
Abstract
Moral distress has been well reviewed in the literature with established deleterious side effects for all healthcare professionals, including nurses, physicians, and others. Yet, little is known about the quality and effectiveness of interventions directed to address moral distress. The aim of this integrative review is to analyze published intervention studies to determine their efficacy and applicability across hospital settings. Of the initial 1373 articles discovered in October 2020, 18 were appraised as relevant, with 1 study added by hand search and 2 after a repeated search was completed in January and then in May of 2021, for a total of 22 reviewed articles. This review revealed data mostly from nurses, with some studies making efforts to include other healthcare professions who have experienced moral distress. Education-based interventions showed the most success, though many reported limited power and few revealed statistically lowered moral distress post intervention. This may point to the difficulty in adequately addressing moral distress in real time without adequate support systems. Ultimately, these studies suggest potential frameworks which, when bolstered by organization-wide support, may aid in moral distress interventions making a measurable impact.
Keywords
Introduction
Moral distress occurs when clinicians cannot act on what they identify as a professional ethical obligation because of barriers outside their control. 1 Although first studied in critical care nurses,2–4 substantive work has been done using both qualitative5–12 and quantitative methods13–20 to characterize moral distress across settings and healthcare disciplines globally21,22 including nursing,11,17,20 medicine, 18 occupational therapy, 19 social work, 12 and pharmacy. 5 Recently, intervention studies have come into focus, as researchers and practitioners have identified the need to move beyond definitions and descriptions to active mitigation of moral distress.23–28 Thus far, published intervention studies are limited and organizational-level interventions are especially sparse, perhaps suggesting barriers in applicability, sustainability, or support.
High levels of moral distress are associated with deleterious side effects, such as burnout, compassion fatigue, and intention to leave a position.18,29–35 These symptoms occur because of the unpredictable and often distressing work conditions in hospitals, which can range from moral issues of perceived inappropriate treatment at the end of life20,29,36–39 and intra-team conflict36,40,41 to organizational aspects outside providers’ control, such as excessive documentation requirements, 39 high patient to staff ratios,42–46 or poor ethical climate.39,47–50 Research has linked such a complex moral and professional environment to moral distress, job dissatisfaction, medication errors, and burnout,51–54 underpinning its relevance to patients and providers alike. While some providers will adapt or react positively to morally distressing situations, 55 this is not always the case, 56 especially when organizational support is absent.39,50,57 An organization is responsible for creating context for its employees,28,56,58,59 and that context is integral to an employee’s sense of moral agency (or their willingness to act on ethical values, obligations, or commitments) which, in turn, is inversely mapped to moral distress.56,60–62 For healthcare providers working in organizations that do not attend to ethical climate or moral distress, moral distress may increase over time.30,63,64 Higher levels of moral distress are associated with intention to leave a current position for physicians, nurses, and other providers, with 15% to 26% actively considering leaving.29,39,40,64,65 Leaving their job may only further exacerbate moral distress symptoms for remaining staff (e.g. creating even higher patient: staff ratios). Furthermore, studies linking moral distress to burnout,54,66–69 especially across professions, 31 are concerning. Burnout and intention to leave the position, therefore, are perhaps the most concerning of moral distress side effects. A strong, consistent healthcare workforce is necessary not only to ensure job satisfaction among providers, but also to provide safe patient care.70,71 At the organizational level, retention is also important as high turnover is expensive and disruptive to unit functioning. 72
The Nursing Sensitive Indicators (NSI), National Health Care Retention, and RN (registered nurse) Staffing Report estimated the average cost in turnover of a single bedside nurse is US$44,375. 73 This results in the yearly average hospital loss of around US$4.9 million. 73 This gap can be bridged with agency or travel staff, critical staffing premium pay, or allowing the internal staffing pool to flex up their hours. 73 Yet, all of these strategies add expenses to an often already strained hospital budget. Furthermore, losing other healthcare providers, such as physicians (costing from US$36,743 to US$89,800), 74 pharmacists (costing from US$50,000 to US$90,000), 75 or respiratory therapists (replacement cost in one hospital totaling US$3447) 76 can also lead to an increase in hospital costs. No healthcare professional appears immune to moral distress,5,18,77 so organizational-level strategies to address moral distress may hold promise in addressing moral distress–related staff retention.
Given the prevalence of moral distress and its potential for negative consequences, organizations, clinicians, and researchers have been following its trajectory and recognize the need to intervene.24,26,27,78,79 The purpose of this integrative review was to examine existing moral distress interventions, inclusive of healthcare professions, and to describe the structure and overall effectiveness. A previous review was limited to interventions directed at critical care nurses published. 80 The authors reported many methodological limitations, low quality of evidence among predominantly quasi-experimental studies, and moderate level of intervention effectiveness in decreasing moral distress. 80 The articles presented in that review will be included here, in addition to any other hospital-based moral distress interventions (regardless of provider role).
Methods
Design and information sources
An integrative literature review using Whittemore and Knafl’s 81 methodology was performed. An integrative framework calls for inclusion of both non-experimental and experimental studies, 81 and was chosen to allow for a more holistic review of the literature. The electronic databases searched were: PubMed, CINAHL, Web of Science, and PsycINFO. Studies matching the search terms “moral distress” AND (“hospital” OR “unit” OR “organization”) were evaluated. Moral distress served as a linked term to help isolate it from other ethical constructs focused solely on “moral” or “distress.” Several search iterations were attempted to specifically target interventional studies, including terms, such as “intervention,” “program,” “education,” “model,” “pilot,” and “workshop,” but were ultimately rejected because they were discovered to erroneously exclude some key studies. A health sciences librarian was consulted to help with focusing search terms and collating data.
Search process
The initial search completed in October 2020 yielded 1373 articles. All results were transferred to the reference manager tool Zotero and remaining reporting guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement 82 (Figure 1). After removing duplicates, 786 articles remained. The articles’ titles and abstracts were then screened for relevance to the research questions and meeting of eligibility criteria. The remaining 47 articles were screened under more stringent exclusion criteria (see Figure 1). One article 83 was discovered and added to the study using a hand search of a moral distress review article. 80 The search was repeated in January and May of 2021 (with date limitations set to 2020–2021), to capture any additional studies since the initial search was completed. After completing this evaluation, 22 articles were chosen for final analysis.
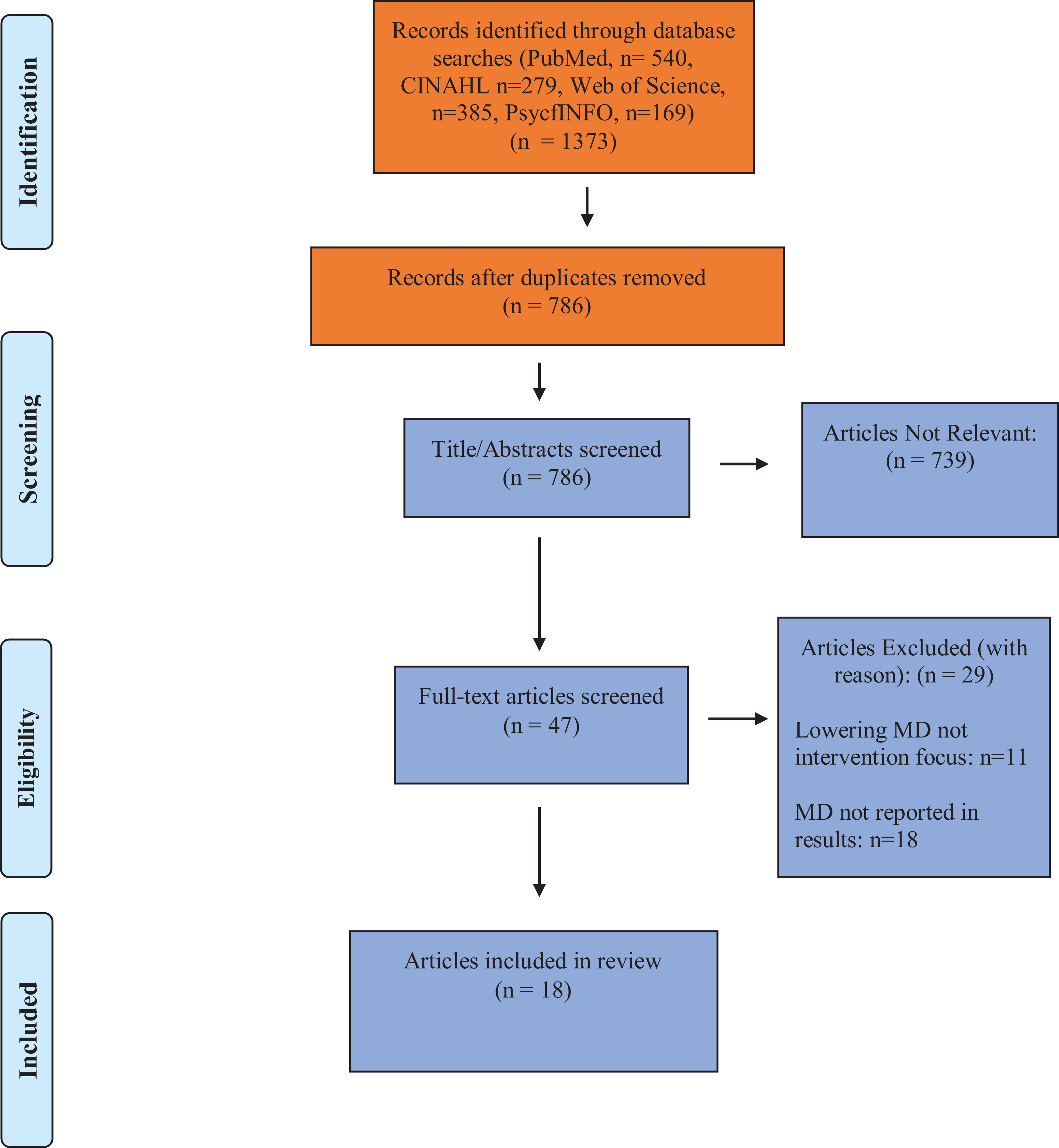
Initial search, October 2020, article flow diagram (modified PRISMA flow diagram).
Eligibility criteria
To allow for the most inclusive results, both experimental and quasi-experimental studies with an intervention component were included. In addition, interventional studies across the individual, unit, and organizational level were included, regardless of care setting (critical care, acute care, outpatient care facilities), specialty (pediatric, general, surgical, cardiac, etc.), healthcare profession, or locality. Reviews, commentaries, recommendations, and case studies were excluded. Studies not available in English, without an abstract, or were not full-text were excluded. Finally, no date constraints were placed for more robust study retrieval.
Data extraction
Extracted data included publication date, country, purpose, focus area, sample characteristics, research design and theory, intervention, outcome measures, results, and limitations (Table 1).
Moral distress interventions

ICU: intensive care unit; RCT: randomized control trial; MDS-R: Moral Distress Scale–Revised; RN: registered nurse; AACN: Association of Critical Care Nursing; NP: nurse practitioner; HCP: healthcare provider; PICU: pediatric intensive care unit; MDT: moral distress thermometer; CICU: cardiac intensive care unit.
Quality appraisal and risk of bias
Quality appraisal was conducted using the Johns Hopkins Nurse Evidence-Based Practice (JHNEBP) Model 105 for each of the final 22 identified studies. The studies ranged from level 1 (randomized control trials, RCTs) to level 3 (qualitative or mixed-methods studies) with quality scores ranging from 7 (out of 11) to 12 (out of 13). Quality scores were influenced by several factors, including non-random sampling, use of unvalidated instruments to measure intervention effectiveness, unreported demographic data, lack of power analysis, and small sample sizes. All 22 studies met quality criteria for this review. Finally, while publication bias is often a concern in literature reviews, 106 most of the articles included in this review had non-significant or marginally significant results, which reduced our concern for this type of bias.
Results
This review included 22 publications (see Table 1) as outlined in Figure 1.
Study characteristics
Four studies84,97,101,102 (18%) were RCTs. Two (9%) were qualitative,94,98 and seven (32%) were mixed methods, with a quasi-experimental pre- and post-test design and thematic analysis.83,86,87,91,93,96,99 The remainder (41%) were quasi-experimental with pre- and post-test design elements.85,88–90,92,95,100,103,104 Three studies were conducted in Iran,84,97,101 one in Sweden, 102 one in Canada, 96 and the remainder in the United States.83,85–89,91–95,98–100,103,104 All but three studies (86%)99–101 were conducted at a single institution. Sixteen studies (76%) were focused on nurses only.83–87,89–91,95–101,103 Six (27%) had mixed sample populations88,92,93,94,102,104 containing mostly nurses, followed by physicians, pharmacists, and then a small fraction of other healthcare providers (e.g. respiratory therapists, social workers, occupational therapists). Only four studies (18%) were hospital-wide.93,94,99,100 Twelve (55%) were focused in the intensive care unit (ICU)83–86,89,91,92,95,97,98,101,104 and five (23%) were in acute care units.87,90,96,102,103 The study by Brandon et al. 88 was population based and so included both ICU and acute care units. Demographic differences, such as professional, gender, or age bias were not uniformly addressed. Some studies made clear inclusion criteria for intervention recruitment,86,96,97,99,101,102 but most reported convenience sampling. Participants were predominantly female and employed as nurses, with at least 6 months of experience.
Theoretical frameworks
A theoretical framework did not consistently dictate interventional study design; 50% did not report any particular theory or model.87,89,90,92–95,98,100,101,104 Three (14%)83,84,91 used Nathaniel’s 107 model of moral reckoning. Nathaniel’s 107 three stages of ease, resolution, and reflection were integral to authors’ intervention layouts.83,84,91 For example, Abbasi et al. 84 regarded their training strategies for overcoming moral distress as the “resolution stage” 107 of Nathaniel’s theory; Chiafery et al. 91 adapted Nathaniel’s wording of “taking a stand or giving up” 107 to empower nurses beyond moral distress situations, and Allen and Butler 83 identified a “situational bind” within Nathaniel’s theory 107 to implement their educational intervention. The American Association of Critical Care Nursing (AACN) 4A model, 108 was used in two studies (9%).97,85 This model provides a systematic framework for addressing moral distress in critical care nurses, 109 which suited the critical care nurse–focused interventions of both Beumer 85 and Molazem et al. 97 Both Beumer 85 and Molazem et al. 97 presented the AACN 4A model in its entirety during their interventions, as a defined path to aid its participants in navigating moral distress events.
Other studies did mention other frameworks, including Robinson et al., 99 who embedded Rest’s 110 four components (moral sensitivity, guided process of decision-making, reflective practice, and continued development) into their residency program and utilized those principles to guide participant instruction. Bevan & Emerson 86 relied on Friere’s 111 Pedagogy of the Oppressed to develop a problem-posing education model to illuminate collective awareness and transformational change. Similarly, other single studies did make use of other frameworks, but none were repeated across studies. For example, Watson’s 112 concept of caring coupled with Johns’s 113 model of structured reflection, 96 Felgen’s 114 change model, 103 a comprehensive family centered model,88,115 and the democratic dialogue model,102,116 were all reported.
Interventions
Most interventions (59%) were completed in 3 months or less.83–86,91,93,94,96–98,100,101,103 The remainder were completed either in 6–8 months (23%),87,89,90,92,95 or in 12 months or more (18%).88,99,102,104 Outliers included four studies (18%),91,93,98,100 where evaluation took place only once immediately after intervention, and one (5%) study testing 20 months after. 88 No consistent length was advocated or followed.
Educational presentations or workshops were the most common (55%) intervention structure.83–86,89,90,95–97,99,100,102 These workshops varied in length from 30 min to 6 h, over weeks to several months. No specific format was followed across all studies, but each workshop typically included education on moral distress, debriefing sessions of moral distressing moments, case study analysis with role-play, and strategy development to help alleviate moral distress. Workshops were typically (83%) led by the authors,83,84,86,90,95–97,99,100,102 but one was run by unit leadership 85 and one by a social worker. 89 Additional details of each intervention are provided in Table 1.
The next predominant intervention (27%) was rooted in reflective practice.88,91,94,98,101,104 Open discussion of moral distressing situations with debriefing were provided by medical leadership, 88 an ethicist,91,98,104 or trained consult team members. 94 Saeedi et al. 101 differed in their intervention, using only written personal reflection over interactive discussions. In addition, Hamric and Epstein 94 took reflective practice further, by also identifying barriers and developing action-focused strategies aimed at alleviating the root causes of moral distress.
Four studies (18%) were outliers from the two main intervention groupings. Bosshardt et al. 87 focused on a policy change to give nurses ordering power for palliative care consults. The “mindfulness bundle,” of Vaclavik et al. 103 used tangible items (e.g. lavender sachets and yoga classes) aimed at relieving bedside nurses’ stress. Davis and Batcheller 92 provided electronic education on “resiliency strengthening techniques” (such as mindfulness reminders through cell phone applications or structured debriefings with pastoral care) to learn if staff awareness of these techniques increased over time. Epstein et al. 93 used an already established institution-wide intervention (the Moral Distress Consult Service) and assessed its effectiveness via the moral distress thermometer (MDT) and semi-structured interviews.
Intervention outcomes
Quantitative
To quantify changes in moral distress in response to an intervention, quantitative studies used either Corley’s Moral Distress Scale97,101 (MDS) or its revised version, the Moral Distress Scale–Revised83,84,86,87,89,90,95,96,99,103,104 (MDS-R), and four studies91,93,100,104 used the MDT. Corley et al. 42 developed the MDS, which was later revised by Hamric et al. 117 The MDS-R is shorter (with a reduction of 32 testing items to 21, as well as a Likert-type scale reduction from 1–7 to 0–4) and, like the MDS, allows for a composite score of moral distress intensity and frequency. 117 Both the MDS and the MDS-R include two additional questions about intention to leave due to moral distress. The MDT is a validated tool developed by Wocial and Weaver 118 and allows for point prevalence of moral distress via an 11-point scale. The remaining studies (24%) used other measures potentially linked to moral distress such as self-efficacy (Self-Efficacy Scale (SE)), 95 resilience (Connor–Davidson Resilience Scale (CD-RISC-25)), 92 empowerment (Psychological Empowerment Scale (PES)), 86 work effectiveness (Condition of Work Effectiveness Questionnaire-II (CWEQ-II)). 86
Six of the 16 studies (38%) measuring moral distress using the MDS, MDS-R, or MDT showed significant difference post intervention (see Table 2). A trend in moral distress levels was reported by seven studies,83,88,89,92,98,103,104 but none were statistically significant. Leggett et al. 95 revealed higher moral distress immediately post intervention, but ultimately no difference at 6 months. Using other instruments as detailed in Table 1, Rushton et al. 100 reported significant increase in ethical confidence, ethical competence, resiliency, engagement, and mindful awareness. Davis and Batcheller 92 also reported an increase in self-resiliency post intervention.
Significant quantitative reported results from intervention studies.
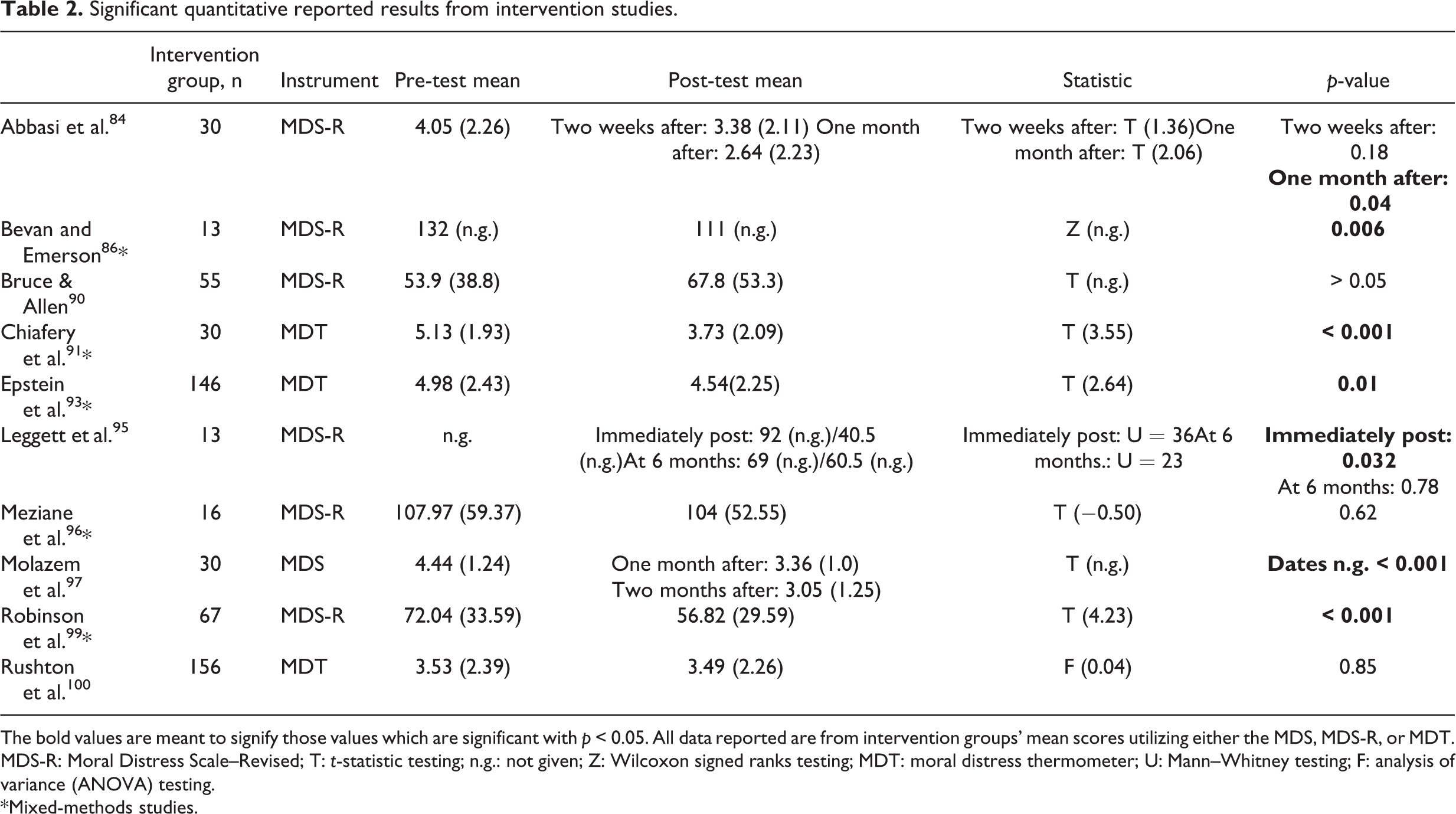
The bold values are meant to signify those values which are significant with p < 0.05. All data reported are from intervention groups’ mean scores utilizing either the MDS, MDS-R, or MDT. MDS-R: Moral Distress Scale–Revised; T: t-statistic testing; n.g.: not given; Z: Wilcoxon signed ranks testing; MDT: moral distress thermometer; U: Mann–Whitney testing; F: analysis of variance (ANOVA) testing.
*Mixed-methods studies.
Qualitative
Hamric and Epstein 94 and Reilly and Jurchak 98 used thematic analysis to describe staff evaluations of a moral distress intervention. Hamric and Epstein 94 performed post-intervention interviews to reveal five overlapping themes: acknowledgment of staff concerns, staff empowerment, staff engagement, improved team collaboration, and unit- or organizational-level change. Reilly and Jurchak 98 used focus groups post intervention to report similar themes of increased sense of value, personal growth and development, and an improved ethical practice environment.
Mixed methods
The mixed-methods studies83,86,87,91,93,96,99 combined quantitative measures (either the MDS-R,83,87,96 the MDT,91,93 or a combination of the MDS-R with other moral distress–related measures)86,99 and some form of qualitative assessment (either focus groups, 83 a free-text comment section in a questionnaire,87,91,96,99 or interviews)86,93 to assess intervention effectiveness from their participants’ perspectives. Quantitative data were similarly varied as in the strictly quantitative studies: Bevan and Emerson 86 reported no statistically significant difference in empowerment or work effectiveness post intervention, Allen and Butler 83 noted a decreasing trend in moral distress, which was not significant, Bosshardt et al. 87 and Meziane et al. 96 reported no difference in moral distress scores. Some qualitative data were similar to that reported by Hamric and Epstein 94 and Reilly and Jurchak, 98 with themes surrounding empowerment83,93 and self-efficacy, 99 but others reflected possible sources of moral distress, like inadequate staffing 87 or power dynamics86,93 or even general appreciation of the intervention,91,96 rather than changes in staff outcomes.
Other outcomes
Ten studies reported participants receiving interventions as positive experiences.83,88,89,91–94,96,98,102 No studies reported interventions as negatively received. As a counterpoint, however, and although not a measured outcome, Hamric and Epstein 94 mentioned possible re-traumatization during debriefings. Furthermore, Saeedi et al. 101 and Meziane et al. 96 lamented the time-intensive nature of their journaling interventions.
Six studies reported on intent to leave the position. Beumer 85 and Brandon et al. 88 found a decreasing trend in intent to leave post intervention, while Abbasi et al., 84 Bosshardt et al., 87 Browning and Cruz, 89 and Rushton et al. 100 reported no difference.
Discussion
A main finding of this integrative review is that a variety of moral distress interventions have been implemented, though mainly within the scope of educational workshops and reflective practice. Interventions in the hospital setting can be difficult to achieve, especially given healthcare providers’ busy schedules and the complex, chaotic realm of a hospital. Participants capable of engaging in interventions and providing unhurried responses about morally distressing situations can prove challenging, and was reflected in the commonly reported study limitation of small sample size.83–86,89–98,101,103,104 Most of the interventions discovered in this review were likely chosen to best suit their particular environment and took into account available resources, leadership support, and cultural differences, but recruitment should remain a high priority for future intervention studies. This will likely add to overall intervention implementation costs, which may prove prohibitive in some settings, especially with limited external funding. The role of organizational support in supporting an effective moral distress intervention is tantamount, and was elucidated in several studies reviewed here.94,98,101,102 Without such support, intervention implementation is likely to be challenging. Theoretical frameworks varied, though Nathaniel’s 107 model of moral reckoning and the AACN 4A Model 108 were the most often used.83–85,97,91 Both of these frameworks center on moral distress alone, which may point to their overall usefulness when planning future interventions. However, the AACN 4A Model is specifically geared toward critical care nurses, 108 so adjustments may need to be made if a planned intervention is targeted to other healthcare populations. Varcoe et al. 28 highlighted the need for an underpinning framework when considering moral distress interventions, and we would agree.
Prior systematic reviews on moral distress are mostly descriptive in nature. They do, however, offer conclusions about the general paucity of evidence on moral distress interventions.17,21,119 The studies reviewed here reflect moral distress, its negative consequences for staff, and the potential for effective interventions. The variety of intervention designs and outcome measures may be an indication of the difficulty in addressing moral distress. A more standardized, robust approach for moral distress interventions using validated tools and consistent follow-up is likely needed to determine if moral distress interventions are effective. Furthermore, these interventions need not be limited to single units, particular staff, or specific patient populations as moral distress is pervasive across hospital systems. A larger intervention group will not only aide in determining effectiveness, but also has the potential to help more staff who may be suffering. Organizations, therefore, may be in a unique space to advocate for hospital-wide interventions to combat moral distress. By financially and structurally supporting their staff in developing plans outside of their units and professions, hospitals could ultimately help develop the robust, effective interventions that its staff needs.
Limitations
This review was based exclusively on full-text articles in English, which could have excluded abstracts, presentations, theses, and unpublished reports capable of adding to the presented evidence. In addition, studies were screened by a single author, which cannot excuse the possibility of some interventional studies being excluded in error.
Conclusion
Many stress-inducing factors embedded in hospital environments have no hope of being controlled, as politico-cultural influences, advanced patient care, and technological interfaces become increasingly complex. To that end, moral distress may never be completely erased from healthcare providers’ experiences. However, this review highlights that no standard intervention framework to alleviate moral distress currently exists. With knowledge of what moral distress is and is not, and especially considering some problems responsible for moral distress are systems oriented, organizations can provide resources to help their practitioners consider and address the malleable system factors that tend to cause moral distress.