
Abstract
Background
Duty to care is integral to nursing practice. Personal obligations that normally conflict with professional obligations are likely amplified during a public health emergency such as COVID-19. Organizations can facilitate a nurse’s ability to fulfill the duty to care without compromising on personal obligations.
Research Aim
The study aimed to explore the relationships among duty to care, perception of supportive environment, perceived stress, and COVID-19-specific anxieties in nurses working directly with COVID-19 patients.
Research Design
The study design was a cross-sectional descriptive study using an online survey. It was conducted at an ANCC Magnet® designated 385-bed acute care teaching hospital located in a suburban area.
Participants and Research Context
Included in this study were 339 medical surgical nurses working directly with COVID-19 patients during the early phase of the pandemic.
Ethical Considerations
The study was reviewed by the institution’s clinical research committee and determined to be exempt. A survey invitation letter with a voluntary implied consent agreement was sent to participants with a description of the research study attached to the anonymous survey.
Results
Nurses with specific COVID-19-related anxieties were more likely to agree that it was ethical to abandon the workplace during a pandemic.
Conclusions
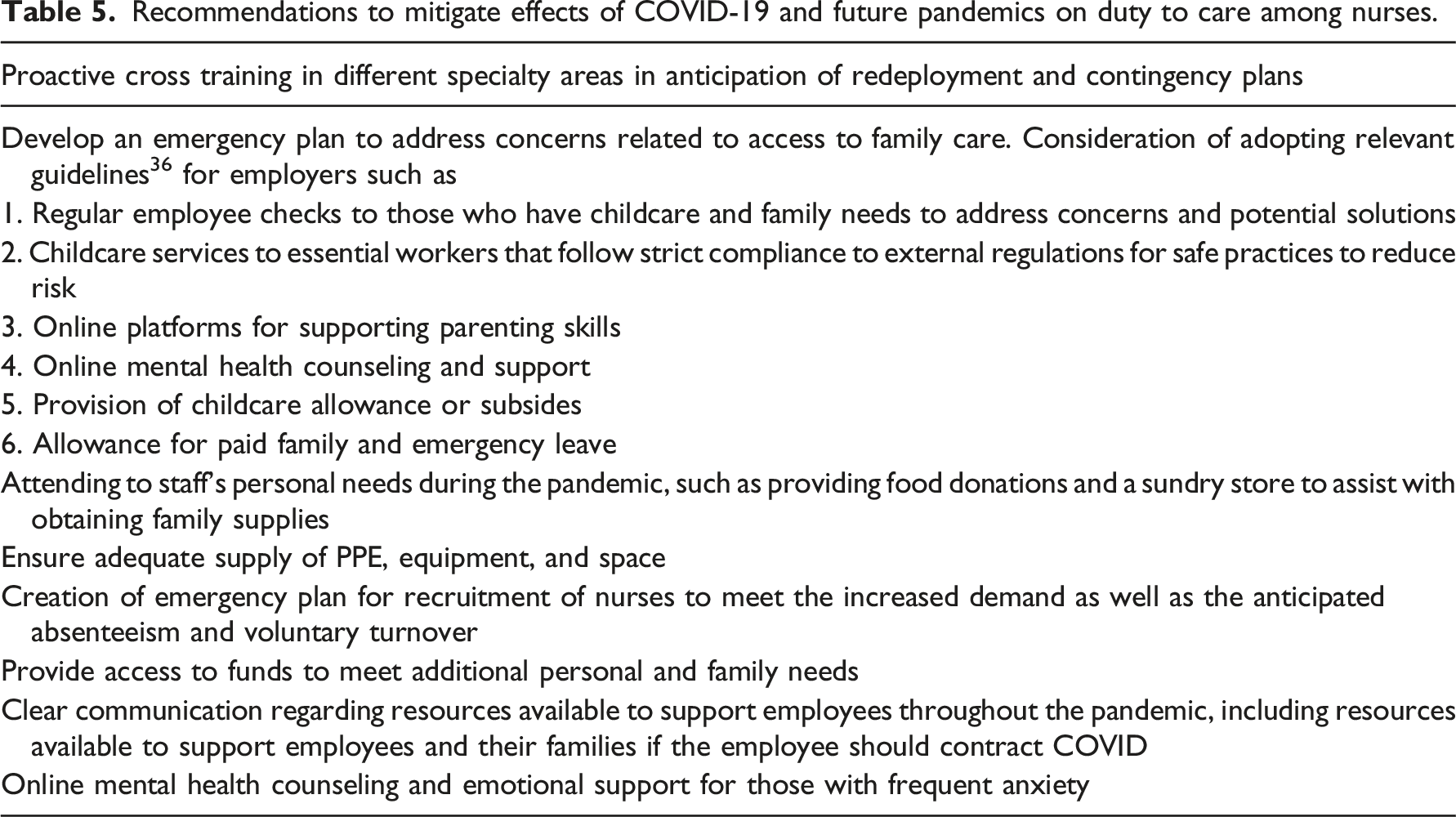
Organizations can and ought to mitigate the negative effects of COVID-19 on duty to care in future pandemics and healthcare emergencies by incorporating several recommendations derived from this study.
Introduction
Early in 2020, the COVID-19 pandemic expanded its global reach to include North America. Along with evolving information about the complexities and uncertainties of clinical management came stories of health systems overwhelmed by the number of patients requiring treatment. Epidemiological and clinical unknowns and COVID’s rapid global spread distinguished it from other recent pandemics. During March and April 2020, healthcare workers (HCWs), and in particular nurses, were confronted with unknowns of patient management, including mechanism of spread and uncertain clinical and epidemiologic challenges of COVID-19. Other concerns confronting individual HCW were availability of employee virus testing, consequences of a positive test, adequacy of personal protective equipment (PPE), and provider coverage for increasing patient needs. 1 This study sought to identify specific concerns that cause nurses to question the duty to care within the context of t the COVID-19 pandemic.
Background
Within bioethics, the duty to care, as noted by Ruderman et al. and others2, 3 obliges nurses to act on the ethical principle of beneficence. The American Nurses Association Code of Ethics for Nurses with Interpretive Statements notes that the nurse’s primary duty is to the recipient of nursing care; however, it also notes that nurses have a duty to protect their own health so that they remain available to serve patients and the community.4, 5 Reporting to work is the first step in exercising both beneficence and the duty to care 6 ; however, Qureshi et al. 7 found barriers to reporting to work during a public health emergency (PHE), including concern for family and personal health.
In addition, there are other obstacles to satisfying the duty to care during a PHE. First, during a PHE such as a pandemic, HCW and systems may need to reorient their clinical focus from the individual relationship of provider to patient to that of provider for the public good. 8 One example of this is the restriction of family access to hospitalized patients, adversely impacting the quality of the patient experience and the nursing workflow, but reducing the risk of viral transmission in the community. Second, the HCW may be placed in the stressful position of having personal concerns and obligations such as the health and safety of their family members that compete with their professional obligations.7, 9 Those personal obligations that may normally challenge the nurse’s duty to care can be further exacerbated by the inherent psychological and of a PHE. 10 Third, HCWs may be distressed by having to provide care in hospital areas/units with which they are unfamiliar. Taken together, these obstacles can be overwhelming, contribute to the perception that the work environment is not supportive, and weaken the influence of the duty to care tenet. A supportive work environment is known to have positive correlations with burnout and safe patient care, 1 but further study on the limits on the duty to care as it relates to the relationship between organizational support was required. 3
Building upon the SARS research11–15 that addressed the psychological burden and responses of HCW, Bohlken et al. 16 and others 17 suggest that the COVID-19 pandemic uniquely complicates decisions about fulfilling the duty to care.17–19 Examining the relationship between the nurse’s sense of organizational support during a time of crisis is an essential component in understanding how nurses negotiate obligations that compete with the duty to care.17, 20, 21 Furthermore, understanding the role of a supportive environment in regard to COVID-19-specific anxieties was important to improve future emergency response preparedness plans relative to ensuring safe and quality patient care.2, 7
The various stressors influenced by COVID-19 were investigated because of their relationship to the HCW’s duty to care. As Sperling recently found, 22 some nurses expressed a preference to not care for patients with COVID-19 and concern about their competency in caring for those patients, suggesting that these factors may influence the duty to care. Sperling did not, however, explore additional COVID-19-specific anxieties or perceptions of organizational support that directly affect the duty to care. Thus, identifying the specific concerns that caused nurses to question the duty to care is essential for future emergency preparedness planning within healthcare systems. Accordingly, we investigated the relationship between the duty to care, healthcare worker’s perceptions of organizational support and certain other recognized COVID-19-related anxieties, such as access to appropriate PPE, risk of contracting or transmitting infection, the level of organizational support in such circumstances, and receipt of trustworthy information from organizational leaders. 21
Purpose
The purpose of this research study was to explore the relationships among duty to care, perception of supportive environment, perceived stress, and COVID-19-specific anxieties in nurses working directly with COVID-19 patients. Additionally, the study sought to provide recommendations for future emergency response planning and operations so as to mitigate the factors inhibiting the duty to care.
Methods
The study design was a cross sectional descriptive study using an anonymous online survey conducted over a 3-week period from 27 April 2020 to 15 May 2020. The study was conducted at an American Nurses Credentialing Center (ANCC) twice-designated Magnet® 385-bed acute care teaching hospital. During this time period the average COVID-19 census was 70, with an average of 20 patients in the intensive care unit.
The survey was sent to approximately 1,000 direct care nurses working on medical surgical units. 462 nurses responded, yielding an estimated response rate of 46%. In this analysis, we included only those 339 nurse respondents with direct responsibility for COVID-19 patients.
Ethical Considerations
The study was reviewed by the institutional clinical research committee and determined to be exempt under category II per 45CFR 46.101(b) because it was anonymous and investigators had no way to identify the respondents or non-respondents. A survey invitation letter with a voluntary implied consent agreement was sent to all participants with a description of the research study was attached to the anonymous survey. By completing the survey, participants were determined to have consented to participate in the research study. The survey was administered online via Survey Monkey™ in secured format. In order to ensure the confidentiality of survey responses, the survey was configured to collect strictly anonymous responses; first and last names, Email address, and IP address were not collected.
Data Collection
Statistical Analysis
Descriptive statistics were used to summarize respondents’ demographic characteristics. Bivariate and multivariate analyses were performed. Unadjusted and adjusted odds ratios (adjusted for longevity in the profession and presence of a minor child in the household) were calculated with upper and lower 95% confidence intervals. Linear regression analysis was used to measure the correlation between the continuous variables of levels of perceived stress and levels of perceived organizational support.
Results
The survey was sent to approximately 1,000 direct care nurses working on medical surgical units. 462 nurses responded, yielding an estimated response rate of 46%. In this analysis, we included only those 339 nurse respondents with direct responsibility for delivering care to COVID-19 patients.
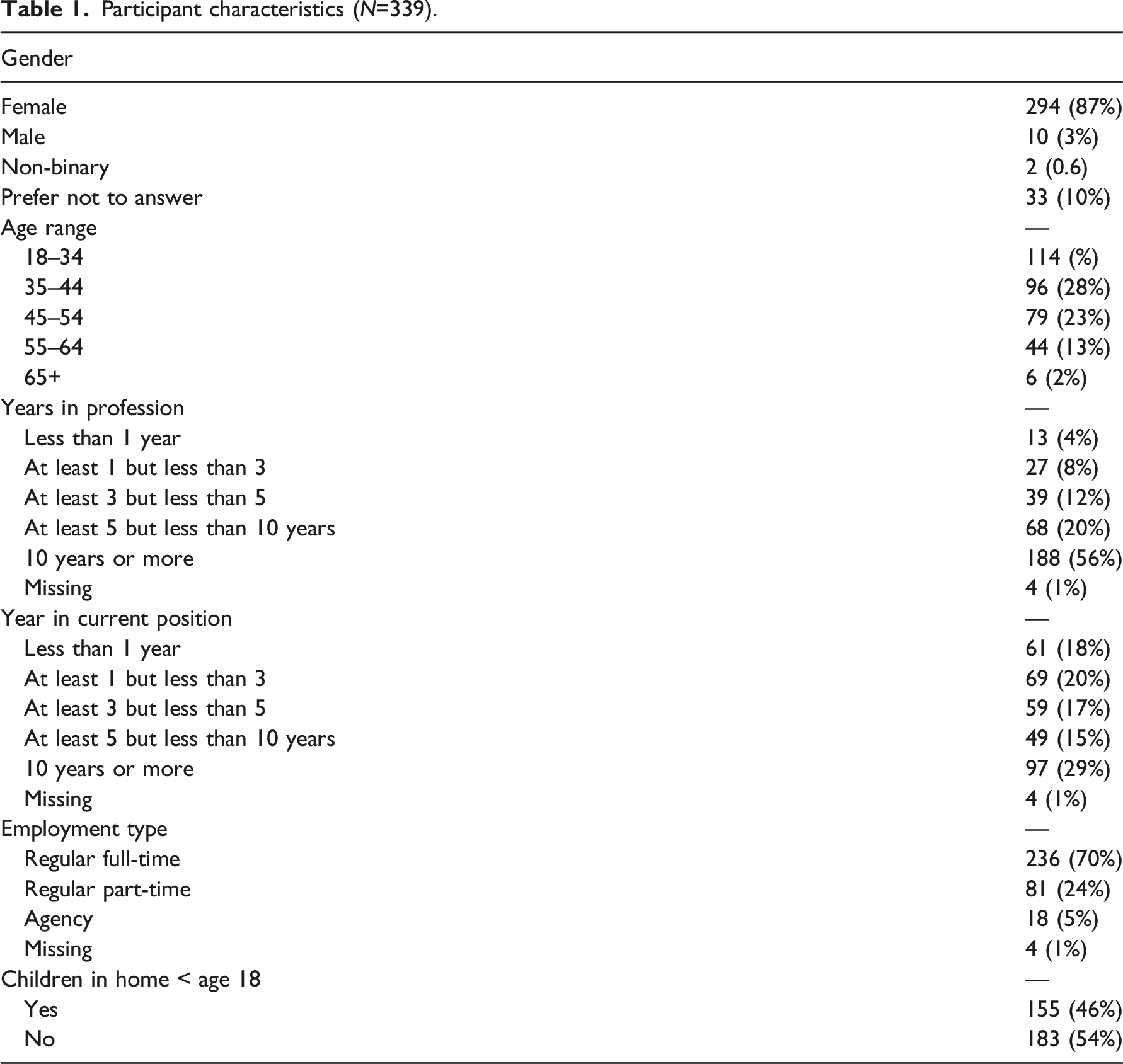
Participant characteristics (N=339).
Stress responses
The mean stress score of 339 respondents was 7.5 (range 0–15; standard deviation 3.0).
Perceived Organizational Support
The mean score of 339 respondents was 25.0 (range 8–36; standard deviation 4.2).
Anxiety Responses
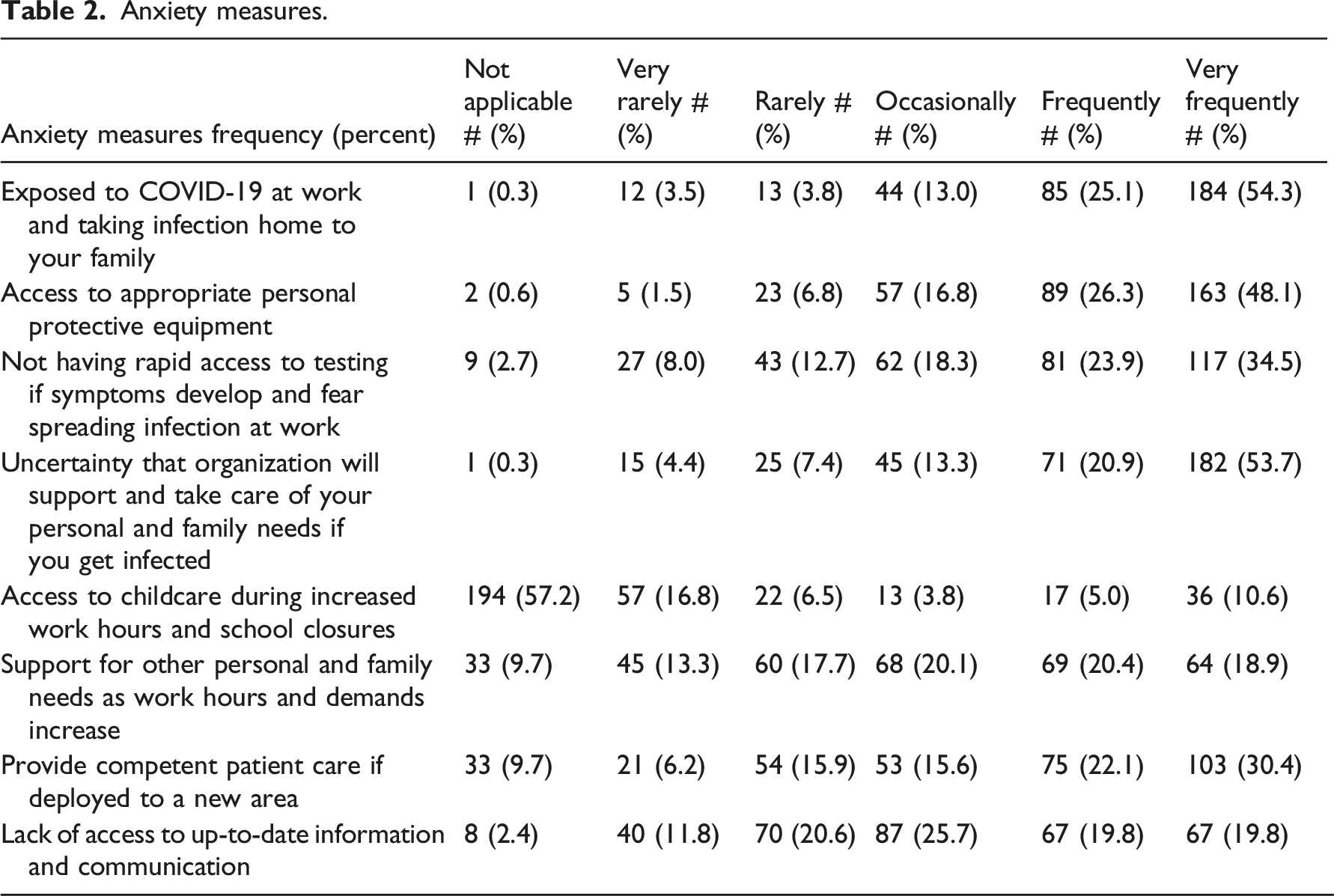
Anxiety measures.
Duty to Care
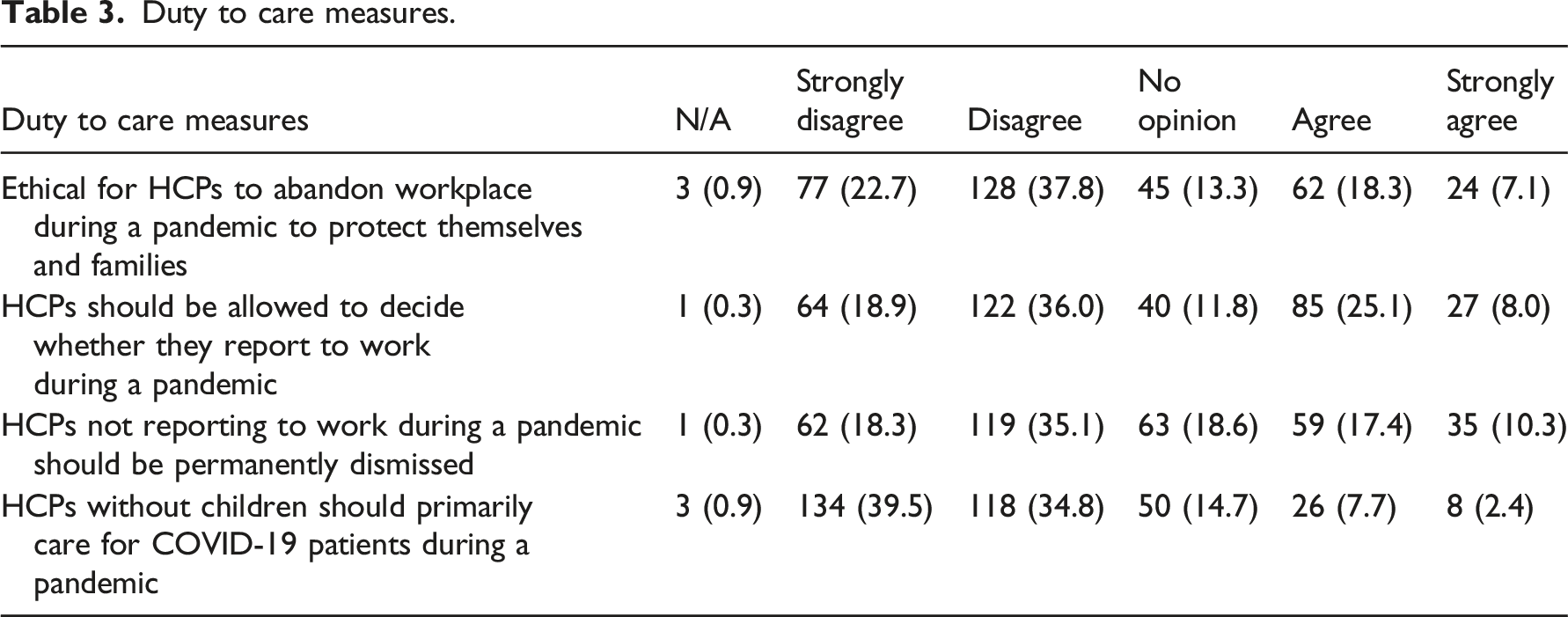
Duty to care measures.
This study also examined the interaction between the duty to care items (Table 3) and the eight anxiety measures (Table 2) via unadjusted and adjusted odds ratios on non-neutral responses. These analyses are shown in Figures 1–4 and discussed below. Adjustments were for longevity in the profession and presence of a minor child in the household. Non-neutral respondents excluded those who answered “non-applicable” or “no opinion” on duty to care questions and those who answered “not applicable” or “occasionally” on anxiety questions. Abbreviations: est=odds ratio, ll=lower confidence limit, ucl=upper confidence limit, prob=p value, n=count, ORG=organization, PPE=personal protective equipment. Abbreviations: est=odds ratio, ll=lower confidence limit, ucl=upper confidence limit, prob=p value, n=count, ORG=organization, PPE=personal protective equipment. Abbreviations: est=odds ratio, ll=lower confidence limit, ucl=upper confidence limit, prob=p value, n=count, ORG=organization, PPE=personal protective equipment. Abbreviations: est=odds ratio, ll=lower confidence limit, ucl=upper confidence limit, prob=p value, n=count, ORG=organization, PPE=personal protective equipment.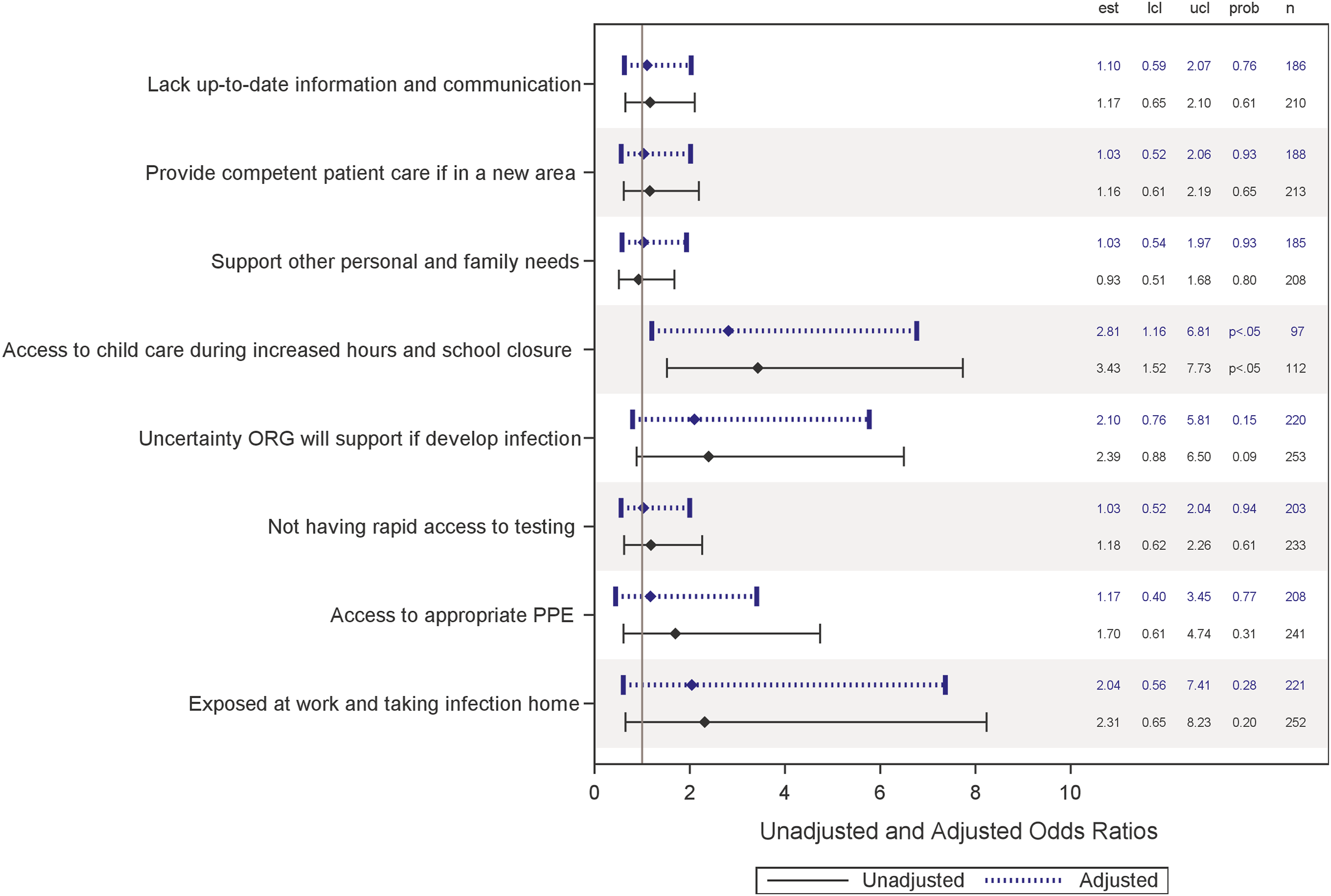
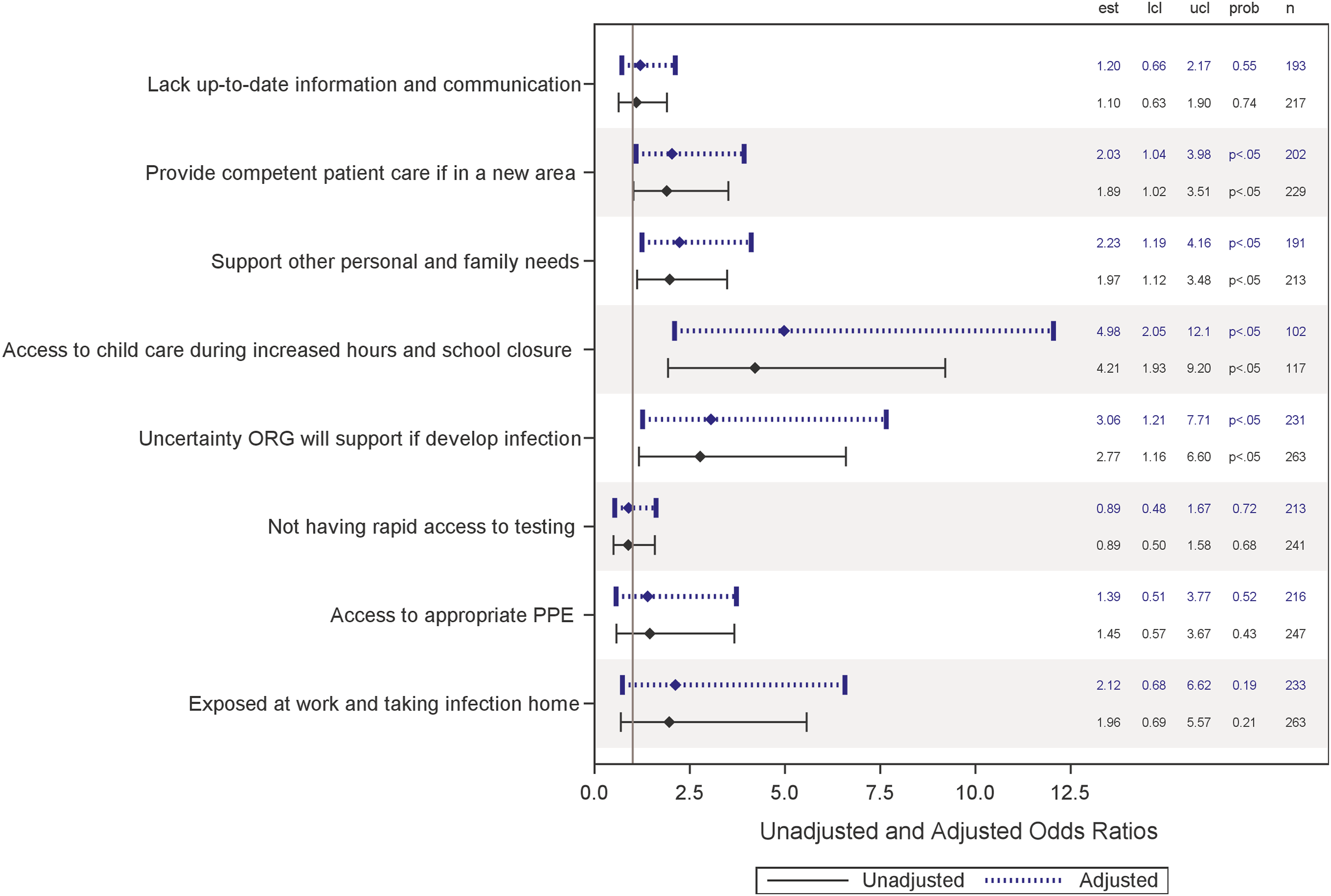
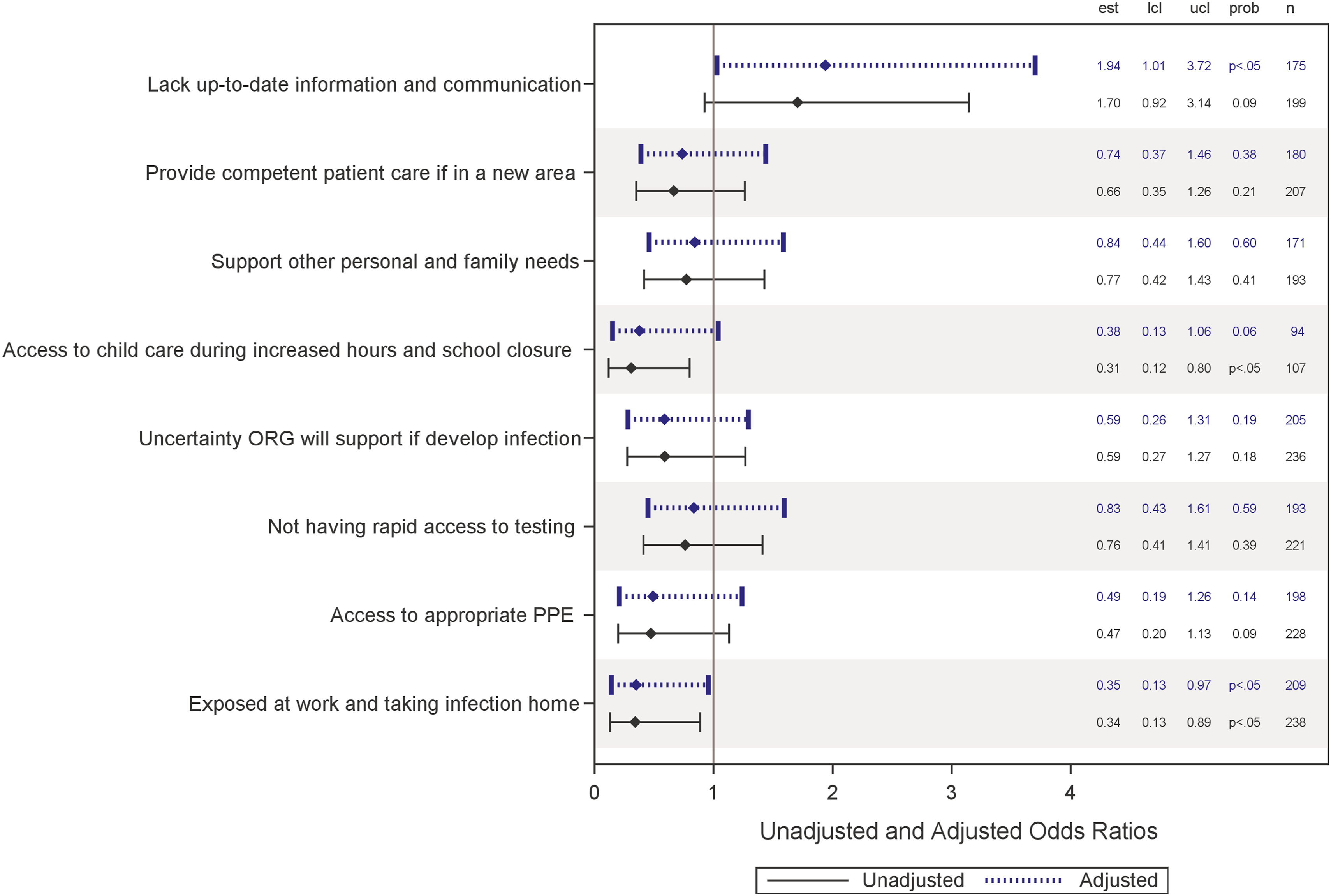
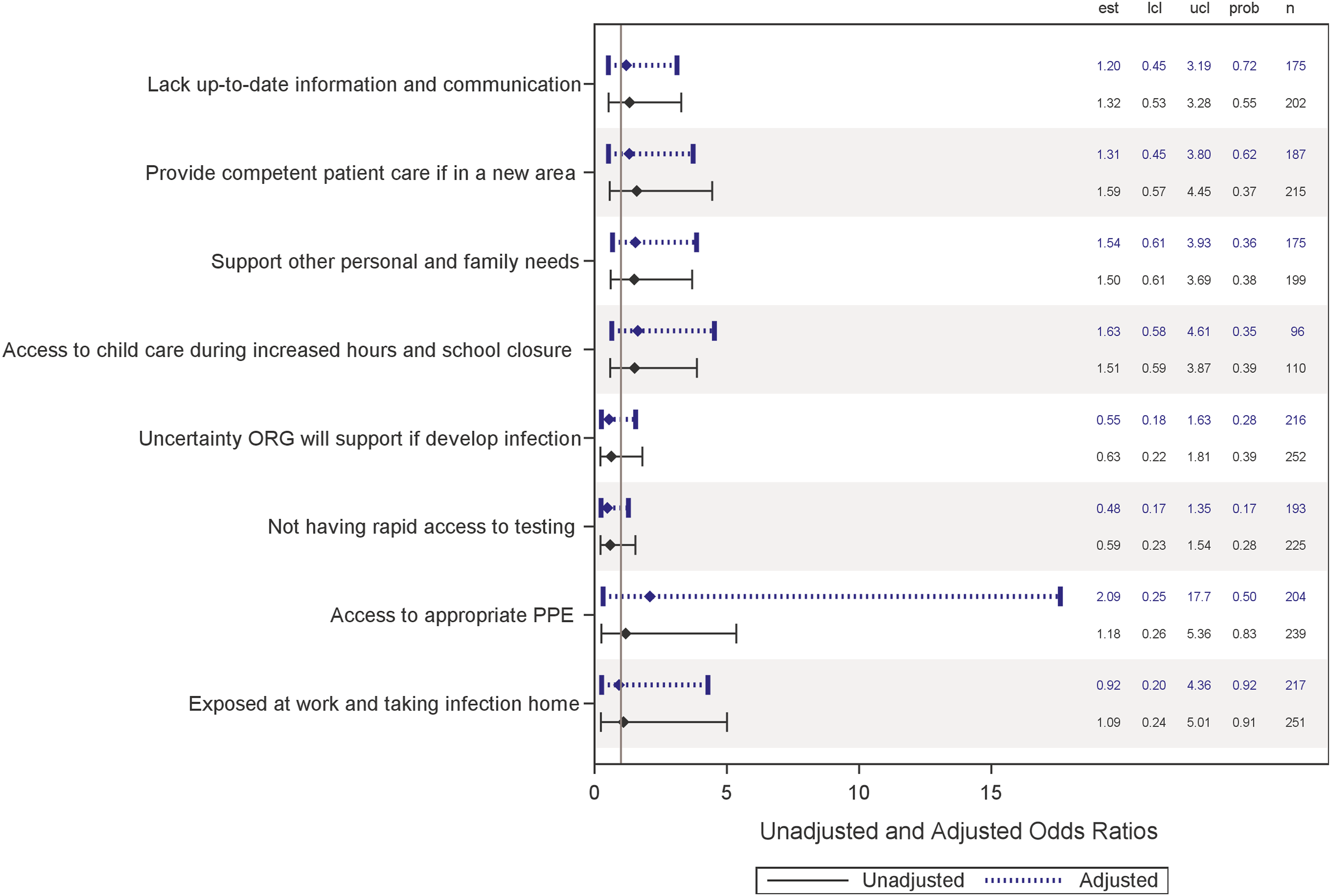
Figure 1 shows the unadjusted and adjusted odds ratios for the eight anxiety measures with the belief that individuals should be able to decide not to report to work. The three 3 significant effects (both unadjusted and adjusted) were: anxiety about providing competent care in a new area (2.0 times more likely); anxiety over whether the organization will support personal and family needs (2.2 times more likely); anxiety over uncertainty that the organization will support the individual if infected (3.1 times as likely); and anxiety over access to childcare during times of school closure (5.0 times more likely).
Moreover, respondents who expressed frequent or very frequent anxiety over access to childcare during increased work hours and school closures were 2.8 times more likely (adjusted effect is 3.4 times more likely) to believe that it is ethical to abandon the workplace as other respondents (Figure 2).
In addition, respondents were 2.9 times less likely to believe that healthcare providers should be dismissed for failing to report to work if they were anxious about being exposed at work and taking infection home or anxious about childcare and school closure. For anxiety about childcare, the adjusted odds ratio was not significant. But those with anxiety about lacking up-to-date information about COVID-19 were nearly 1.9 times more likely after adjusting for longevity and presence of children under 18 at home to believe that healthcare providers should be dismissed for not reporting to work (Figure 3). The unadjusted odds ratio for this measure was not significant.
Finally, significant unadjusted or adjusted odds ratios were found between the COVID-19-related anxieties and the belief that frontline care should be provided only by those without children at home (Figure 4).
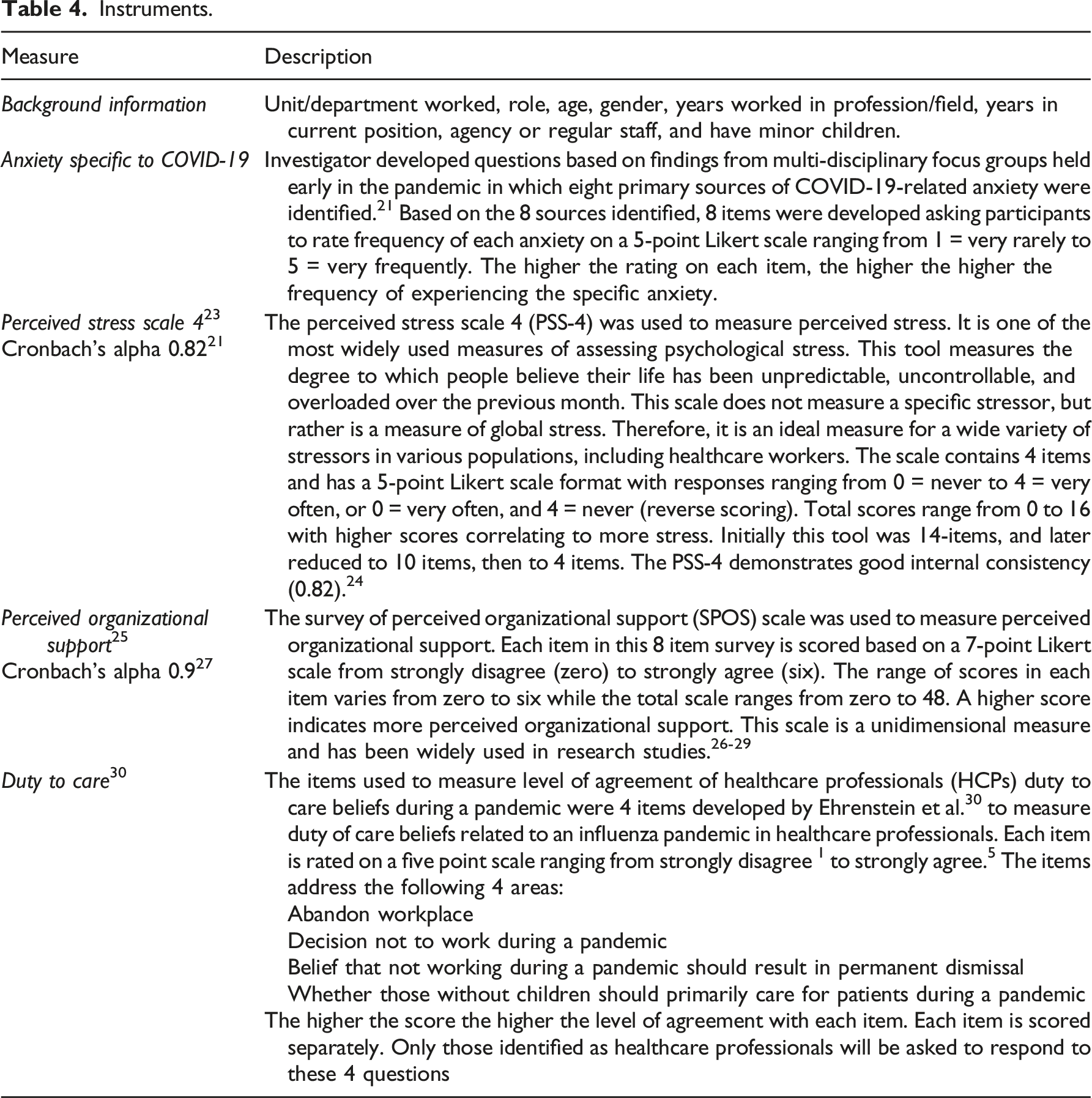
Instruments.
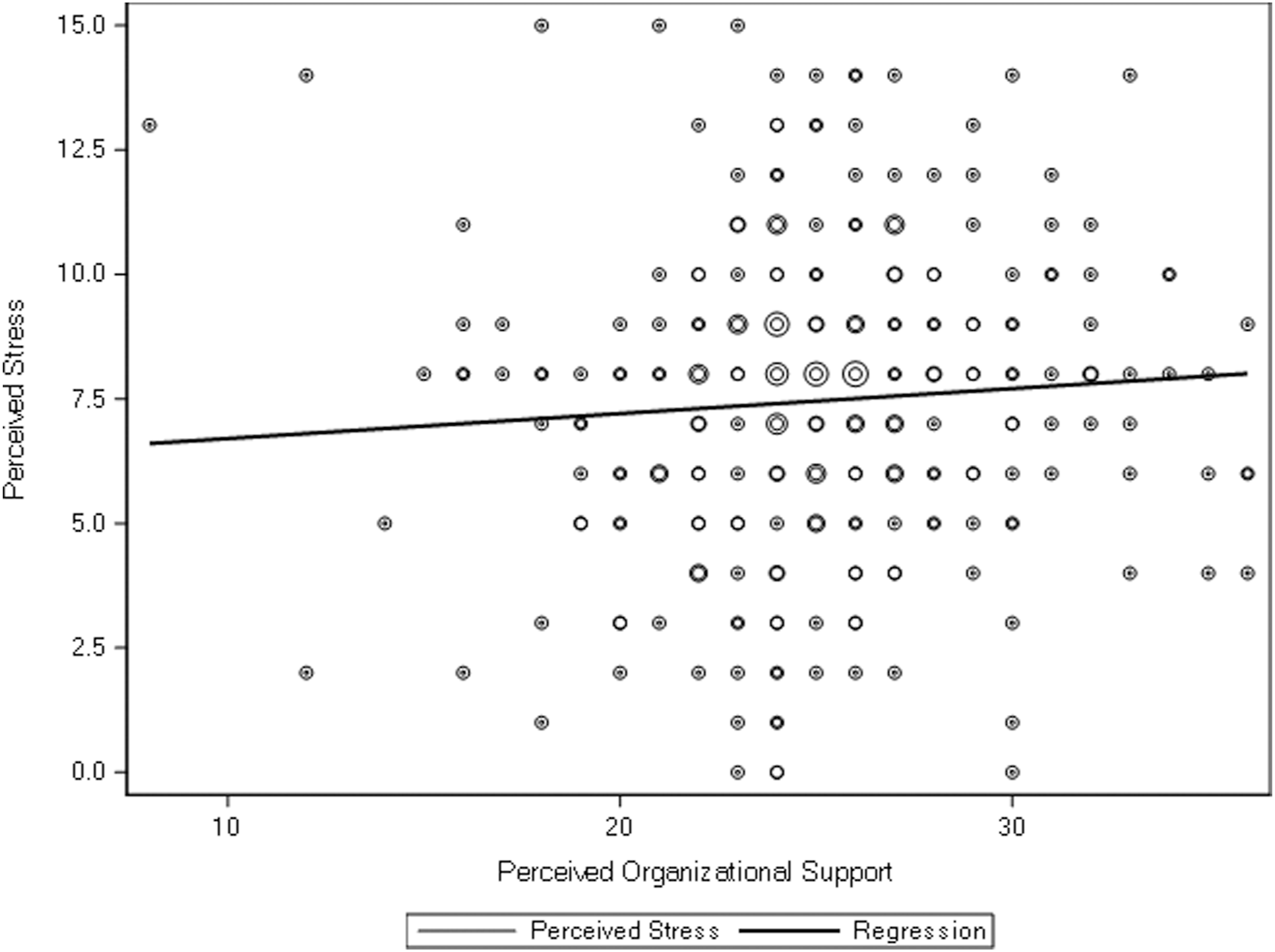
Linear regression analysis of the association between levels of perceived stress and perceived organizational support. Each bubble point represents paired scores of perceptions of stress and level of organizational support. The size of the bubble represents the underlying count of respondents with those paired scores.
Discussion
A public health emergency, particularly one deriving from a communicable illness, can exacerbate the dissonance between nurses’ duty to care and personal responsibilities because of the simultaneous increase in both public need and personal obligations. Early in the COVID-19 pandemic, Shanafelt et al. developed a taxonomy of potential sources of anxieties for HCW. 21 Our survey results confirm the high frequency of anxiety deriving from several issues related to COVID-19 (Table 2). The current study also found high frequency of attitudes that undermine duty to care principles (Table 3).
While stress levels among nurses were high generally, stress levels were not associated with perception of organizational support (Figure 5). In addition to documenting high frequency of anxieties and challenges to duty of care principles, the current study also tested the association between the specific domains of anxiety and ethical concerns affecting the duty to care. The data showed that of the eight domains of anxiety, five were associated with one of the four beliefs that undermine duty to care (Figures 1–4). These domains of anxiety were: feeling competent to provide care in an unfamiliar area; access to childcare during periods of increased work and school closures; anxiety about adequate support for self and family if infected with SARS CoV-2; exposing family at home to infection; and uncertainty about organizational support if infected. Of these five, concern about access to childcare, though not as frequent as other anxieties in the survey, was most strongly associated with erosion of two key duty to care principles: willingness to abandon the workplace and freedom to decide when to work (Figures 1, 2).
These results confirm similar findings from around the world. One previous study found a relationship between adequacy of resources and employee organizational commitment, though duty to care was not specifically measured. 31 In the current study, there was an inverse association between anxiety about access to PPE and belief in duty to care principles. Similar findings were made earlier by Qureshi et al. who found that access to PPE directly influences HCW willingness to report to work during many different types of theoretical emergencies. 7
The types of anxieties demonstrated in our survey were also seen in a study of nurses in Israel. 32 In that study, Sperling used an original tool to survey 231 acute care nurses during the pandemic and found that the issues that most concerned nurses were contracting COVID-19 from work, bringing it home to family members, and certain work conditions, including being forced to care for COVID-19 patients without adequate training and PPE. These domains of concern were also highlighted in the current study which demonstrated that they were associated with an erosion of duty to care principles.
Finally, a survey of 550 frontline hospital workers in multiple disciplines in Palestine found that 25% of survey respondents were not willing to work during a pandemic, though physicians and nurses expressed this feeling less often than other healthcare workers. 33 Those with more longevity and lower stress levels were less likely to consider abandoning the workplace. Healthcare workers felt poorly prepared for COVID-19 care, unappreciated, and frustrated by unfair work distribution.
The relationship between global stress and perceived organizational support was also evaluated. Unexpectedly, we found no statistically significant association (Figure 5), possibly due to lack of organizational support being only one of many sources of COVID-19-related stress. Overall stress levels are not affected by any single anxiety source, but rather represent an amalgam of perceptions.
Similarly, a Canadian study that found personal sources of stress, especially childcare and eldercare responsibilities, were the most impactful on the psychological wellbeing of HCW during the COVID-19 pandemic, 34 supporting the idea that organizational support specific to child and/or family care may be important in mitigating overall stress.
Increased stress emerging from COVID-19-related anxieties affected by perceptions of organizational support proved influential in nurses’ attempts to resolve the ethical dilemma intrinsic to the duty to care. Our data revealed that nurses who were frequently anxious about personal needs were more likely to believe that healthcare workers should be allowed to decide whether or not to report to work. In a worst-case scenario, this confluence of anxieties could lead to nurses abandoning the workplace on a wide scale, leaving hospitals ill-equipped to adequately provide the standard of care to all patients seeking acute care during a surge of COVID-19 patients. There is evidence that this has already occurred on a problematic scale. In future emergency responses, particularly those involving contagious diseases, organizations should address the specific impactful anxieties we have identified while simultaneously seeking out new resources appropriate for the next PHE. Though the circumstances of the next PHE may change, the general taxonomy of concerns will be similar: workplace safety; adequate training for unfamiliar clinical placements; personal and family safety; and adequate access to resources such as PPE.
Study Limitations
This study has several limitations including that it was conducted at a single acute care hospital at a single point in time. No statement can be made about longitudinal trends. The study was conducted over a short period of time early in the pandemic when there was more uncertainty about risks of contagion and less access to PPE. It is possible that conditions during that time influenced the outcome of our research.
Study participation was voluntary and therefore may demonstrate a response bias toward interest in the topic. The survey was only sent to those currently working; those who had already left the workforce because of COVID-19-related issues did not participate.
Finally, while the study did evaluate the impact of caring for minor children, it did not query the impact of caring for elderly parents or other high risk individuals living in the home.
Despite these limitations, the study is important because of the large size of a homogeneous population of healthcare workers, namely, nurses with direct COVID-19 care responsibility. Moreover, it explores some areas not previously addressed, including the relationship between specific COVID-19 anxieties and duty to care, and the relationship between perceptions of organizational support and global stress.
Conclusion and Recommendations
While the COVID-19 crisis has become the worst global pandemic in over one hundred years, it likely will not be the last public health crisis of its kind in this century. Indeed, infectious disease experts cite increased globalization, deforestation, loss of animal habitat, and climate change as among some of the factors likely to contribute to future pandemics. 35 Thus, it is imperative that nations and healthcare organizations learn how to address the concerns of an essential nursing workforce in order to ensure availability.
While previous studies suggested accounting for psychological stresses in planning organizational responses, they did not offer specific recommendations for response or preventative measures that may mitigate a nurse’s ethical dilemma.30, 31 Based upon our findings that anxieties around access to childcare, the availability of PPE, confidence in providing competent care when redeployed to new clinical areas, and uncertainty about the organization’s commitment to care for the nurse and/or nurse’s family in the event of infection may undermine duty to care, it is incumbent upon healthcare systems to find ways to mitigate these particular concerns in a subsequent infectious PHE. One possible way of reducing the anxiety associated with redeployment is to proactively cross train HCW in anticipation of emergencies. While costly, failure to prepare will result in similar problems in the next PHE.
Similarly, mitigation steps to ease anxiety around family care might include cultivating relationships with local trained day care providers or using re-purposed campus space for ad hoc arrangements. Emergency declarations by government authorities, such as easing license expirations or telemedicine protocols, could reduce the regulatory burdens of implementing such strategies. To help nurses offset competing family care obligations, hospitals might collaborate with childcare centers, nanny-share programs, and community health workers for family/elder check-in visits. Such arrangements are more problematic during a contagious PHE, but some of the health system’s own employees could be made available for these tasks.
Nurses’ concerns about deficits in organizational support should they become sick might be addressed with extension of typical sick leave time. Other efforts to attend to the personal needs of nurses during the pandemic might include providing food donations and a sundry store on site. Such efforts demonstrate a culture of caring and strengthen the bond between employer and employee.
Anxieties about bringing the infection home to family could be addressed by providing redeployed onsite dressing room so nurses (and others) can change out of work clothes before going home (a particular concern early in the pandemic). With the more widespread availability of testing, hospitals could offer frequent and free infection testing for those with particular worries about vulnerable family members, an issue which remains relevant despite widespread availability of vaccination.
While access to up-to-date and clear communication about the pandemic was a source of anxiety, it did not emerge as a significant finding related to duty to care in the current study. Nevertheless a commitment to do this in a transparent and frequent way should be upheld as a way of building trust. Information delivery should include access to local and trusted experts in infectious diseases and epidemiology who are known to the nursing staff.
Recommendations to mitigate effects of COVID-19 and future pandemics on duty to care among nurses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute of Environmental Health Sciences Grants R01ES027815, R01ES030743, and R21ES032161.