
Abstract
Introduction
Organ transplantation is a life-saving treatment method that improves the quality of life for patients by allowing them to make a fresh start. However, individuals with organ failure often cannot find a healthy organ in time, leading to an increasing number of patients waiting for transplantation. Many countries are making various efforts to increase organ donations; however, the global organ donation rate is still not at the desired level, and the gap between organ donation and demand is widening. 1
When examining the literature, societies demonstrate negative attitudes towards organ donation, and it is observed that various factors influence individuals’ decisions regarding organ donation. These include socio-economic status, psychosocial environment, religious and cultural beliefs, family structure, ethnic background, and individual characteristics as sociodemographic factors. Additionally, religious, traditional, and spiritual beliefs play a significant role in influencing decisions about organ donation. 2 In Turkey, like in other countries, there is a high number of patients waiting for organ donations, but the donor population is low. This situation indicates that the Turkish society, similar to others, lacks sufficient information about organ donation and demonstrates negative attitudes towards organ donation. 3
Background
Organ transplantation, an effective and sometimes the only way to treat end-stage organ failure, is a solution dating back to the 1950s, demonstrating the realization of ancient medical ideas. 4 Today, many tissue and organ transplants, such as kidney, heart, liver, cornea, and skin, can be performed more efficiently with the developments in medical technology and surgical techniques.5,6 Despite these developments, many people worldwide are waiting for organ transplants, and this number is increasing daily due to insufficient donations. 7 For example, approximately 4,600 transplants were facilitated in the UK in 2022/23, but it is estimated that there are around 7,000 people on the Organ Transplant Waiting List. 8 According to Eurotransplant, 13,888 patients were registered on the active organ waiting list in 2022. 9 The Health Resources & Services Administration reported that in the United States, about 105,229 adults and children were waiting for organs, including over 90 thousand kidney transplants, about 12 thousand liver transplants, and 3,502 heart transplants in September 2021. 10 According to November 2021 data from the Tissue, Organ Transplant and Dialysıs Department, 700 people were waiting for heart transplantation, 1,150 for liver transplantation, and 17,499 awaiting kidney transplantation in Turkey. 11
The first legal regulation regarding organ donation in Turkey was enacted in 1979 and has been preserved through additional laws to the present day. In these laws, criteria for brain death, brain death determination, and organ transplant regulations are clearly specified. Organ transplants in our country are carried out with informed consent obtained from the patient or their next of kin in accordance with these laws. In the process, organ transplant units and coordinators in hospitals undertake important roles, but there are no legal consultants. In Turkey, there are two consent practices: opt-in and opt-out. The opt-in consent aims to enable individuals to donate their organs voluntarily. In this system, based on Turkish medical legislation, healthcare professionals must obtain explicit consent from the patient or their relatives. In the opt-out consent system, all members of society are considered potential donors. In the event of death, consent is obtained from the family.12,13
The relationship between donor and recipient is significant in organ transplantation. In transplantation from a living individual, the donor is a specific person close to the recipient with whom he or she has an emotional attachment. In transplantation performed from cadaver donors, the recipient is uncertain, and the organ donation list is essential. While cadaver donors provide most organ transplants in developed countries, transplants are provided by living donors in developing countries. In transplantation performed from cadaver donors, the recipient is uncertain, and the organ donation list is essential. 14 While cadaver donors provide most organ transplants in developed countries, transplants are provided by living donors in developing countries. 15 In organ transplants from cadavers, many organs such as the heart, lungs, kidneys, liver, small intestine, pancreas, corneas, tissues, and bone marrow of the deceased donor can be donated and transplanted to compatible recipients on the waiting list. In organ transplantation from cadaver donors, numerous patients awaiting transplants can be reached, while in living donation, only one person is reached. 16 This situation increases the gap between the number of recipients and donors, prolongs the waiting period for organ transplantation, and causes deaths. 17
When the 2021 data of the International Registry in Organ Donation and Transplantation were examined, the rate of live donors was 19.75% in the USA, 11.88% in England, and 51.92% in Turkey. In the same year, it was seen that organ donation from cadavers per million people was 41.88% in the USA, 20.12% in England, and 3.5% in Turkey. 18 According to the Health Resources & Services Administration, 19 people die daily waiting for a donated organ in the U.S. 10 In England, over 430 people died while waiting for a transplant in 2021. 8 In Turkey, approximately 1.9 thousand patients awaiting kidney transplants and 670 patients awaiting liver transplants lost their lives in 2022. 19
When the literature is examined, it is seen that most people have a positive attitude toward organ donation and transplantation but have not successfully taken concrete actions. For this reason, it is clear that there is a global shortage of organs in organ donation. 20 Religious beliefs, ethical grounds, moral and sociocultural inhibitions, and economic and political differences of the individual and his family can cause this inadequacy in organ donation.21,22 People also approach medical institutions with fear and suspicion. 23 Families are in a dilemma as to whether they have made the right decision for their loved one to donate his/her organs or they worry about the deterioration of the body integrity of their loved one during organ and tissue removal. 24
The main reason for the distinctions between individuals’ ethical thinking, decision-making, and behavior is the individuals’ ethical positions. Forsyth defined Ethics Position Theory as a means that enables individuals to determine which direction their decisions should take in the face of the situations they face. 25 According to Forsyth, the ethics position consists of two basic positions: idealism and relativism. While idealism is seen as a position that needs guidance from the rules of right and wrong to make decisions for the welfare of others, relativism can vary according to the view of the consequences of a situation.26,27 When the literature is examined, it is seen that ethical positions are influential in the approaches and solutions of individuals from different cultures and age groups to ethical dilemmas.28,29 When the literature is examined, it is seen that the relatives of patients who decide to donate their loved one’s organs experience dilemmas about organ donation and are affected by culture, religion, and individual views. 21 Therefore, in this study, it was aimed to determine the relationship between the ethical position and personal characteristics of the family members of the patients receiving end-of-life care and their thoughts about organ donation.
Methods
Hypotheses
(1) There is a relationship between the views on organ donation of family members of the patients receiving end-of-life care and their idealistic tendencies. (2) There is a relationship between the individual characteristics of family members of the patients receiving end-of-life care and their idealistic tendencies. (3) There is a relationship between the views on organ donation of family members of the patients receiving end-of-life care and their relativism tendencies. (4) There is a relationship between the characteristics of individual characteristics of family members of the patients receiving end-of-life care and their relativism tendencies.
Design and sample size
This descriptive and cross-sectional study was conducted with family members of the patients in the intensive care unit at a university hospital between September 2021 and February 2022 during the pandemic. The STROBE cross-sectional reporting guideline was used to design and implement the research. The Free Statistics Calculators (version 4.0) was used to determine the power analysis of the sample. The minimum sample size was determined to be 153 with a medium effect size (Cohen’s f2 = 0.15), 0.05 level of error with a 95% confidence interval, 80% power, and 18 predictors according to the linear multiple regression statistical power analysis. The study was conducted with 158 family members of the patients receiving end-of-life care. The inclusion criteria were as follows: The participants (1) were aged 18 years or older, (2) were willing to participate in this study, and (3) filled out complete questionnaire forms. The face-to-face interview method was used for data collection. The purpose of the research was explained to the participants, and the researchers were informed that participation is voluntary, they could leave whenever they wanted, and how to fill out the questionnaires. In this study, participants’ confidentiality was maintained.
Measures
Personal information form
The study data were collected in a questionnaire prepared by the researchers based on the literatüre30–32 and took 15–20 min to answer. The questionnaire form consisted of two parts. The first part consisted of nine questions about the participants’ sociodemographic characteristics (age, gender, marital status, etc…), and the second part consisted of 10 questions measuring their attention to organ donation and transplantation.
Ethics position questionnaire (EPQ)
The Ethical Status Scale (EPQ) consists of 20 questions, prepared according to the five-point Likert type, and covers two main dimensions: idealism and relativism, and each dimensions consisting of 10 questions. Response choices of scale range from completely disagree to agree completely. Individuals with idealistic tendencies avoid harming others by considering how their actions’ consequences will affect others' well-being. Individuals with relativistic tendencies reject universal and absolute moral rules and think that moral rules exist in a situational context as a function of time, place, and culture. 33
Data analysis
IBM SPSS 26.0 (Statistical Package for Social Sciences 26.0) program was used to analyse research data. Firstly, the Shapiro–Wilk test was used to determine the fit of data to normal distribution. Descriptive statistical methods (number, percentage, mean, and standard deviation) were used to evaluate categorical data. Then, the requirements of the data for regression analysis were checked. Whether there was a strong linear dependence between the independent variables was evaluated using the Variance Inflation Factor (VIF) for Multicollinearity. VIF should be under 10. 34 Then, the multiple linear regression analysis enter method was used to define descriptive variables in the idealism and relativism dimensions. In the current study, the VIF of idealism dimensions was found to be 1.188–5.985, and the VIF of relativism dimensions was found to be 1.361–5.985, indicating no multicollinearity problem. P < 0.05 was considered significant in this study.
Ethical considerations
To carry out this study, ethical approval was obtained by the Ethics Committee of a university (dated 11.08.2021 and meeting number: 140). The scale was used in the research after obtaining permission via email from the original author of the scale. The purpose and procedure of the study were explained to the participants. Informed consent was obtained verbally and in writing using the Informed Consent Form. Participants were provided with a statement assuring the anonymity of their responses.
Results
Characteristics of participants
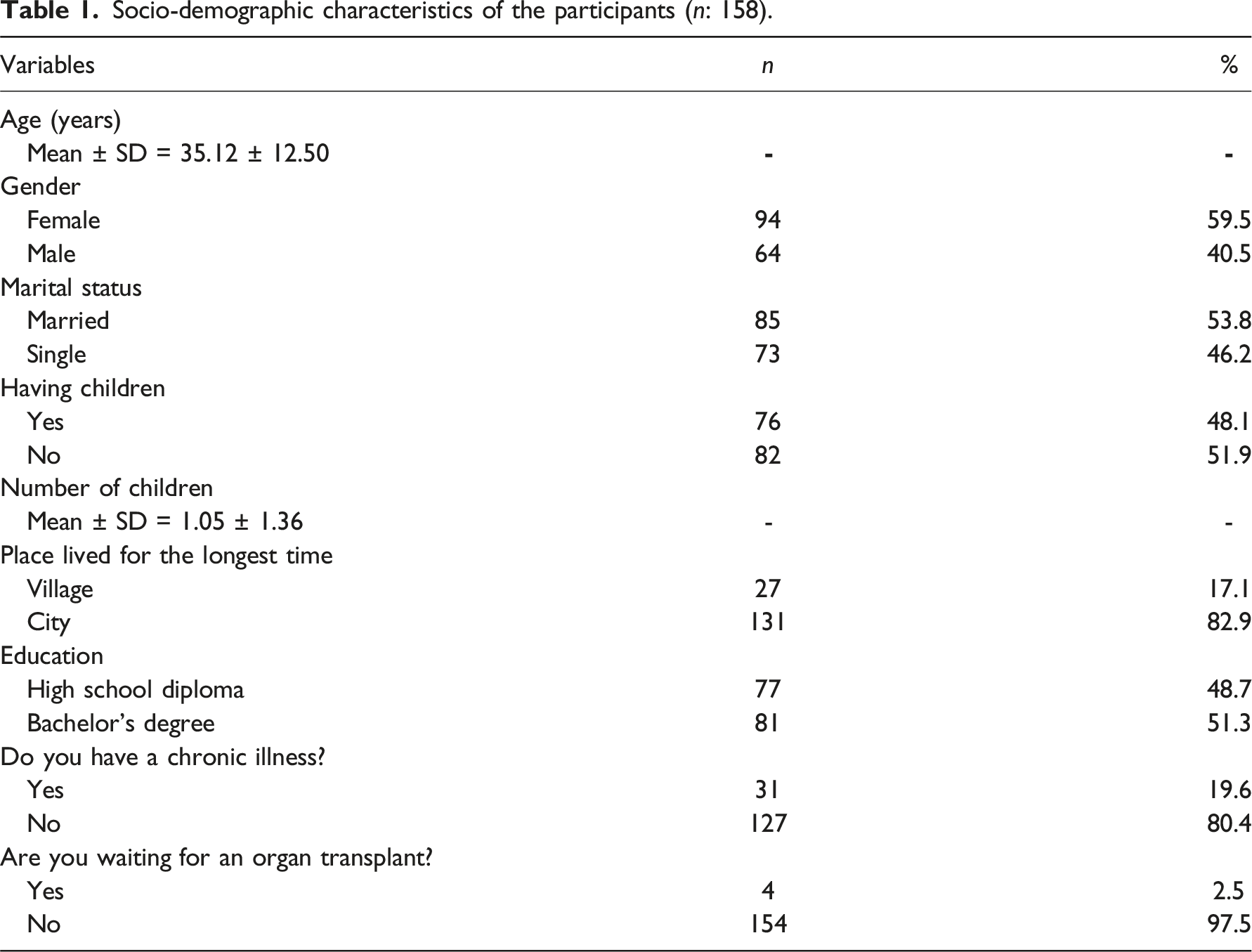
Socio-demographic characteristics of the participants (n: 158).
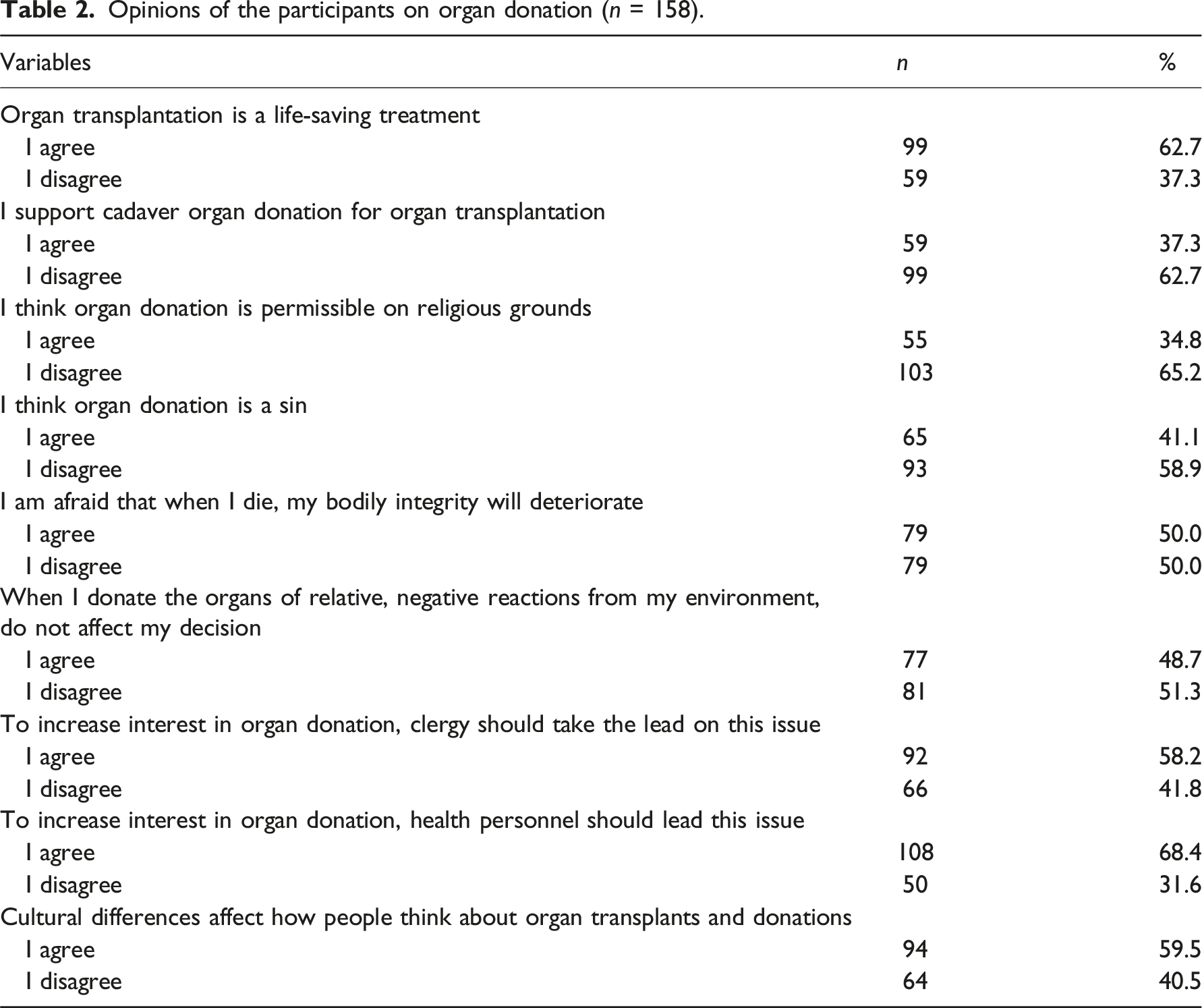
Opinions of the participants on organ donation (n = 158).
Score averages of dimensions
Subscales scores of the participants’ ethics position questionnaire and related Cronbach’s alpha values (n = 158).

Relationship between the characteristics and views on organ donation of family members and their idealism and relativism tendencies
The multiple linear regression model was calculated to determine if there was a significant relationship between the sociodemographic characteristics and views on organ donation of family members and their idealism and relativism tendencies. Number of children participants have (p = 0.020; B:-0.0.120), participants’ status of organ transplant waiting (p = 0.013; B = 0.664), the view that the clergy will increase interest in organ donation (p = 0.038; B: 0.205), and the view that the health personnel will increase interest in organ donation (p = 0.004; B = −0.317) have been identified as factors associated with idealism tendencies.
Participants’ status of having children (p = 0.022: B = −0.411), number of children participants have (p = 0.000; B:0.198), participants' status of organ transplant waiting (p = 0.013; B = 0.664), and the view that the health personnel will increase interest in organ donation (p = −0.374; B = 009) have been identified as factors associated with relativism tendencies.
Participants who have a large number of children, who are waiting for organ donations, who think that clergy should be a guide in increasing the number of organ donations, and who believe that there is no need for healthcare professionals to be a guide to increase the number of organ donations, have higher idealism and relativism scores than those who have a small number of children, who are not waiting for organ donations, who think that clergy should not be a guide in increasing the number of organ donations, and who believed that healthcare professionals should be a guide to increase the number of organ donations.
Discussion
Factors contributing to subscales scores of participants’ ethics position questionnaire (n = 158).
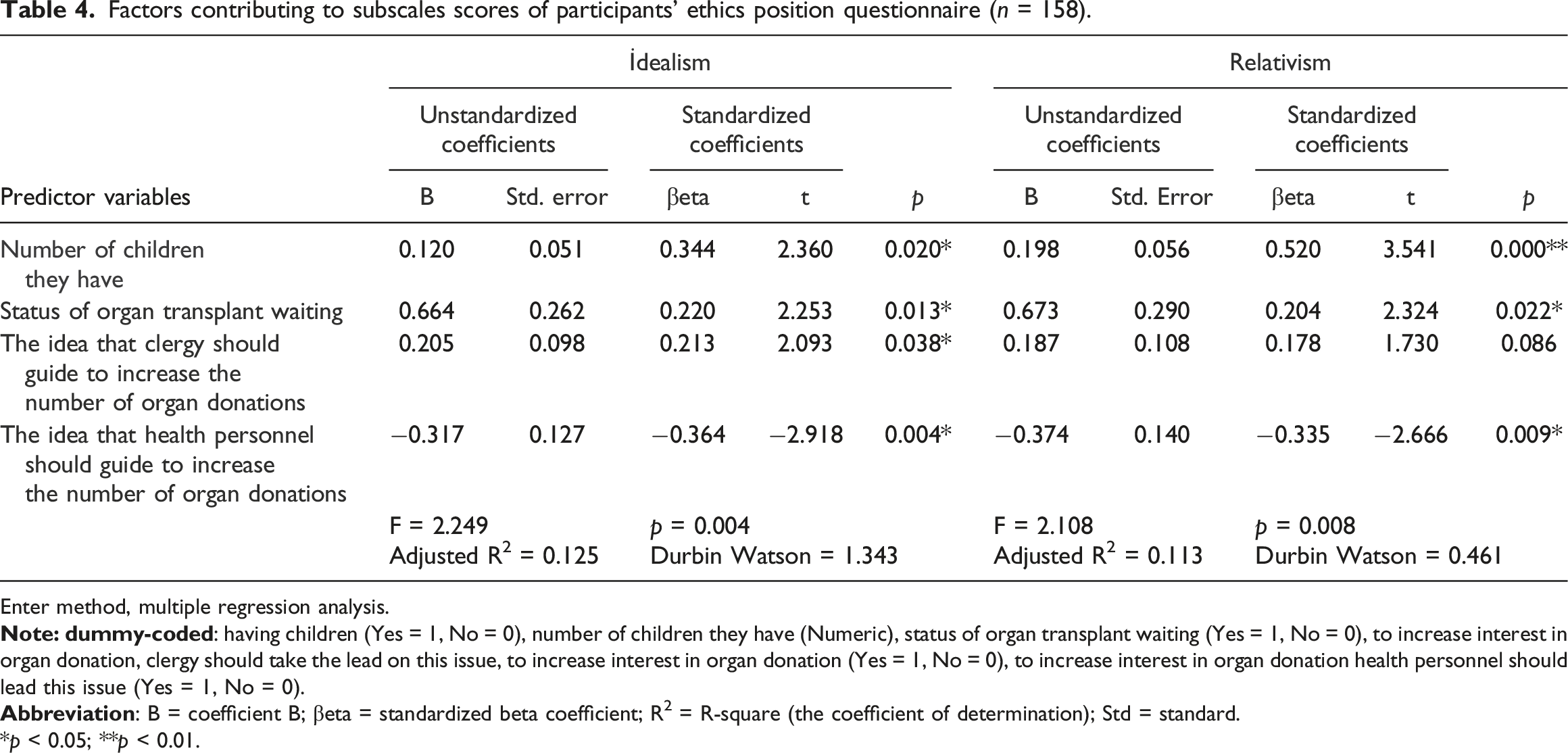
Enter method, multiple regression analysis.
*p < 0.05; **p < 0.01.
When a relative agrees to donate the organs of a family member after death, eight lives may be saved. 35 In the study of Kentish-Barnes et al. (2019), it was emphasized that family members who donated their relative's organs think life is stronger than death. 36 In this study, 62.7% of family members thought organ transplantation was a life-saving treatment.
Organ donation rates that can be performed with organs taken from living or recently deceased individuals vary according to the development level of the countries. While most organ donations are made from cadavers in developed countries, donations are made by living individuals in developing countries. 15 In the study conducted by Siminoff et al. (2020), most participants stated they prefer to donate only to individuals from their immediate family or ethnic group. 37 The study by Akbulut et al. (2020) reported that 41.5% of participants supported deceased donors for organ transplantation. 30 In this current study, 37.3% of family members supported cadaveric organ donation for organ transplantation. Considering that our country is developing, this low rate supports the literature.
Religion is a significant factor that helps people organize their lives and provides guidance on moral issues. Christianity and Judaism have a favorable view of organ transplantation, and donation is an important issue. Giving life to people is an essential virtue in these religions.37,38 Organ transplantation and donation are also permissible in Islam, and it has been declared by the High Council of Religious Affairs of Turkey that organ donation is permissible according to the religion of Islam in our country. 39 Although religions encourage saving lives, relieving suffering, and eliminating harm, religious beliefs are one of the universal barriers to organ donation.30,35 In one study, it was stated that many of the Catholics who participated believed that donating the organs of the deceased was contrary to Catholic teaching. 37
In the study conducted by Doerry et al. (2022) with the Israeli community, it was reported that the behavioral intentions of the participants towards organ donation were low, and participants with a high level of religiosity were reluctant to donate organs. 38 In the study by Kapikiran et al. (2020), 48.1% of Turkish participants reported that organ transplantation was religiously appropriate. 31 The study by Akbuğa and Sürme (2022) reported that %41.2 of university students thought organ donation was a sin in Turkey. 40 In this recent study, all participants were Muslim, and the results were supportive of the literature. While 34.8% of family members found organ donation permissible for religious reasons, 58.9% believed organ donation to be a sin. These findings suggest that attitudes and lack of knowledge regarding religious philosophies may serve as barriers to organ donation.
When the literature is examined, it is seen that there are different opinions between organ donation and the idea of protecting body integrity. In the study of Zhang et al. (2020), it is emphasized that many Chinese perceive maintaining body integrity after death as a responsibility. 41 In the study of Siminoff et al. (2020), it is reported that, according to a Vietnamese participant’s opinion, being reborn with one’s body is possible by preserving body integrity. 37 In this current study, half of the participants feared that their body integrity would be compromised when they died. We believe that this fear stems from individuals’ concerns about compromising the sanctity of their bodies, starting their afterlives incomplete, and the idea of causing harm to their eternal lives.
When examining the literature, it is observed that family members who donate organs often face negative reactions, condemnations, and rejections from others. In Ahmadian et al. (2019) study, it was reported that some of the participating family members were criticized and scolded by their relatives at the post-donation stage, and that they had doubts about the veracity of organ donation. 42 In this current study, which aligns with the literature, 48.7% of the participants stated that negative reactions from relatives do not influence their decisions regarding donating a relative’s organs, while 51.3% reported that such reactions do affect their decisions.
Forsyth defines idealism as the tendency of an individual to perceive the universe more positively and to work for the benefit of others, while relativism is the degree to which one accepts absolutes or universal principles. Individuals with relativistic tendencies make decisions and act according to their experiences, knowledge, and internal moral compass. 33 Wiid et al. (2014) determined in their study that participants’ idealism tendencies were high, relativistic tendencies were moderate, and participants’ idealism scores were higher than their relativism scores. 32 The study by Davis et al. (2001) stated that the idealism factor had a more substantial effect on moral judgment than the relativism factor. 43 This study is compatible with the literature. It was found that the idealism and relativism tendencies of the family members tended to be high, and participants’ idealism scores were higher than their relativism scores.
Ethical position is a commitment to values and creating a way of existence for oneself. 44 In this study, participants with a large number of children had higher idealism and relativism scores than those without a large number of children. We attribute this result to the fact that individuals begin to prioritize the well-being of others and engage in ethical behavior, such as distributing their resources equally, as the number of children increases.
Patients waiting for organ donation are placed on at least one transplant waiting list in their country and remain there until a suitable tissue match is found. During this waiting period, their quality of life decreases, and sometimes this waiting results in death. 45 In this study, participants who were waiting for organ donations had higher idealism and relativism scores than those who were not waiting for organ donations. This result stems from the fact that relatives of patients awaiting organ donations have more empathy with other individuals in similar situations because they undergo the same process and, they believe that organ donation is meaningful for those awaiting donations and can enrich their lives.
There is a wrong and widespread notion in countries like ours, where most of the citizens are Muslim. This notion is that organ donation is not compatible with the Islamic religion. 46 The role played by religious officials, as seen in the case of Saudi Arabia, is crucial in dispelling such misconceptions and garnering societal acceptance for organ donation. Following the publication of a sermon by religious officials in Saudi Arabia supporting organ donation, the number of donations in the country increased. 47 In this current study, participants who believe that clergy should guide in increasing the number of organ donations exhibit higher idealism and relativism scores compared to those who think otherwise. These results suggest that participants consider donation important for individuals awaiting organs, acknowledge that factors such as culture and religion influence organ donation decisions, and advocate for religious officials’ involvement in facilitating such decisions.
Health workers provide a vital link between society and the health system. These professionals’ attitudes, behaviors, and leadership regarding organ donation are essential factors in increasing awareness of organ donation within society.48,49 However, when the literature is examined, it is seen that family members report that they do not want to discuss and talk about organ donation with healthcare professionals when they receive distressing news about their relatives. 50 It is emphasized in the Fernandes et al. (2015) study that a participant felt that he had no strength after receiving the news of his relative’s brain death and started shouting at that moment and that he thought that it was not appropriate for the physician to talk about organ donation during these situations. 51 Similarly, in the Kentish-Barnes et al. (2018) study, it was reported that 65% of relatives of non-donor patients considered the initial request for organ donation by the intensive care team as shocking. 52 In this study, participants who believe there is no need for healthcare professionals to guide efforts in increasing the number of organ donations exhibit higher idealism and relativism scores compared to those who think otherwise. This result suggests that although the participants recognize the value of organ donation for society, they avoided discussing the issue of donation with healthcare professionals during the decision process. Additionally, their reluctance to discuss this issue with healthcare workers stems from their belief that such discussions will diminish the hope of healthcare workers for their patients and result in their loved ones being deprived of necessary treatment and care.
Study limitations
This study was conducted with the participation of family members of patients receiving end-of-life care in a hospital during a specific time period. Because the sample size in this study was small, we cannot generalize the findings to the broader population. Further studies should be conducted on larger sample groups in societies with a multicultural structure.
Conclusion
The study contributes to the literature by revealing the relationship between their ethical situations and their thoughts on organ donation based on the experiences of family members of patients receiving end-of-life care. Accordingly, the idealism and relativity tendencies of the participants who had a large number of children, who were waiting for organ donation, who thought that clergy should be a guide in increasing the number of organ donations, and who believed that there was no need for health professionals to be a guide to increase the number of organ donations, were higher. In line with these results, we recommend that effective training be provided to families about organ donation, that families be given time to decide, that all their questions and reservations are answered, and that strategies be developed to ensure that family members benefit from the support systems they need.
Footnotes
Acknowledgements
The authors thank all the nurses who participated in the study.
Author contributions
Study conception and design: BA, EKT. Data collection: BA, EKT. Data analysis and interpretation: BA. Drafting of the article: BA, EKT. Critical revision of the article: BA
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.