
Abstract
Background
Recently, palliative care is increasingly important, with an emphasis on the process of dying with dignity. However, nurses who care for such patients experience the associated ethical dilemmas.
Objective
To explore the meaning of nurses’ experiences in dealing with ethical dilemmas in relation to palliative sedation.
Research design
A qualitative research design was employed with a thematic analysis approach.
Participants and research context
Using purposive sampling, 15 nurses, working at palliative care units for at least 1 year, were recruited as participants. Data were collected using unstructured in-depth interviews, and data collection and analysis was performed simultaneously.
Ethical considerations
Ethical approval was obtained from the authors’ institutional review board. All participants provided informed consent. For the face-to-face interview, the South Korean standard COVID-19 quarantine guidelines, such as mandatory masking and social distancing, were followed.
Results
Dilemmas raised by patients, were related to concerns about appropriate drug dose; dilemmas raised by nurses, were related to passive care, sense of guilt for failure to predict death, and colleague’s disrespectful attitudes toward patients; dilemmas from patients’ families were related to demands for palliative sedation and reversal of those demands. Care actions to deal with ethical dilemmas comprised evidence-based care, person-centered thinking, reflecting on the death situation, compassion, providing explanation and help to family members.
Conclusion
Nurses’ ethical dilemmas were pre-dominantly influenced by themselves, rather than by the patients or their families, especially if they felt they could not do their best for patients. The core concept of care actions to deal with the ethical dilemmas, was person-centered care and compassion. Then, how patients and their family members perceive person-centered care and compassion, should be further explored to improve palliative sedation.
Introduction
The South Korean population is increasingly aging, with 14.2% of the population’s age being 65 years and older in 2017. The increase in the number of older adults has changed society’s view of death, with as much importance attached to death as the process of living. Dying with dignity has been highlighted as a condition of human life 1 ; therefore, national government of South Korea prepared the Life-sustaining Medical Decision Law in 2018, for terminally ill patients close to death, to facilitate the achievement of death with dignity. Although palliative care is increasingly important nowadays, considerable disparity and inequality exists in the supply and use of palliative care. 2
Palliative care is based on the biopsychosocial-spiritual model of care. 3 Palliative sedation is a medical practice in which deep sedation is induced to alleviate terminal refractory symptoms in terminally ill patients close to death, and continues until demise.4,5 Although there is a concern that palliative sedation may advance the death of terminally ill patients, palliative sedation is reported to be ethically correct, 6 because it is conducted during the dying process in the last days or hours of life, and it does not advance death nor have any detrimental effect on life. 7 According to the guidelines in South Korea, 8 only patients with terminal cancer can be admitted to palliative care units. Therefore, this study specifically focused on patients with terminal cancer. In previous studies on palliative sedation conducted for terminally ill patients, it was performed in 14.0–33.6% of cases, mainly to control symptoms of delirium, pain, and dyspnea, with the average time until death being 24–72 h.9–12
Palliative care nurses face ethical dilemmas. These originate from conflicts between values, norms, and interests. 13 Ethical dilemmas for clinical nurses entail the conflicts from personal and professional values, the nurses’ ability to provide high-quality and compassionate care. 14 These dilemmas among palliative care nurses, occur because they administer sedatives to terminally ill patients with refractory symptoms, observe them, and stay with them for greater lengths of time. 15 Such dilemmas are related to the decision to use sedatives, depth of sedative administration, likelihood of shortening the patient’s life, and loss of social interactions. 16 They further occur when the patient’s family demands an increase of the sedation level for the patient.17,18
Nurses were able to alleviate their ethical dilemmas when they provided care that helped patients experience a peaceful death, 19 or when they received support from colleagues and supervisors. 16 However, in most of the studies conducted on the experiences of nurses who care for palliative sedation patients,16,18–20 they had serious burdens or ethical difficulties with palliative sedation, and sometimes had conflicting thoughts that it was not the most beneficial step for the patients. Few studies have focused on nurses’ practices, attitudes toward, and experiences in palliative sedation nursing care.16,19 Furthermore, no study has investigated how nurses who experience ethical dilemmas, deal with such problems.
Therefore, this study explored the significance of the experiences of nurses in dealing with their ethical dilemmas in relation to palliative sedation, and to present basic data for improving the quality of palliative sedation nursing care.
Methods
Research design
This was a qualitative study with a thematic analysis approach to understand how nurses, who care for terminal cancer patients receiving palliative sedation, deal with their ethical dilemmas.
Participants
To obtain prior permission, the first author explained the study to the nurse managers of four university hospitals and general hospitals from the institutions specializing in residential hospice, respectively, as published on the Web site of the Central Hospice Center in South Korea. The researcher asked them to introduce nurses who had experience in caring for patients with palliative sedation. Despite the selection bias, purposive sampling was used to recruit the participants and elicit relevant data. 21
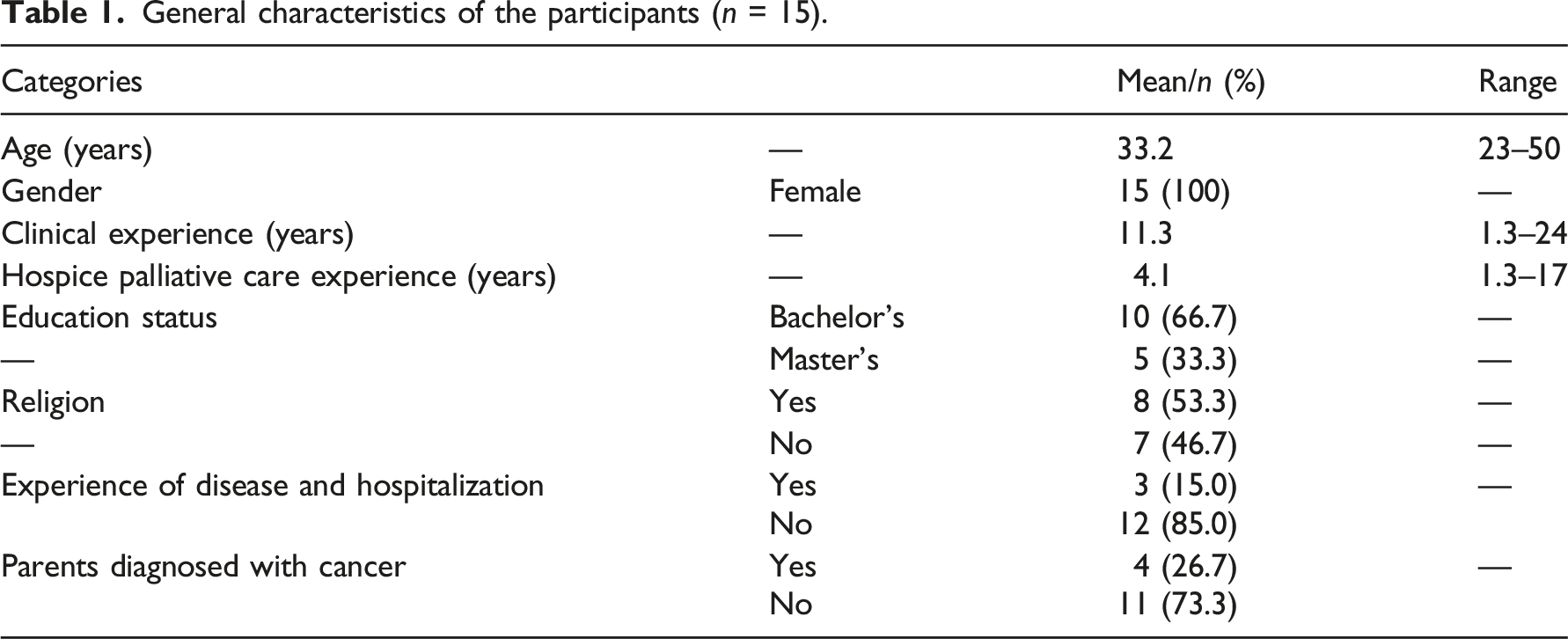
General characteristics of the participants (n = 15).
Data collection and ethical consideration
Data were collected through unstructured in-depth interviews, between May 17 and 11 July 2021, after ethical approval from the authors’ institutional review board. The participants gave informed consent after they were assured of their right to withdraw at any time, anonymity, and interview being recorded. For the face-to-face interview, the South Korean standard COVID-19 quarantine guidelines, such as mandatory masking and social distancing were followed. Considering the convenience of participants, the interviews were conducted in a conference room or rest zone. The first author, who has experience in qualitative studies, conducted the interviews. The interviews began with an open, unstructured question: “What do you think about performing palliative sedation for patients with terminal cancer?” The interviews lasted an average of 60 min. The second set of interviews were conducted with five participants, and additional questions, such as “Can you explain more concretely?” were asked to clarify or supplement the participants’ responses. The interviews ended at the 20th interview, when the participant’s narration was repetitive, and no novel themes appeared. For the duration of the interviews, the participants’ facial expressions, tones, and behaviors were documented, and the researcher’s thoughts were noted in line with keywords in field notes. All interviews were recorded and then transcribed verbatim.
Data analysis
The data were analyzed using thematic analysis.22,23 First, we read the transcribed contents of the interviews several times to become familiarized with the data. To enhance reliability of coding, both the first and second authors analyzed the data. Subsequently, we generated codes and used tables to sort the different codes and organize them into potential themes. We reviewed and refined potential themes, while ensuring that a clear distinction existed between them, and further named them by identifying the essence of each theme. Finally, we comprehensively described each theme in relation to the experiences of nurses caring for patients with terminal cancer with palliative sedation, and identified the essential structure of the research topic (Figure 1). Ethical dilemmas and care actions in nurses providing palliative sedation.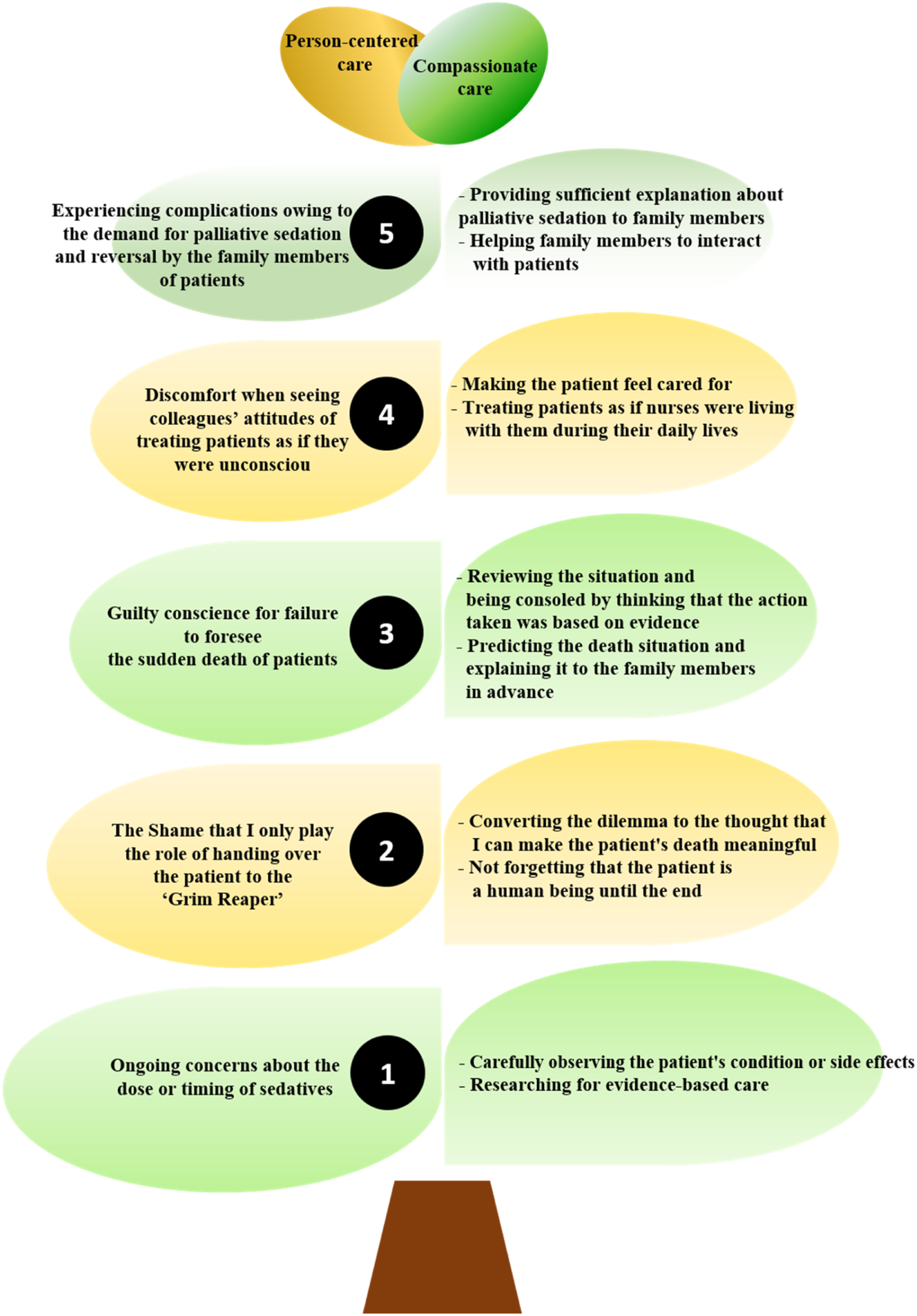
The study rigor was achieved by establishing credibility, transferability, dependability, and confirmability 24 through strategies, such as member checking, peer debriefing, audit trail, and checking the researchers’ bias and prejudice.
Results
Specifically, five themes focusing on the ethical dilemmas experienced by participants caring for palliatively sedated patients, and 10 unique themes focused on the care actions the participants took and how they addressed the dilemmas, were comprehensively examined.
Ethical dilemma 1: Ongoing concerns about the dose or timing of sedatives
While monitoring the effectiveness of palliative sedation, the participants checked the patients’ respiration and oxygen saturation when they were not adequately sedated, and constantly discussed with fellow nurses and the doctor when to adjust the dose.
Whether the dose of the drug is appropriate, whether the dose of the drug was too high from the beginning, whether this dose is appropriate when the sleeping is prolonged… I think these should be considered. (Participant 7)
Care action 1: Carefully observing the patient’s condition or side effects
While slowly tapering the dose of the sedatives, the participants were relieved when the patient’s dyspnea or pain symptoms decreased, but they closely observed the changes in secretions, respiration patterns, and excretion volumes, and ensured the patients’ personal hygiene in case of sweating and wetting of clothes. Regarding infrequent and rare side effects, the participants referred to articles related to palliative sedation nursing care.
When midazolam is continuously administered, the patient’s clothes are often wet every day, Therefore, I greatly care about personal hygiene. (Participant 6)
Care action 2: Researching for evidence-based care
When patients died earlier than expected after sedation, case studies were conducted in the ward to determine the cause. When the cause was identified, the accumulated evidence was preserved appropriately, to be utilized for similar situations. The participants researched articles or websites on palliative sedation and ascertained the justification for their care direction.
When a patient who was on low-dose midazolam died earlier, we figured out what was the cause, and a case study was conducted in our ward. I checked while agonizing what should be considered if a similar case occurs later. (Participant 1)
Ethical dilemma 2: The shame felt that the nurses only play the role of handing over the patient to the ‘Grim Reaper’
The participants reported that the average time until death of patients who started palliative sedation was 2–3 days, but the time until death could be lengthened up to 14 days, unintentionally. When caring for the patients sleeping for more extended periods, the participants were distressed, and compared the care to expressions, such as “handing over to the Grim Reaper.” This demonstrated that the participants experienced shame for not giving meaning to their care for patients or caring for them with a passive attitude.
There were times when I thought that I was handing over the patient to the Grim Reaper on the express train to death. I was distressed when I thought this way because I did not actively care for the patient… (Participant 5) Care action 1: Converting the dilemma to the thought that I can make the patient’s death meaningful
Although the time required for the patients to take a deep sleep was prolonged, the participants realized that their care for such patients was not meaningless and focused on giving meaning to their care. Participants who followed a religion had respect for the patients who had endured their difficult journey and emphasized that sharing the last journey through care could make the death of the patients meaningful.
At that time, I did not think that our talking to the guardians and providing religious care were part of nursing. When I felt, “These actions that I did were not meaningless. If I do this well, the thought of the guardians will change, and the patient can die well;” the thought (that my care was meaningless) seemed to have disappeared. (Participant 7)
Care action 2: Not forgetting that the patient is a human being
Treating the patient as a human being throughout the duration of care, meant trying to provide the patient a sense of stability, by meeting them, letting them hear the voices of their family members, and playing their favorite music. One participant reported that she does not forget that she is the last nurse of the patient, and cares for the patient so that they feel dignified, to the fullest extent.
I should pay more attention to this patient as he cannot express what he wants… I care for patients thinking that I should keep their dignity in the best possible way as I am the last medical worker for the patients. (Participant 15)
Ethical dilemma 3: Guilty conscience for failure to foresee the sudden death of patients
Most of the participants experienced the most difficult time of self-reproach when a patient had died in a situation where the death was unforeseen. They felt guilt, pertaining to their judgment to administer the sedative, which might have been wrong.
One day, the patient frowned severely… He was grimacing severely in an unconscious state, so I used the as necessary (PRN) painkiller, and when I went back to him 30 min later, I found him dead. Did I indeed judge this patient well to give the drug? (Participant 3)
Care action 1: Reviewing the situation and being consoled by thinking that the action taken was based on evidence
When a patient died suddenly, the participants surveyed the situation and evaluated whether any details were missed. They consoled themselves by concluding that they would make the same decision when a similar situation occurs in the future.
I looked back on the situation. ‘I took the patient’s respiration rate, and it was in the normal range.’ I looked back on details to see if there was anything I did wrong in the process. I thought whether I would give the injection or not if the same situation would occur later… and I felt that I would give the injection. (Participant 12)
Care action 2: Predicting the death situation and explaining it to the family members in advance
The participants emphasized that death should be predicted if possible, and the prediction should be explained to the family members in advance. They suggested that when administering sedatives to patients with excessive secretions in the airways, it is necessary to explain to the family members that breathing may be suppressed before administration.
Ethical dilemma 4: Discomfort when seeing colleagues’ attitudes of treating patients as if they were unconscious
The participants felt ethical discomfort when a fellow nurse showed an attitude which arose from a low level of ethical competence, such as a disrespectful attitude toward the patient, treating the patient without speaking to them, or only providing necessary treatment.
They think that the patient would not be able to hear because he is unconscious and speak ‘What should I say? Without dignity?’ I think we should not omit the procedure of speaking and explaining to patients. (Participant 4)
Care action 1: Making the patient feel cared for
The participants who had experience of disease and hospitalization themselves or their parents, argued that nurses should provide palliative sedation care with sincerity, by putting themselves in the patient’s shoes and thinking from their perspective, such as “If I were lying down, what would I want?” and “Is this what the patient really wants?” The participants made efforts to make the patients know that they were there to care for them.
Care action 2: Treating patients as if nurses were living with them during their daily lives
The participants reported that they should be able to express their feelings about patients, understanding that patients hear what they say; when they change patients’ posture, they say “I will change here.” They should care for patients with an utmost concern, assuming they were living their daily life with them.
Ethical dilemma 5: Experiencing complications owing to the demand for palliative sedation and reversal by the family members of patients
Family members request palliative sedation when the patient’s behaviors make them exhausted, or when they cannot stay next to the patient. Otherwise, they request medication be stopped after seeing the patient has an unstable orientation. The participants experienced difficulties in adhering to this decision because they were able to understand the family members’ position.
There are cases where even when the nurse explains, the family members say that what they wanted was not sleeping as such and they want to make eye contact, and so the dose should be reduced. (Participant 8)
Care action 1: Providing sufficient explanation about palliative sedation to family members
The participants reported that they sometimes should check whether sufficient consent for drug use has been obtained from the family members, and should continuously provide sufficient explanations to ensure that the family members correctly understand palliative sedation.
Care action 2: Helping family members to interact with patients
When family members wished for the patient to be awake as they intended to spend some meaningful time with them, the participants gave guidance to the family members about the care they can provide when the patient is sedated, and helped the family members to interact with the sedated patient, by mentioning the appropriate time.
Trying together to find out what to do at this point… In the case of family members who clean the patient’s body when the patient is not yet sedated… telling the appropriate time to do that. (Participant 10)
Discussion
This study explored the ethical dilemmas experienced by nurses providing palliative sedation, and identified their care actions to deal with these dilemmas. Ethical dilemmas caused by the nurses themselves or fellow nurses, were more pronounced than those caused by patients or their family members. This indicates differences in ethical competence among nurses. Further, it demonstrates that South Korean nurses, who provide palliative sedation, engage in reflecting, sharing, and learning about the new dilemmas. The nurses’ care actions and reflective attitudes toward ethical dilemmas are an essential element of person-centered and compassionate care, which is the core concept of dealing with ethical dilemmas, like the leaves and stems of the care tree, as shown in Figure 1. In this study, person-centered care indicates that nurses provide holistic care at the physical, psychological, social, and spiritual level of the patient; compassionate care indicates that nurses provide nursing care, based on understanding and thinking of themselves in the patients’ position.
The nurses were always concerned about the appropriate dosage of sedatives. The depth of palliative sedation should be such that the level thereof should be the lowest level necessary to provide adequate relief from pain. 4 They exchanged opinions with fellow nurses on the patients’ sleep patterns and changes in vital signs. Additionally, the nurses in this study showed the will to identify and improve palliative sedation-related issues by referring to related studies, thereby formulating evidence for improving palliative sedation nursing care.
Although the nurses experienced shame at times, owing to the role they undertook with dying patients, they reflected on it by giving meaning to the dignity and death of humans. According to the previous studies, patients being close to death is an essential element in determining palliative sedation.15,18 Therefore, providing compassionate care to patients during the prolonged dying period is complicated. In general, healthcare providers have doubts about their abilities, because they do not know whether care is appropriate in a state where communication with palliative sedation patients is impossible. 25 This is similar to the nurses’ reflective attitudes displayed in this study. Providing care to preserve the dignity of humans requires an effort of inducing a sense of worthiness for patients with cancer, who need palliative care, 26 with the nurses suggesting that this type of care should be kept in mind and retained throughout the duration of care. Additionally, dignity was emphasized in terms of holistic perspectives, 27 suggesting that it is an important characteristic in providing high-quality palliative care. However, the nurses in this study did not present a spiritual approach in person-centered care, suggesting the need for further research on spiritual care among nurses providing palliative sedation.
Although the nurses experienced guilt for their failure to foresee the sudden deaths of patients, they consoled themselves by believing that they did their best. In addition to continuous sedation, the nurses may inject PRN sedatives when necessary. However, there is inherent uncertainty in the prognosis of palliative sedation patients. 6 Nurses relied on personal experiences and justified palliative sedation with the view that it relieved unbearable pain and that sudden, unpredictable death was an unintended side effect, thereby emphasizing the necessity to relieve the nurses’ sense of guilt. 19 This can be understood in relation to a previous study that had documented difficulties of comfort assessment on palliative sedation patients. 28
Whenever the nurses felt uncomfortable with the attitude of colleagues who did not respect the patient, they suggested that nurses should consider what they would need if they were in the patient’s position and that they should treat patients as if they lived their daily lives with them. In dealing with ethical dilemmas, the nurses reported their person-centered beliefs and feelings in consideration of patients’ perspectives. It indicates that the attitudes of nurses toward patients stem from differences in ethical competence for the protection of the patient’s dignity and rights. Also, nurses who experienced cancer treatment or the death of a family member, understood and sympathized more when caring for a patient facing death,29,30 but this is not a self-centered thought; instead, it stems from a deep understanding of and compassion for patients. Compassion is considered a cornerstone of high-quality palliative care. 31 In previous studies, empathy was mainly emphasized in the concept of compassion, by describing empathy as a facilitator for compassion, 32 or the first step of performing compassion. 3 Compared with the previous study, this study showed a similar finding, as thinking about oneself in the patients’ position was emphasized in the concept of compassion.
Although the nurses had ethical dilemmas, owing to the demand for palliative sedation and reversal thereof by the family members of patients who were in agony, the nurses connected the family members to the patients, to facilitate their interaction with the patients who were in deep sleep. The same context was reported in a study indicating that family members feel pain when they cannot interact with the patient when sedatives are administered. 33 As nurses administer palliative sedation and have valuable information about the needs and wishes of patients and their family members, 16 they can help family members interact with patients in deep sleep. Unlike the study 34 in which South Korean healthcare workers (doctors, nurses, and medical technicians) recognized death as a phenomenon derived from medical failure, the present study suggests that palliative care nurses understood humans holistically, especially when providing palliative sedation care.
The implications of the findings for nursing practice and research are as follows: First, this study identified that general characteristics of nurses with disease experience and religion emphasized person-centered and compassionate care. Nurses should reflect on the characteristics in a person-centered and compassionate manner. Second, this study highlighted that person-centered thinking, compassion, introspection, evidence-based nursing, meaning-seeking activities, and leading daily life together with patients, are the central attitudes and behaviors of nurses who deal with ethical dilemmas, while caring for palliative sedation patients. Third, this study is meaningful in that the view of life concerning the life and death of nurses themselves, view of dignity in humans, and hospice spirit of nurses, presented a role model for holistic nursing, including emotional and psychological care, as well as physical care for palliative sedation patients and their family members.
Limitations
The participants constituted a homogenous sample, as all of them were nurses working at palliative care wards and were women. However, as female medical experts are expected to show considerable empathy and sympathy (females are considered more sensitive and affectionate than males), 35 gender characteristics should be considered when selecting participants in future studies. Moreover, this study described only nurses’ ethical dilemmas on palliative sedation, owing to the limitation of longtime visiting patients during the COVID-19 pandemic, therefore, it is necessary to include interviews with patients or families for enhancing the validity of data triangulation in the future.
Conclusion
Nurses provide end-of-life care for patients, while being closest to the patients for extended periods of time; therefore, understanding the ethical dilemmas they experience when they deliver palliative sedation care and how they deal with those dilemmas, is crucial to improving the quality of palliative sedation care. The ethical dilemmas of nurses were noticeably affected by the care of nurses who did not do their best for patients, rather than by patients themselves or their family members. The core concept to deal with ethical dilemmas was person-centered and compassionate care. Future studies should investigate what person-centered and compassionate care means from the perspective of patients or their family members, and how they recognize it, thereby approaching the topic from multilateral viewpoints. This would likely improve the quality of palliative sedation care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.