met the inclusion criteria and explained study purpose and procedures. Nurses were assured of privacy of their data and their right to withdraw from the study at any time and for any reason. All participants provided signed informed consent prior to being interviewed. Participant nurses were assured of privacy of their data and their right to withdraw from the study at any time and for any reason. All interview data were anonymized using identification numbers to ensure that personal data could not be traced back to any participant.
Data analysis
Data analysis was conducted by the primary investigator and the first three authors. Transcribed interview data were analyzed using the seven-step phenomenological approach developed by Colaizzi. 26 In the first step of the analysis, all the taped interviews were read and listened to numerous times until a sense of the whole was obtained. In the second step, significant statements relevant to the experiences of nurses as they cared for the color-dust explosion burn-injured patients were extracted from each transcript. In the third step, the formulated meanings were created from the significant statements. The authors conducted discussions with the research team to determine whether significant statements were compatible with the formulated meanings. During the fourth step, clusters of themes were identified and organized from the formulated meanings. Data were synthesized by the authors to express the essential structure of the caring experiences of the participants. The fifth step involved composing exhaustive descriptions of the experiences of the nurses when they were caring for the burn-injured patients. The researchers made the comparison between transcripts and themes several times to validate the findings. Supporting statements considered to be descriptions of themes identified in our findings were further validated in the sixth step. The final step involved a draft of the themes, which were then returned to the participants to confirm the study findings.
Rigor
Trustworthiness of the data was established by the criteria of Lincoln and Guba. 27 Credibility of our findings was enhanced by verbatim quotes from participants as well as member checking, which provided participants an opportunity to confirm or amend the researchers’ interpretation of their experiences. Transferability was enhanced by the thick descriptions provided by the participants and a reflective journal maintained by the first author. Transparency of the data was enhanced by maintaining an audit trail, which included details of participant selection, the context and the process of data collection, and data analysis. Consensus between the primary investigator and the first three authors was obtained for descriptions of meaning units from significant statements, themes formed from meaning units, and the study findings, which enhanced confirmability. In addition, researchers maintained in-depth descriptions of the findings, which confirmed the research process was consistent with the results.
Findings
When the color-dust disaster occurred, the Disaster Prevention and Response Department called hundreds of nurses to help manage burn-injured patients who had been transported to medical centers for emergent intensive care and treatment. The participants in our study had 6 to 25 years of experience in nursing, which included care of burn patients. However, caring for patients with critical burns was limited. Although one nurse had worked for 13 years in a burn unit (Participant #3), few participants had any experience in this type of unit.
Participants were an integral to the interprofessional teams for developing guidelines, discussing patients’ conditions, treatment protocols, and interventions. Responsibilities included wound dressing, monitoring vital signs, therapeutic treatments, and providing emotional support. All participants’ patients recovered completely and were discharged. To maintain continuity and provide holistic care, nurses remained with the patient from the acute care stage up to discharge.
Nurses viewed the request for help as a calling. Three main themes described the essence of the experiences of nurses who responded to the calling to care for patients who suffered from burn injuries following the color-dust explosion: (1) the calling must be answered, (2) the calling provoked my feelings, and (3) the calling called out my strengths. The third theme was divided into three subthemes: labor of nursing, work of nursing, and action of nursing. Themes and subthemes are summarized in Table 2.
Themes and subthemes of responses to call from the burn victims after color-dust explosion.
Theme 1: The calling must be answered
Nurses described responding to the call to care for patients immediately and without thought. They returned to the hospital to provide care for the severely burn-injured patients, regardless of what they were doing or where they were. They were eager to help take care of the patients; however, they also felt nervous and fearful, and were uncertain about how to care for severe burn injuries: At that time, I was honestly excited. I felt that I was needed. It seemed that I was helpful and was able to do something. I could also learn from taking care of the burned patients. (Participant 9) After receiving the notification from the hospital, I answered the call very soon. It felt it was a second-to-none choice, but I didn’t know exactly what I could do to help. I had a lot of professional nursing knowledge and skills. I hoped that I would be able to help the injured patients. (Participant 2) The biggest feeling was that everything was in chaos. For the burn-injured patients, the burns were like purgatory on earth. Patients who were less severely injured were transferred out. The ICU was at capacity with patients from the Color-Dust explosion. At that time, it was really out of order, and very chaotic. Supplies needed to manage the burn-injured patients were being delivered one-after-another. Patient care and management was challenging for caregivers of all levels. At the time, I was thinking, “How do I help these people?” (Participant 8)
Theme 2: The calling provoked my feelings
Nurses were caring for large numbers of patients, and this was their first experience with burn injuries. They had never encountered conditions like this before. Most patients had second- or third-degree burns, which were difficult to treat and made nurses uncertain about their ability to provide care: Many patients were admitted to the burn center with second- and third-degree burns. The blistered and charred skin was stuck to their burned clothes. I needed to remove the burned clothes first, and clean the broken skin. In fact, one patient was very scared when I cleaned her skin and I was fearful of touching it. I had never taken care of a patient with such severe burns. I did not know how to take care of and how to help these patients. I was fearful and nervous, but I couldn’t express my feelings. I only could be expressionless. (Participant 11) I remember I was very angry because the patient was irritable and restless. I could not help him calm down. I did not know what to do. It was difficult to control my emotions. I lost my temper and yelled directly at the patient. I complained to my colleagues that I was angry about the patient attending the party for pleasure and getting severely injured. The care for the injured patient increased our workload, and made us so busy. (Participant 9) Regarding the psychological aspect of the patients, I did not think that I could help them much. Because there were too many patients admitted to the burn center at the same time. We knew how provide surgical care of their wounds, but not how to heal their mind. The time for conversation with the patients was so limited, and I really couldn’t help them solve their psychological problems. (Participant 10)
Theme 3: The calling called out my strengths
Subtheme 3.1. Labor of nursing
Despite working under high pressure, nurses needed to face and manage the patient’s health problems that came one-after-the-other. Despite the heavy workload and feelings of exhaustion, nurses’ ethics and feelings of responsibility helped them focus their time and energy on caring for the needs of the patients. They drew on their personal strength to complete all their nursing tasks. One nurse mentioned, “Just work, just work, just complete everything that needed to be done. Although I was very tired and exhausted, I knew I must complete all the tasks nurses should do” (Participant 12). Another nurse had a similar experience saying, “Nursing care was full of challenges and uncertainty. I encountered severe burn-injured patients during my shifts, I tried my best to complete all the nursing tasks. Completed everything as the best as I could” (Participant 5).
Subtheme 3.2. Work of nursing
Nurses believed that care for patients was their job and responsibility. It was necessary to take on the responsibility and mission of the nursing profession. Their sense of nursing was a mission because they were invested in nursing as a profession, which motivated them to care for sick and fragile, and prompted them to provide appropriate interventions to alleviate patients’ suffering and discomfort resulting from their burn injuries: I was able to care for the burn-injured patients after the Color-Dust explosion because I accepted the sacred mission. At first, I did not dare to touch the severe burn wound. Then I learned how to help change the dressing, I adjusted myself to adapt to the care for these burn-injured patients, and tried as best as I possibly could. (Participant7) My job is nursing care, and my responsibility was the patient. I have received so much professional nursing training and education, and learned a lot of knowledge and skills to help alleviate patients’ pain and suffering. It was time for me to commit what I had learned to the burn patients. I tried my best to assist the patient to reduce their pain and discomfort. (Participant 10) He was my patient. I wanted to take good care of my patient. I never thought that there were other special powers driving me to work for my patients. However, the atmosphere of our interprofessional team members and coworkers united us, and helped us work hard together, which provided additional motivation. (Participant 1)
Subtheme 3.3. Action of nursing
Nurses developed a caring relationship with the burn-injured patients, committed themselves to the calling from the mass burn casualty, and focused on the process of recovery and rehabilitation of the patients. Nurses reported gaining valuable experiences in using their skills to care for burn-injured patients. One nurse choreographed a dance to help rehabilitate a patients’ movements as part of recovery. The nurse danced with the patients at their bedside. Dancing not only increased patients’ motivation for rehabilitation, but also produced a pleasing environment for the process of rehabilitation. This nurse stated, During dancing, I would squat down because the movement of squatting can help with rehabilitation. These patients might have a scar contracture behind their knee, so we taught them to squat and squat again to practice the rehabilitation movements. We all felt very happy. We escaped the low mood and depression present during the first moments. (Participant 11) The patient could walk all the way from their bed to the entrance door of the room. Because he could not wear shoes and he was afraid of infection on the soles, I paved the sterile skin towel along the whole way. Although the patient felt pain, we encouraged him by telling him he was very glorious, and was walking on the Green Avenue of Stars. (Participant 7) When I completed my tasks step by step, I really hoped that my efforts and hard work could be seen. I also expected to receive applause. However, I found later that I did not need to wait for applause. When I saw the effects of what I had done for the patients, and the values and importance of my existence, I felt very satisfied with my jobs and performances. My inner self told me that I did not need praise and applause. (Participant 9)
Discussion
Nurses responded to the calling of the color-dust explosion without any thoughts of the ethical dilemma of caring for patients needing a level of expertise they were uncertain they possessed and in a setting that was unfamiliar territory for most. However, participants were able to put aside their feelings of uncertainty to meet the challenge of providing critical care and establishing personal caring relationships with the patients because of their ethics, which they associated the nursing profession. The three themes that describe our findings are compared with other related studies and literature below.
Taking on the responsibilities of a nurse
Nurses were eager to apply their professional knowledge and skills to care for the burn-injured patients. The science of nursing has been demonstrated to be a powerful tool for transforming knowledge into the ability to act in an unfamiliar situation. 28 This caring in adverse situations is similar to nurses who cared for earthquake victims in Taiwan. 29 Participants believed they had an ethical responsibility to care for the patient to the best of their ability, in spite of their inexperience.
Although the average nursing experience was 11 years, few participants had hands-on proficiency in treating severe burn injuries. However, rather than succumbing to feelings of fear and uncertainty about being able to meet the needs of the burn victims, they faced this dilemma by refusing to abandon their ethical responsibility of providing patient care and met the challenge unselfishly. This finding is similar to a qualitative study in Iran in which nurses felt ethically responsible to prioritize patient care in a disaster, regardless of the challenges. 30 Although our participants overcame many challenges, we suggest disaster plans for burn victims include the availability of a senior nurse as a knowledge resource to reduce the fear and uncertainty for nurses in unfamiliar care settings.
Nurses also needed to overcome the chaos present in the burn units during the disaster. A qualitative meta-synthesis of nurses’ experiences in disaster situations found chaotic situations at disaster scenes impeded nurses’ ability to respond effectively. 31 Nurses needed to locate their own position in the chaotic situation and stabilize their body and their self before they could provide appropriate care to the burn-injured patients.
Feelings as cues for ethical caring
Nurses were not psychologically prepared to care for patients with second- and third-degree burns, a situation which is difficult even for experienced healthcare providers. The unfamiliar circumstances provoked feelings of stress, uncertainty, and a lack of confidence. Nurses needed to manage their feelings and emotions to focus on caregiving, and their caseloads were larger than normal. They were fearful of being short-tempered with patients, and one nurse regretted becoming angry with a patient. However, nurses were able to overcome these feelings by focusing on “the face of the Other,” which describes the concept of a relationship with another person that is experienced ethically and socially. 32
Although nurses lacked confidence due to inexperience with burn patients and the enormous number of patients admitted simultaneously during the disaster, none of the participants were hesitant to respond. A survey found nurses who experienced anticipatory disaster distress were more likely to be motivated to engage in disasters. 33 Therefore, despite the psychological stress of caring for patients in a chaotic environment with limited resources, the nurses in our study may have been motivated to overcome their inexperience and withstand the emotional stress to answer the calling to care for the burn victims. Nevertheless, a qualitative study of the experiences of nurses who cared for earthquake victims in New Zealand found support from family and friends helped with the stress during caregiving, but support was also needed once the disaster care concluded. 34 Therefore, administrative staff should consider follow-up support for nurses who have participated in disasters with high numbers of casualties such as BMCI.
The high workload and lack of support caused one nurse (Participant 9) to reproach her patient for getting injured while attending the water sports party. It was cathartic for the nurse, but not helpful for the patient. Emotions can influence nurse–patient relationships and compassion is an emotion important for demonstrating that a patient is cared for by a nurse. 35 The reproach from the nurse in our study demonstrated a lack of compassion for the patient’s suffering, although she was aware no one chooses to be injured. Compassion allows one to assume the responsibility for another’s suffering and is an ethical dimension of the human experience. 36 When nurses focus on themselves rather than the disaster victims, they have difficulty adjusting to the challenges of caregiving, which can not only affect the quality of nurse–patient interactions but also interfere with patient recovery. 30
Encounters between nurse and patient
Nurses believed their success in helping patients recover from their severe burns was because the calling to respond to the disaster caused them to actively use their creative strengths to improve nurse–patient relationships. The three subthemes that described this experience, labor of nursing, work of nursing, and action of nursing are similar to Hannah Arendt’s elements of taking an active approach to being human. 37 These three events are hierarchical: labor is a biological activity that sustains life in relation to one’s work; work affects one’s activity; however, activity is the only element that occurs between people. 38
Labor of nursing allowed nurses to balance their workload while meeting their nursing responsibilities. The nurses just did what was needed, using their body’s physical strength to complete all tasks. The work of nursing allowed nurses to care for the burn-injured patients by giving them strength to go beyond their own personal discomforts, such as touching the burns and changing the dressings. Nurses believed their previous training, as well as support from an interprofessional team, helped them provide the care that was needed by the critically injured patients. The third subtheme, the action of nursing, involved the development of nurse–patient intersubjective encounter, which facilitated relationships that were therapeutic as well as compassionate. Nurses worked with patients in creative ways to help patients set and meet their goals for rehabilitation and recovery.
Nurses established intersubjective encounter with patients as part of the patient’s care and became aware of their needs and feelings. In return, nurses developed an awareness of their true value as a nurse professional, which fostered a healing relationship with the patient. The nurses’ recognition of the meaning of their life’s activity allowed them to nourish themselves. One nurse (Participant 9) discovered she did not need applause from others. The meaning of caring for the injured patients confirmed the nurses’ value in helping these patients recover. Thus, our findings support Dahlberg’s perspective that intersubjective meetings, in which the carer helps the cared-for as an individual, fosters nurses’ maintenance of their own sense of worth. 22 Intersubjectivity is a central notion in nursing, which describes the important relationship between nurse and patient, and helps the nurse proceed from existence to being.
Limitations
This study had several limitations. The color-dust explosion occurred in 2015; thus, the participants’ retrospective descriptions of their experiences draw on memories that are 5 years old. Memories fade over time and we cannot be certain that participants remembered and reported every experience during the interviews. Second, we cannot compare our findings with studies on experiences of the care of other disaster victims, which are typically conducted shortly after the event. The nurses in this study were interviewed in a safe environment and the disaster was long past. Therefore, the study findings only can be applied to situations where life-threatening conditions no longer exist. However, the study results provide rich and meaningful descriptions of the nurses’ experiences, and can be used as a foundation for helping healthcare providers care for disaster victims and nurses involved in mass casualty incidents.
Conclusion and implications
Three main themes described the ethical dilemmas faced by nurses during their experiences of caring for burn-injured patients after the color-dust explosion: (1) the calling must be answered; (2) the calling provoked my feelings; and (3) the calling called out my strengths (labor of nursing, work of nursing, and action of nursing). These themes describe how both patient and nurse benefited from solving these ethical dilemmas and helped the nurses provide quality care for burn-injured patients. These experiences fill a gap in the literature regarding the personal experiences of nurses caring for patients of a BMCI. Nurses’ emotional responses could help healthcare providers recognize the impact of the need to fulfill the ethical responsibilities of nursing professionals while providing quality care during the process of answering the calling of a BMCI. Our findings could be used as a guide for developing supportive interventions for nurses working in high-pressure environments.
The three elements described by the third theme (labor, work, action) suggest that facilitating intersubjective encounters between nurses and patients could help nurses differentiate between the self and the other, which could not only help nurses develop caring and therapeutic relationships with the patients, but also help nurses proceed from existence to being. Nurses’ caregiving can provide self-nourishment and help them overcome the ethical dilemmas of their caregiving actions. Even without praise and applause from others, the nurses can commit their time and life to the care for these severely injured patients.
Supplemental material
Supplemental Material, sj-doc-1-nej-10.1177_09697330211003239 Calling nurses to care for burn victims after color-dust explosion
Supplemental Material, sj-doc-1-nej-10.1177_09697330211003239 for Calling nurses to care for burn victims after color-dust explosion by Yu-Lun Tsai, Tin Yi, Hsien-Hsien Chiang, Hsiang-Yun Lan, Hui-Hsun Chiang and Jen-Jiuan Liaw in Nursing Ethics
Footnotes
Acknowledgements
The authors wish to express their deepest appreciation to all participants in this study. We extend our thanks to all professional team in the caring of the color-dust explosion at Tri-Service General Hospital, Taipei, Taiwan.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a grant from the Ministry of National Defense-Medical Affairs Bureau (MAB-109-106).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.