
Abstract
Background
Clinical empathy is an essential part of healthcare, and patient-centered care models require clinical empathy to be established. Despite this, little is known about its measurement in the neonatal scenario.
Research Aim
To measure clinical empathy in health professionals who work with medium and high-risk neonates and build a construct of this empathy.
Research Design
Single-center survey study.
Participants and Research Context
The Jefferson Scale of Empathy for Health Professionals questionnaire was applied to health professionals who work in an intensive care unit and a medium-risk unit, in Brazil. Analysis was done using descriptive statistics and a factor analysis model, to build the construct of empathy. Overall empathy was calculated, and the domains’ punctuations were analyzed and compared to the maximum punctuation possible. The study followed the STROBE checklist.
Ethical Considerations
This study was approved by the Research Ethics Committee of the institution. All participants signed the informed consent form. Participants’ confidentiality and anonymity were protected.
Findings
Median empathy was 117 (IQR 113–124). The domain of Walking in the Patient’s Shoes had lower scores and represented 77.6% of the maximum punctuation possible. The factor analysis included three factors named Understanding, Experiences, and Treatment, and Emotional Relationships, explaining 64.3% of the overall variance. The domain Walking in the Patient’s Shoes was not included in the model.
Conclusions
In this scenario, clinical empathy should improve. There is a need to improve the domain of Walking in the Patient’s Shoes, in this case, the neonate, and provide more empathic care to them.
Introduction
Technological advances have resulted in a reduction in neonatal mortality during the last decades, but the current model of care is still biomedical, instead of biopsychosocial one.1,2 Health professionals who work in neonatal intensive care units (NICU) are frequently faced with barriers to clinical empathy, such as the severity of illness, terminal diseases, advanced technology, and crucial decisions. Also, moral concerns are frequent in intensive care, such as situations involving “too much treatment” or the process of dying, “die peacefully and with dignity,” for example. 3 In this scenario, clinical empathy could help change the model of care offered to neonates into a more holistic one that is patient-centered and respects their mental state, aligned with Healthcare Bioethics, which is based on this empathy. 4
Empathy is an umbrella term that describes how people respond to others’ emotions, needs, and perspectives. It is the glue that connects people in general, as relationships need empathy to be established. In the healthcare scenario, clinical empathy expresses the way health professionals empathize with patients, which comprises a cognitive and an emotional component. 5 It is a multidimensional ability that enables health professionals to understand and be concerned with patients’ feelings. Clinical empathy has ethical functions such as intrinsic moral value, epistemic functions, promotion of human dignity, and patient-centered care. 6 In healthcare, clinical empathy has an important moral role and contributes to marking out the ethics of care. 7 Caring is relational and neonatal care involves the family, health professionals, and the patient who in this context is the neonate.
There is a difficulty in seeing neonates as patients and, even more, in centering the care on them, and we should reflect on this. In the neonatal scenario, care centered on the family has been the practice, and this can create a barrier between health professionals and the patient. Neonates are persons; their suffering is singular, and this should be acknowledged, as well as its ethical consequences. They are vulnerable and worthy of care and have their own experiences as patients. We must emphasize that healthcare relationships are engagements actively constructed,8,9 and patient-centered care models require clinical empathy to be established, to provide quality care.10,11
Clinical empathy can be measured in health professionals by using validated scales. The Jefferson Scale of Empathy for Health Professionals (JSE-HP) is a brief instrument created by researchers at Thomas Jefferson University. It has been recognized as the most frequently used instrument for measuring empathy in healthcare, but it has not been studied in the neonatal care scenario. The higher the score, the higher the empathy. 12 Of concern, clinical empathy can be enhanced by strategies driven toward the healthcare team, such as storytelling, narrative skills, reflective writing, and the Balint method. There is a lack of studies on clinical empathy in Brazil.13,14
Aim
This study aimed to measure clinical empathy in health professionals who work with medium and high-risk neonates and build a construct of this empathy.
Method
This is a survey study, with data collected at one time point between May 15 and September 14, 2023. The scenario was a 6-bed NICU and a 6-bed intermediate neonatal care unit at a public tertiary maternity hospital located in São Paulo, Brazil. The estimated multidisciplinary team has 67 health professionals. Inclusion criteria were all health professionals who work in the NICU who agreed to participate. Exclusion criteria were those who were absent from work during data collection. Sample size estimation was calculated at Raosoft and considered a 50% response distribution, a maximum estimation error of 5%, and a confidence level of 95%, resulting in a minimum of 58 professionals to be included (https://www.raosoft.com/samplesize.html).
A questionnaire was built in REDCap with information about professionals’ characteristics (such as age, gender, specialty, and year of clinical experience) and the JSE-HP (© Thomas Jefferson University, 2001. All rights reserved) with three domains (Perspective-Taking, Compassionate Care, and Walking in Patient’s Shoes) divided into 20 components (variables) in a seven-level Likert scale. The JSE-HP was used in this study by permission from Thomas Jefferson University. REDCap is an international, secure web application for building and managing online surveys and databases. The questionnaire was self-answered by health professionals through a tablet, in person, and during work time. The components of JSE-HP were analyzed according to the recommendations of Thomas Jefferson University. Ten negative components were inverted to be scored (1, 3, 6, 7, 8, 11, 12, 14, 18, and 19), as recommended. The maximum score for each professional was 140.
For the analyses, data was exported to Stata program version 18.0 (Stata Corp, L.C.). Qualitative variables are presented in percentages. Normality was calculated by the Shapiro–Wilk test. Numeric variables are presented as median and interquartile range (IQR). The primary outcome was the JSE-HP score. We observed the domains according to their overall score to detect the lowest and highest ones. Also, we determined the observed domain’s scores and the maximum score possible. The Kruskal–Wallis test compared differences between more than two medians. A secondary outcome was the construct that summarized or explained empathy in this group of professionals. A factor analysis was performed. This is a multivariate method that provides for the reduction of a group of variables into a smaller set of factors that represent the underlying latent structural dimensions. 15 Initially, the correlations between the variables were observed, and correlations with values greater than 0.3 in the matrix were considered adequate, and the others were excluded. Bartlett’s test of sphericity was applied. Subsequently, the Kaiser–Meyer–Olkin (KMO) test was applied to the selected matrix to show the proportion of the common variance and to investigate if factorization was adequate. The extraction of factors was performed using the principal components model to estimate the best combination of variables that explained most of the observed variance. The factors were selected by the latent root criterion (Eigenvalue), keeping those with Eigenvalues greater than 1.0. The rotation of the factors to adjust the loads was performed using the Varimax method. For the construction of the model, parsimony was used. The results are presented in tables and graphs. For all analyses, a p-value of 0.05 was considered.
Ethical considerations
This project was approved by the Research Ethics Committee of the institution, and all participants signed the informed consent form. Participants’ confidentiality and anonymity were protected, and no personal information was exported from REDCap to the Stata data set. This study follows the CROSS checklist for survey studies. 16
Results
Sixty-one professionals were included; 60 (98.3%) were female, and the median age was 34 years (IQR 38–40). Thirteen (21.3%) were nurses, 28 (45.9%) were nurse assistants, 12 (19.7%) were physicians, 8 (13.1%) were physiotherapists, and 22 (36.0%) were post-graduated. Twenty-two (36.0%) worked in the neonatal area ≤ 2 years, 23 (37.7%) between 2 and 10 years, and 16 (26.3%) more than 10 years. The overall median JSE-HP was 117.0 (IQR 113–124). Considering the groups of health professionals, the median JSE-HP for nurse assistants was 115 (IQR 111–118), for nurse professionals it was 117 (IQR 111–121), for physicians it was 121.5 (IQR 114–129.5), and for physiotherapists, it was 124.0 (IQR 117.5–130), with differences among them (p value = .04).
The observation of the scores of each domain revealed that the domain Walking in Patient’s Shoes had the lowest scores and Perspective-Taking, the highest ones (Figure 1). Each variable could punctuate a maximum of 427 points. Observed scores for the three domains of the Jefferson Scale of Empathy-Health Professionals version. Var: variable; Perspective-Taking (variables 20, 17, 16, 15, 13, 10, 9, 5, 4, and 2). Compassionate Care (variables 19, 18, 14, 12, 11, 8, 7, and 1). Walking in Patient’s Shoes (variables 6 and 3).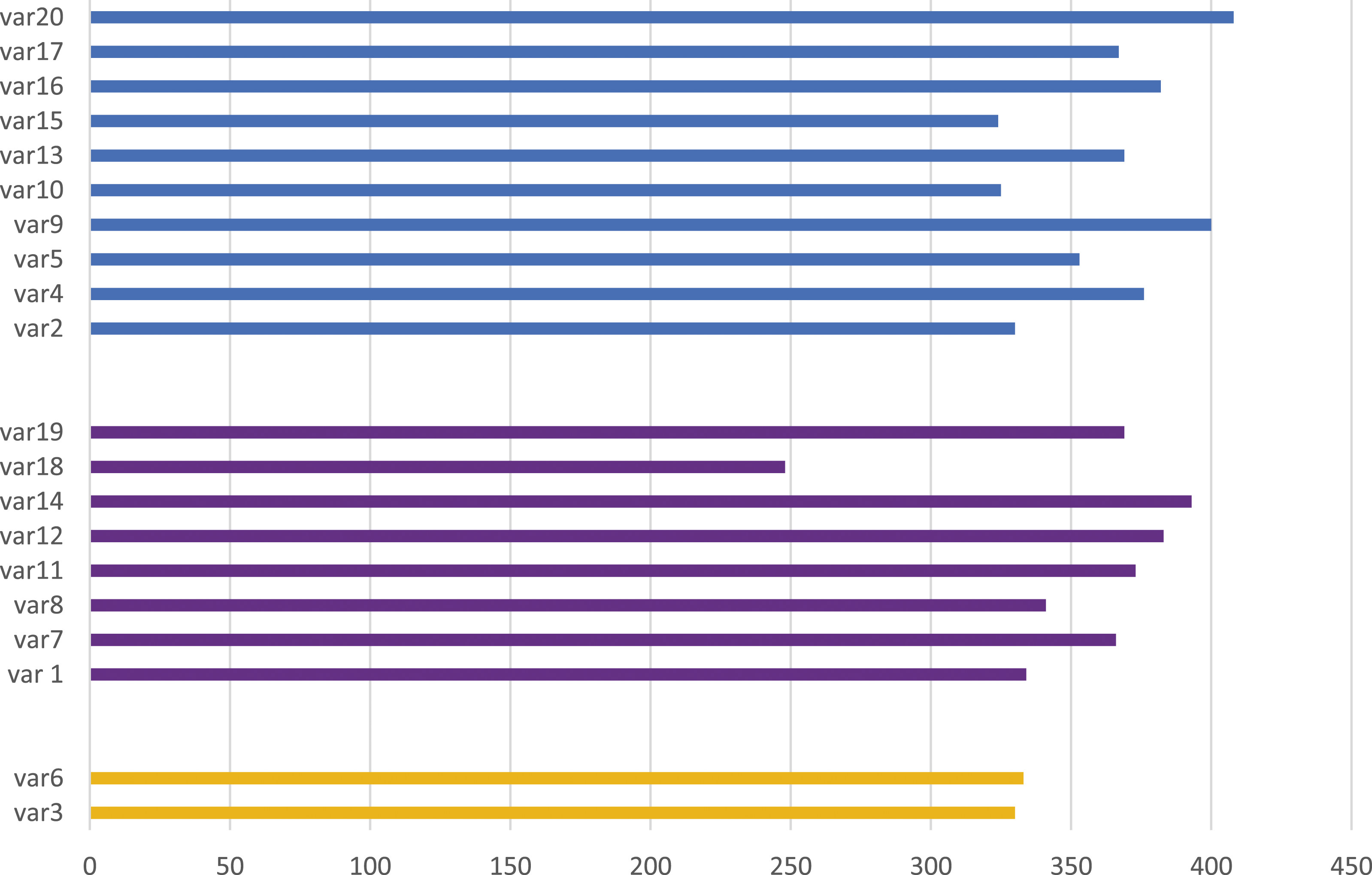
We compared the maximum observed scores to determine the proportion of the maximum score possible (Figure 1). The Perspective-Taking domain observed score was 3634 (85.1% of the maximum). Compassionate Care was 2807 (82.2% of the maximum) and Walking in Patient’s Shoes was 663 (77.6% of the maximum).
Nine variables were included in the factor analysis: 4. I consider understanding my patients’ body language as important as verbal communication in physician-patient relationships 8. Attentiveness to my patients’ personal experiences is irrelevant to treatment effectiveness 10. My understanding of my patients’ feelings gives them a sense of validation that is therapeutic in its own right 11. Patients’ illnesses can be cured only by medical treatment; therefore, affectionate ties to my patients cannot have a significant place in this endeavor 13. I try to understand what is going on in my patients’ minds by paying attention to their non-verbal cues and body language 15. Empathy is a therapeutic skill, without which my success as a physician would be limited 16. An important component of the relationship with my patients is my understanding of the emotional status of the patients and their families 18. I do not allow myself to be touched by intense emotional relationships between my patients and their family members 20. I believe that empathy is an important therapeutic factor in medical treatment
The correlation matrix was inspected and generated a moderate KMO test (0.70). Bartlett’s test of sphericity (approximate χ2 139.03; p < .001) indicated that the correlational matrix was not an identity matrix, which was followed by a factor analysis.
The analysis of Eigenvalues suggested the existence of three main factors, which can be confirmed by the Scree graph (Figure 2). Screen graph of Eigenvalues.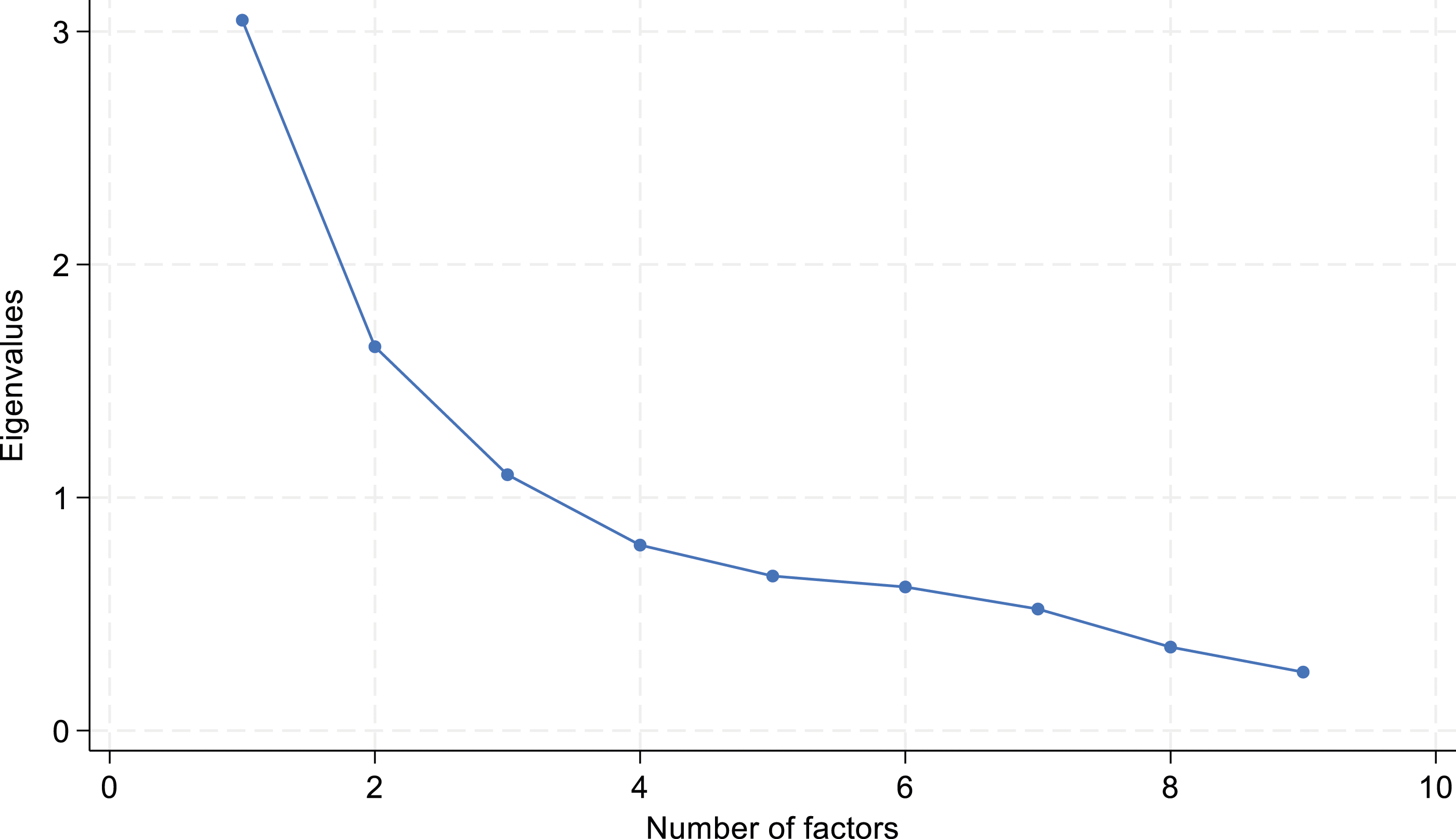
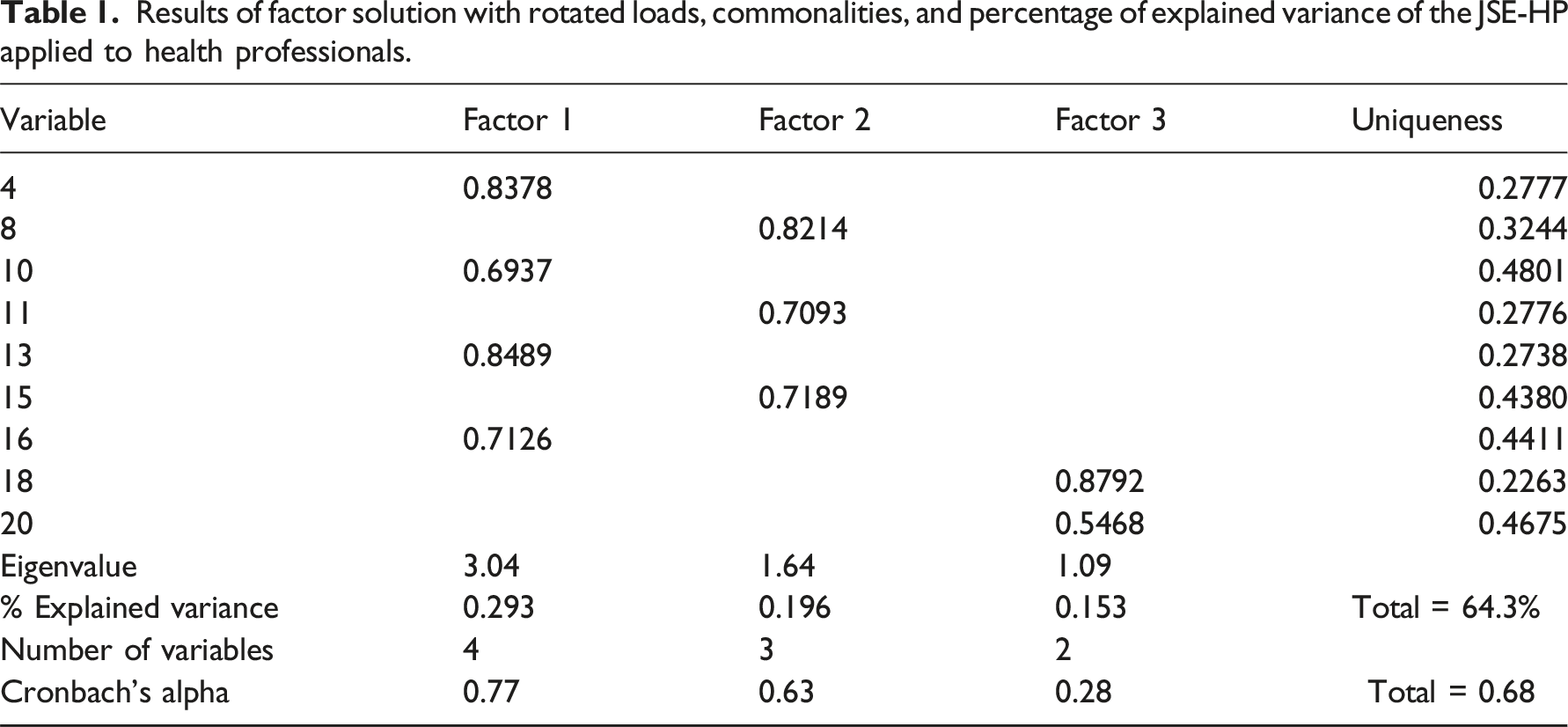
The factor analysis model identified three factors that were named, considering the factor loadings obtained. Thus, Factor 1 refers to Understanding, Factor 2 refers to Experiences and Treatment and Factor 3 refers to Emotional Relationships (Figure 3). The resulting factor analysis model for the JSE-HP applied to health professionals who work in medium and high-risk neonatal care.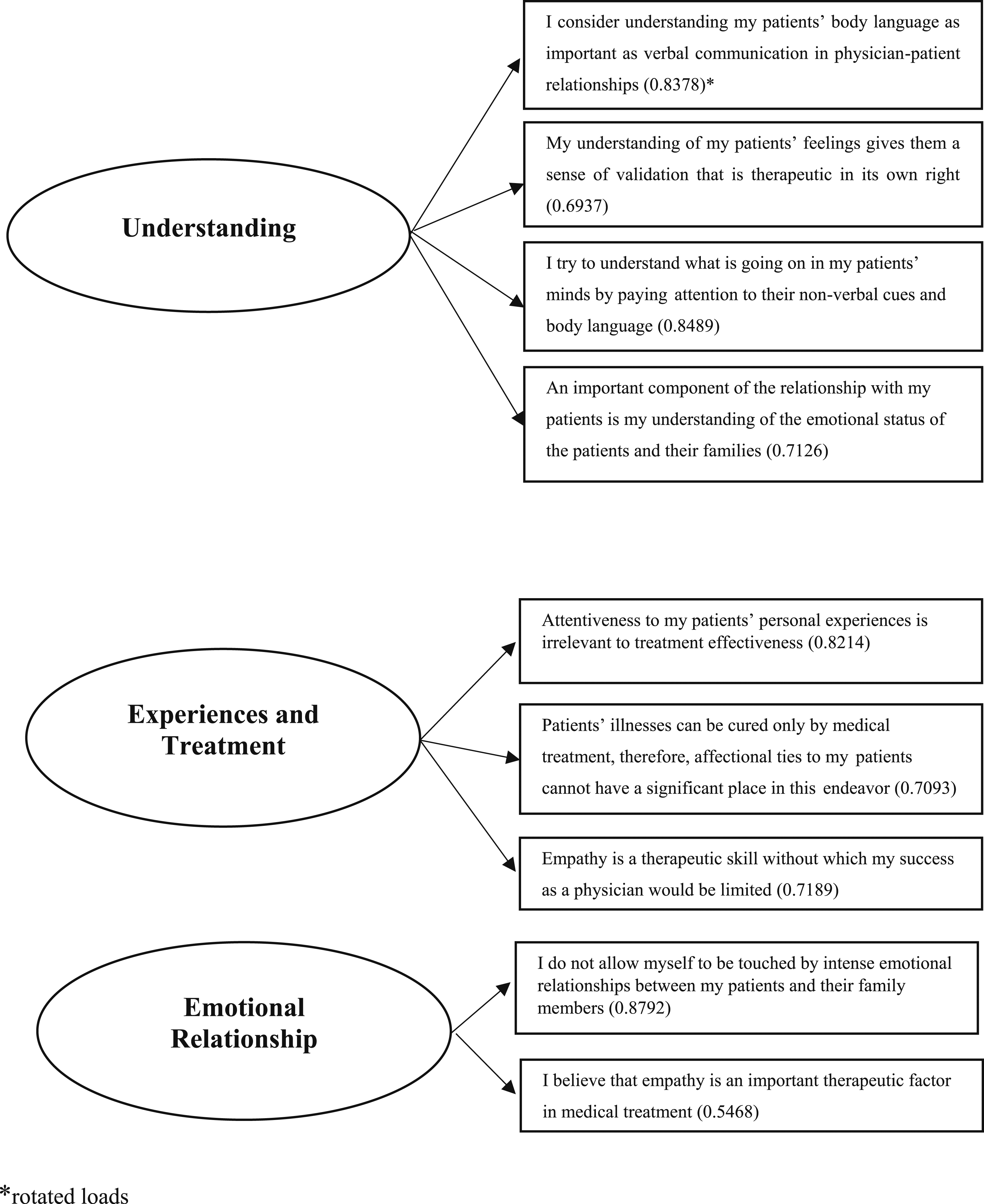
Results of factor solution with rotated loads, commonalities, and percentage of explained variance of the JSE-HP applied to health professionals.
Discussion
In this study, we analyzed healthcare professionals who work with medium and high-risk neonates. Median empathy was 117. The domains’ scores obtained that reached the highest punctuations were Perspective-Taking, Compassionate Care, and Walking in the Patient’s Shoes, in order. The construct of empathy was represented by three factors, which included variables from the domains of Perspective-Taking and Compassionate Care.
The Cronbach’s alpha observed in the present study was 0.68, reflecting moderate reliability. 17 As we were not validating a questionnaire, we were applying an already validated one to determine a construct, we do not think this influenced our results.
The median empathy score was 117. We did not find studies that have measured empathy in healthcare professionals who work in neonatal care, to make comparisons. Chaitoff et al. included adults with diabetes and observed a mean JSE of 118.4, higher than the score observed in the present study. 18 Hojat et al., in a study that included adults with diabetes, observed a higher mean score, and according to the distribution of the observed JSE scale, they suggested for statistical analyses two cutoffs, 117 and 128, classifying empathy as low, moderate, or high. 19 Of concern, we must emphasize that neonates are vulnerable and do not communicate verbally, but they perceive everything that reaches them. 20 This particularity may influence clinical empathy in this scenario. If we compare our results with these two studies, we will conclude that the observed empathy score was on the limit to a low score, revealing an opportunity for empathy improvement in the neonatal unit, and some strategies could help this. 13
The domain that reached the highest score, considering the maximum score possible, was Perspective-Taking. This domain is considered the cognitive arm of empathy, and this result suggests that health professionals can understand the neonate’s suffering. The objectivity implicit in this result agrees with the results of the validation of JSE-HP when the cognitive domain was more important than the others. 12 According to Hojat et al., cognitive empathy in abundance in patient care is always beneficial and can lead to strong trusting relationships, more accurate diagnosis, greater compliance, and better healthcare outcomes. 13 We did not find other studies that have described the JSE-HP by each domain in the neonatal scenario, to make comparisons.
The construct of empathy was composed of variables from the domains of Perspective-Taking and Compassionate Care. Three factors were included in the model: Understanding, Experiences and Treatment, and Emotional Relationships. The model did not include variables from the domain Walking in Patient’s Shoes, in this case, Walking in Neonate’s Shoes. This domain is composed of two variables and is the smallest one in JSE-HP. It is part of affective empathy, reflecting the ability to experience the same emotion as another. 21 Studies have suggested that affective empathy can be influenced by acute stress, in a context-dependent manner, and this can block the contagion of others’ emotions and thus implicate in the ability to care for others. 22 Considering that we explored the NICU and medium-risk neonatal care scenarios, which are very stressful wards and where moral obligations and work responsibilities are balanced all the time, 3 this result reflects the difficulty for healthcare professionals to view things from the neonate’s experience and perspective, and this should change. For a long time, neonates were considered receptors, taken by the other’s stimuli, constituted from the outside to the inner side. Differently, they build their perceptions, decoding the world in which they live. 23 According to Trevarthen et al., neonates build their senses and interact with other people, and that’s what enables them to engage in human society. 24 Neonatal care is unique. Historically, the center of care has evolved to a family-centered one, and although this has improved the health and safety of neonates in the healthcare scenario, this does not guarantee that neonates are seen as patients and that their best interests will be protected. More recently, it has been suggested that families be seen as essential team members, and this should raise the question of where the patient is. 25 This was an evolution, but we need to advance. It is an ethical imperative that health professionals respect the neonate’s particularities and mental states, which does not exclude the family from the care and does not minimize the family’s importance, but instead, acknowledges the neonate as a person. By doing so, the neonatal units can implement strategies to improve clinical empathy, such as storytelling, simulation methods, and techniques that evoke emotional experiences.26,27 These strategies should be considered for the neonatal unit investigated.
This study has limitations. The single-center study design impairs generalizations. Because the scenario is a small NICU and a small medium-risk care unit, the sample size was small. The strength of this study relies on its design, without loss of information, and with a multivariate analysis to build the construct of empathy. To the best of our knowledge, this is the first study that measured clinical empathy in health professionals who work with high- and medium-risk neonates in Brazil. Future studies in other NICU in Brazil and other countries are needed to increase knowledge in this area and provide improved quality of care to these neonates.
Conclusion
In this scenario, clinical empathy should improve. There is a need to improve the domain of Walking in the Patient’s Shoes, in this case, the neonate, and provide more empathic care to these patients. We must emphasize that this study was conducted in Brazil, a country with continental dimensions and income disparities. It is important to study clinical empathy in neonatal care in other cultural contexts, for a better understanding of this issue, especially for nurses, whose care is so close to medium and high-risk neonates and their families. Although differences may exist between different countries, with different empathetic behaviors—those more individualistic and those more collectivistic—empathy crosses cultures. It is possible that providing more empathic care could help in fighting discrepancies in healthcare provision across the world, particularly for those patients who are more vulnerable, such as neonates.
Footnotes
Author contributions
COSV, AA, and EALF made substantial contributions to the concept and design of work, analysis, and interpretation of data, revised it critically, and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.