
Abstract
Background
Ensuring that mothers and newborns receive respectful care is crucial to providing high-quality care. Our research aimed to describe the care received by neonates and identify risk variables for Disrespect and Abuse (D&A) in neonates.
Methods
We carried out a comprehensive analysis of published, quantitative research on D&A on newborns. The databases of SCOPUS, Web of Science, PubMed, Embase, ProQuest, and Cochrane Library were thoroughly searched for articles. The quality of the research was assessed using the STROBE measures. Studies meeting certain requirements were eligible for inclusion: they had to evaluate the prevalence and risk factors associated with the mistreatment of newborns after childbirth; finally, 525 potentially relevant articles were carefully reviewed, and only 10 were ultimately selected.
Result
Six prospective cohort studies, one retrospective cohort study, two cross-sectional studies, and one mixed-method research comprised the 10 papers that made up this review. In included studies infants had experienced at least one D&A episode. We have divided them into two categories: indicators of disrespect and factors affecting disrespect. Indicators of disrespect were the major contributing factor to D&A. According to this review, some maternal and newborn factors contributed to the D&A of newborns: preterm births, female deliveries assisted by an instrument, rural births, mothers living in rural areas, births with parity greater than 2, and unmarried birth mothers.
Conclusion
Health systems must be confident that no neonate is denied medical care due to family socio-economic and cultural factors. This study can inform future research around interventions for improving policy and practice.
Introduction
Prioritizing the care of mothers was the main emphasis of the respectful maternity care agenda until recently 1 ; however, as attention to newborn care increased, the agenda started to grow. 2 A declaration on the prevention and elimination of disrespect and abuse during facility-based delivery was produced by the World Health Organization in September of 2017. 2 The 2019 edition of the Respectful Maternity Care Charter included provisions pertaining to infant rights, including the right to birth registration and the prohibition against needless separation from mothers or relatives. 3 The percentage of births that take place in medical facilities has increased significantly over the last 20 years, yet the rate of decline in maternal and newborn mortality has not slowed down. According to World Health Organization information sheets from 2021, 47% of all fatalities in children under five occurred during the newborn era, an increase from 40% in 1990. Sub-Saharan Africa has the greatest rate of newborn fatalities worldwide, with 27 deaths per 1000 live births, followed by southern Asia, which has 23 deaths per 1000 live births. 4 Infants have the right to warmth, feeding, and protection from harm and illness. It is imperative that all infants are provided with essential neonatal care, which is of the utmost importance during the initial days following delivery. Therefore, it is imperative to ensure that women and infants receive superior care that takes into consideration their rights, requirements, experiences, and preferences in order to achieve both national and Sustainable Development Goal (SDG) objectives. However, a growing body of data demonstrates a variety of hazardous and disrespectful treatments given to infants, such as holding or slapping the infant upside down, suctioning the airway without a need, and placing the blame for the infant’s poor result on the mother.5,6 A basic human right, respectful care is violated when it is manifestations of mistreatment of women during labor, including physical and verbal abuse, discrimination based on maternal age (young or elderly), and ethnicity or social class the provision of care without consent, obstructing the presence of a birth companion, and withholding food during labor without the woman’s consent or a clinical indication7,8 consistently provided at medical facilities. 9 As a consequence of these traumatic experiences, some women, particularly the most vulnerable, such as impoverished mothers and teens, may inadvertently abuse the infant, which leads to disrupting the establishment of a healthy psychological start with the newborn. 3 Therefore, D&A is a red flag for low-quality care and has profound implications for trust in health systems more broadly. 7
There is currently no consensus on which neonatal care practices might be classified as mistreatment. However, practices can be observed that do not meet WHO recommendations for quality neonatal clinical care. A limited but increasing body of research indicates that infants are not always provided courteous, evidence-based care.10,11 Recently, several studies have reported evidence of disrespect and abuse of infants. 12 There have been instances of babies being left alone, being taken from their mothers too soon after delivery, 13 and having their parents' permission not to move them to another facility. 8 Additional allegations have included the discrimination against newborns with congenital diseases or abnormalities, the dangerous early release of women and their babies owing to space constraints, and the denial of postnatal care due to financial hardship.8,14 These practices might also constitute violations of human rights standards.
In addition to, the effects of disrespectful care by medical staff on mothers will have a negative impact on their behavior with newborns. If the dignified care training program is implemented well, it will become a culture in that community in the long run. Ultimately, a culture of dignity will be formed in that society, improving the quality of obstetric and neonatal care. 10
Evidence about the effects of respectful care on the health, well-being, and care-seeking behaviors of mothers and babies is required to influence program implementation, policy, and advocacy, in addition to the need for changes in the quality of care received by these groups of people throughout the intrapartum period. To offer evidence for future research, hospital-level intervention, and policy advocacy for respectful newborn care (RNC), our research aimed to describe the care received by neonates and identify risk variables for Disrespect and Abuse (D&A) in neonates. This finding provided a detailed description of the elements that contribute to and impact the provision of considerate infant care.
There were no results for any current or planned research to identify variables related with respect and D&A among infants by health care providers from a search of the Cochrane Library and PROSPERO.
Review Methods
Following a procedure (available from the authors), we carried out this review in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 15
Eligibility criteria
Studies meeting certain requirements were eligible for inclusion: they had assessing the prevalence and risk factors associated with mistreatment of newborns after childbirth; they had to be original studies published in an English-language peer-reviewed journal; and they had to be designed with the intention of care providers or parents inquiring or observing newborns receiving respectful or disrespectful care immediately after birth or postpartum care.
Excluded content included protocol studies, brief reports, comments, editorials, short communications, review articles, and non-full-text papers. Research that was specifically addressed home births, had a poor quality score, had traditional birth attendants during labor, or had an uncertain delivery site were all disqualified from consideration.
Search strategy
“Infant, Newborn” OR “Newborn Infant” OR “Newborn Infants” OR Newborns OR Newborn OR Neonate OR Neonates
“Culturally Competent Care” OR “Culturally Congruent Care” OR “Culturally Competent Health Care” OR “Cross-Cultural Care” OR “Cross Cultural Care” OR “Cultural Care” OR “Culturally Sensitive Care” OR “Culturally Sensitive Cares” OR Disrespectful OR disrespect OR abuse OR abusive OR respectful OR Respect OR “Personal Respect” OR Dignity OR “maternity care” OR “maternity cares” OR Obstetrics OR “Quality of Health Care” OR “Health Care Quality” OR “Quality of Healthcare” OR “Healthcare Quality” OR “Quality of Care” OR “Care Quality” OR “Pharmacy Audit” OR “Pharmacy Audits” OR “Quality of care” OR MNCH OR “maternal health” OR “Maternal Health Services” OR “Maternal Health Service” OR “health services” OR “health service” OR “Newborn care” OR “Newborn cares”
Caregivers OR Caregiver OR Carers OR Carer OR “Care Givers” OR “Care Giver” OR “Spouse Caregivers” OR “Spouse Caregiver” OR “Family Caregivers” OR “Family Caregiver” OR “Informal Caregivers” OR “Informal Caregiver” OR midwife OR midwives OR Midwifery OR “Traditional Birth Attendant” OR “Traditional Birth Attendants” OR “nurse midwifes” OR “nurse midwife” OR “Nurse-Midwives” OR “Nurse-Midwife” OR “Nurse Midwives”
To systematically retrieve publications without date constraints, electronic databases including SCOPUS, Web of Science, PubMed, Embase, and Cochrane Library were searched from the time of their creation until February 2024.
Study selection
The eligibility of the studies was evaluated separately by two reviewers. Two reviewers (SH and SM) manually screened the article titles and abstracts according to the inclusion and exclusion criteria. The reviewers separately examined the complete texts of possible articles as well. All authors (SH and SM and MI) were unanimous. Ten studies were included after they were evaluated in comparison to the qualifying criteria.
Quality assessment
A modification of the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) criteria was used to assess the quality of the quantitative studies. The 22-item STROBE checklist included the following topics: participant characteristics, eligibility requirements, technique of variable assessment, summary measures outcome events, and discussion of causes of bias and/or imprecision.
Data extraction and analysis
Two reviewers independently retrieved the findings from the included papers using a standardized approach. Information on the population and research parameters (author publication year, sample size, inclusion criteria, setting, country, data collection, and contributing variables) were included in a summary of results.
Qualifications for inclusion
The study included quantitative studies of primary data, including reports on indicators that fall under the category of newborn disrespect and abuse, reports on contributing factors, reports on the quality of care related to the abuse and disrespect of newborn and reports on any type of abuse or disrespect
Qualifications for exclusion
Research published in languages other than English were excluded, and studies could not access the whole text. Determining the types, manifestations, and causes of neonatal maltreatment and disrespect was the main goal of this research; finding contributory variables was the secondary goal.
Ethics
This study was a part of the research PhD thesis, which was approved by the Ethics Committee of the Research Deputy at Ahvaz Jundishapur University of Medical Science (approval code: IR.AJUMS.REC.1403.200).
Result
Study the selection and qualities
Database searches conducted online produced 8525 citations. Using a methodical process, 8061 of the returned studies from this scan were eliminated for the following reasons: 2522 were eliminated as duplicates, 5478 were rejected because their titles and abstracts were inappropriate, and 61 were reviewed and 165 were protocol and 89 were guideline 201 were home birth and 5 were traditional birth attendance and 4 were brief reports (Figure 1). PRISMA (2020) diagram for searching resources.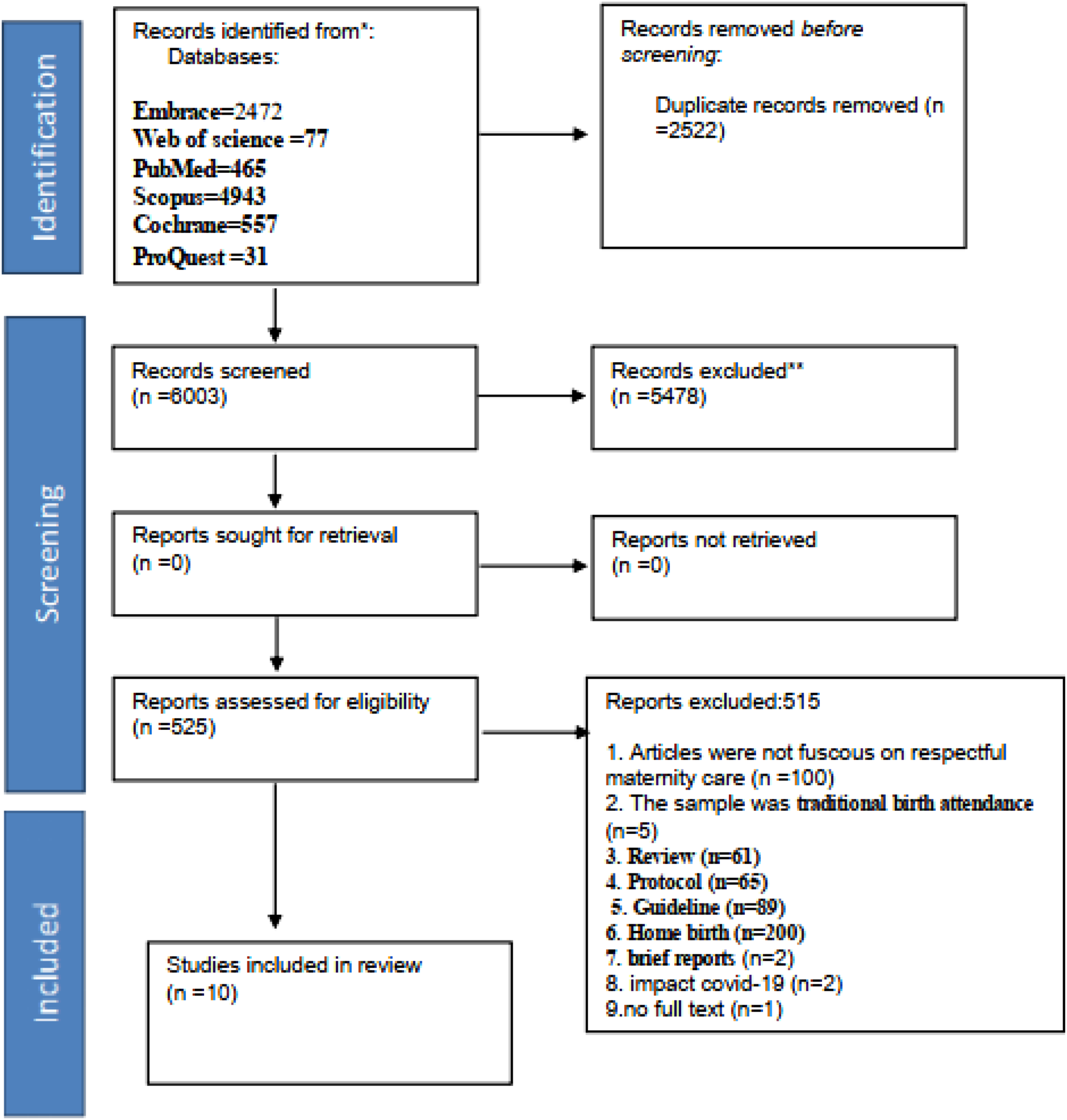
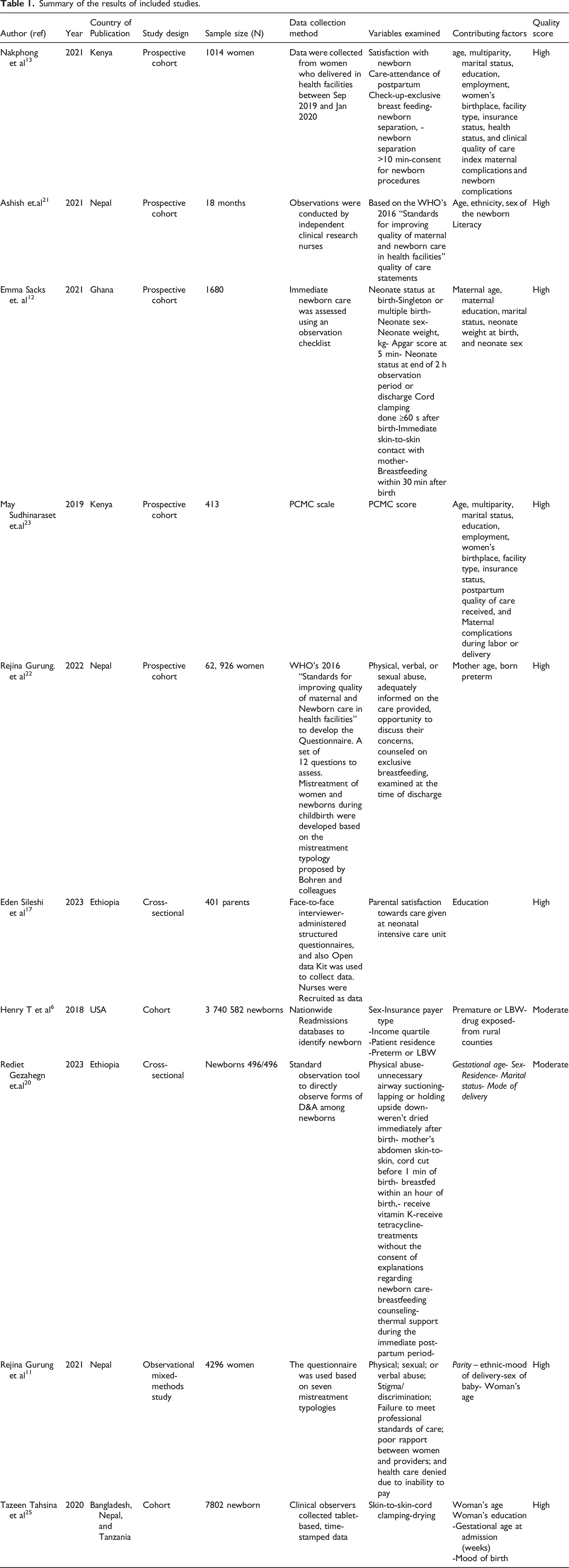
Six prospective cohort studies, one retrospective cohort study, two cross-sectional studies, and one mixed-method research (in which only quantitative data was employed) comprised the 10 papers that made up this review.
Summary of the results of included studies.
Composite results
According to prevalence data from research, between 18.5% 17 and 91.8% 21 of babies encounter at least one kind of disrespect and maltreatment during labor. There are high rates of care provider mistreatment. We have divided them into two categories: indicators of disrespect and contributing Factors to Disrespect and Abuse. A more detailed explanation of each is given below.
Indicators of disrespect of neonatal care
Indicators of Disrespect of Neonatal Care includes Physical violence, Neonate separation from the mother after birth, Medical interventions without obtaining consent from the parents, and Insufficient explanations regarding newborn care.
Physical violence
Physical violence was experienced by 41.1% 23 of newborns in Kenya and in the form of unnecessary airway suctioning (23.2%) in a cohort study in Nepal, 22 or slapping or holding upside down in a cohort study conducted in the USA (33.5%). 6
Neonate separated from mother after birth
According to four observational studies conducted in Bangladesh, Nepal, Tanzania, Kenya, and Ethiopia, lone mothers were more likely to separate from their newborns without a medical reason.11,20,23,25
Medical interventions without obtaining consent from the parents
In a prospective observational cohort study conducted in Nepal, 63.0% (95% CI, 62.5–63.5) of neonates had medical procedures done on them without their parents' permission. Of them, 21.4% (95% CI: 20.9–21.8) were suctioned without needing medical attention. 21 According to an observational study conducted in Nepal, 80.4% of caregivers were not given enough information before administering care. 11 In a cohort study in Nepal, 59.9% of parents said that their newborn’s operations did not get their permission. 22 Furthermore, according to cohort research conducted in the USA, over half of the women said they were never asked for permission before having any procedures done on their babies. 6 In another research conducted in Addis Ababa on directly observed childbirth care, the authors found that all neonates with problems (69/69) were treated without the parents' or caregivers’ permission. 20
Insufficient explanations regarding newborn care
In a research conducted in Addis Ababa on directly observed childbirth care, 93.6% of parents/caregivers didn’t receive explanations regarding newborn care, while the lack of breastfeeding counseling and thermal support during the immediate post-partum period was 87.3%. 20 Furthermore, according to cohort research in the USA. Based on parent experience and interpretation, 93.6% of parents did not get explanations on infant care. 6 A cross-sectional study in Ethiopia reported that within an hour of delivery, 77.6% (95% CI, 77.1–78.1) of the infants in the study were not breastfed. 20 The authors of an observational study conducted in Nepal found that 57.9% of women were not given advice about exclusive breastfeeding. 11 73.7% (n = 46,376) of mothers in Nepalese research said that they had not received advice on newborn danger indicators. 21 However, research in Ethiopia found that 31.4% of parents did not have access to the knowledge they needed to care for their infant. 17 34.9% of newborns in another study were not nursed within 1 hour. 6
According to cohort research by Tahsina et al. in Kenya, the percentage of women who started nursing after an hour was startlingly low (10.9, 95% CI 3.8–21.0 overall). 13 However, according to a single survey in Nepal, 96% of women expressed satisfaction with nursing technique advice. 22
Unmet need for timely and accurate care
The research in this section demonstrated the need of prompt, evidence-based treatment for babies from medical professionals. Therefore, statistics are required to guide measures taken by the health system to close gaps as well as by healthcare providers’ practices.
Immediate skin-to-skin contact with the mother
In quantitative section of a mixed method study conducted in Nepal showed that babies born by cesarean had a 98% decrease in the odds (an OR = 0.02, 95% CI, 0.01–0.05) of receiving skin-to-skin contact than those with vaginal births. 11 According to observational research in Addis Ababa, 9.1% were not positioned skin-to-skin on the mother’s tummy. 22 In a cross-sectional study conducted in Ethiopia, authors found that skin-to-skin contact was less prevalent (1048 [64·4%]). 20 According to observational research conducted in Ghana, just 3.5% (95% CI, 3.2–3.8) of the babies were maintained in skin-to-skin contact in the delivery room after birth. 12 However, in Pokhara, Nepal, only 18.7% (95% CI, 17.6%–19.9%) of women said that they initiated skin-to-skin contact with their baby immediately after birth. 11
Cord clamping done ≥60 seconds after birth
For the majority of Ethiopian newborns (1493 [91·8%] of 1627), delayed cord clamping was performed. 17 According to observational research in Addis Ababa, 71.7% (95% CI, 71.2–72.3) of infants clamped their cords later than expected. 22 In another research conducted in Kenya, 73.5% of respondents rated delayed cord clamping as fair or unsatisfactory. 13 Another research conducted in Addis Ababa showed directly observed childbirth care. 61.7% had their cord cut before 1 minute of birth. 20
Not dried immediately after birth
In another research, 29.0% of the drying was rated fair or poor. 13 In a different research, the authors found that 42.3% of the newborns were not properly wrapped with a clean, dry towel right after delivery. 6
Lack of breastfeeding within an hour of birth
In research conducted in Addis Ababa on directly observed childbirth care, 34.9% weren’t breastfed within an hour of birth. 20
Contributing factors to disrespect and abuse
This review examined the elements that contribute to disrespect and maltreatment towards infants, drawing on studies on caregivers' experiences as well as parents' experiences and interpretations.
Maternal contributing factors
This section examines the maternal contributing factors in providing disrespectful care by the health care providers, with the following results expressed under the subtheme:
Maternal education
Lack of maternal knowledge was linked to a higher chance of newborns not obtaining the recommended breastfeeding practices, according to research based on the experiences of mothers in Kenya.22,23 Compared to full-weight neonates, neonates with low birth weight (<2.5 kg) were more likely not to initiate nursing on demand in a cross-sectional study conducted in Ethiopia. 20 However, in an observational study conducted in Nepal, all women reported receiving breastfeeding counseling. 11 In the other study conducted in southern Ethiopia, The finding of the study showed that agreement with the availability of necessary information using direction indicators was significantly associated with parental satisfaction. 17
Maternal ethnic groups
Maximum variance in abuse was seen among babies born to mothers from relatively poor ethnic groups (chhetri) and infants born to women who had given birth to two or more children, according to a research done in Nepal. 20
Maternal age
Three studies were conducted in Addis Ababa. They directly observed childbirth care. Compared to babies born to mothers who were 18 years of age or younger, those born to women who were 35 years of age or older and those born to women who were 30–34 years old showed reduced signs of maltreatment.20,22,23
Mothers’ residence
Mothers who live in rural regions are more likely to experience disrespect and abuse from healthcare personnel, according to observational research done in Addis Ababa, USA, and Kenya.6,17,22 According to a cohort study conducted in Kenya, neonates whose mothers live in rural regions are more likely to experience physical abuse (AOR = 1.97; 95% CI: 1.22–3.20). 23
Single mothers
According to research done in Addis Ababa, Kenya, Ghana, Guinea, and Nigeria, children of single mothers were more likely to experience mistreatment and abuse at the hands of medical professionals.6,12,22,23 According to an observational study in Ghana, Guinea, and Nigeria, babies born to single mothers had a greater risk of physical abuse (AOR = 2.77; 95% CI 1.26–6.06). 12
Time of antenatal care visits
Observational research carried out in G Addis Ababa, Ghana, Guinea, Ethiopia, Kenya, and Nigeria included mothers who did not obtain prenatal care (ANC) visits more than four times had a greater risk of physical abuse.6,13,16,24 (AOR = 2.37; 95% CI: 1.42–3.96). 13
Mood of delivery
According to Gurung research carried out in Nepal, kids delivered by cesarean had a 98% lower chance (aOR = 0.02, 95% CI, 0.01–0.05) of having skin-to-skin contact compared to babies born vaginally. 10
Inability to pay hospital cost
Rejina Gurung’s research from Nepal revealed that throughout the postpartum period, n = 944 newborns were denied treatment because they were unable to pay. 21 According to observational research done in the USA, the highest risk factor for experiencing an abuse hospitalization was not being able to pay hospital expenses (aRR 3.17; 95% CI: 2.75–3.66). 6
Mother experienced physical abuse
According to a multicountry, observational study carried out in Ghana, Guinea, and Nigeria, when women experienced physical abuse from providers within 1 h before childbirth, their neonates were more likely to be slapped compared with women not experiencing physical abuse, (AOR 1∙9, 1∙1–3∙9). 12
Newborn contributing factors
The results of this section’s reflection on the newborn’s role in disrespectful care are grouped under the subtheme.
Neonate sex
According to cohort research done in Guinea and Nigeria, female neonates had a higher chance of mistreatment than male newborns (β, 0.016; p-value, 0.015).17,20 Also, cohort research carried out in Addis Ababa by Gezahegn et al. found a higher likelihood of contempt and mistreatment towards female neonates by healthcare workers (AOR = 2.01; 95% CI: 1.37–2.95). 6
According to cohort research done in the USA, there was a 1.2 CI (1.08–1.36) higher chance of maltreatment of female babies compared to male neonates. 6 Also, in cohort research conducted in Bangladesh, Nepal, and Tanzania, female babies were more likely to experience physical abuse (AOR = 2.01; 95% CI: 1.37–2.95). 25
Gestational age of newborn
Based on the experiences of mothers in Addis Ababa, Ghana, Guinea, Ethiopia, Nigeria, and the United States, the research revealed that preterm and instrumentally delivered babies were more likely to face mistreatment and abuse (18–16). 20 Preterm neonates had a greater incidence of physical abuse, according to the authors reported in a cohort study carried out in Ghana (AOR = 2.02; 95% CI: 1.11–3.69). 6
Drug exposed
According to cohort research done in the USA, neonates exposed to drugs had a higher risk of misuse hospitalization (aRR 2.86; 95% CI: 2.15–3.80). 6
Birth defect
According to research done in the USA, having any kind of birth abnormality raised the risk (aRR 1.5; 95% CI: 1.1–2.0). 6
Discussion
This comprehensive analysis discovered that many newborns are often subjected to cruel and disrespectful care in the included studies. The purpose of this review research was to identify risk variables for D&A in neonates.
This practice’s characteristics and manifestations vary according to studies: Contributing Factors to Disrespect and Abuse, not dried right away after delivery, Closing the cord ≥60 seconds after delivery skin-to-skin touch with the mother right away, the need for prompt care, inadequate justifications for infant care, after delivery, a newborn and its mother were separated by violence. The number of prenatal care visits, the newborn’s sex, the mother’s domicile, her marital status, the manner of delivery, and the newborn’s race were all very important contributing variables to the disrespect and maltreatment of infants.6,17,20
According to a recent study, mothers who are illiterate or have low levels of education are more likely to experience separation from their newborns (17=16). Single mothers and those who live in rural areas are also more likely to experience this kind of separation. Respect for all women and their babies may be ensured via the eradication of gender-based discrimination and the advancement of female education and health literacy. Additionally, compared to newborns of normal weight, neonates with low birthweights were less likely to be nursed on demand in the first few hours of life. 17 All newborns have the right to be nursed as soon as possible after delivery, including those with low birth weights who can do so. Low birthweight neonates should get extra assistance for breastfeeding, start as soon as feasible, and have frequent feedings, according to the WHO Nurturing Care Framework. 25
Furthermore, women who experienced physical abuse in the hour immediately before childbirth were more likely to have their neonates slapped. Maternal mistreatment might be related to discrimination, low health literacy, or lack of empowerment in the face of unequal power dynamics, which might extend to their neonates. Elimination of gendered discrimination, as well as promotion of female education and health literacy, can help ensure a more respectful environment for all mothers and their infants. 15
According to WHO guidelines, essential newborn care (ENC) should be given as soon as possible after delivery. This includes drying the baby right away, starting skin-to-skin care early, delaying cord care, starting breastfeeding as soon as possible, and giving vitamin K and tetracycline. 26
This investigation did, however, find a deficit in the availability of certain ENC components.6,13,24 Discrimination and insufficient health literacy may be linked to the newborn’s removal from the mother in the absence of medical need. Parental stress is brought on by this separation, which also has detrimental effects on breastfeeding and mother-infant bonding. 24 Respectful infant care is believed to revolve on allowing newborns to have immediate skin-to-skin contact. 27 However, compared to babies delivered vaginally, cesarean babies had lower skin-to-skin initiation rates. In certain clinical crises and situations when general anesthesia is necessary, delaying the start of skin-to-skin care may be justified, but for most babies, this constitutes a serious gap in care. 9 To guarantee that all infants get the care they require, an effort must be made by all parties involved to expand the availability of high-quality ENC services. Potentially dangerous infant care procedures covered in this review research comprised a broad variety of primary studies,6,11,17,20 including regular airway suctioning, shaking or slapping, and holding the baby upside down. Due to conflicting data on their advantages or disadvantages, the WHO now advises against using them.26,28
Our results indicate that three clinical perinatal disorders, including preterm and low birth weight (LBW), intrauterine medication exposure, and medical complexity, have been linked to an increased risk of physical abuse.29–31 There are limited legal options for mothers who believe they or their newborns have been subjected to physical assault or mistreatment. 32 In order to better providing care to newborns, health personnel will need to undergo training.
Future research should focus on: 1. The majority of research done to far has been descriptive; in order to both prevent and lessen instances of maltreatment, like those being developed to address abuse of mothers, should be created and assessed for those that target neonates. 2. In order to determine the effects of D&A on the health result of babies, implementation studies will be necessary. 3- Standardized instruments must be created in order to measure inconsiderate neonatal care 4. In addition, study is required to comprehend the expectations and desires of families and women about facility-based newborn care procedures.
This review highlighted several recommendations:
1-Evidence-based care must be implemented, and pre- and in-service trainings must demonstrate respectful infant care. 2. It should be possible for providers to get the most recent guidelines and recommendations. Improved pre-service and in-service clinical training might address some of the behaviors that were still seen in this research, even though there was evidence against them. Examples of these practices include holding the neonate upside down or by their leg, or rubbing them with alcohol. 3. In order to empower healthcare professionals and improve health policies, it is critical to identify the stressors that they face and how they could be mistreated. 4. Reducing mistreatment towards newborns based on maternal and newborn characteristics will require training on medical ethics and implicit bias. 5. It is necessary to create efficient strategies to lower D&A in neonates. 6. In order to provide a family-centered model (FCC) of newborn care, policies that guarantee that a newborn never be separated from its mother or father from the moment of birth onward, early skin-to-skin and Kangaroo Mother Care, and parental involvement in the care and decision-making process during the newborn’s hospital stay are all necessary. These care delivery models will contribute to the achievement of universal health coverage, equality, and dignity of care via an effective and responsive health system. They also fit in well with the WHO quality of care framework. Hospital rules and the culture of care to be altered, and provider and parent education is necessary for the effective implementation of FCC. Implementing the achieving the Baby Friendly Hospital Initiative accreditation is essential to ensure quality of maternity care received by mothers and families, regardless of their social, economic, race and religious background.
Strengths
This study is the first of its kind, according to an assessment of the literature on the disrespectful treatment of babies. To the best of our knowledge, it is the first D&A contributing element for neonatal care. We carried out a comprehensive analysis of published, quantitative research on D&A and its effects on newborns worldwide. Future research on possible therapies may benefit from these data. The eligibility of the studies was evaluated separately by two reviewers, which reduced bias in the selection of articles.
Methodological limitations
1. Although the research was conducted in different contexts, the smaller number of studies from Asia and Latin America compared to Africa may have an impact on generalizability. 2. There might have been observer-reported bias, especially when the caseload for births was high, possibly resulting in fewer observations and detection of mistreatments. 3. Given that the results of the included studies differ or are heterogeneous in terms of design and implementation methods, some are questionnaire-based, and others are observational, these issues can affect interpretation of the results. 4. The observational instruments had limitations when it came to monitoring newborn care practices since its primary function in the included studies was to quantify abuse of women after delivery. 5. This study presents important multicountry evidence on respectful/ disrespectful neonatal care practices in health facilities and links these practices with maternal and provider perceptions of care. While the extent to which one feels mistreated might be dependent on cultural norms and individual expectations, data presented here are observational, some of which might be considered mistreatment by women and families, or it may not be considered mistreatment due to the caregivers' ignorance.
Conclusion
This research offers a critical analysis of the many forms of disrespectful infant care practices that take place in medical facilities and identifies the contributing elements, such as indicators of disrespect, maternal or neonatal contributing characteristics, that lead to disrespectful care given by healthcare professionals. Neglect of newborns may be associated with maltreatment of their mothers in terms of comprehension care. This review adding new insights to physical care and attention to the infant’s respect as an independent human being. The unique requirements of women during delivery must be taken into consideration by health systems and caregivers, and it must be mandatory to enact regulations that mandate the norm of respectful infant care. Improved pre-service and in-service clinical training might address some of the behaviors that were still seen in this research, even though there was evidence against them. Cost-effective interventions (such as skin-to-skin contact and continued breastfeeding) should be implemented routinely for all neonates after birth. Improving care at delivery and the early postnatal period is essential to achieving the 2030 objectives for reducing avoidable infant deaths.
Footnotes
Acknowledgments
The authors wish to express their gratitude to the reviewer comments. Also, we are grateful of the ethical committee of Ahvaz Jundishapur University of medical science provided support this research.
Author Contributions
S.H designed the study. Analyzed the data: S.H, S.M. Wrote the first draft of the manuscript: S.H, S.M. Contributed to the writing of the manuscript: S.H, S.M. Conducted the title and abstract screening: SH.SM.MI Conducted the full text screening and data extraction: S.H, S.M, MI Conducted the quality assessments: S.H, S.M, M.I. Assessed the confidence of the review findings: S.M, M.I.. Supervision: MI. SM. Agree with the manuscript’s results and conclusions: S.H, S.M, M.I. A librarian at the University of Ahvaz Jundishapur medical science provided support with the database search (MZ).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
All relevant data are given within the manuscript.