
Abstract
Moral distress among nurses has been well examined within the literature since the concept’s introduction in 1984. Moral distress occurs when constraints result in an individual being unable to act or compelled to act against their professional moral obligations, resulting in a sense of complicity and wrongdoing. Extensive research has explored the experience and consequences of moral distress, particularly among bedside nurses. Despite an abundance of articles regarding moral distress in nursing, few examine the concept among nurse leaders. Leadership roles within nursing can be at the patient care, unit, middle, and executive levels. Existing evidence suggests that nurse leaders experience moral distress similarly to other nursing populations; however, their leadership roles introduce unique challenges and experiences. The purpose of this paper is to present a framework for understanding moral distress among nurse leaders grounded in existing theory and evidence. The Moral Distress Theory, Crescendo Effect, and Ecological Systems Theory served as theoretical frameworks. The conceptual framework was developed from 2022 to 2024 following literature review, empirical (qualitative) validation, and content expert review and validation (n = 5). The Conceptual Framework of Moral Distress Among Nurse Leaders consists of four primary elements: (1) nurse leaders as moral agents within a moral ecology, (2) antecedents of moral distress among nurse leaders, (3) physiological, psychological, and emotional effects of moral distress among nurse leaders, and (4) responsive action(s) versus inaction. This proposed conceptual framework may serve as a foundational understanding of moral distress experienced by nurse leaders and a guide for future moral distress research among nurse leaders.
Introduction
Nurses may serve in a variety of leadership roles, including, but not limited to, the level of patient care (e.g., Charge Nurse, Team Lead, Resource Nurse), unit-level (e.g., Unit Educator, Unit Manager, Unit Director), mid-level (e.g., Service Line Director, Assistant Administrators), and executive level (e.g., Chief Nursing Officer, Chief Executive Officer, Chief Quality Officer). Nurse leaders are urged to model ethical leadership within their units and organizations as a means to establish psychologically safe working environments for their staff and colleagues. 1 Sound ethical leaders may be better situated to address ethical challenges in practice. 2 One such ethical challenge impacting nurse leaders and their working environment is moral distress.
The term moral distress was first coined by Dr Andrew Jameton in his 1984 work, Nursing Practice: The Ethical Issues. 3 Jameton defined moral distress as arising “when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action” (p6). 3 Over the past 40 years, the concept of moral distress has evolved. It occurs when nurses or other clinicians face constraints that prevent them from taking ethically appropriate actions or force them to act against their professional obligations. This leads to a sense of complicity and wrongdoing.4–7 Moral distress is a recognized phenomenon clinicians face in practice. When left unaddressed, recent workforce studies suggest frequent and intense levels of moral distress are a factor associated with role dissatisfaction, unhealthy work environments, and decreased well-being among nurses. 8 Additionally, a longitudinal study conducted by the American Organization for Nursing Leadership and Joslin Insight revealed nurse leaders consider emotional health and well-being a top challenge impacting leadership practice and an area requiring support. 9
While moral distress has been well examined among bedside nurses, only recently have researchers begun to focus on how nurse leaders experience moral distress.10–25 Studies suggest nurse leaders experience moral distress comparatively to other nursing populations.20–22 Challenges and barriers associated with the leadership role have been identified as unique contributing factors of moral distress among nurse leaders.20–22 To date, a scoping review 19 and qualitative systematic review 20 examining the experience of moral distress among nurse leaders have noted the absence of a conceptual framework to guide research of moral distress within the nurse leader population. Despite increasing recognition of moral distress among nurse leaders, there is no existing conceptual framework to systematically examine and address this issue. This paper seeks to bridge this gap by presenting a framework grounded in both empirical evidence and theoretical models. This framework contextualizes the phenomenon of moral distress in the nurse leader population and may serve as a guide for future research.
Conceptual framework development
The Conceptual Framework of Moral Distress Among Nurse Leaders (Figure 1) was developed in three phases: (1) review of the literature and theoretical underpinnings, (2) empirical validation, and (3) content expert review and validation. The conceptual framework of moral distress among nurse leaders.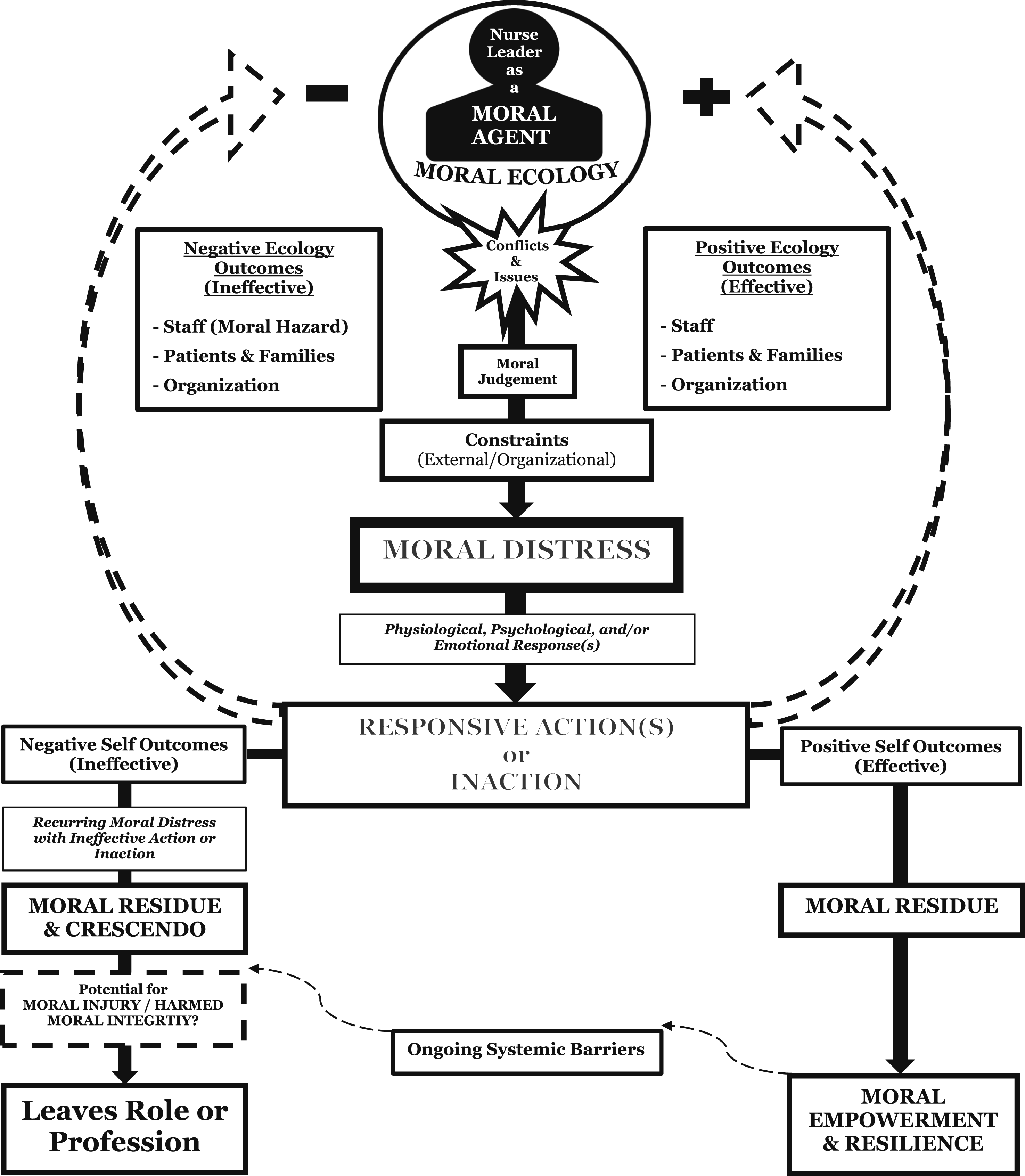
Phase 1: Review of the literature and theoretical underpinnings
A literature review was conducted in 2022 following a qualitative study 21 on unit-based critical care nurse leaders’ experiences with moral distress. This qualitative study unveiled that nurse leaders often experience moral distress when they are unable to alleviate the moral distress experienced by their staff. A qualitative systematic literature review 20 was then conducted and affirmed an evident gap in the examination of moral distress within the nurse leader population. While the search strategy was systematic and holistic, there were few resulting studies that met review criteria. Most of the studies identified were qualitative in nature and a systematic review of the qualitative literature was conducted. The findings of the review revealed that nurse leaders are often consumed by moral distress when little or ineffective organizational support exists and they often have to adapt to overcome moral distress. 20 The qualitative systematic review identified studies examining the experience of moral distress among nurse managers and executives, but no studies among unit-based nurse leaders. 20 Additionally, no prior article detailed a conceptual framework or model to guide future research of moral distress among nurse leaders. These findings from the literature were published in 2023 20 and, along with existing theories, informed the initial development of the Conceptual Framework of Moral Distress Among Nurse Leaders.
Corley’s Moral Distress Theory 26 was applied as an overall foundation of the framework in which the nurse leader is the central focus as the moral agent and the experience of moral distress is associated with an array of potential outcomes. These outcomes can have an impact on the leader individually and the system to which they work within. 26 Corley’s Moral Distress Theory 26 was further expanded upon by incorporating moral residue and the crescendo effect 27 as a potential consequence associated with the nurse leader’s experience of moral distress. These theoretical underpinnings were affirmed by both findings within the literature and a qualitative study conducted by the author and colleagues.
Moral distress theory
Corley’s Moral Distress Theory 26 has served as a framework for understanding a nurse’s experience of moral distress in the context of incongruencies between their internal environment (i.e., values and perceived obligations) and external work environment inhibiting the ability to advocate for patients. Corley’s framework 26 centers nurses as moral agents. As moral agents, nurses are often presented with morally and/or ethically challenging situations requiring action. 26 At times, a nurse’s perceived correct course of action may be hindered by constraints from the organization, other providers, patients, patient families, and/or society resulting in a moral conflict. 26 A nurse’s ability to navigate moral conflicts as a moral agent stems from their overall moral commitment, moral sensitivity, moral autonomy, and moral competency. 26 Corley theorized nurses with a higher level of moral commitment, moral sensitivity, moral autonomy, and moral competency are less likely to experience moral distress and more likely to experience moral comfort, the opposite of moral distress, when they are capable of having a moral intent to act coupled with the moral courage to challenge the constraining factor. 26 When nurses are unable to act due to a lack of moral courage or underdeveloped moral agency, they may experience moral distress, moral suffering, and moral residue. 26
Crescendo effect
The crescendo effect was introduced into the literature by Epstein and Hamric in 2009. 27 This model was developed to describe two crescendos experienced by clinicians, increasing moral distress and increasing moral residue. 27 Moral residue occurs as a result of lingering distress experienced after a morally problematic situation has ended. 27 As one’s baseline level of moral residue increases, higher crescendos can occur, evoking stronger reactions as one is reminded of prior morally distressing events. 27 The term moral residue was introduced by Webster and Bayliss to describe the moral compromise and betrayal that occurs following the experience of moral distress. 28 This betrayal results in moral injury, which encompasses the deep, lasting harm to a person’s moral integrity when they are unable to act in accordance with their ethical beliefs. As moral distress and moral residue build up due to repeated experiences of moral distress, negative personal and professional consequences can occur. 27 Such consequences may include moral numbing or blunting, conscious objection, and burnout. 27
Ecological systems theory and moral ecology
Bronfenbrenner describes the micro-, meso-, exo-, macro-, and chronosystems for which human behavior and development occurs through his Ecological Systems Theory. 29 The microsystem is the relationships between a person and their immediate setting (work, school, friends, family, and neighbors) and is the most influential on an individual. An individual both influences and is influenced by the microsystem. The mesosystem is the relationship between the microsystem’s settings which may have a direct impact on the individual. The exosystem is an extension of the mesosystem consisting of other social structures such as local government and mass media that can indirectly impact an individual. The macrosystem constitutes the societal structure and norms impacting cultural ideologies and social conditions an individual exists within. The macrosystem can have impacts within the micro- and mesosystems. Finally, the chronosystem describes the impacts of time and the influence on an individual’s development. To illustrate these relationships, a social-ecological framework can be developed.
Copeland adapted the Ecological Systems Theory to describe the various ways a nurse’s moral actions are influenced by the ethical systems in which the actions occur from the micro- to the macrosystem. 30 Copeland posits that a nurse’s moral agency is influenced by institutional or organizational objectives, the American Nurses Association Code of Ethics, medical/bioethics, normative ethics, and western philosophical thought. 30 These components constitute the moral ecology for which a nurse exists and has moral agency within. Ecological Systems Theory provides a valuable lens to understand how nurse leaders navigate moral distress within the broader healthcare system. By adapting Copeland’s moral ecology framework, the various ethical influences that shape nurse leaders’ experiences and responses to moral distress are recognized.
Phase 2: Empirical validation
The initial conceptual framework guided a qualitative descriptive study 22 examining the experience of moral distress among unit-based nurse leaders in the critical care setting conducted in the Summer of 2023. Institutional Review Board approval (Ref. No. EE202313) for this study was obtained from the University of Alabama in Huntsville prior to recruitment and data collection. The semi-structured interview questions were developed based on the initial conceptual framework, existing moral distress theories, and findings from the literature review. Ten unit-based critical care nurse leaders participated in the study. Data was analyzed using inductive thematic analysis. Findings were published in 2024 and revealed unit-based nurse leaders in the critical care setting may experience moral distress as a result of difficult end-of-life situations and barriers within the system. Additionally, findings suggested that unit-based critical care nurse leaders may experience negative physiological, psychological, and emotional responses to moral distress. 22 The findings from this study affirmed the initial conceptual framework.
Phase 3: Content expert review and validation
In August of 2023, Content experts (N = 6) were invited by the author to offer feedback and input on the framework. Ethical considerations for this phase were to include experts based on relevance to the topic of moral distress. Content experts were informed of the purpose of their review of the framework and notified that their contribution would be voluntary. Experts invited by the author to serve as content validators and who provided feedback agreed to be acknowledged for their validator roles as a means to promote transparency. The author would like to acknowledge that one of the content validators served as an external content expert on his dissertation committee.
The Conceptual framework of moral distress among nurse leaders
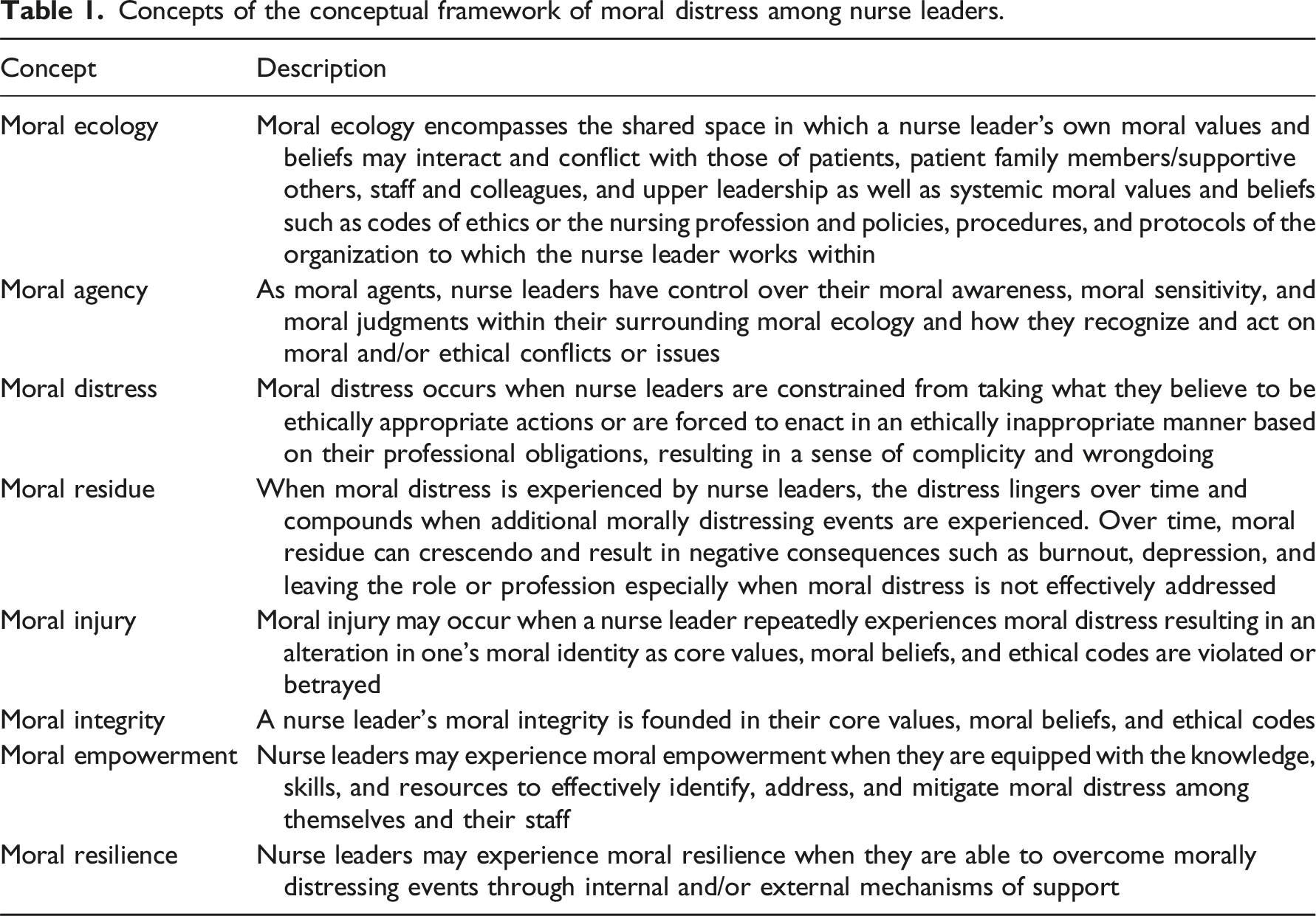
Concepts of the conceptual framework of moral distress among nurse leaders.
Nurse leaders as moral agents within a moral ecology
While nurse leaders function as moral agents, they must do so within their respective environment, or moral ecosystem. This moral ecosystem can be illustrated by an adaptation of the social-ecological framework (Figure 2). A nurse leader’s moral agency is influenced by their individual values, beliefs, knowledge, skills, and attitudes in conjunction with the established norms existing within their moral ecosystem. In this social-ecological model, nurse leaders and their associated moral agency form the individual level. Established norms are generated at the interpersonal/organizational (mesosystem), communal (exosystem), and societal levels (macrosystem) and are learned by the nurse leader through exposure, education, and/or practice. By framing the nurse leader acting as a moral agent within a broader moral ecosystem, the Conceptual Framework of Moral Distress Among Nurse Leaders accounts for these social structures influencing the moral agency and ethical practices of a nurse leader. These structures have an impact on and can be impacted by the nurse leader’s experience of moral distress and the associated response(s).20,22 Nurse leader moral ecosystem.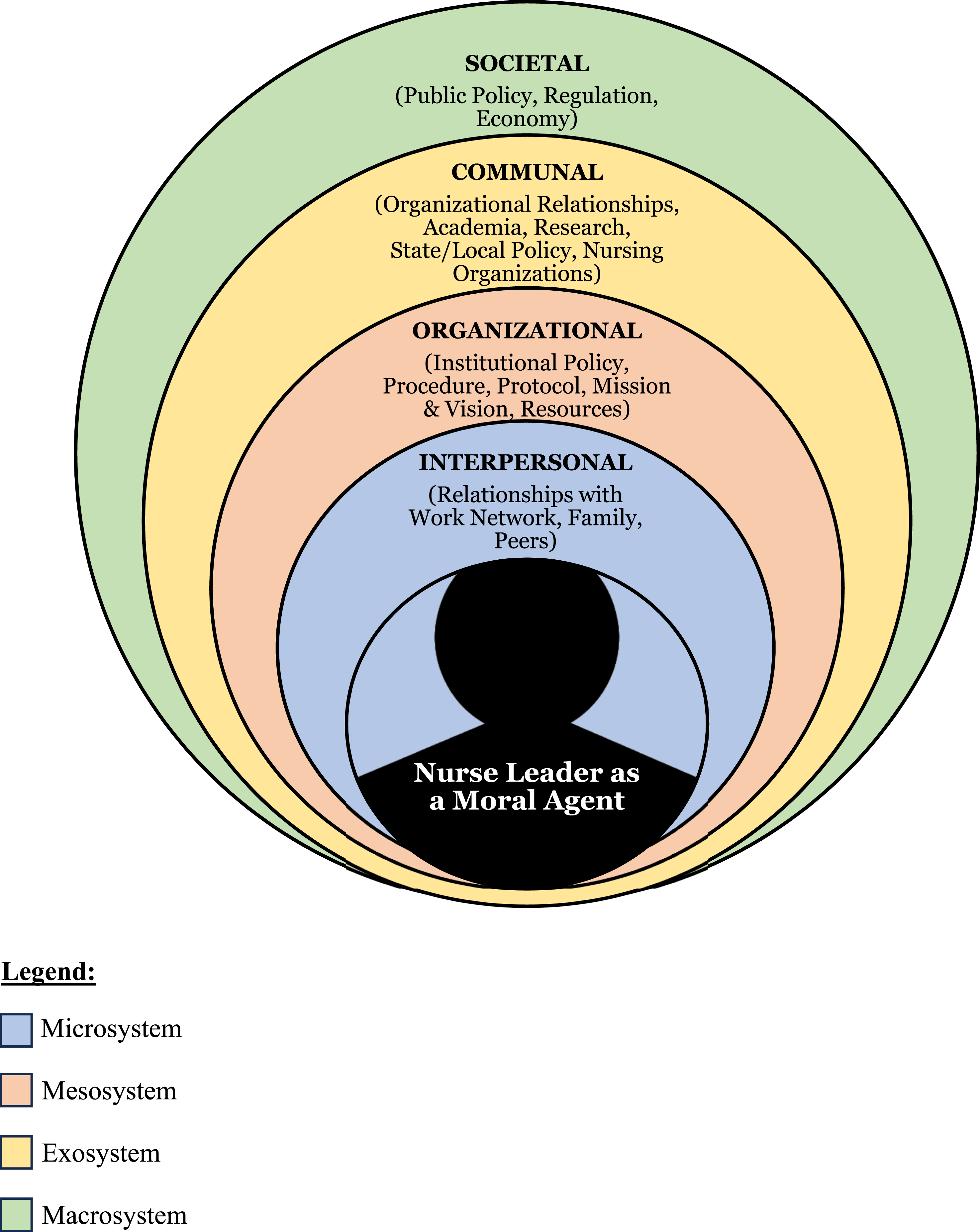
Antecedents of moral distress among nurse leaders
Moral distress in the nurse leader is precipitated by a conflict or issue to which the nurse leader makes a moral judgment they perceive as the correct action to take but are unable to take action as a result of personal, external, and/or systemic constraints. Constraining factors precipitating moral distress detailed within the literature review and the qualitative study include difficult end-of-life situations and systemic barriers.20,22 Difficult end-of-life situations contribute to moral distress when treatment goals are unclear among the healthcare team or when families and providers pursue futile care.20,22 Constraints arising from systemic barriers that cause moral distress among nurse leaders are an inability to address staff moral distress due to a lack of support systems within the organization, inadequate staffing and/or resources, powerlessness in the policy development and approval process, imbalanced hierarchies, poor teamwork and communication, unaddressed incompetence or unprofessionalism hindering the work environment and patient care, and lack of quality leadership training.20,22 Over time, constraints leading to moral distress can challenge and erode a nurse leader’s moral compass. 20
Physiologic, psychologic, and emotional responses to moral dsitress by nurse leaders
Nurse leaders who experience moral distress may consequently suffer physiologic, psychologic, and/or emotional effects. (1) (2) (3)
Because of moral residue and the crescendo effect, these responses to moral distress by the nurse leader can build up over time resulting in detrimental personal and professional consequences.20,22 A systematic review 20 highlighted a case in which a nurse leader’s moral distress led to hospitalization, with their physician recommending resignation from their leadership role. While moral distress is an unavoidable phenomenon in some situations, nurse leaders and organizations must be equipped with knowledge and skills to take action when moral distress occurs.
Responsive action(s) versus inaction
When nurse leaders experience moral distress, their response—or lack thereof—determines its long-term impact. Effective actions involve proactive interventions at both individual and organizational levels, whereas ineffective responses or inaction can exacerbate moral distress. Action or inaction can result in an array of outcomes for both the nurse leader and their work environment. Findings both from the literature review 20 and the qualitative validation study 22 suggest that ineffective action and inaction to address moral distress can result in nurse leader and staff turnover, organizational distrust, and decreased quality of patient care. Conversely, organizations that empower nurse leaders to address moral distress were able to mitigate the severe impacts of moral distress. 20 The effectiveness of a response determines the outcomes for nurse leaders, their teams, and the organization. Below, the distinct consequences of effective versus ineffective responses are explored.
Outcomes of effective action
Effective action by the nurse leader as a moral agent in conjunction with resources and support from the nurse leader’s institution may result in positive outcomes. These positive outcomes can manifest within the individual nurse leader, staff, patients and families, and/or the organization. Ultimately, the nurse leader may experience moral empowerment and/or moral resilience as a result of effective action while also noticing a positive impact within their moral ecology. Because the nurse leader’s experience of moral distress is often precipitated by their inability to adequately address the moral distress of their staff, effective action may have a global impact; thus, positively affecting the nurse leader’s moral ecology. Organizational resources noted to be beneficial in addressing moral distress by nurse leaders include ethics and moral distress consultation, employee assistance programs, and formal debriefing processes following morally distressing events.20,22 Nurse leaders may also seek personal resources to address and mitigate moral distress, to include informal debriefs with co-workers outside of work, conversations with friends and family, exercise, mindfulness, and spirituality.20,22 While organizational and personal resources can mitigate negative responses to moral distress, moral residue from the experience still remains; albeit not as severe. While effective coping mechanisms can mitigate moral distress, the persistence of unresolved ethical challenges contributes to moral residue, which can accumulate over time, potentially leading to moral injury.
Outcomes of ineffective actions or inaction
Even when action is taken, the resources or support available to the nurse leader may be inadequate to effectively address their moral distress or mitigate the precipitating factors. When action is ineffective or not taken, negative outcomes related to moral distress are enhanced. Without adequate support, recurring moral distress accumulates as moral residue. Over time, this unresolved distress may erode the nurse leader’s moral integrity, potentially leading to burnout, resignation, or moral injury. Further studies are needed to explore the relationship between moral injury and moral distress. The nurse leader’s moral ecology may also be negatively impacted due to leader turnover and retention, lack of effective leadership, and poor quality of care.20,22
Discussion
The Conceptual Framework of Moral Distress Among Nurse Leaders was developed over two and a half years through a systematic literature review, qualitative validation, and expert validation. This framework provides a comprehensive perspective on the moral distress experienced by nurse leaders, offering a structured approach to studying its causes, manifestations, and consequences. While nurse leaders serve in a variety of leadership roles at various levels, evidence suggests the factors and consequences associated with moral distress within this population are consistent across leadership levels. This framework provides a guide to support future research and education regarding the nurse leader’s experience of moral distress.
The Conceptual Framework of Moral Distress Among Nurse Leaders can be used as a guide to support the adaptation or develop of a tool to measure moral distress among nurse leaders. By providing a comprehensive depiction of moral distress and its consequences, this framework lays the groundwork for developing psychometrically sound measurement tools tailored to nurse leaders. Once a tool has been developed or adapted, further validation of the framework can be conducted by researchers to provide quantitative evidence to further support the framework. Previous studies have demonstrated the importance of adapting existing moral distress measurement tools to specific nursing roles. One such adaptation is detailed in a study by Ganz and colleagues. 10 In this study, Ganz and colleagues adapted the Ethical Dilemmas in Nursing (EDN) to be more specific and congruent with the nurse middle manager’s experience. 10 The Measure of Moral Distress for Healthcare Professionals (MMD-HP) 31 has yet to be adapted and validated among nurse leaders and may be a viable next step for researchers interested in moral distress within this population. A formal valid and reliable tool to measure moral distress among nurse leaders can aid the development and evaluation of interventions targeted at addressing moral distress within this population.
The Conceptual Framework of Moral Distress Among Nurse Leaders can inform the design and implementation of targeted interventions aimed at mitigating moral distress among nurse leaders across various levels, including individual, unit, departmental, and organizational structures. Researchers, implementation scientists, and clinicians interested in addressing moral distress among nurse leaders may find the framework beneficial in targeting interventions at multiple levels such as the individual, unit, department, or organizational level. Several interventions aligned with this framework have already been explored, including moral distress consultation services, 4 moral resilience and moral empowerment programs, 24 formal critical incident debriefing processes, 32 and ethics rounding. 33 Research is needed to evaluate the effectiveness of these interventions on addressing the moral distress of nurse leaders.
Furthermore, the framework may serve as a valuable education tool to prepare nurse leaders. Current evidence indicates that many nurse leaders lack adequate preparation to effectively manage moral distress in both themselves and their teams. This framework can be used by academics and clinicians alike to equip nurses and nurse leaders with the skills needed to navigate ethical challenges in leadership. Additionally, this framework may be beneficial for other professionals in leadership roles in which they oversee or collaborate with nurse leaders as it provides a holistic view on the impacts of nurse leaders experiencing moral distress within an organization. Programs such as the Clinical Ethics Residency for Nurses (CERN) 34 could integrate this framework into their curriculum to strengthen nurse leaders’ moral agency and ethical decision-making skills.
Limitations
A key limitation of this model is the absence of a validated quantitative tool specifically designed to measure moral distress among nurse leaders, which limits further empirical validation. While tools to measure moral distress exist, none have been specifically developed or validated for nurse leaders. Since the qualitative validation study 22 was conducted in a single state, additional research across diverse geographic regions is needed to confirm the framework’s applicability and identify potential refinements. As moral distress remains underexplored across different levels of nursing leadership, future research may reveal necessary refinements to the framework.
Conclusion
Moral distress is an inevitable challenge for nurse leaders, and when unaddressed, it can have significant negative consequences for both individuals and healthcare systems. Nurse leaders are challenged with intervening and addressing moral distress in practice; however, research on how nurse leaders personally experience and manage moral distress remains limited. The Conceptual Framework of Moral Distress Among Nurse Leaders establishes a theoretical foundation for understanding moral distress among nurse leaders, integrating existing theories and empirical evidence. The framework may benefit researchers seeking to further explore the experience of moral distress by nurse leaders and/or develop tools or interventions to measure and address moral distress among nurse leaders. Future research should focus on validating this framework among nurse leaders and exploring its applicability to other healthcare professionals in leadership roles. Additionally, developing reliable tools based on this framework will be essential for measuring and addressing the moral distress of nurse leaders in practice.
Footnotes
Acknowledgments
The author would like to extend his gratitude to Dr Elizabeth Epstein, Dr Lucia Wocial, Dr Micah Hester, Dr Alissa Swota, and Dr Dawn Bourne for their expert review of and feedback on the Conceptual Framework of Moral Distress Among Nurse Leaders. The author would also like to thank his Doctoral Dissertation Chair, Dr Jennifer Bail, and Committee, Dr Elizabeth Epstein, Dr Todd Smith, Dr Miranda Smith, and Dr Teresa Welch for their support on the work leading up to this framework.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.