
Abstract
Background
Patients with intellectual developmental disabilities (IDDs), as members of a vulnerable population, require specialized care that many ICU nurses feel inadequately prepared to provide. The complexity of caring for IDD patients often leads to feelings of moral distress, self-doubt, and a struggle to maintain resilience among ICU nurses.
Research question/aim/objectives
This study aims to explore ICU nurses’ lived experiences caring for patients with IDD.
Research design
A descriptive, phenomenological qualitative approach was used along with inductive analysis to explore the meanings ICU nurses attribute to experiences caring for IDD patients.
Participants and research context
ICU nurses (N = 20) who met inclusion criteria were purposively sampled.
Ethical considerations
The study received ethical approval from an institutional review board. Informed consent was obtained from all participants.
Findings/results
Three main themes emerged from the analysis. First, in main theme 1, If Only I Had Known More, nurses reported insufficient training specific to IDD care, expressing shame about their knowledge gaps. Second, in main theme 2, They Deserve Better, nurses highlighted the lack of resources and institutional support, complicating efforts to deliver appropriate care. Finally, in main theme 3, It Weighs on My Soul, nurses reflected on the emotional toll of caring for IDD patients, discussing subthemes such as self-doubt, emotional detachment, coping efforts, witnessing isolation, and moral distress.
Discussion
These findings highlight personal, educational, and systemic gaps shaping ICU nurses’ experiences with IDD patients. Limited training and insufficient resources intensified moral distress. There is an urgent need for IDD-oriented education, institutional support, and policies that promote compassionate, tailored care.
Conclusions
Findings suggest there is a strong alignment with the ethics of care framework. Such a connection emphasizes the need for systemic changes to empower ICU nurses to deliver compassionate, individualized care to IDD patients and enhance professional resilience and patient outcomes.
Introduction
Exploring the lived experiences of ICU nurses caring for patients with intellectual developmental disabilities (IDD) is essential to understanding how they impact nurse well-being, ethical decision-making, and care practices. Lived experience can help guide interventions that improve patient outcomes and strengthen nurses’ professional and emotional well-being. Components of this inquiry may reveal sources of moral distress, identify ways to foster resilience, and support nurses’ capacity for moral agency.
For example, nurses’ beliefs about the quality of life of patients with IDD can shape attitudes, emotions, and approaches to care. When nurses view IDD patients’ lives as limited, they often experience moral distress, feeling conflicted about the value of intensive interventions. In contrast, nurses who see IDD patients as capable of having meaningful lives may be more likely to exhibit moral agency and, therefore, resilience. 1
Background
Individuals with IDD experience significant healthcare disparities, including higher morbidity, increased hospitalization rates, and poorer overall health outcomes due to systemic barriers in healthcare access and provider preparedness.2–4 Nurses play a crucial role in addressing these disparities, yet research indicates a persistent gap in both nursing education and professional development related to IDD care.5,6
Educational gaps and preparedness in IDD care
Gaps in medical and nursing education contribute to inadequate preparation for healthcare providers treating individuals with IDD. Clarke highlighted that medical students and physicians report low confidence in treating IDD patients due to insufficient training and exposure, a challenge that also persists in nursing curricula. 7 Non-specialty track nursing students also receive minimal IDD-specific education, leaving them underprepared for encountering this patient population during clinical practice. To address this, Clarke advocated for integrating IDD-related content into coursework, utilizing standardized patients with IDD, and incorporating case-based learning to improve competency. 7
In fact, multiple studies highlight the lack of IDD-specific education in undergraduate and postgraduate nursing curricula. Cashin et al. found that 68.5% of Australian registered nurses (RNs) had no undergraduate coursework on IDD, and 80.8% lacked dedicated clinical placements. 2 Postgraduate education and continuing professional development (CPD) on IDD remained significantly low, with 92.4% and 65.2% of nurses reporting no formal training, respectively. 2 This educational deficiency directly affects nurses’ preparedness, with many reporting feeling only somewhat knowledgeable (55.7%) or not knowledgeable (27%) in IDD care. 2
Similar findings emerged in a qualitative study of Swedish RNs in home-care settings, where nurses relied heavily on intuition and prior experience rather than formal education when providing care for IDD patients. 5 Nurses expressed frustration over limited access to training and support, which impeded their ability to communicate with non-verbal patients and advocate for specialized care effectively. 5 These findings emphasize an urgent need for global IDD-focused curriculum integration in nursing education. 5
Impact of training and educational interventions
Educational interventions have been shown to enhance nurses’ knowledge, confidence, and attitudes toward IDD care. A systematic review by Hay et al. examined various educational approaches and their impact on healthcare professionals. 3 The review found that 60% of interventions resulted in measurable improvements in knowledge and skills, while 40% led to positive shifts in confidence and attitudes. 3 Practical training methods included didactic learning, interactive workshops, experiential learning, and immersive training, with experiential learning (e.g., direct patient interactions) yielding the greatest improvements in confidence. 3 However, challenges remain in sustaining a long-term educational impact. Most interventions studied were short-term and lacked follow-up assessments to determine whether improved knowledge translated into better clinical outcomes. 3 Additionally, there is no standardized IDD training framework across healthcare institutions, leading to inconsistent educational experiences among nurses internationally. 3
Systemic barriers and the role of advocacy
Beyond education, systemic barriers within healthcare institutions further complicate IDD care. Nurses expressed feeling ‘held hostage’ by an unsupportive system that fails to accommodate the unique needs of IDD patients. 5 Time constraints, inadequate staffing, and over-reliance on support staff for patient communication contribute to fragmented and suboptimal care. 5 Nurses also struggle to access mental health services for IDD patients, as psychiatric concerns are often dismissed due to diagnostic overshadowing. 6
The American Nurses Association (ANA) position statement emphasizes an ethical responsibility of nurses to advocate for equitable and developmentally appropriate care for individuals with IDD. 6 Key recommendations include promoting self-determination in healthcare decisions, addressing healthcare disparities through policy advocacy, and ensuring interdisciplinary collaboration. 6 The ANA also emphasizes the need for specialized IDD nursing roles and increased research on best practices in IDD healthcare delivery. 6
Literature gap
Despite increasing recognition of healthcare disparities for individuals with IDD, research on the lived experiences of ICU nurses caring for this vulnerable population in the United States remains minimal. Over the past decade, there has been limited literature focusing specifically on nursing perspectives in intensive care settings when managing the complex needs of patients with IDD. Understanding the challenges ICU nurses face, including communication barriers, ethical dilemmas, and gaps in institutional support, is essential for improving both patient care and nurse preparedness. Addressing this gap through qualitative inquiry can inform policy changes, guide educational reforms and future research, and enhance clinical practice to better serve patients at the bedside in critical care environments.
Purpose
The purpose of this study was to understand how ICU nurses interpret and manage the lived experience of caring for patients with IDD.
Methods
Qualitative approach and research paradigm
Approach
We used a descriptive phenomenological approach to explore the personal, meaning-making processes of ICU nurses caring for patients with IDD. Descriptive phenomenology allowed for deeply examining the participants’ lived experiences, focusing on the essence of their encounters, challenges, and responses in critical care settings.9,11–15
Paradigm
Situated within an interpretivist paradigm, reality is considered to be constructed through individual perceptions and experiences. An interpretivist lens supports a reflective exploration of how participants’ experiences with IDD patients shape, challenge, and redefine their professional resilience and moral agency. Such perspectives allowed for capturing evolving ways ICU nurses internalize their professional experiences and build moral resilience amidst ongoing challenges.9–15
Researcher characteristics and reflexivity
The research team comprised three nursing faculty members with extensive critical care backgrounds and two research assistants who were undergraduate nursing students. The faculty members’ clinical experience in critical care provided valuable insights into the complexities of ICU nursing, particularly in understanding the unique challenges associated with caring for patients with IDD. Their background enabled them to interpret the emotional and ethical dimensions of participants’ experiences with depth and empathy.
However, this expertise also required the researchers to engage in careful reflexive practices to avoid potential biases that could influence data interpretation. To ensure unbiased perspectives, the researchers regularly engaged in reflective discussions, acknowledging their assumptions and experiences that might shape their understanding of the participants’ narratives. This reflexive approach helped to maintain objectivity, allowing the data to speak authentically to the lived experiences of the ICU nurses interviewed.9–15
The two undergraduate research assistants provided a fresh perspective, unclouded by extensive clinical experience. Their involvement in the study allowed for additional reflexivity, as they offered interpretations less influenced by preconceived notions of ICU care, enhancing the study’s rigor. Merging insights from experienced faculty and undergraduate researchers allowed the team to foster a balanced analysis, leading to a clearer understanding of the challenges ICU nurses face with IDD patients.11–15
Context
ICU settings are inherently high-stress environments characterized by the need for rapid decision-making, continuous monitoring, and the management of critically ill patients. These intense conditions often amplify the emotional and moral challenges faced by healthcare providers, particularly when caring for vulnerable populations such as patients with IDD. 16 In this context, ICU nurses are frequently confronted with ethically complex situations that challenge their professional resilience and moral agency. The high stakes of patient outcomes, coupled with the specialized needs of IDD patients, place additional demands on nurses, requiring them to navigate both clinical complexities along with personal and professional experiences.
Sampling strategy
Recruitment occurred electronically through a professional organization exclusive to critical care nurses. A purposive sampling strategy was employed to recruit ICU nurses with substantial experience and direct exposure to ethically challenging scenarios, particularly involving patients with IDD. 10 This approach ensured that participants had the necessary background to provide in-depth insights into their roles’ moral and emotional complexities. Sampling continued until data saturation was reached, and no new codes emerged during the interviews and analysis.11–15
Ethical considerations
The study received ethical approval from the relevant institutional review board, ensuring all research activities adhered to ethical standards for human subjects research. Before data collection, all participants were given the information necessary for informed consent, which included detailed explanations of the study’s purpose, procedures, potential risks, and benefits. Participants were also informed of their right to withdraw from the study without consequences.
Confidentiality was maintained through secure data storage and anonymization of interview transcripts, with identifiers removed to protect participants’ identities. Given the emotional sensitivity of discussing moral distress, special care was taken to create a supportive interview environment. Researchers were trained to approach discussions of distressing experiences with empathy and sensitivity, providing participants with resources and support information if needed.8,10
Data collection
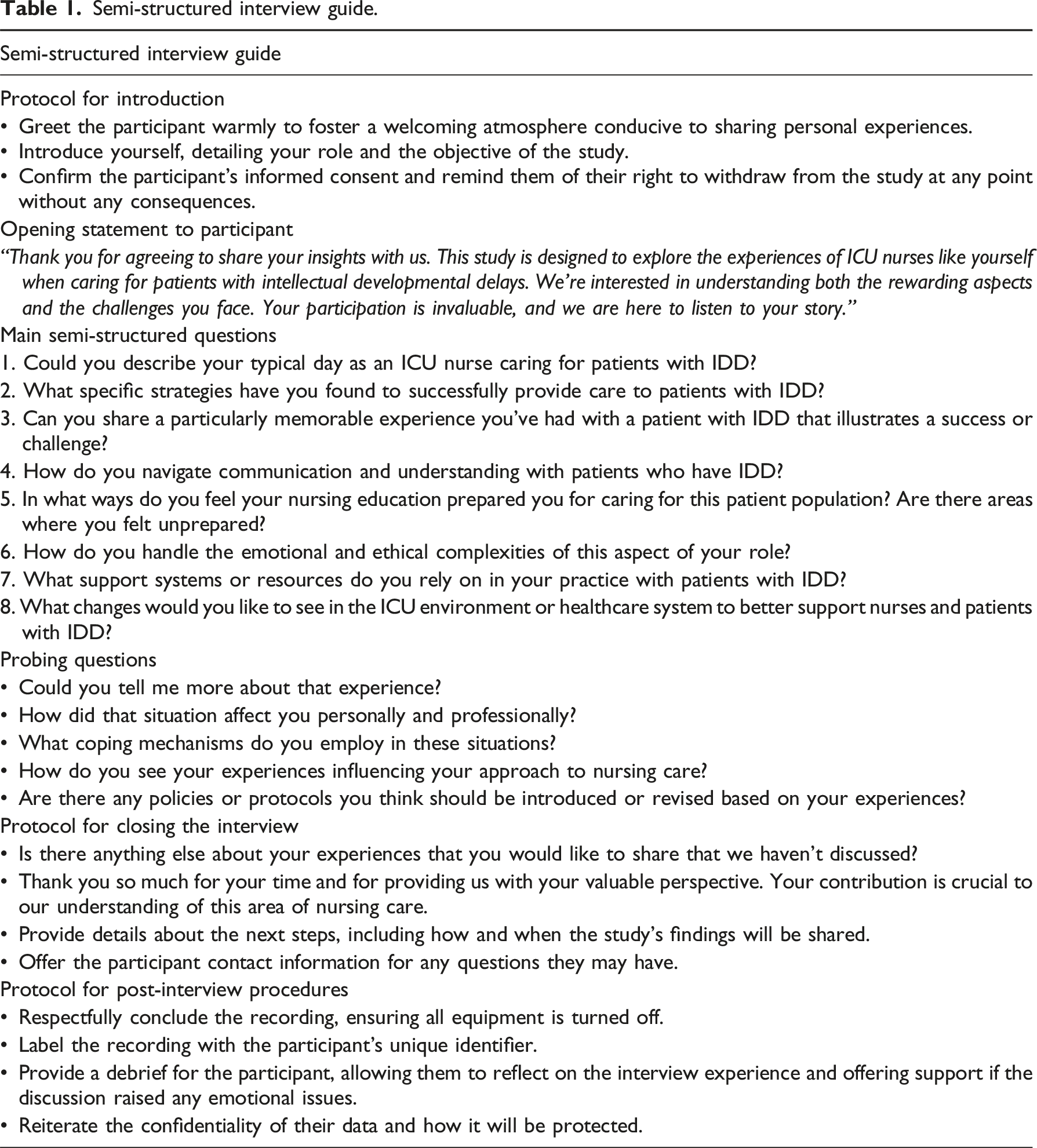
In-depth, semi-structured interviews were conducted with each participant, lasting approximately 60 min. Participants shared detailed accounts of their experiences with moral distress, resilience, and agency when caring for patients with IDD in ICU settings. The interview process incorporated adaptive questioning, enabling the researchers to refine and adjust questions based on emerging insights during each session. The iterative approach allowed for a more comprehensive exploration of the participants’ perspectives, capturing the full scope of moral resilience and agency.
Data collection instruments and technologies
Instruments
Semi-structured interview guide.
Technology
Zoom software was utilized to conduct and audio-record the interviews, providing a reliable and secure platform for data collection. The recordings enabled detailed data capture, ensuring accuracy in transcription and facilitating in-depth analysis of participants’ responses.
Data processing
Transcription
All audio-recorded interviews were transcribed verbatim to capture participants’ exact words and expressions, accurately reflecting their experiences.
Deidentification
To protect participant confidentiality, identifying information was removed from the transcripts. Participants were assigned unique codes, and any specific references to names, locations, or other personal details were replaced with generic descriptors to ensure that individuals could not be identified.
Secure storage
All data, including audio recordings, transcripts, and coded documents, were securely stored on password-protected devices and secure servers accessible only to authorized research team members.
Data management
Emphasis was placed on systematic data management to ensure accuracy and consistency throughout the analysis process. Verification included cross-checking transcripts against audio recordings for accuracy and ongoing coding verification to maintain thematic consistency.
Data analysis
Data analysis followed an iterative approach consistent with descriptive phenomenology based on the work of Edmund Husserl.11–15 Researchers were trained to code data in alignment with the reflexive thematic analysis method. Training sessions ensured a shared understanding of the analytical approach, emphasizing the iterative nature of coding, reflexivity, and consistency in theme development. Regular meetings were held to discuss coding decisions and enhance coherence in the analysis. The following steps outline the analysis process: 1. Researchers (AW, GSC, and SP) began by immersing themselves collaboratively in the data, repeatedly listening to audio recordings, and reading transcripts. This process deepened their familiarity with the content and enabled them to understand the context and meaning of participants’ experiences. 2. During the initial coding phase, transcripts were reviewed collaboratively line by line, and text segments inductively emerged as relevant to moral resilience, moral distress, and agency, which were then coded. The focus was on capturing detailed descriptions and specific experiences, highlighting the emotional and ethical dimensions of caring for IDD patients in ICU settings. 3. After initial coding, researchers independently clustered similar codes together to identify patterns across participants. This clustering helped in recognizing commonalities and differences, setting the foundation for the emergence of broader themes. 4. Researchers then began regular, collaborative meetings to cluster related codes organized into preliminary themes representing key aspects of nurses’ experiences. These initial themes reflected the complexity of their responses to moral challenges and their strategies for resilience. 5. The initial themes were then refined collaboratively by revisiting the transcripts and coded data to ensure consistency and coherence. This iterative process involved revising themes to capture subtle variations in meaning and eliminate redundancies. 6. Researchers collaboratively determined that themes were finalized once they had established boundaries so that they were distinct. At this stage, themes were reviewed to ensure they accurately reflected the essence of the participants’ experiences and aligned with the study’s research question. 7. Each theme was collaboratively defined with a detailed description and then supported by representative quotes from the raw data. Definitions encapsulated the essence of each theme, highlighting how ICU nurses interpret, cope with, and find meaning in their roles amidst moral challenges.
Techniques to enhance trustworthiness
Following the principles of phenomenology introduced by Husserl, the researchers employed bracketing, or epoché, to set aside preconceptions and biases that could influence data collection and analysis.11–15 Consciously suspending personal judgments and previous knowledge about ICU nurses’ experiences with IDD patients, the researchers aimed to capture participants’ authentic perspectives. Bracketing involved reflective journaling and regular discussions among the research team to identify and address potential biases throughout the study. This process allowed the researchers to approach each interview with an open mind, fostering a deeper understanding of participants’ lived experiences without undue influence from prior assumptions.
An audit trail was maintained to document each research process step, from data collection to analysis and interpretation. Detailed records of coding decisions, thematic development, and researcher reflections were kept, ensuring transparency and accountability. The study allowed for an external evaluation of the research process by a detailed audit trail, thereby reinforcing the dependability of the findings. 17
Data triangulation was applied by cross-referencing findings with current research on ICU nursing, moral distress, and care for IDD patients to further strengthen trustworthiness. The researchers identified consistencies and divergences by comparing the emerging themes with existing literature, enhancing the study’s transferability. Triangulation provided a broader context for interpreting the findings, situating the experiences of ICU nurses within established knowledge, and helping to identify areas where additional support and training might be necessary.9,10,17
Findings
Participant characteristics
The participants of this study represented a range of ethnic origins, primary shifts worked, ages, and years of experience (see Figure 1). Demographics of intensive care nurse participants.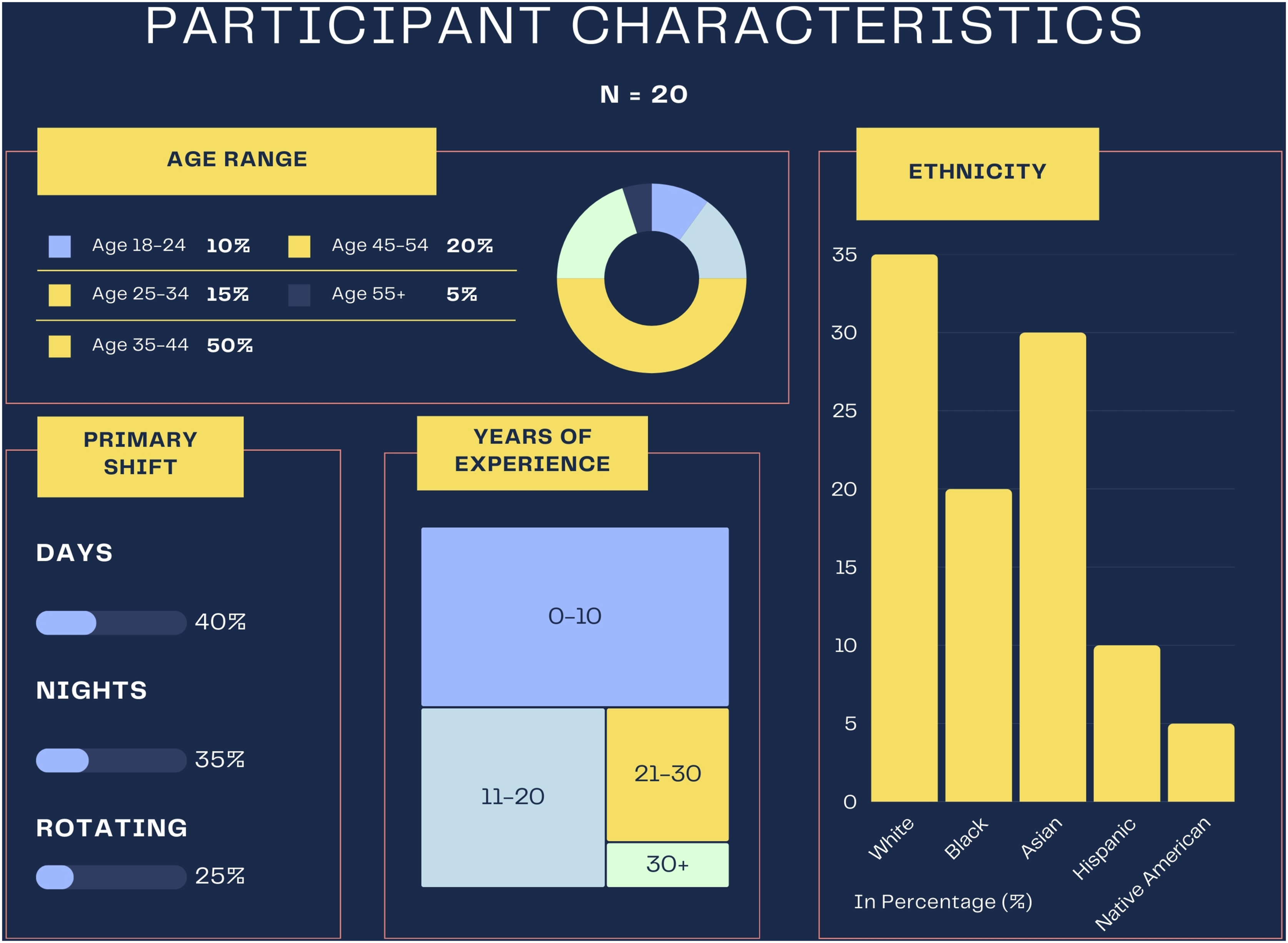
Main themes and subthemes
Three main themes emerged organically from the data during analysis. They were 1) If Only I Had Known More, 2) They Deserve Better, and 3) It Weighs on My Soul. Each theme, along with its respective subthemes, is discussed in further detail below.
Theme 1: If Only I Had Known More
In Theme 1, If Only I Had Known More, the lack of formal training for caring for patients with IDD was a prominent theme across participant narratives. ICU nurses expressed feelings of unpreparedness and frustration stemming from a gap in their nursing education, highlighting a pervasive need for dedicated training on IDD care (see Figure 2). Main Theme 1 and subthemes.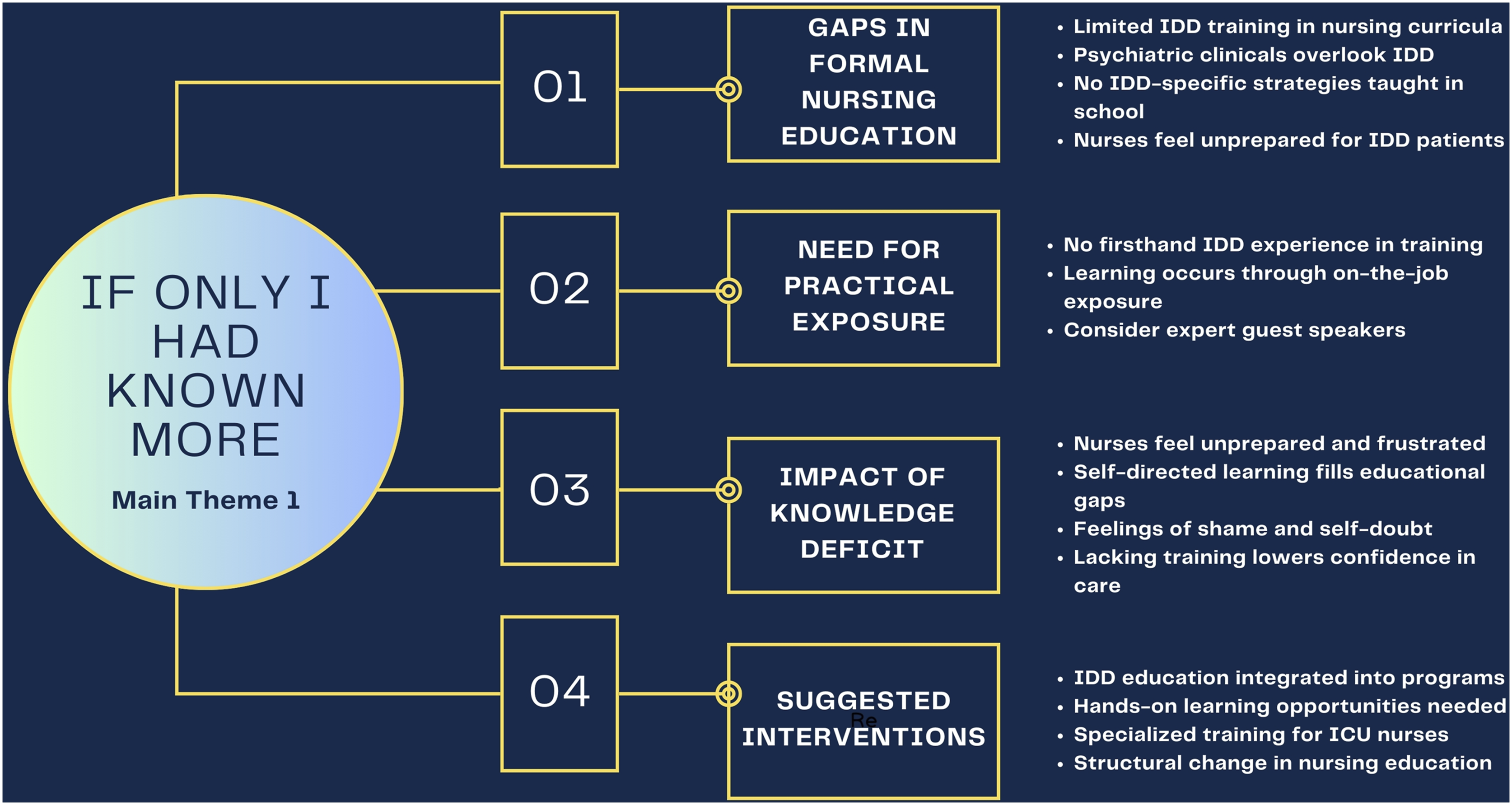
Subtheme 1: Gaps in Formal Nursing Education
One participant reflected on their clinical education, noting that while they completed a psychiatric clinical, “the setting of the psychiatric clinical is people with…psychiatric problems” (ICURN8). They explained that there was a lack of emphasis on chronic psychiatric conditions, especially for patients whose primary reason for admission was not related to mental health. This oversight left them unprepared when encountering patients with developmental delays in a critical care setting.
Several participants emphasized the lack of IDD-specific education within nursing curricula. One nurse shared, “I did not, not at all. I was a CNA in an ICU, so I did get exposure to that, so that prepared me… But nursing support… There was nothing in nursing school that was specifically related to how to care for these patients. There was nothing like, ‘Here are some strategies to use with a patient with a developmental delay’” (ICURN2). The sentiment echoed the views of other participants who felt that their training did not prepare them for the unique challenges presented by IDD patients in ICU settings.
Another participant expressed frustration with the curriculum structure, suggesting that nursing programs should bring in “nurses that are working [with these patients], who come in and speak to classes and really share what their days look like, what this patient population looks like, and how to communicate with different types of patients” (ICURN13). This participant argued that the absence of such practical exposure in nursing education leaves a significant gap in preparing future nurses for real-world scenarios.
Subtheme 2: Need for Practical Exposure
The gap in training also became apparent once nurses began working in the ICU. One participant admitted, “I never had experience taking care of anyone with intellectual developmental delays in nursing school. … It wasn’t until I became a nurse working that I really got to experience these patients” (ICURN7). They described the experience as “on-the-job training” (ICURN16) and shared how they encountered “severely challenged patients” for the first time, not through formal education but due to the proximity of their ICU to developmental care centers (ICURN3).
Subtheme 3: Impact of Knowledge Deficit
The lack of formalized IDD training not only impacted the nurses' confidence but also led to feelings of shame and self-doubt. A participant who felt their education was entirely self-initiated said, “The only reason why I have any education on it at all is because I made the decision to. I have been around these individuals all my life, and that’s where I got my education. Nothing from nursing school” (ICURN11).
Subtheme 4: Suggested Interventions
Many participants expressed a desire for nursing programs to address this gap. One nurse recommended, “We need some specialized training… it would be really nice to have some training because it takes a lot to take care of these patients… or honestly even integrating it into a nursing program would be amazing” (ICURN9). This sentiment captures a broader call for structural changes in nursing education to better equip nurses for the complexities of IDD patient care in ICU environments.
Theme 2: They Deserve Better
In Theme 2, They Deserve Better, ICU nurses expressed frustration over the lack of resources available for caring for patients with IDD. This theme revealed the struggle to provide adequate and compassionate care in an environment where necessary resources and support structures were missing or insufficient. Nurses described this deficiency as a significant barrier that left the patients and the care team underserved (see Figure 3). Main Theme 2 and subthemes.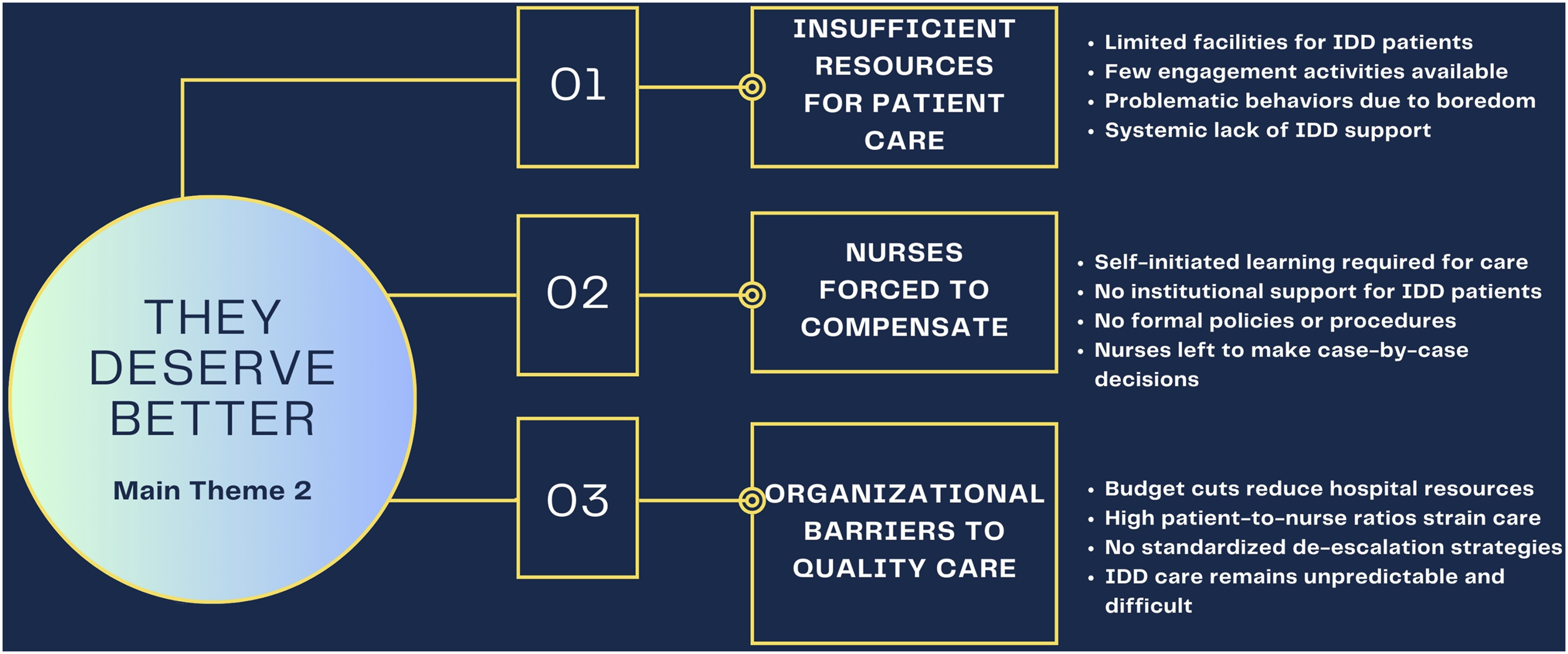
Subtheme 1: Insufficient Resources for Patient Care
One nurse highlighted the challenge of meeting the unique needs of IDD patients in a hospital with limited facilities, sharing, “We need more resources. At my hospital, we get a lot of these patients and not enough places to put them. They are basically stuck in a room with a TV only, trying to be entertained for days on end while we look for places for them” (ICURN20). The lack of appropriate activities or environments to engage and calm these patients often led to problematic behaviors, as when, “you give them toys and they may damage themselves with them, or you give them an iPad and they throw it across the room” (ICURN12). This lack of appropriate resources not only impacts the patients’ quality of life during their stay but also creates additional challenges for the nurses tasked with their care.
Another nurse, who had worked across multiple states as a traveling nurse, emphasized the widespread nature of this issue: “I work in West Virginia, and you often don’t see a lot of resources for patients with intellectual disabilities. That’s one area I think is lacking. … I’ve worked as a traveler also in a lot of different states, and honestly, I haven’t seen a lot of resources for caring for patients with intellectual disabilities” (ICURN4). This nurse’s perspective suggests a systemic lack of support across healthcare settings, not just isolated to specific institutions.
Subtheme 2: Nurses Forced to Compensate
Participants repeatedly expressed that they often had to rely on their own initiative to bridge this resource gap. One nurse noted, “Any research that you do by yourself on your own time. That’s basically all the resources you have” (ICURN17). Another reflected, “As a nurse, I feel like there are no resources I can pull outta my pocket that are actually something you can use to help your IDD patient and their family get through this. That is something that is also very much lacking” (ICURN19). These comments underline a sense of abandonment, as nurses must independently seek information and strategies, often without institutional support.
Despite years of experience, some nurses expressed that without adequate resources, managing the care of IDD patients remains a challenge. One nurse shared, “Our hospital doesn’t have a lot of resources… maybe if we had some de-escalation tips… it would be a little bit better. After all this time and experience, I thought I’d be better at it, but this patient population… they’re still a challenge to work with. They’re always different. It’s never like you can find one tactic that works for everybody” (ICURN6).
Subtheme 3: Organizational Barriers to Quality Care
Nurses also pointed out the lack of structured policies and procedures specifically for IDD patient care. “We have policies and procedures for 65 years and older patients with broken ribs on whether they need to be in the ICU. … I wish I had the knowledge and information to pull out actual policies and procedures that I could implement for this population because, right now, we have none,” ICURN5 explained. Without established protocols, nurses are left to make difficult decisions on a case-by-case basis, potentially compromising care quality.
Some participants indicated that budget cuts and high patient-to-nurse ratios further exacerbated these issues. One nurse explained, “Sometimes there are things that the hospital will offer, but I think it’s pretty limited. The hospital, because of the budgets, will be cutting staff and raising patient-to-nurse assignments…if you’re strung out with two critical patients and one of them is disabled, then you’ve got extra challenges to deal with… it’s rough” (ICURN18). This perspective illustrates the compounded difficulty in caring for IDD patients, as nurses feel stretched thin and unsupported by their institutions.
Theme 3: It Weighs on My Soul
For Theme 3, It Weighs on My Soul, caring for patients with IDD in the ICU presents not only clinical challenges but also deep emotional and moral burdens for nurses. This theme, It Weighs on My Soul, captures the psychological and ethical toll ICU nurses experience in this setting. Subthemes that emerged include the emotional impact of care, self-doubt, the development of experience, the need for detachment, and coping strategies for dealing with the distress associated with these patients (see Figure 4). Main Theme 3 and subthemes.
Subtheme 1: The Cumulative Effect Takes a Toll
In Subtheme 1, The Cumulative Effect Takes a Toll, nurses described the emotional weight of caring for IDD patients in critical conditions, where, despite their best efforts, some patients could not be saved. One nurse shared, “You see different kinds of patients, you try your best to save the patients, even on multiple drips, on multiple vasopressors. Sometimes there's really nothing you can do… they end up passing at the end of the day. So, sometimes it takes a lot” (ICURN1). Another nurse discussed the emotional toll when patients lack family involvement, sharing, “Sometimes I just feel empathetic with the patient 'cause like there's no one to do that for them in their toughest moments… it takes a toll but, I mean, that's what you sign up for. That's what I always tell myself. As ICU nurses, that's what we sign up for” (ICURN14). These reflections underscore the cumulative emotional burden and the mental preparation nurses must adopt to cope with these experiences.
Subtheme 2: Self-Talk of Self-Doubt and Shame
In Subtheme 2, Self-Talk of Self-Doubt and Shame emerged as a common response, especially in cases where nurses questioned their own abilities and decisions or faced undesired outcomes. One nurse admitted, “These patients, when they come in, are very sick patients, and you try everything to save them… sometimes, at the end of the day, they don’t end up passing away… and that helps you a lot. Other times, they do end up passing away, and you think, ‘Should I have done something different, or did I do enough to try to save this patient?’” (ICURN10). This reflection highlights how the intensity of ICU care, especially for vulnerable patients like those with IDD, often leads nurses to internalize outcomes, feeling personal responsibility for their patient’s survival.
Subtheme 3: Finding Purpose in the Experiences
In Subtheme 3, Finding Purpose in the Experiences
Subtheme 4: Detachment as a Protective Coping Mechanism
In Subtheme 4, Detachment as a Protective Coping Mechanism
Subtheme 5: Seeking Release by “Letting It All Out”
In Subtheme 5, Seeking Release by “Letting It All Out,” nurses reflected on various active coping strategies, such as seeking therapy and physical exercise, which also played a role in managing the emotional toll of this work. One nurse revealed, “I see a therapist and then I also, since I became a nurse, started working out a lot. I really use that as my stress relief to let all those emotions loose. It's really hard sometimes, but I mean, luckily, I have a mom who worked as a social worker and a boyfriend who lets me cry, but I know not everybody has that” (ICURN11). This statement reflects the importance of external support systems and healthy outlets for emotional release in helping nurses manage the stress inherent in their roles.
Subtheme 6: Witnessing Isolation and Disconnection
Nurses often encounter heartbreaking situations where IDD patients lack family support, and they are left alone in critical moments. One nurse explained, “A lot of them, the parents that are out of the picture or the state has taken over. … It’s really sad to see them kind of left on their own. Then when they get into critical situations… we have to make decisions with the medical directors rather than a parent… it has got to be very challenging for the parent, and for the child” (ICURN3). This reflection captures the sorrow nurses feel when they witness the social isolation faced by some IDD patients and the ethical complexities that arise in these cases.
Subtheme 7: Moral Agency versus Moral Distress
Some nurses reported feeling moral distress, especially when the treatment they provided felt ethically misaligned with the patient’s needs. One nurse shared, “I just do the best I can, and I work within my scope. I think there are a lot of ethical gaps there because I feel like treating them like I would treat anyone else… sometimes is cruel for them” (ICURN16). This insight reveals the ethical conflicts nurses face when attempting to balance professional standards with the perceived best interests of IDD patients, often resulting in inner turmoil.
Discussion
Synthesis and interpretation
Inductive analysis of the themes revealed that ICU nurses strongly preferred an ethics of care approach when managing the unique challenges of patients with IDD. Our findings align with Carol Gilligan’s feminist ethics of care framework, which emphasizes relational sensitivity, empathy, and the moral importance of addressing the needs of vulnerable individuals. 18 Nurses voiced frustration with their lack of training and institutional resources for IDD care, encapsulated in the theme If Only I Had Known More, which highlights their desire to provide more informed and compassionate care. The theme They Deserve Better underscores a commitment to equitable care for IDD patients despite systemic limitations, reflecting Gilligan’s call to recognize and act upon moral responsibilities in caregiving relationships. Finally, It Weighs on My Soul captures the emotional burden and moral distress experienced by ICU nurses, reinforcing the need for institutional support to maintain resilience and ethical practice.
The ethical challenges ICU nurses face when caring for IDD patients extend beyond general moral distress, highlighting critical gaps in patient autonomy, informed consent, and equity of care.6,8 Nurses in our study reported difficulties in consensus on when to supplement decision-making in IDD patients, especially when patients required but lacked a legal guardian or advocate. Without clear ethical guidance or institutional policies, nurses found themselves contributing to difficult choices about aggressive interventions versus palliative care for patients with IDD, revealing a significant gap in current ethical frameworks. These findings align with previous research on moral distress in ICU settings but provide a unique contribution by demonstrating how these ethical conflicts are intensified when patients have cognitive impairments that significantly limit communication and self-advocacy.6,19–23
Education and training deficiencies
Prior studies emphasize the importance of structured education and training in improving nurses’ confidence and competence in caring for IDD patients. However, research has consistently shown that nursing curricula lack adequate IDD-specific content, leading to knowledge gaps and feelings of unpreparedness in clinical practice.2,5 Our findings in If Only I Had Known More reinforce this issue, as ICU nurses described relying heavily on personal experiences rather than formal education. Helmers et al. highlighted that structured ethics debriefs and mentorship can reduce moral distress and enhance resilience, suggesting that similar strategies could be adapted to support IDD-related education in ICU settings. 24 Addressing these educational gaps is critical to ensuring that nurses feel equipped to navigate complex ethical decisions when caring for IDD patients. 6
Systemic barriers and institutional support
The theme They Deserve Better reflects systemic challenges in IDD patient care, consistent with previous studies identifying inadequate policies, staffing shortages, and a lack of standardized protocols as key barriers.6,16 Giannetta et al. emphasized the need for standardized ethical guidelines to mitigate moral distress, a finding our study extends by illustrating how these issues manifest uniquely in IDD care. 25 Nurses in our study frequently advocated for IDD patients to receive the same quality of care as neurotypical patients, challenging implicit biases within the healthcare system. Such advocacy efforts, while ethically necessary, often placed additional emotional burdens on nurses who felt unsupported by institutional structures. These findings highlight the need for targeted policy interventions to ensure equitable resource allocation and support ICU nurses in providing high-quality, ethically sound care for IDD patients.
Our findings also highlighted how inadequate staffing and institutional resources exacerbate these ethical concerns. Unlike previous studies that focus on moral distress in general ICU practice, our research identifies how these systemic barriers disproportionately impact IDD patient care.19,20,22 Nurses frequently expressed that without specialized training, support, and clear protocols, they were left to make ethically complex decisions without institutional guidance or support.
Emotional and ethical strain in ICU IDD care
The emotional toll of caring for IDD patients in high-acuity settings emerged prominently in It Weighs on My Soul. Nurses reported moral distress when standard ICU interventions were applied to IDD patients who struggled to communicate their needs without appropriate consideration of context and patient-specific needs. While previous research has explored moral distress broadly, our study uniquely highlights how ICU nurses perceive these interventions as conflicting with principles of dignity-centered and person-focused care.19–23 In some cases, nurses felt ethically compromised, forced to choose between patient safety and respecting autonomy in a system that lacked alternative or compensatory regulations.
Strengths and limitations
Reflecting on this study, the researchers identified several areas where different approaches could have enhanced the depth and breadth of insights gained. One key aspect that could have been explored further is end-of-life care for patients with IDD in the ICU. Asking participants more specific questions about their experiences with end-of-life care would have allowed the researchers to capture the unique ethical and emotional challenges that arise in these situations and understand how nurses navigate these sensitive moments with IDD patients and their families.
The researchers also recognize that asking more detailed questions about experiences with resuscitation for IDD patients may have provided valuable insights into the complexities of critical decision-making in high-stakes scenarios. Focused questions on these topics could have allowed participants to reflect on their moral and professional responsibilities when faced with resuscitation decisions. This is especially ethically relevant for patients with limited communication abilities or who lack an advocate. Consequently, this area of inquiry could shed light on the specific support and training nurses need to feel equipped and confident in handling resuscitation events with compassion and ethical integrity.
In future studies, the researchers would consider incorporating more structured prompts to explore these critical areas. Such an approach would provide a more comprehensive understanding of ICU nurses’ experiences and challenges, particularly around the ethical dilemmas associated with end-of-life and resuscitation care for IDD patients. Additional research can further inform initiatives to support nurses and improve care practices for this vulnerable patient population. 10
Nursing implications
For bedside nurses
Bedside nurses often experience moral distress when they feel underprepared to care for patients with IDD effectively. Limited exposure to IDD-specific training during professional education contributes to this lack of confidence, leading to increased stress and healthcare disparities for IDD patients. 26 Studies indicate that structured education and hands-on experience are critical for improving nurse competency and reducing emotional burden. 27 Practical tools, such as de-escalation techniques, structured communication strategies, and sensory-friendly care approaches, can enhance nurses’ ability to provide compassionate, individualized care to patients with IDD, ultimately improving patient outcomes and reducing stress for nurses. 23
Participating in training programs that include hands-on workshops, interactive case studies, and simulated clinical encounters can equip nurses with practical experience in managing the unique needs of IDD patients. 26 Engaging in mentorship opportunities with experienced nurses in IDD care can also further build confidence and skill proficiency, reinforcing a supportive learning environment. 27 Given the healthcare disparities and systemic barriers faced by individuals with IDD, expanding nursing education and professional development initiatives is essential to improving both patient care and provider well-being.26,27
For nursing educators
Nursing educators play a crucial role in preparing future nurses for the realities of caring for diverse patient populations. However, the absence of IDD-specific content in standardized nursing curricula contributes to health disparities and leaves nurses feeling unprepared to provide competent care.6,26 To bridge this gap, nursing programs should integrate IDD concepts into both theoretical and practical components of education, aligning with legislative frameworks and self-advocacy movements that emphasize equitable healthcare access. 26 Effective teaching strategies can include guest lectures, simulation-based learning that incorporates standardized patients with IDD, and hands-on clinical experiences in IDD-focused healthcare settings.3,7,26
Programs such as the Self-Advocates as Medical Educators–Family-Advocates as Medical Educators (SAME-FAME) model have demonstrated success in teaching nursing students about IDD care through direct engagement with self-advocates and caregivers.26,28 Partnerships with IDD advocacy organizations and campus disability resources can provide faculty with the tools needed to implement inclusive curricula. Additionally, nurse residency programs (NRPs)—evidence-based initiatives designed to help new graduate nurses transition from student to professional nurse—offer a structured platform for embedding person-centered IDD education and strengthening ethical decision-making skills. 29 Nursing educators can better equip students with the knowledge, skills, and confidence to provide safe, person-centered care to individuals with IDD by adopting these strategies. 26
For nurse leaders
Nurse leaders are well-positioned to advocate for systemic changes that enhance resources, training, and support structures for nurses providing care to individuals with IDD. Despite the growing recognition of health disparities in IDD care, major nursing organizations have yet to prioritize nurse-led models of care, leaving gaps in education, practice, and policy advocacy. 30 Nurse leaders should also push for dedicated staffing allocations for IDD care coordination, ensuring that specialized nurse-led models improve continuity and quality of care. Addressing the emotional strain on staff caring for IDD patients is crucial. Implementing well-being programs, emotional resilience training, and peer support groups can help reduce burnout and moral distress, ultimately improving staff retention and patient outcomes. 30 Nurse leaders can drive transformative changes in healthcare systems that prioritize equitable, person-centered care for individuals with IDD.26,30
For hospital organizations
Hospitals and healthcare organizations are responsible for providing structured resources and policies that support the care of patients with IDD. We propose this includes developing structured protocols, offering continuing education for staff, and conducting regular needs assessments. The development of standardized care plans for IDD patients could ensure consistency and quality of care across settings. Offering ongoing IDD-specific training for all healthcare providers, with incentives for participation, can increase caregiver engagement, confidence, and competency in caring for this patient population. Last, conducting needs assessments to identify gaps in IDD patient care and tailoring staff training accordingly will promote addressing organization-specific gaps and promote the efficiency and effectiveness of these efforts. Investing in these initiatives enhances patient safety and satisfaction while also improving staff morale and reducing turnover by addressing the unique challenges faced by nurses in IDD care.
ABILITY program
Successfully addressing the challenges faced by ICU nurses caring for patients with IDD requires targeted structural reforms, expanded nursing education, and the adoption of evidence-based initiatives. Several existing models demonstrate effective strategies for improving healthcare outcomes for this population. For example, Huber et al. describe the Adaptive Behavioral Intellectual/Developmental Disability Individualized & Integrated Tertiary Care for Youth and Children (ABILITY) program, a multidisciplinary, hospital-based care model designed to provide individualized, adaptive support for children and adolescents with IDD in a tertiary pediatric setting. 31 The program integrates developmental-behavioral and mental health expertise into inpatient, emergency, and outpatient services, drawing inspiration from adaptive care models and school-based multidisciplinary teams. Incorporating developmental pediatricians, psychiatrists, behavior analysts, nurses, and service coordinators allowed the ABILITY program to facilitate tailored care plans, reduce healthcare inequities, and enhance provider capacity. The success of this initiative highlights the urgent need for dedicated IDD hospital care teams. Establishing similar models in tertiary settings can enhance healthcare accessibility, improve patient safety, and ensure better outcomes for this population. 31
LEND and UCEDD training programs
Another promising approach involves leveraging the Leadership Education in Neurodevelopmental and Related Disabilities (LEND) and University Centers for Excellence in Developmental Disabilities (UCEDD) training programs to bridge existing gaps in IDD competency among healthcare providers. 30 These federally-funded initiatives focus on interdisciplinary training, clinical experience, and policy advocacy to enhance healthcare delivery for individuals with IDD. LEND programs equip healthcare professionals, including nurses, with advanced knowledge in neurodevelopmental disabilities, patient-centered care models, and leadership training. Similarly, UCEDD centers function as hubs for IDD research, education, and service innovation, collaborating with hospitals and universities to develop and disseminate best practices for IDD care. 30
For policymakers
Policymakers can contribute to improving IDD patient care by creating standards and funding initiatives that support specialized training across healthcare settings. One way to address such concerns is through legislative mandates, which would consist of establishing competency in IDD care as part of nursing licensure or continuing education requirements. Another method of addressing these concerns would be through incentivizing equitable care at an organizational level, consisting of encouraging hospitals to develop programs and resources for IDD care through funding and policy support. Finally, drawing from existing mandates for mental health training in nursing curricula as policy frameworks may assist in establishing comprehensive IDD competency requirements. Championing policies that empower education and training for individuals with intellectual and developmental disabilities can create access to equitable, high-quality healthcare. 32
Conclusion
The cumulative effect of these findings, along with current research, culminate in an urgent call for systemic changes in nursing education, resource allocation, and institutional support to better equip ICU nurses to care for IDD patients. Addressing these gaps can enhance patient outcomes and support nurses’ moral resilience and agency. Acting in these areas can allow nurses to fulfill their ethical obligations, resulting in enhanced professional quality of life for nurses and better patient outcomes for this vulnerable population.
Footnotes
Author contributions
Adrianna Watson—Original draft, review and editing, investigation, methodology, resources, supervision, funding acquisition, and conceptualization. Jeanette Drake—Original draft, review and editing, and resources. Matthew Anderson—Original draft, review and editing, and resources. Gabby Sutton-Clark—Investigation, review and editing, and resources. Sara Prescott—Investigation and resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding through the Myrtie Fulton Endowment Award from Brigham Young University.