
Abstract
Background
Intensive Care Unit (ICU) nurses face ethical challenges during decision-making in terms of the sophisticated nature of in-patients. Moral comfort is known as a phenomenon with a positive effect on moral decision-making and moral actions of nurses.
Aim
This study investigated ICU nurses’ level of moral comfort and factors affecting it.
Research Design
This study used a cross-sectional descriptive design.
Participants and research context
A total of 350 ICU nurses were selected with the convenience sampling method. The data collection tool included the Demographic Characteristics Questionnaire and the Moral Comfort Questionnaire. The data were analyzed with SPSS19 using descriptive and inferential statistics.
Ethical Considerations
Upon the Committee of Ethics in Human Research’s acceptance of the research concept, approvals were secured, and informed written consent was acquired from all participants. They were assured of the information confidentiality of participation.
Findings
The mean moral comfort score was 112.75 ± 13.18. The mean score of personal factors related to ethics was higher than the external factors pertaining to the environment/organization. The mean scores of “moral comfort in a specific situation” and “moral comfort in general” were 50.52 ± 5.08 and 62.32 ± 9.31, respectively. The mean moral comfort score of nurses was significantly correlated with age, clinical work experience, ICU work experience, marital status, education, and employment status (p < .05). Regression analysis revealed that ICU work experience as the strongest predictor variable predicted 17.7% of moral comfort variance.
Conclusion
Although moral comfort score was at a favorable level, ICU nurses did not feel comfortable when making decisions in moral situations, and nursing managers did not support the decisions of nursing staff. Consequently, this issue warrants the attention of nursing managers and policy-makers. They need to enhance the quality of healthcare by offering more support and addressing the variables influencing the moral comfort of nurses.
Introduction
The Intensive Care Unit (ICU) is a place where patients with life-threatening conditions are treated using various invasive interventions. 1 In the ICU, treatment involves intricate interventions 2 that necessitate the formulation of critical and challenging decisions. 3 Nursing performance is influenced by ethical decision-making and ethical actions in order to deliver safe and ethical care. 4 To make moral decisions in this environment, nurses suffer from moral adversities. In response to various types of these adversities, they experience moral suffering including moral distress, conflict, and damage. 5
Moral comfort is a person’s sense of comfort in decisions and actions related to moral problems. 6 In fact, the positive outcome of a moral situation or dilemma is moral comfort. The principle of moral comfort derives from the nurse’s ability to do the right thing for themselves or their patients and subsequently arises from experiencing the feeling of comfort associated with their actions. 7 Moral comfort happens when the expert can make choices that benefit the patients, incorporate his or her thoughts about the patient into the treatment plan, or reduce or alleviate the patient’s suffering. 6 Wurzbach 8 first introduced the concept of moral comfort in 1996. He described comfort as a moral principle in performing and feeling. This feeling is the nurse’s sense of peace in connection with their actions. The opposite of this situation occurs when nurses see their acts as inconsistent with the ethical principles of exemplary nursing practice. 7 The nurse’s willingness to perform moral action despite the personal consequences and mental peace related to moral action are two defining characteristics of moral comfort. 6
Moral comfort is enhanced by the presence of personal factors such as moral competence, and environmental factors such as managers’ support, and positive moral atmosphere.6,9 Nonetheless, studies indicate contradictory findings of the effect of factors such as culture, gender, religion, age, years of experience, and effect of the organization on ethical concepts.10–13 Personal and environmental factors that foster moral comfort yield beneficial results for nurses, patients, and organizations, including the retention of nursing staff, a decrease in instances of lost nursing care, and a reduction in occupational burnout. Consequently, this mitigates adverse outcomes such as nurse turnover, and staff shortages, which jeopardize patient safety and lead to detrimental patient outcomes. 9
The potential of moral comfort for positive outcomes demands studies focusing the moral comfort. It is essential to understand nursing phenomena such as moral comfort, which contribute to ethical decision-making and/or ethical actions. 9 Nevertheless, sporadic studies have been conducted on moral comfort and factors affecting it. Hence, this study was conducted to determine the level of moral comfort in ICU nurses and factors affecting it.
Methodology
Study design
This descriptive cross-sectional study was conducted in 2024.
Participants
The statistical population of the study compromised ICU nurses working in Iranian hospitals. Considering a correlation coefficient of 0.16, as determined by a pilot study, and a 10% subject attrition rate, the sample volume was estimated to be 350 nurses with a significance level of 95% and a test power of 80%. The sample was a convenience sample of eligible nurses who self-selected to participate. The inclusion criteria were: having at least a BS degree, working in a hospital as a nurse, and having at least 6 months of ICU work experience. Exclusion criteria were: unwillingness to participate in the study and leaving or transferring to other centers. In so doing, after obtaining the necessary permissions, the questionnaire link was provided in virtual groups to be completed with the coordination of the group manager after providing the necessary explanations.
Data collection
To glean the required data, two questionnaires were used as the following. (A) The Demographic Characteristics Questionnaire: It consisted of 6 items about age, gender, marital status, education level, shift work, clinical work experience, ICU work experience, and employment status. (B) Moral Comfort Questionnaire (MCQ): This questionnaire was first developed by Bermudez (2020).
14
It entails 35 items in two parts: the items of the first part are related to the specific situation and the second part pertains to the general experience of nurses. In the initial section, the participant is required to respond to 15 items regarding a specific moral situation or dilemma that occurred within the past 6 months. In the subsequent section, the participant is required to evaluate their general knowledge in order to respond to 20 items. Items are scored using a 4-point Likert scale as follows: 4 = strongly agree, 3 = somewhat agree, 2 = somewhat disagree, and 4 = strongly disagree. This questionnaire has two dimensions wherein 21 items pertain to personal factors dimension related to ethics and 14 items pertain to external factors dimension related to the environment/organization. Moral comfort is measured by summing up the points obtained by each item in the instrument (ranging from 35 to 140), with higher scores indicating higher levels of moral comfort and vice versa. Items can be individually scored to identify specific areas that may affect the overall score. Bermudez
14
investigated the validity of the questionnaire using content, construct and differential validity. In the reliability test, the test-retest results showed a strong positive correlation between time 1 and time 2 (r = 0.769, P < .001), as well as Cronbach’s α = 0.785.
14
Using the forward-backward method, Abbasivand et al.
15
translated the questionnaire into Persian and verified the face, content, and construct validity of the Persian version of questionnaire. The results confirmed the questionnaire’s validity. In confirmatory factor analysis (CFA), the indices confirmed the appropriate fit of the model. A Cronbach’s α of 0.888 and intra-class correlation coefficient of 0.825 indicated the reliability of the questionnaire. Criterion-referenced validity indicated an inverse and significant relationship between the Persian version of the questionnaire and moral distress.
Ethical considerations
After approval of the project proposal in Committee of Ethics in Human Research at the university with code of ethics: IR.IAU.KHUISF.REC.1403.035, the questionnaires were provided to the research units after obtaining legal permissions. To comply with the ethical principles of the research, the informed written consent was completed by all participants. Besides, the confidentiality and anonymity of information was emphasized to the participants. All participants were aware of the objectives of the research and the voluntary nature of their participation.
Data analysis
The data were imported into SPSS19 after coding. Descriptive statistics such as absolute and relative frequency, mean, and standard deviation were used for data analysis. Smirnov–Kolmogorov test was employed to verify the normality of the data distribution. The data distribution was normal, as evidenced by the results (p > .05). Parametric tests such as t test, one-way analysis of variance (One-way ANOVA), and Pearson’s correlation coefficient were used to analyze the data (p = .05). Also, a step-by-step linear multiple regression was used with moral comfort as the dependent variable and demographic characteristics as the independent variables.
Results
Demographic characteristics of participants and their relationship with moral comfort.
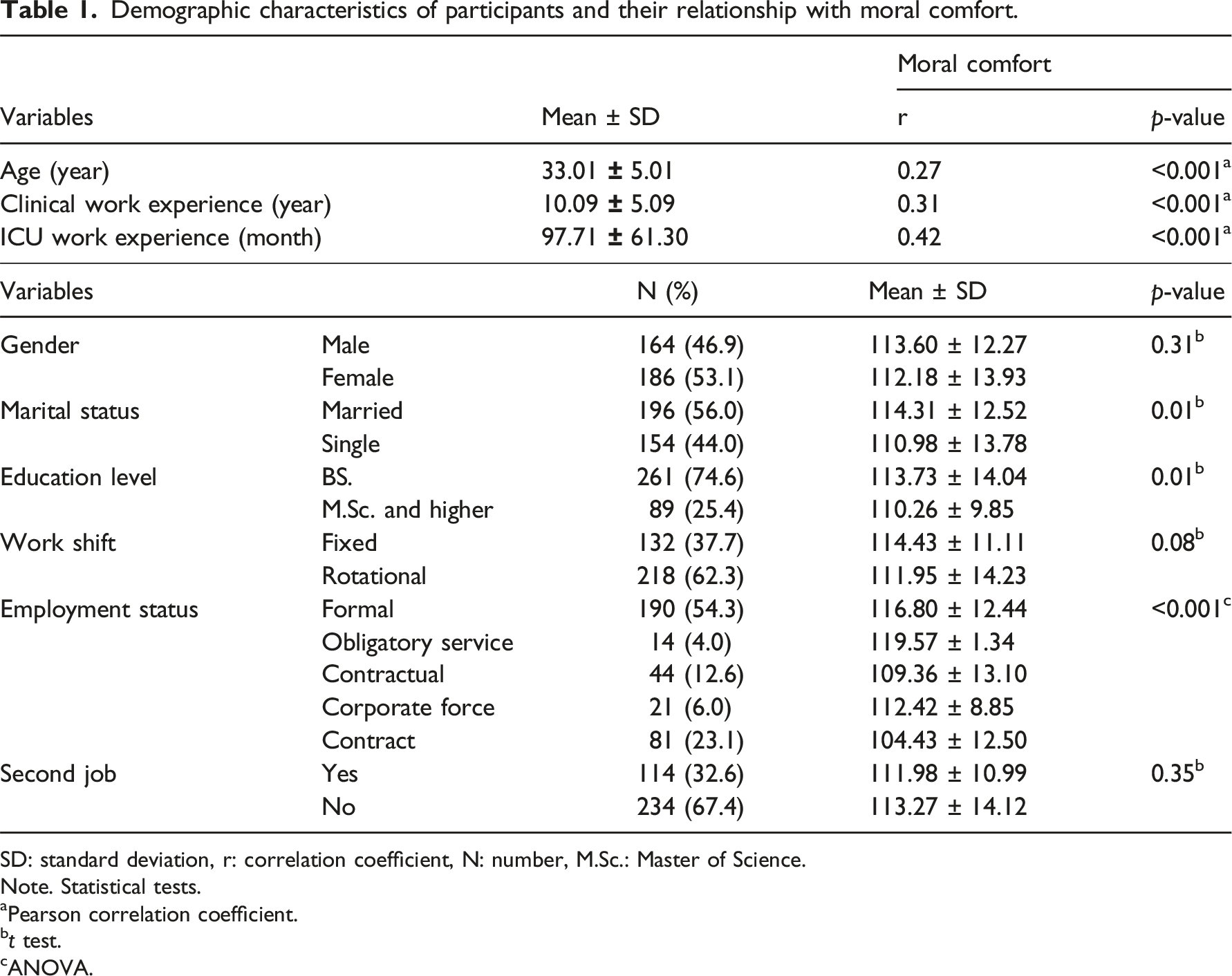
SD: standard deviation, r: correlation coefficient, N: number, M.Sc.: Master of Science.
Note. Statistical tests.
aPearson correlation coefficient.
bt test.
cANOVA.
Mean and standard deviation of moral comfort items in ICU nurses.
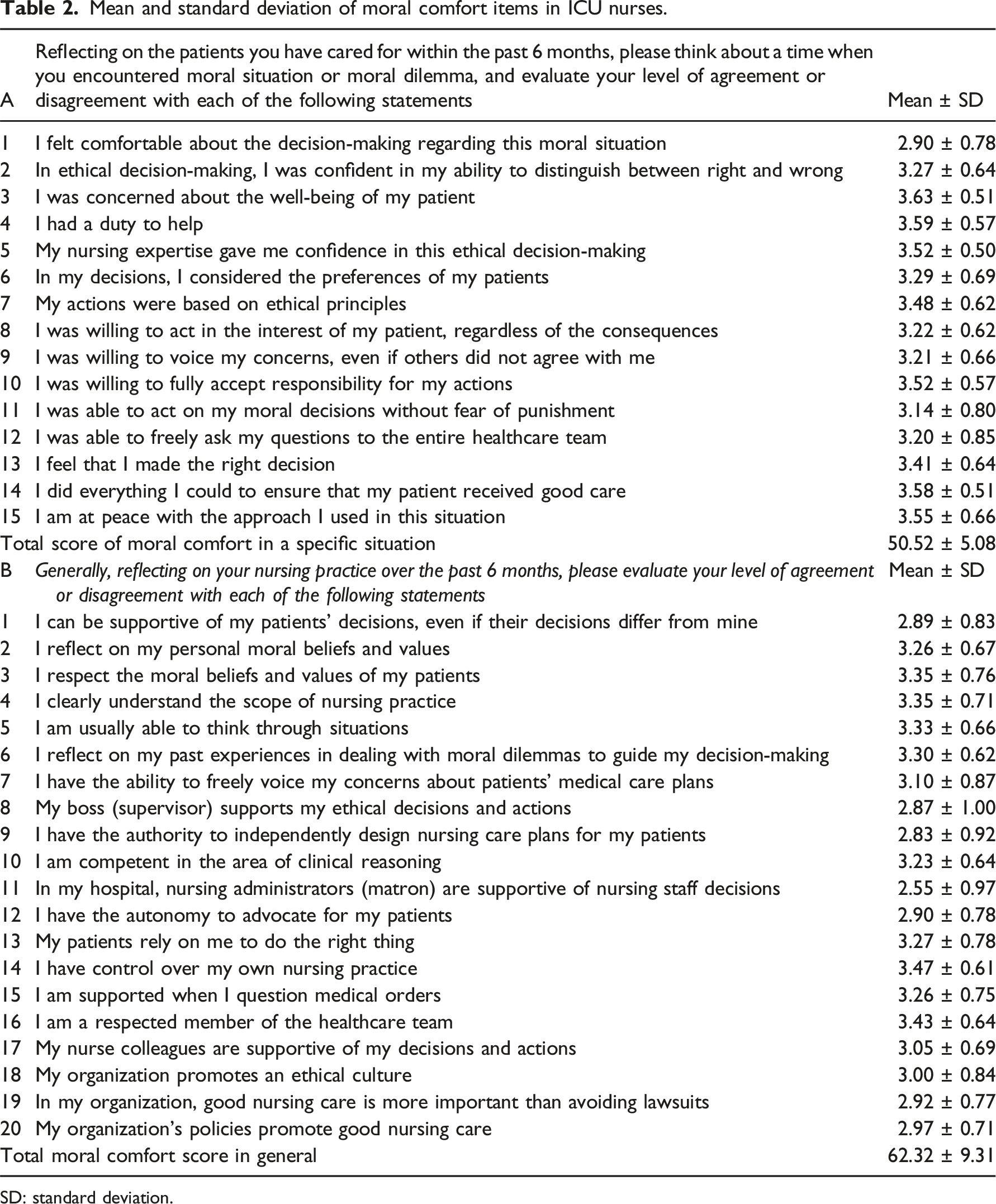
SD: standard deviation.
The mean score of “Moral comfort in general” was 62.32 ± 9.31. None of the items had a score higher than 3.50. In this section, 13 items (2, 3, 4, 5, 6, 7, 10, 13, 14, 15, 16, 17, and 18) had an average score of 3.00 to 3.50. Item 14, that is, “I have control over my own nursing practice,” obtained the highest mean score (3.47 ± 0.61). The average score of remaining seven items was below 3.00. The item: “In my hospital, nursing administrators (Matron) are supportive of nursing staff decisions.” obtained the lowest score with a mean score of 2.55 ± 0.97 (Table 2).
Descriptive statistics of moral comfort and its dimensions.
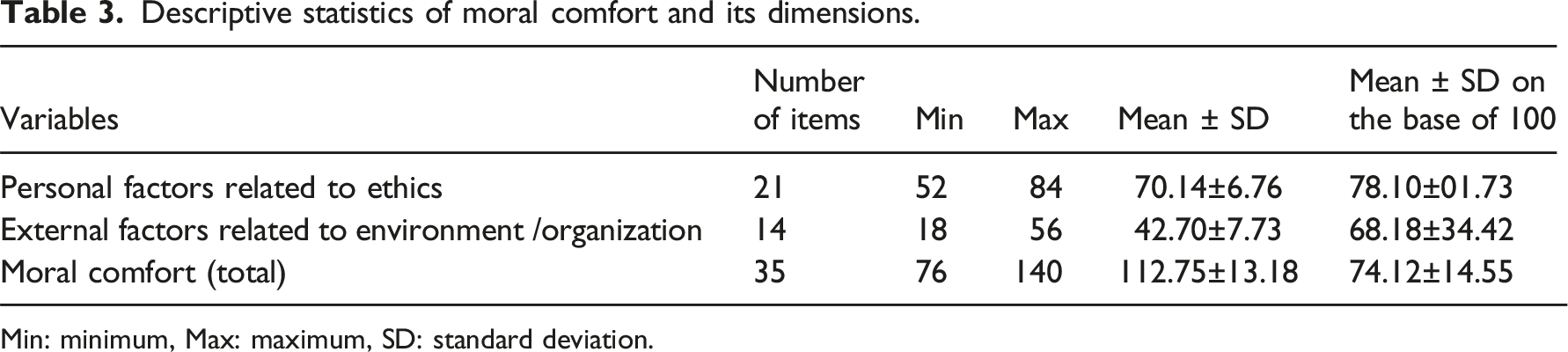
Min: minimum, Max: maximum, SD: standard deviation.
Summary of step-by-step linear multiple regression model.
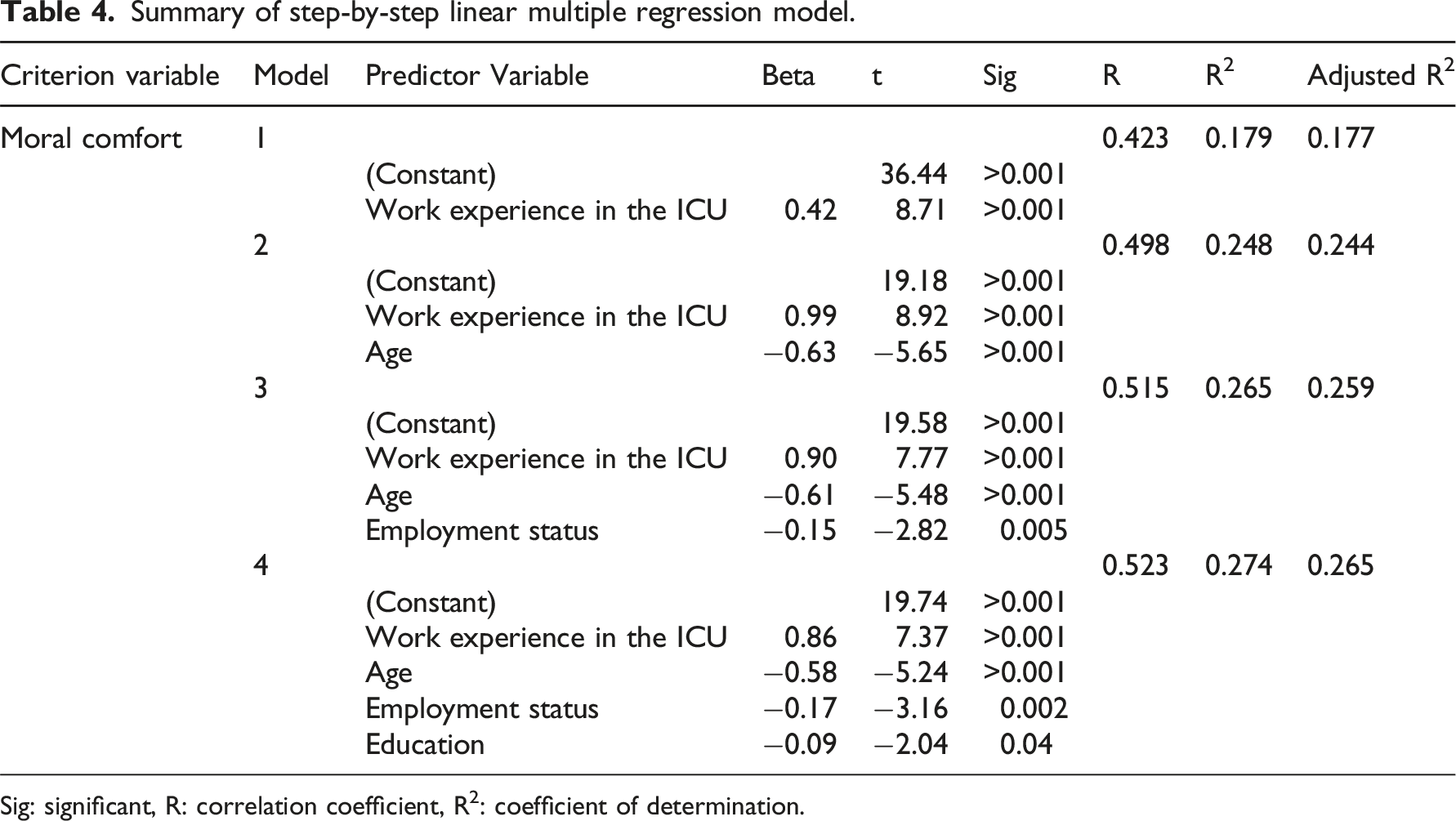
Sig: significant, R: correlation coefficient, R2: coefficient of determination.
Discussion
ICU nurses regularly face patient-related ethical dilemmas requiring their ability to make sound ethical decisions and act on them to achieve the best outcomes for patients and healthcare organizations. As such, it is necessary to understand the nursing phenomena that hinder or potentially promote ethical decision-making and/or ethical actions of nurses. This study investigated the level of moral comfort and the factors affecting it in ICU nurses.
The findings indicated that ICU nurses had substantial moral comfort. Moreover, personal ethical variables had a greater influence on their moral comfort than external environmental or organizational ones. In this regard, Bermudez 9 concluded in a qualitative research that the foreground and beginning of moral comfort is the presence of a moral dilemma or moral situation. Without a moral dilemma, the outcome of moral comfort neither occurs nor exists. He identified the antecedents of moral comfort and classified them as internal (personal) and external (environmental) factors. 9 In other studies, internal factors affecting moral comfort were mentioned. These factors are moral commitment to “good nursing practice,” 8 having moral competence (knowledge) and moral courage that motivate action/moral agency, 6 and expertise and experience with previous moral dilemmas. 16 Corley & Minick enumerate external factors affecting moral comfort as: nursing empowerment via administrative support, availability of material and human resources, access to organizational information, opportunities to participate in decisions related to nursing performance, organizational mission and ethical atmosphere, and clarity of the nurse’s role with defined boundaries. 6
The findings indicated that the mean score of “moral comfort in a specific situation” among ICU nurses was 50.52 ± 5.08, and the lowest mean score was related to “I felt comfortable when making a decision in relation to this moral situation.” In this regard, Crisham 17 states that nurses feel pressure in the decision-making process regarding ethical dilemmas. She asserts that this may result from environmental factors, including organizational policies that conflict with nurses' notions of justice, adherence to physician directives, time limitations, allegiance to the nursing profession, the patient, and the hospital, the continual escalation of professional information demands, and the intricacy of optimizing the utilization of this information. 17 Bermudez points to internal factors (moral commitment, moral competence, and moral courage with nursing experience and expertise) and external factors (administrative support/empowerment, participation in decision-making, access to information and human/material resources, moral climate, and role/boundary clarity) as antecedents of moral comfort. 9 Most studies show the sophisticated and challenging role of ICU nurses during the decision-making process.18,19 In this regard, Heradstveit concluded in a qualitative systematic review that ICU nurses make ethical decisions to protect patients' concerns, guide the family’s decision-making process, and assume the role of mediator. 19 The results of another study in northern Turkey showed that nurses had moderate decision-making ability when faced with ethical dilemmas and that their ethical decisions were influenced by environmental factors such as the nurses' perception of the support provided by the organization. 4
The mean score for “moral comfort in general” was 62.32 ± 9.31. The item “In my hospital, the nursing director (matron) supports the decisions of the nursing staff” obtained the lowest score. This finding confirms the results of previous studies.20,21 Organizational support has been investigated in many studies and its level was evaluated in a low range.20,21 Nevertheless, the study conducted by Gorji et al. 22 in emergency nurses and the research conducted by Jay Maningo-Salinas 23 in oncology nurses both reported moderate levels of perceived support. The discrepancy between the results of the studies may be attributed to the diverse leadership styles and organizational climates of the managers. Studies show that leadership plays an important role in developing and maintaining nursing ethics. Ethical nurse leaders create work environments that affect employees' choices, behaviors, and values24,25 The nurse manager should support the staff in performing appropriate ethical care for ethical reflection. 26
The findings suggested that there was a significant relationship between “nurses' moral comfort” and “age, clinical work experience, ICU work experience, marital status, education, and employment status.” No research was identified to compare the relationship between these variables and moral comfort as a result of the sporadic studies on moral comfort. However, the findings of prior research on moral distress, which is the antithesis of moral comfort, indicated that reports of moral distress may be influenced by culture, gender, age, and years of performance.13,27,28 Despite the results of the present study in effect that there is no relationship between moral comfort and gender, other studies showed that female nurses reported more moral comfort than males.27,28 Some studies report that younger nurses experience higher levels of moral distress.11,29 Nurses with older age reported more moral comfort. Finally, contrary to the result of the present study, which stated the relationship between moral comfort and work experience and that work experience in the ICU was the strongest predictive variable in moral comfort, some studies showed that nurses with more nursing experience or years in a clinical situation had higher levels of moral distress.30,31 Hence, it is stated that these differences depend on the working environment and the patients' community. 32
Limitations of the study
One of the limitations of the present study was the self-reporting of the questionnaires. Social desirability bias is a problem that should be considered using self-report instruments. Moreover, a cross-sectional design was used in this research making causality impossible.
Conclusion
Even though the moral comfort score was at a favorable level, ICU nurses expressed that they did not feel comfortable when making decisions in moral situations, and nursing managers, as expected, did not support the decisions of nursing staff. Thus, nursing managers and policymakers should carefully evaluate this problem. They should improve healthcare quality by offering additional assistance and taking into account the elements that influence nurses’ morale. Nursing managers and officials can create more moral comfort in nurses, especially ICU nurses by supporting the decisions of nurses, which affects mental health and improves the quality of patient care. The results of this research can be used in micro and macro policies regarding planning to improve the obtained results.
Footnotes
Acknowledgments
The researchers should thank all the participants that helped us in the completion of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.