
Abstract
Introduction
Although there have been reports of misbehavior and disrespectful maternal care by healthcare providers worldwide, there are few intervention studies aimed at promoting respectful care, particularly among midwives.
Research objectives
The aim of this study was to examine the effect of Moral Case Deliberation (MCD) on the of midwives’ knowledge and practice in the field of respectful maternity care.
Research design and methods
This semi-experimental study involved 46 midwives working in the maternity departments of two hospitals affiliated with Bushehr University of Medical Sciences in 2023. The two hospitals were randomly divided into control and intervention groups. All midwives from both hospitals were included in the study. The Dilemma Method of MCD was implemented for midwives of intervention hospital. The Midwives’ Knowledge and Practice of Respectful Maternity Care scale was used for data collection. It was administered both before and two weeks after the intervention. Data were analyzed using SPSS (version 20).
Ethical considerations
The study was approved by ethics committee of Bushehr University of Medical Sciences in Bushehr, Iran (ethics code: IR.BPUMS.REC.1402.017). All participants provided written informed consent.
Findings
The intervention group showed a significantly greater increase in knowledge scores from pre-test to post-test compared to the control group (p < .001). The intervention group had a significantly higher mean change score in practice self-assessment and practice peer evaluation, from pre-test to post-test, than in the control group (p < .001).
Discussion
MCD based on the dilemma method can improve practice in the field of respect-oriented midwifery care by increasing knowledge and potentially changing attitudes.
Conclusion
The Dilemma Method of MCD improved midwives’ knowledge and practice regarding respectful maternity care. This method can be included in the midwifery care quality improvement program to promote respectful maternity care. It is necessary to develop methods for wider dissemination of MCD in the cultural context of Iran.
Introduction
Childbirth is a significant event in a woman’s life. 1 The memories of a woman’s childbearing experiences, whether positive or negative, can stay with her for a lifetime. 2 The way caregivers interact with women is an important and influential factor in ensuring a positive and pleasant childbirth experience.1–3 Therefore, the experiences women have with their caregivers can cause them to feel happy and relieved or emotionally distressed. 2
In the last decade, reports of mistreatment, disrespectful care, and abuse during childbirth have been documented in medical facilities worldwide. Disrespectful behaviors have been reported in the United States, Switzerland, the Netherlands, Italy, and Spain, with prevalence ranging from 17 to 67%. 4 A study of Iranian women found that 75.7% of them experienced disrespectful care during childbirth. 5 Disrespectful care during childbirth is a violation of the Charter of Rights of Pregnant Women.6,7 Pregnant women have seven general rights. 1. The right to be protected from harm and mistreatment; 2. The right to receive information, informed consent and refusal, and respect for the patient’s choice and preferences, including companionship during the birth process; 3. The right to privacy and confidentiality; 4. The right to maintain human dignity; 5. The right to equality, freedom from discrimination, and fair care; 6. The right to the highest level of available healthcare; 7. The right to freedom, autonomy, self-determination, and freedom from coercion. 8
Disrespectful maternity care, can include verbal abuse, demanding informal payments, and performing medical interventions such as non-emergency cesarean sections, episiotomies, blood transfusions, and hysterectomies without informed consent, being denied pain relief when needed, restricted visitation with family members, limited decision-making abilities, separation from one’s child, abandonment of care, lack of privacy protection, and restricted mobility.5,9,10
The consequences of disrespectful maternity care can include dissatisfaction with childbirth, a decrease in the mother’s desire to have more children, 11 distrust in the health system, delays in accessing health facilities, 3 an increase in the number of home births, 12 an increased risk of birth complications, 13 sleep problems, a negative impact on sexuality, disruptions in interpersonal relationships, 13 dehumanization of women, 14 negative feelings and thoughts, 15 and an increase in breastfeeding problems.13,16
To promote respectful maternity care, interventions must be carried out and should aim to enhance awareness and attitude, as they are frequently the underlying factors of incorrect behavior.2,3 Studies on midwives’ awareness of charter of rights for pregnant women indicate that their awareness is generally at an optimal level. However, the performance of midwives is not optimal.5,17 This issue suggests that midwives may not have a positive attitude towards respecting the rights of mothers. Therefore, it is important to change their negative attitude in order to improve respectful maternity care. 18 Additionally, midwives may encounter various ethical dilemmas. These may arise from conflicts between a patient’s wishes and the best possible care that can be provided, or from conflicts between a doctor’s orders and a midwife’s professional judgment. 19 These cases require dialogue and discussion to reach the best solution. Moral Case Deliberation (MCD) is a method that focuses on dialogue with others. In MCD, a group of healthcare workers led by a facilitator discusses an ethically difficult patient situation that arises from daily practice. The facilitator’s role is to encourage an open dialogue and stimulate the group’s reflection process. The case should involve a specific, personal experience from the past or present, rather than a hypothetical scenario.20,21 The primary objective of MCD is not to reach a solution, but to collaboratively examine the ethical question at hand and thereby promote critical reflection on the values associated with the specific facts of the case. 20 The dilemma method is the most well-known approach to performing moral case deliberation. 22 The Dilemma Method is an approach to MCD that focuses on situations in which healthcare providers experience a moral dilemma and feel they have to choose between two options. 23 Although dilemma method of MCD is a well-known method in many countries, most studies on its consequences are qualitative.23–25 The interventional studies conducted so far have focused on measuring the effect of MCD on the healthcare provider themselves, such as the impact on moral distress. 26 However, these studies have not addressed the effect of this intervention on caregivers’ future ethical behavior regarding patients. On the other hand, MCD is less known in Iran.
The literature review indicates a scarcity of interventional studies aimed at promoting respectful maternity care, particularly among midwives. Furthermore, these studies have frequently employed methods other than MCD.27–29 Due to the effect of MCD on improving emotional support, collaboration, moral reflexivity, and moral attitude, 30 a question arises regarding whether the implementation of this method can increase compliance with patient rights by healthcare workers, including midwives. If MCD leads to an increase in the performance of respectful maternity care by health care providers, it can be incorporated into the quality improvement program for midwifery care to ultimately bring us closer to global standards of care. Therefore, this study aimed to examine the effect of the Dilemma Method of Moral Case Deliberation on the knowledge and practice of midwives in the field of respectful maternity care.
Methods and materials
Study design and setting
This semi-experimental interventional study with two parallel groups was conducted on midwives working in the maternity department of two hospitals affiliated with Bushehr University of Medical Sciences in Iran, specifically persian Gulf Martyrs Hospital and Shahid Ganji Hospital in Borazjan, from August to December 2023. These two hospitals were selected because they have similar conditions, such as the number of patients and department routines. They are located in two cities within the province, approximately 60 kilometers apart.
Sample size and sampling method
The sample size of 22 participants per group was determined based on Shahabnia’s study, which reported an effect size of 0.93, 31 a type 1 error rate of 0.05, 80% power, and a 10% dropout probability. The sample size was determined using G Power 3.1.9.2 software. As there were a total of 46 midwives, all eligible midwives from the two hospitals were included in the study. One hospital was randomly assigned to the control group, consisting of 25 midwives, while the other hospital was assigned to the intervention group, consisting of 21 midwives. The hospitals were allocated by an individual who was not familiar with the characteristics of the midwives from both hospitals. The allocation assignment was also concealed until the start of the intervention.
Inclusion and exclusion criteria
The inclusion criteria required midwifery associate education or higher and at least 6 months of clinical work experience in the maternity ward. Exclusion criteria for the study included self-reported use of neuropsychiatric drugs, long-term sick leave, transfer to another department or center, failure to participate in MCD sessions (for the intervention group), and failure to complete the questionnaire despite initial consent.
Measures
This study evaluated the knowledge and practice of midwives in providing respectful maternity care. Knowledge was self-assessed, while Practice was evaluated through self-report and co-worker evaluation.
Data was collected using the Demographic Profile Form and the Midwives’ Knowledge and Practice Scale on Respectful Maternity Care (MKP-RMC). The MKP-RMC scale was designed and validated by Moridi et al. in 2020. This scale consists of two sections, Knowledge and Practice. The knowledge section comprises 23 items with binary responses, scored one for a correct answer and zero for an incorrect answer. This section of the scale covers three areas: giving emotional support (items 1–11), providing safe care (items 12–20), and preventing mistreatment (items 21–23). The score ranges for emotional support, providing safe care, and preventing mistreatment were 0–11, 0–9, and 0–3, respectively. The total scale range was 0–23. The practice section comprises 23 items divided into three areas: giving emotional support (items 1–12), providing safe care (items 13–20), and preventing mistreatment (items 21–23). This section is graded using a five-point Likert scale (always, most of the time, sometimes, rarely, and never), with a score of 1 representing the worst situation and a score of 5 representing the best. The score ranges for giving emotional support, providing safe care, and preventing mistreatment were 12–60, 8–40, and 3–15, respectively. The total scale range was 23–115. Moridi et al. measured scale validity and reliability. In a review by 15 experts, all items had a reported content validity ratio above 0.42 and a content validity index above 0.8. The questionnaire’s reliability was assessed using the internal consistency method, and its stability was evaluated through retest-test evaluation. To assess the internal consistency of the knowledge section, Kuder–Richardson’s test was utilized. The coefficient of internal consistency was 0.91 for the total knowledge section and ranged from 0.72 to 0.89 for the three domains. The internal consistency of the scale’s practice section has been confirmed with a Cronbach’s alpha of 0.95 for the total section and between 0.81 and 0.9 for its three areas. The intraclass correlation is reported to be 0.90 for the knowledge section and 0.92 for the practice section. 32 The score obtained for each domain and the total section in both the knowledge and practice sections was converted to a percentage score using linear conversion, as per the instructions. 33 The score range for both scale sections and their areas are between 0 and 100. The practice section of this scale was used with first-person verbs for midwives and with third-person verbs to obtain the opinions of colleagues.
Research implementation method
After the research plan was approved, participant recruitment began following the acquisition of the code of ethic and necessary permits. The first author organized a meeting for midwives at two hospitals, coordinated by the director of midwifery. The meeting covered the objectives and implementation method of the research, as well as the questionnaire that the midwives will complete. The midwives were assured that their information would be kept confidential and that they have the right to withdraw from the research at any stage. After obtaining written informed consent from all eligible midwives participating in the research, they completed a demographic form and the MKP-RMC scale. Furthermore, the practice of each midwife in two intervention and control hospitals was evaluated by two randomly selected colleagues using the practice section of the MKP-RMC scale. The peer evaluation considered the average practice score given by two colleagues. A person who was not aware of the quality of interactions between midwives, randomly selected two colleagues to evaluate each midwife. Then, an envelope containing the assignments of two hospitals to the intervention and control groups was opened, and the intervention began for the midwives of the intervention hospital after necessary coordination.
The intervention was conducted in groups of four or five midwives. Coordination with group members for meeting participation was conducted via phone. Three intervention sessions were conducted over a two-week period for each group. The dilemma method of MCD was used as the intervention method. MCD combines reflection on actual cases with methodical procedures to facilitate moral learning. 20 The dilemma method is based on hermeneutic ethics, which emphasizes the importance of dialogue for learning through the exchange of perspectives and the integration of horizons, and on Socratic epistemology.20,26
Prior to the intervention, an attempt has been made to address the lack of a defined structure in MCD and achieve equalization among groups regarding the moral case presented. The research team, consisting of individuals with experience in the maternity department and two ethics teachers, compiled a list of ethical issues that may arise for midwives and the content of the MCD. The MCD’s content was then reviewed by experts in the fields of midwifery, ethics, and medical education for validation. This content was used to train the facilitator and select cases suggested by participating group members in MCD. In each session, the facilitator asked group members to briefly present any moral issues they would like to discuss during the session. Two cases are then selected to be presented during the MCD session (The facilitator chose the cases based on content developed by the researchers).
The midwifery instructor at the intervention hospital, who is the first author, was trained to act as a facilitator. The second author, a midwifery ethical educator working in the maternity department, attended all meetings. The study supervisor holds a PhD in reproductive health and has 17 years of experience teaching midwifery ethics. She is knowledgeable about the principles of group discussion and the role of the facilitator in group discussion and participated in the training of the first author as a facilitator.
Comparison of demographic and job variable between intervention (MCD group) and control groups.
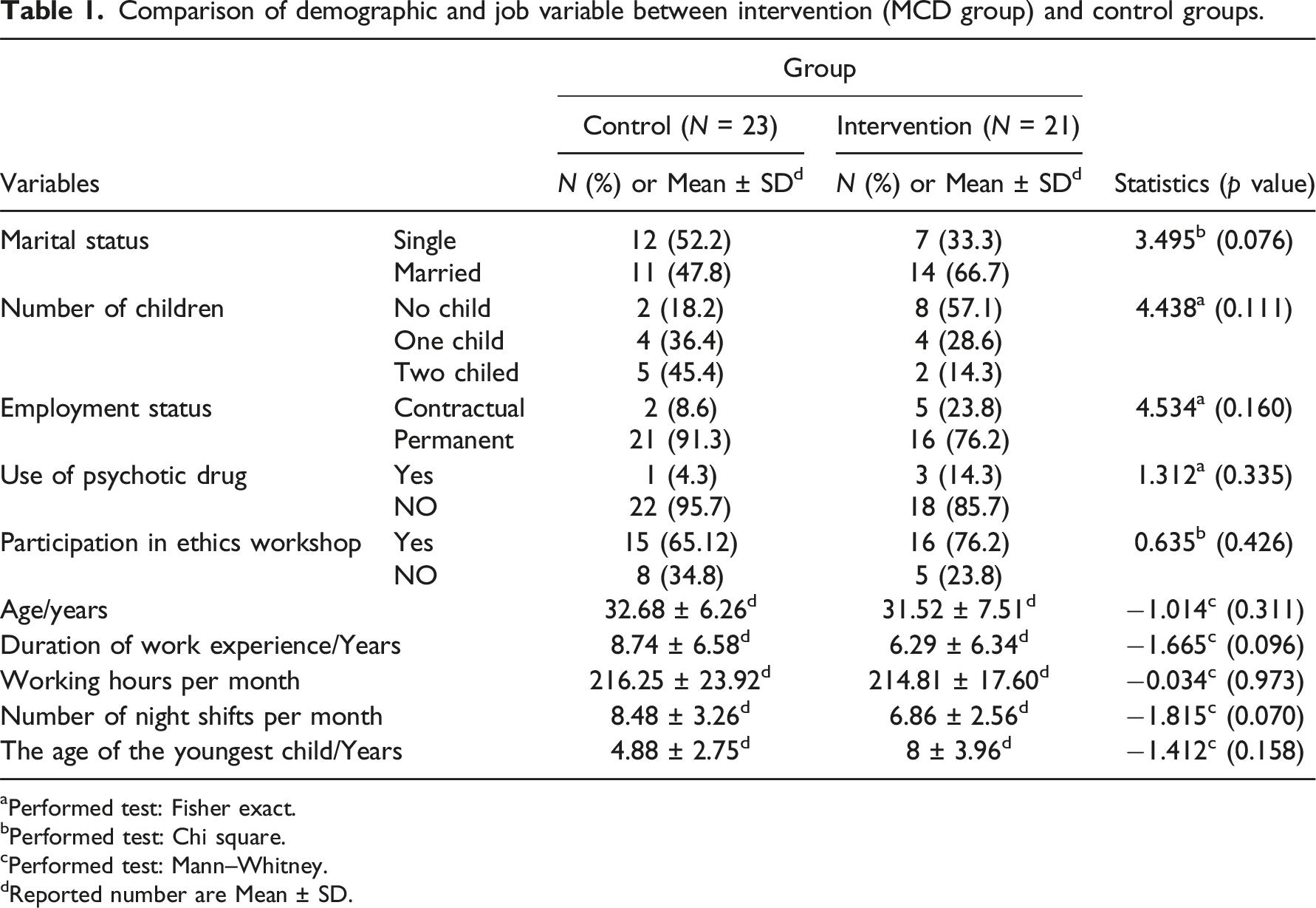
aPerformed test: Fisher exact.
bPerformed test: Chi square.
cPerformed test: Mann–Whitney.
dReported number are Mean ± SD.
In previous studies, the interval between the completion of the intervention and the implementation of the post-test varied. In the present study, as in some previous studies,28,34 two weeks after the intervention, the midwives in both the intervention and control groups completed the MKP-RMC scale, as they did before the intervention. Similar to the pre-test, two colleagues evaluated the practice of each midwife. In this research, department officials were not asked about the practice of midwives because they typically perform executive work and are less involved in clinical care.
No intervention was provided to midwives in the control group. To adhere to ethical principles, the researchers are coordinating a training workshop on patient rights and respectful maternity care for midwives in the control group.
Ethical consideration
This study complies with the Declaration of Helsinki and was performed according to ethics committee approval of Bushehr University of Medical Sciences in Bushehr, Iran (ethics code: IR.BPUMS.REC.1402.017). All participating midwives provided written informed consent and were informed of the research purpose. They were also assured of their right to withdraw at any stage. The results were kept anonymous.
Data analysis
Data analysis was performed using SPSS version 20 software. First, we checked the data for outliers and missing values. No outliers were found. For the main dataset, missing values accounted for up to 2%, which were replaced with the mean. The data was described using mean, standard deviation, number, and percentage. The Shapiro–Wilk test was used to assess normal distribution of the quantitative data. The study employed statistical tests to compare demographic variables between the two groups. The Mann–Whitney U test was used for quantitative variables, while the chi-square test or Fisher’s exact test was used for qualitative variables. The Wilcoxon test was used for within-group comparisons (i.e., pre- and post-test in each group), and the Mann–Whitney test was used for between-group comparisons. The significance level was considered to be less than 0.05 in all cases.
Results
The study included 46 participants, with 21 in the intervention group and 25 in the control group. Two individuals from the control group were withdrawn from the study, leaving 44 individuals for analysis, 21 in the intervention group, and 23 in the control group (Figure 1). Participants flow chart.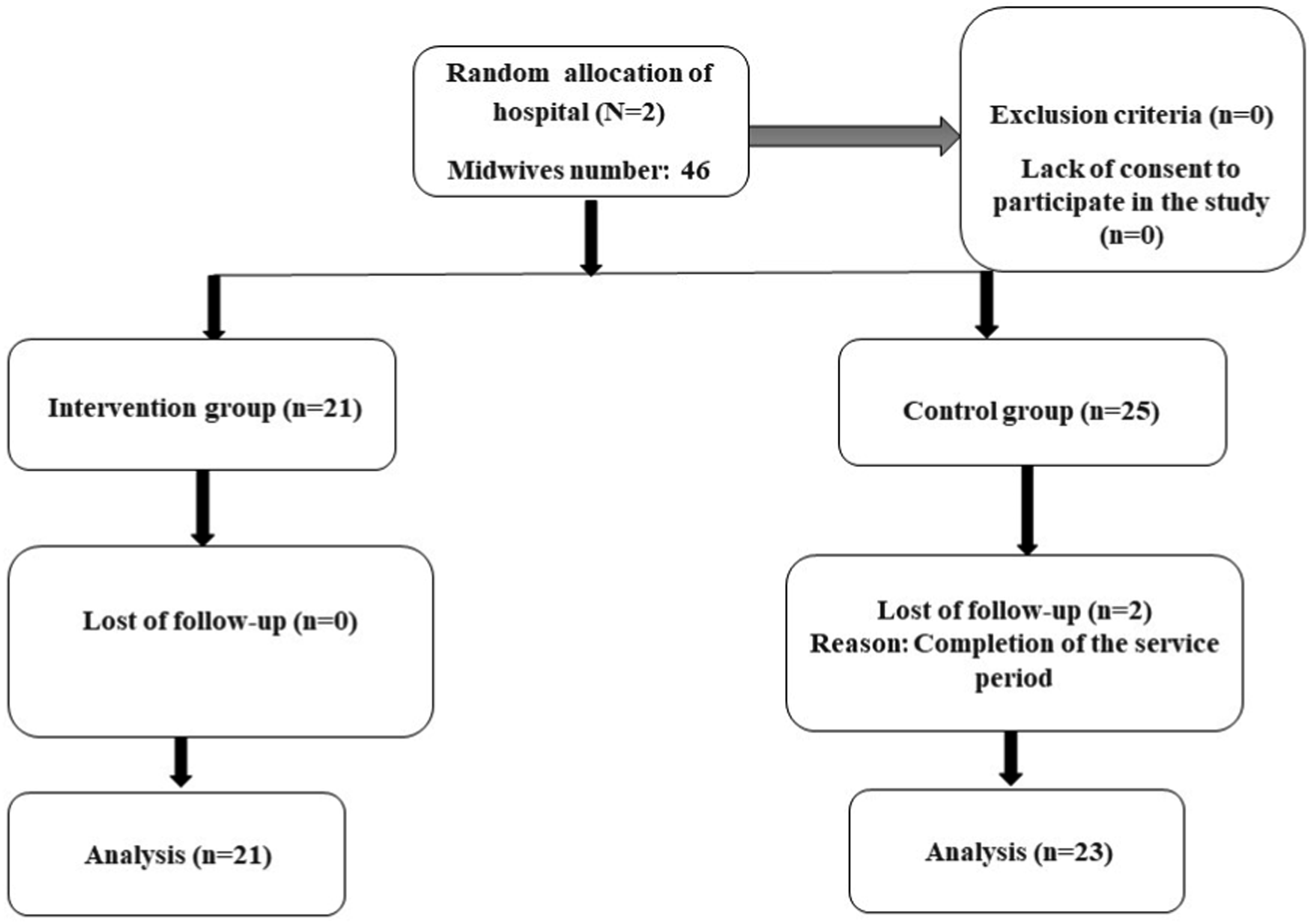
The age of the participants in the intervention and control groups had a mean of 31.52 ± 7.51 and 32.68 ± 6.26 years, respectively. All participants were shift workers. There were no statistically significant differences in demographic variables between the two groups (Table 1).
Within-group comparisons of knowledge regarding respectful maternity care and its domains.
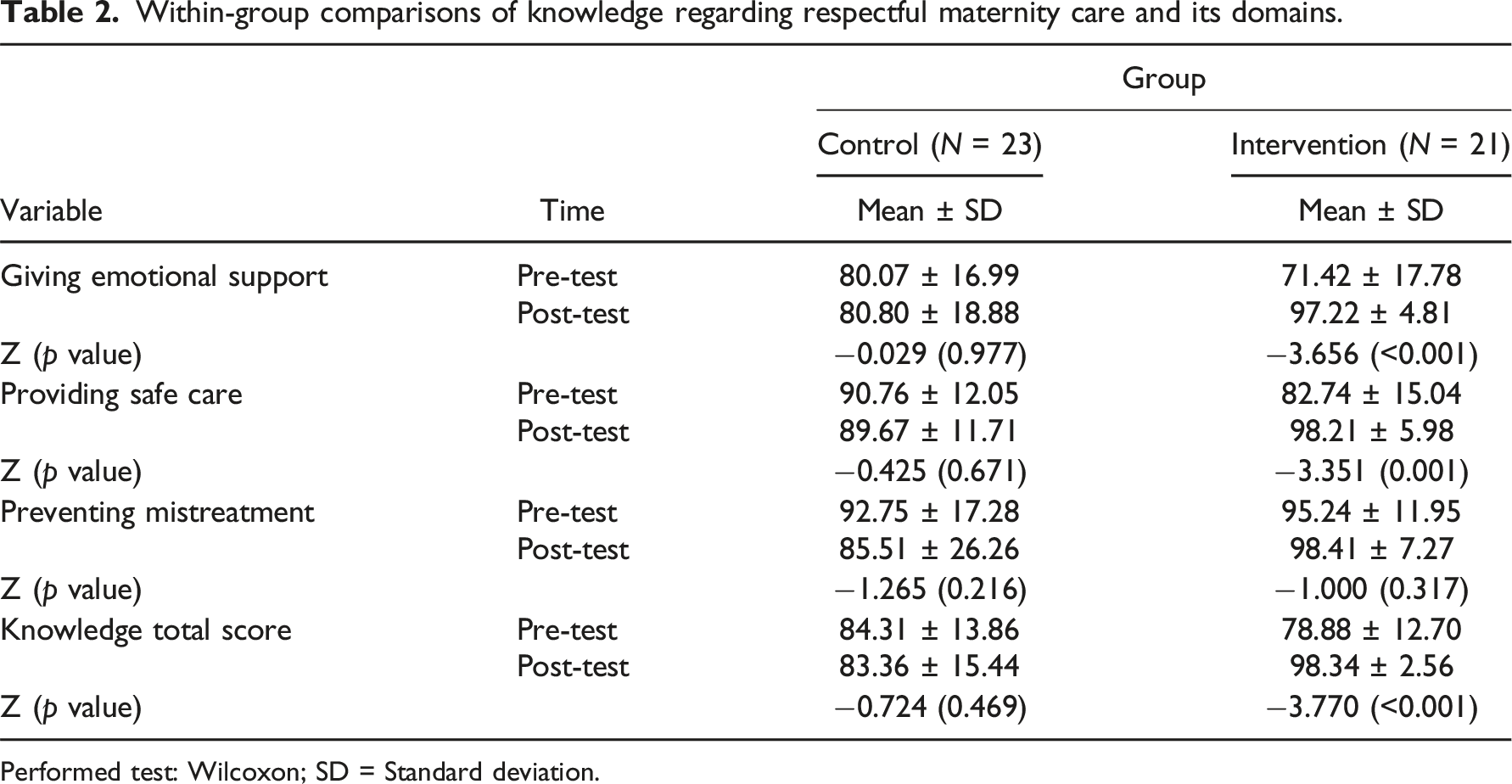
Performed test: Wilcoxon; SD = Standard deviation.
Between-group comparison of mean changes of knowledge regarding respectful maternity care and its domains.
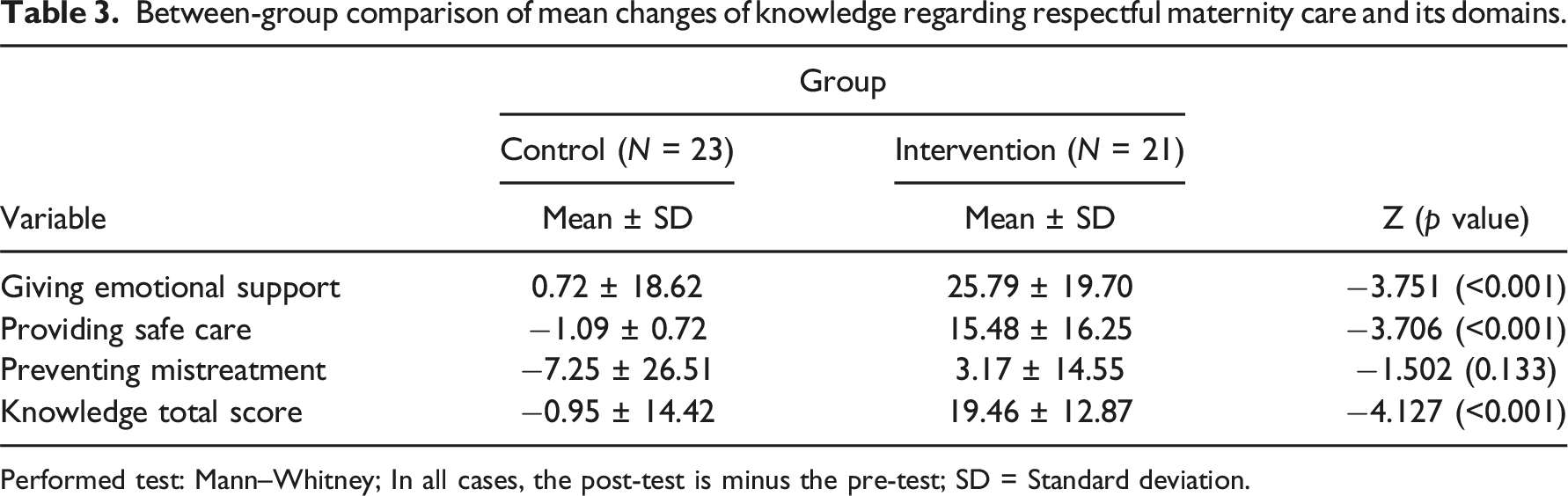
Performed test: Mann–Whitney; In all cases, the post-test is minus the pre-test; SD = Standard deviation.
Within-group comparisons of practice (self-evaluation and peer evaluation) and its domains regarding respectful maternity care.
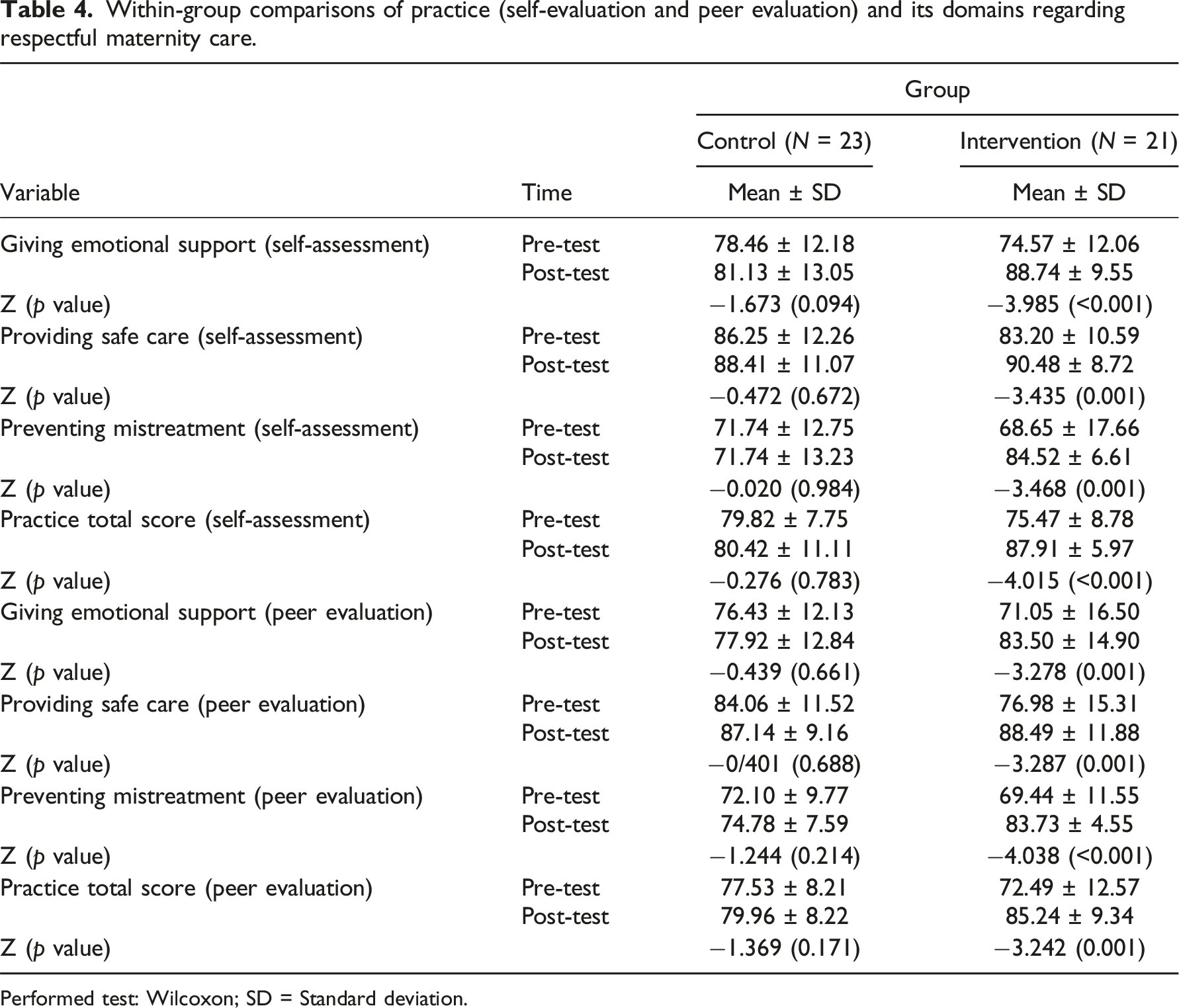
Performed test: Wilcoxon; SD = Standard deviation.
Between-group comparison of mean changes of practice (self-evaluation and peer evaluation) and its domains regarding respectful maternity care.
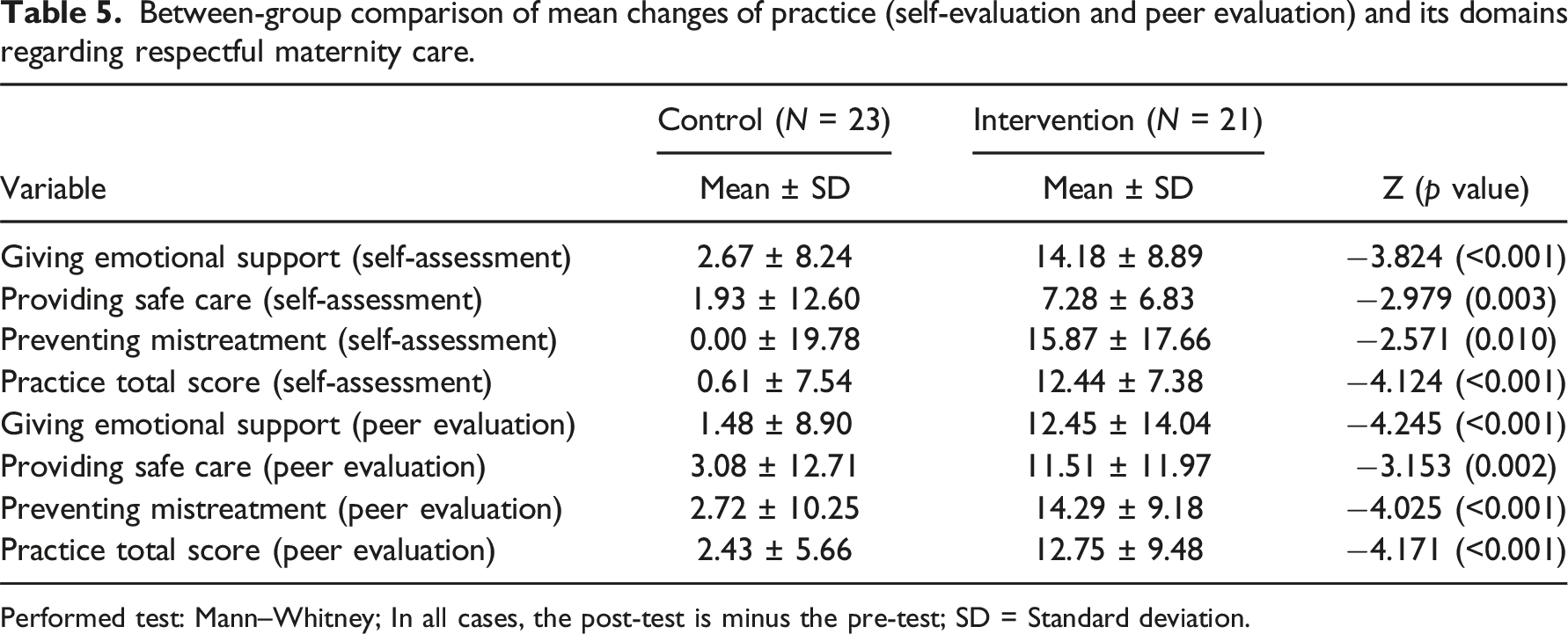
Performed test: Mann–Whitney; In all cases, the post-test is minus the pre-test; SD = Standard deviation.
Discussion
This study aimed to examine the effect of the dilemma method of MCD on the knowledge and practice of midwives in the field of respectful maternity care.
The study results indicate that the intervention group had higher average scores on the knowledge post-test and its two areas, namely, “giving emotional support” and “providing safe care.” Additionally, the intervention group had higher average scores on the practice post-test (self-evaluation and evaluation by colleagues) and its areas compared to the control group. These findings showed the positive impact of the intervention on midwives’ knowledge and practice in the field of respectful maternity care.
To the best of our knowledge, no study has been found that has examined the effect of MCD on midwives’ moral competence or on midwives’ respectful maternity care behaviors. However, studies of other health care professionals show the effect of MCD on moral competence,26,35 which is almost in line with the results of the present study.
A study in Iran found that workshop training on honoring the pregnant mother improved midwives’ knowledge and practice regarding respectful maternity care. 34 Additionally, two studies conducted in Tanzania and Ethiopia showed that interventions for healthcare providers increased the provision of respectful maternity care from the perspective of those receiving care.36,37 A study conducted in southern Ethiopia found that an intervention aimed at providing respectful maternity care resulted in a reduction in the number of mistreatment components experienced by women. 38
A study in Malawi and Zambia investigated the outcome of dignity game. The overall effect of education was observed, but subgroup analysis revealed that education did not have an effect on knowledge in students. Additionally, the training had no effect on attitudes among Malawian nurse-midwives. 39 Perhaps these results suggest that a single educational method may not be universally applicable to all groups and cultures.
Masoumi et al.’s (2016) intervention found that teaching midwives about respectful midwifery care had no impact on the overall satisfaction of care recipients. The only difference between the two groups before and after the intervention was in the psychological domain. This result is not consistent with the present study. Perhaps the reason for this discrepancy is the difference in the intervention method. Masoumi conducted the intervention in the form of lectures and questions and answers. In contrast, the present study aimed to enhance midwives’ knowledge and practice through MCD, an interactive method. 28
Deliberating ethical issues is an interactive way of learning. According to social cognitive theory, which is derived from social learning theory, 40 learning actions and practice result from the interaction of individuals, their environment, and behavioral conditions. Individual characteristics, such as their values and attitudes, and environmental conditions, which can either facilitate or hinder goal achievement, play a crucial role in this interaction. Behavior is the outcome of the interaction between an individual and their environment. 41 The method employed creates conditions for midwives to recognize their needs regarding respectful maternity care. This method allows for adjusting the learning environment and time to the convenience of the learners, based on optimal learning characteristics in education theories. 42 As a result, midwives’ knowledge and practice regarding respectful maternity care have improved.
The intervention did not prove effective in improving midwives’ knowledge about the prevention of mistreatment. No literature was found that examined the three areas of knowledge explored in this study. This result suggests that the interventions may not have successfully covered all topics or that different interventions may be required to improve certain aspects of caregivers’ knowledge. As found in Ratcliffe et al.’s (2016) study, holding a training workshop did not improve knowledge about the principles of confidentiality and privacy. 37 The ineffectiveness of the intervention in our study appears to be due to the ceiling effect. The ceiling effect is observed when a significant proportion of participants begin the study with high scores in the measured variable. As a result, educational experiences may not produce significant gains among these learners. 43
The study revealed a discrepancy between the effect of the intervention on preventing mistreatment and the knowledge of this area. The practice area of preventing mistreatment showed the highest average increase from before to after the intervention. The lower practice in preventing mistreatment may be attributed to midwives’ attitudes towards the matter, despite their knowledge in this area. It is important to note that having sufficient knowledge does not always translate to proper practice, especially when negative attitudes are present. 44
Structural problems may be a reason for the lack of proper interaction and respectful care, despite midwives’ knowledge. Hierarchical structures can cause ethical challenges by reducing the autonomy of midwives. 19 For example, in Iran, midwives perform normal childbirth, but all procedures must align with the physician’s opinion. A difference of opinion between a physician and a midwife can create a dilemma. The power hierarchy within medical teams can create challenges for midwives when resolving conflicts with doctors who hold higher positions. This can lead to stress and inappropriate interactions with patients. Additionally, there is a high rate of caesarean sections in most parts of Iran. Many midwives believe that a significant number of these procedures are performed without medical indication, leading to conflicts between doctors and midwives that prolong decision-making and action time for patients. As a result, midwives may feel unable to provide optimal care for their patients.
It seems that the atmosphere fostered in MCD and its resulting effects have positively influenced the behavior of midwives in the area of respectful maternity care. The Dilemma Method of MCD prompts reflection and facilitates the development of a solution. This intervention examines ethical issues in the desired culture and environment and provides a solution according to the existing culture and context. 20 In the Snoo-Trimp et al. study, healthcare providers reported the consequences of MCD. They experienced positive outcomes related to better collaboration with co-workers, as well as outcomes related to individual moral reflexivity and attitude, both during sessions and in daily practice. 30 During the MCD sessions, participants reflected on their practice and discussed obstacles to providing respectful maternal care, as well as potential solutions to overcome these obstacles. Counseling and discussing ethical issues can reduce perceived interactional difficulties among healthcare providers. Participants engaged in dialogue and interacted with co-workers to clarify their values and beliefs around each moral challenge. As relationships among team members improved, they experienced more openness and fostered a better understanding of different perspectives. 45 As a result, they reached a general and appropriate agreement on how to deal with existing ethical dilemmas. This agreed-upon approach reduced inappropriate interactions with patients that could compromise respect-oriented patient care.
Study limitations
This study was conducted in two hospitals within one province. Therefore, caution should be applied in generalizing the results to midwives in other medical centers. Blinding was not possible in this study due to its nature. Two hospitals in different cities were selected as intervention and control groups to reduce the possibility of content sharing. The intervention group did not receive any written educational content. However, given the prevalence of virtual professional groups, there is a risk of web sharing. Additionally, this research was limited by the fact that random allocation was not performed at the individual level, but rather at the hospital level. Although the midwives in both hospitals had similar demographic and occupational characteristics, there may be individual and geographical differences that could affect the results. Given that the present study measured the effect of the intervention two weeks after its completion, it is recommended that future studies include a longer follow-up period to assess the stability of the intervention’s effect.
Conclusion
The study found that using the dilemma method of MCD can enhance midwives’ knowledge and practice in the area of respectful maternity care. This method can be included in the midwifery care quality improvement program to promote respectful maternity care. The department officials can use this method to discuss ethical cases that midwives encounter in their daily experiences. Additionally, this method can be used in the training of midwifery students. As there are limited studies on the impact of MCD on healthcare workers’ behavior, conducting further studies can help to validate the findings of this study. It is necessary to develop methods for wider dissemination of MCD in the cultural context of Iran. This should be achieved not only through research efforts but also through clinical practice.
Supplemental Material
Supplemental Material - Effect of moral case deliberation on midwives’ knowledge and practice regarding respectful maternity care
Supplemental Material for Effect of moral case deliberation on midwives’ knowledge and practice regarding respectful maternity care by Khatoon Samsami, Maryam Chananeh, Farahnaz Kamalic and Razieh Bagherzadeh in Nursing Ethics.
Footnotes
Acknowledgements
This research is based on the thesis of a Master’s student in midwifery counseling, which received financial support from Bushehr University of Medical Sciences. We sincerely thank the Vice-Chancellor for Research of Bushehr University of Medical Sciences and all study participants
Author contributions
R.B. contributed to the study design and conceptualization, data analysis and interpretation, and article writing. KH.S. and M.CH. conducted intervention and collected data for the study. F.K. contributed to the study design and data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bushehr University of Medical Sciences (Grant No. DP/20/71/642).
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.