
Abstract
Background
Moral distress is a pervasive challenge in nursing practice, adversely impacting nurses’ well-being, career development, patient safety, and organizational performance. Ethical climate, as a modifiable organizational factor, plays a pivotal role in mitigating moral distress. Understanding the association between nurses' moral distress and ethical climate is critical for clinical practice, management, and policymaking.
Aim
The aim was to systematically assess the association between nurses’ moral distress and ethical climate.
Methods
A systematic review and meta-analysis was conducted based on a comprehensive search of ten databases (PubMed, Cochrane Library, Embase, Web of Science, CINAHL, PsycINFO, Scopus, Chinese Biomedical Literature Database, China National Knowledge Infrastructure, and WANFANG) from inception to December 27, 2024. Two reviewers independently screened studies, extracted data, and assessed methodological quality. Correlation coefficients were synthesized using random or fixed-effects models. Subgroup analyses and meta-regression were performed to explore sources of heterogeneity.
Ethical considerations
Ethical approval was not required as the review synthesized publicly available data.
Results
Thirty-one studies involving 7635 nurses were included. Meta-analysis identified a moderate negative association between overall moral distress and ethical climate (r = −0.49, 95% CI: −0.59 to −0.38), and between moral distress frequency and ethical climate (r = −0.37, 95% CI: −0.45 to −0.28). Moderator analyses indicated that participant characteristics (gender composition, age, and work experience), study characteristics (sampling methods and ethical climate measurement tools), and working settings contributed to heterogeneity.
Conclusion
This systematic review and meta-analysis demonstrated a moderate negative association between nurses’ moral distress and ethical climate. Variations in participant demographics, study methodologies, and working settings partially accounted for the observed heterogeneity. Future research should employ larger, more diverse samples and longitudinal designs. Strengthening the ethical climate is essential for alleviating nurses’ moral distress and enhancing organizational effectiveness.
Introduction
Moral distress has emerged as a pervasive and pressing issue in contemporary healthcare, particularly among nurses who often operate at the frontline of complex ethical decision-making. As healthcare systems evolve and medical technologies advance, professionals increasingly encounter situations where they recognize the ethically appropriate course of action yet are constrained from acting accordingly.1,2
The construct of moral distress was first conceptualized by Jameton 3 as the experience of knowing the right action in a moral situation but being unable to act due to external constraints. Subsequent scholars have refined this concept: Wilkinson 4 emphasized the psychological disequilibrium caused by moral constraint, while Crane et al. 5 highlighted the inner conflict arising when actions or omissions violate deeply held ethical beliefs. More recently, Kim et al. 6 redefined moral distress as the experience of the moral emotion agent-regret, triggered by involvement in care-related events perceived as tragic or unjust, where alternative actions are precluded by structural barriers. Despite these definitional nuances, there is a broad consensus that moral distress fundamentally involves a violation of moral agency under institutional or systemic constraints. 7
It is important to distinguish moral distress from general workplace distress. Whereas workplace distress stems from organizational stressors such as workload, lack of autonomy, or interpersonal conflict, 8 moral distress is inherently rooted in ethical conflict. It arises when healthcare providers are compelled to act against their ethical convictions, for example, by implementing non-beneficial treatments under family or institutional pressure. 9 This distinction underscores the ethical specificity of moral distress and its profound implications for moral identity and professional integrity.
The antecedents of moral distress are multifactorial, spanning patient, nurse, organizational, and systemic levels. At the patient level, nurses may experience moral distress when required to provide invasive or futile interventions at the insistence of families. 10 At the nurse level, inadequate ethical training, low confidence in clinical decision-making, and role ambiguity contribute to susceptibility. 11 Organizational factors include rigid hierarchies, limited authority, unsupportive leadership, and bureaucratic obstacles. 12 At the systemic level, the absence of robust legal or institutional frameworks often leaves nurses vulnerable in ethically ambiguous situations. 13
The consequences of moral distress are substantial. Individually, moral distress is associated with psychological outcomes such as anxiety, emotional exhaustion, and sleep disturbances.14–16 Professionally, it is linked to diminished work engagement, burnout, turnover intentions, and erosion of professional identity.9,17 Organizationally, moral distress contributes to reduced care quality, communication breakdowns, and increased absenteeism, ultimately compromising patient safety and organizational productivity. 18
Among healthcare professionals, nurses are particularly vulnerable to moral distress, partly due to their limited decision-making authority within hierarchical medical structures.19,20 Nurses working in high-intensity specialties, such as oncology and intensive care, frequently report elevated levels of moral distress when navigating end-of-life decisions, ethical conflicts with families, or tensions between patient advocacy and organizational constraints.21–23
A growing body of research highlights the critical role of ethical climate, defined as the shared organizational perceptions of ethically appropriate behavior, 24 in shaping the experience of moral distress. A positive ethical climate fosters ethical dialogue, collaborative decision-making, and respect for individual values, 25 and has been associated with reduced moral distress and enhanced job satisfaction. 26 Conversely, a negative ethical climate, characterized by limited ethical support, policy ambiguity, and punitive culture, exacerbates moral distress and suppresses ethical voice.27,28
Despite increasing recognition of this association, empirical findings remain inconsistent. While several studies have reported a significant inverse relationship between moral distress and ethical climate,18,26,29,30 others have found no clear association.31,32 These discrepancies may stem from methodological variations, contextual factors, or unmeasured moderating variables. Drawing on prior research,33–35 we identified participant characteristics (e.g., gender composition, age, and work experience), study characteristics (e.g., country, continent, sampling method, and measurement tools), and working settings as potential moderators.
To date, no comprehensive systematic review and meta-analysis has synthesized the available evidence to clarify the association between moral distress and ethical climate among nurses. The present review addresses this gap by quantitatively summarizing the correlation between moral distress and ethical climate through meta-analytic techniques. Specifically, this review aims to: (1) determine the magnitude and direction of the association, (2) identify sources of heterogeneity through moderator analysis, and (3) provide evidence-based recommendations for nursing leadership and health policy to foster ethically supportive work environments.
Methods
Design
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The review protocol was registered with PROSPERO (CRDXXX).
Search strategy
A comprehensive literature search was conducted across ten databases: PubMed, Cochrane Library, Embase, Web of Science, Scopus, CINAHL, PsycINFO, Chinese Biomedical Literature Database, CNKI, and WANFANG Data. These databases were purposefully selected to ensure a wide search breadth, disciplinary relevance, and language inclusivity. Core biomedical databases such as PubMed, Embase, and the Cochrane Library were included due to their extensive indexing of high-quality clinical and health research, which is essential for capturing robust evidence on moral distress and ethical climate in healthcare settings. Multidisciplinary databases, including Web of Science and Scopus, were selected to extend coverage to broader academic domains such as ethics, psychology, and organizational behavior. CINAHL and PsycINFO were chosen for their specialization in nursing and psychological sciences, both of which are central to the constructs of interest in this review. Furthermore, three major Chinese-language databases, CNKI, WANFANG Data, and the Chinese Biomedical Literature Database, were incorporated to capture research conducted in China, a country with a substantial nursing workforce and distinct sociocultural contexts influencing ethical practice. The inclusion of these databases was also supported by the research team’s Chinese-language proficiency and familiarity with regional healthcare systems. To enhance comprehensiveness and identify potentially unpublished or non-indexed studies, Google Scholar was used to search for gray literature. The search covered studies from the inception of each database through December 27, 2024. A combination of Medical Subject Headings (MeSH) and free-text keywords related to “nurse,” “moral distress,” and “ethical climate” was applied. The complete search strategy is provided in Supplemental Table 1.
Eligibility criteria
Inclusion criteria: (a) Population: Registered nurses, licensed practical nurses, nursing staff, or assistants. (b) Outcome: Studies reporting a correlation (r) between nurses’ moral distress and ethical climate. (c) Design: Quantitative or mixed-methods studies with extractable quantitative data. (d) Language: English or Chinese.
Exclusion criteria: (a) Studies with <50% nurses or without separate analysis for nurses. (b) Inaccessible full texts or insufficient data. (c) Qualitative studies, editorials, abstracts, or reviews. (d) Duplicate publications.
Study selection and data extraction
All records were imported into EndNote V.21 for de-duplication, and then screened using Rayyan. 36 Two reviewers independently screened titles, abstracts, and full texts in a blinded fashion. Discrepancies were resolved through discussion or by consulting a third reviewer. Extracted data included study characteristics, sample demographics, measures used, and statistical results.
Quality appraisal
The methodological quality of included studies was assessed as follows: For quantitative studies, the AHRQ quality checklist 37 was used, scoring studies from 0 to 11: low (0–3), moderate (4–7), and high (8–11) quality. 38 For quantitative components of mixed-methods studies, the Joanna Briggs Institute (JBI) tool for cross-sectional studies 39 was applied and rated similarly: low (0–3), moderate (4–6), and high (7–8).
The appraisal team consisted of five graduate nursing students with formal training in evidence-based practice. Two reviewers (KXX and CCY) were randomly selected to independently evaluate study quality. Inter-rater reliability was calculated using Cohen’s kappa coefficient: values <0.20 (poor), 0.21–0.40 (fair), 0.41–0.60 (moderate), 0.61–0.80 (good), and 0.81–1.00 (very good). 40 Disagreements were resolved through discussion with a senior reviewer (YLZ), a professor with over 17 years of research experience.
Statistical analysis
Meta-analyses were conducted using R (v4.3.1). Correlation coefficients (r) between moral distress and ethical climate were transformed to Fisher’s Z scores for analysis and back-transformed for reporting with 95% confidence intervals (CIs). Effect sizes were interpreted as small (|r| < .30), moderate (|r| = .30 – .50), or strong (|r| > .50). 41
Heterogeneity was evaluated using the I2 statistic: no (0%–25%), low (25%–50%), moderate (50% – 75%), and high (>75%) heterogeneity. 42 A fixed-effects model was used when I2 ≤ 50% and p > .05; otherwise, a random-effects model was applied. 43 Subgroup analyses and meta-regression were conducted to explore potential moderators, and sensitivity analyses assessed the robustness of results. Publication bias was examined via funnel plots and Egger’s regression tests. Meta-analyses can yield reliable estimates with as few as 10–20 studies, depending on heterogeneity and effect size variance. 44
Results
Search results
A total of 2387 studies were initially identified through electronic databases and Google Scholar. After removing duplicates and screening titles and abstracts, 131 studies were retrieved for full-text review. Ultimately, 31 studies met the inclusion criteria. Figure 1 illustrates the literature search and selection process. PRISMA flow diagram of the literature search process.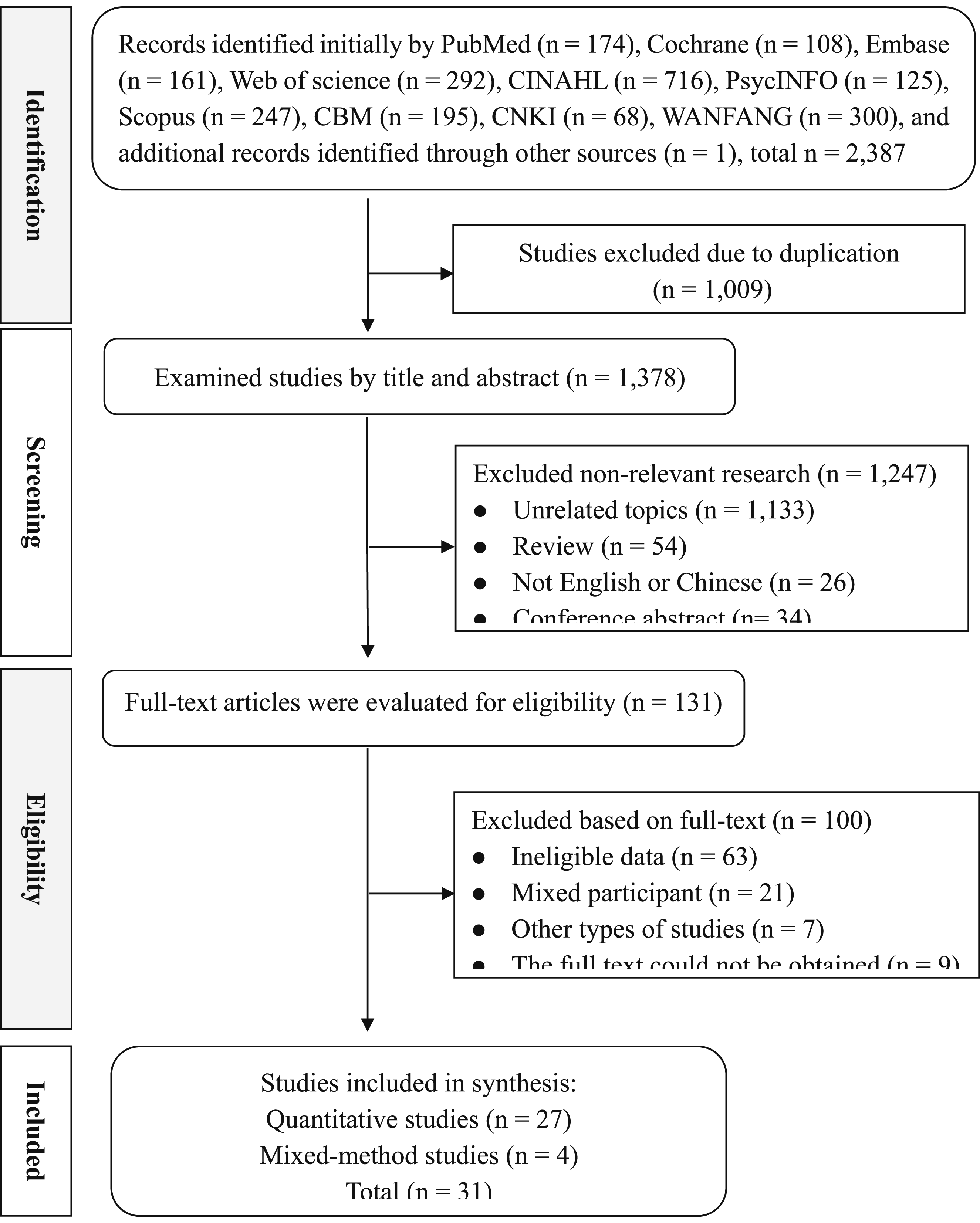
Study characteristics
The 31 studies included 27 quantitative and 4 mixed-methods designs, published between 2005 and 2024, spanning 14 countries. The majority were conducted in the United States (K = 12),18,29,30,45–53 followed by China (K = 5)35,54–57 and Egypt (K = 3).58–60 All quantitative studies and the quantitative components of mixed-method studies employed a cross-sectional design, with only 3 studies adopting random sampling methods.32,58,61
In total, these studies involved 7635 nurses, with females comprising 67.5% of participants. The mean age ranged from 27 to 45.56 years. 9 studies included participants with an average work experience of at least 10 years.29,45,47,49,51,52,59–61 Nurses worked primarily in intensive care units (ICU; K = 19),18,26,31,32,45,47–52,55,57,59,60,62–65 pediatric units (K = 7),29,50,60,62,66–68 oncology wards (K = 5),50,54,66–68 and acute care settings (K = 4).35,47,51,61
The most commonly used measures for moral distress were the Moral Distress Scale-Revised (MDS-R, K = 10),30,31,35,45,54–59 the original Moral Distress Scale (MDS, K = 7),32,48,49,51,60,61,68 and the Measure of Moral Distress for Healthcare Professionals (MMD-HP, K = 6).18,26,29,47,50,63 Ethical climate was predominantly assessed using the Hospital Ethical Climate Scale (HECS, K = 17).29,31,32,35,45,47,48,50–53,55–58,60,61
Characteristics of the included studies.
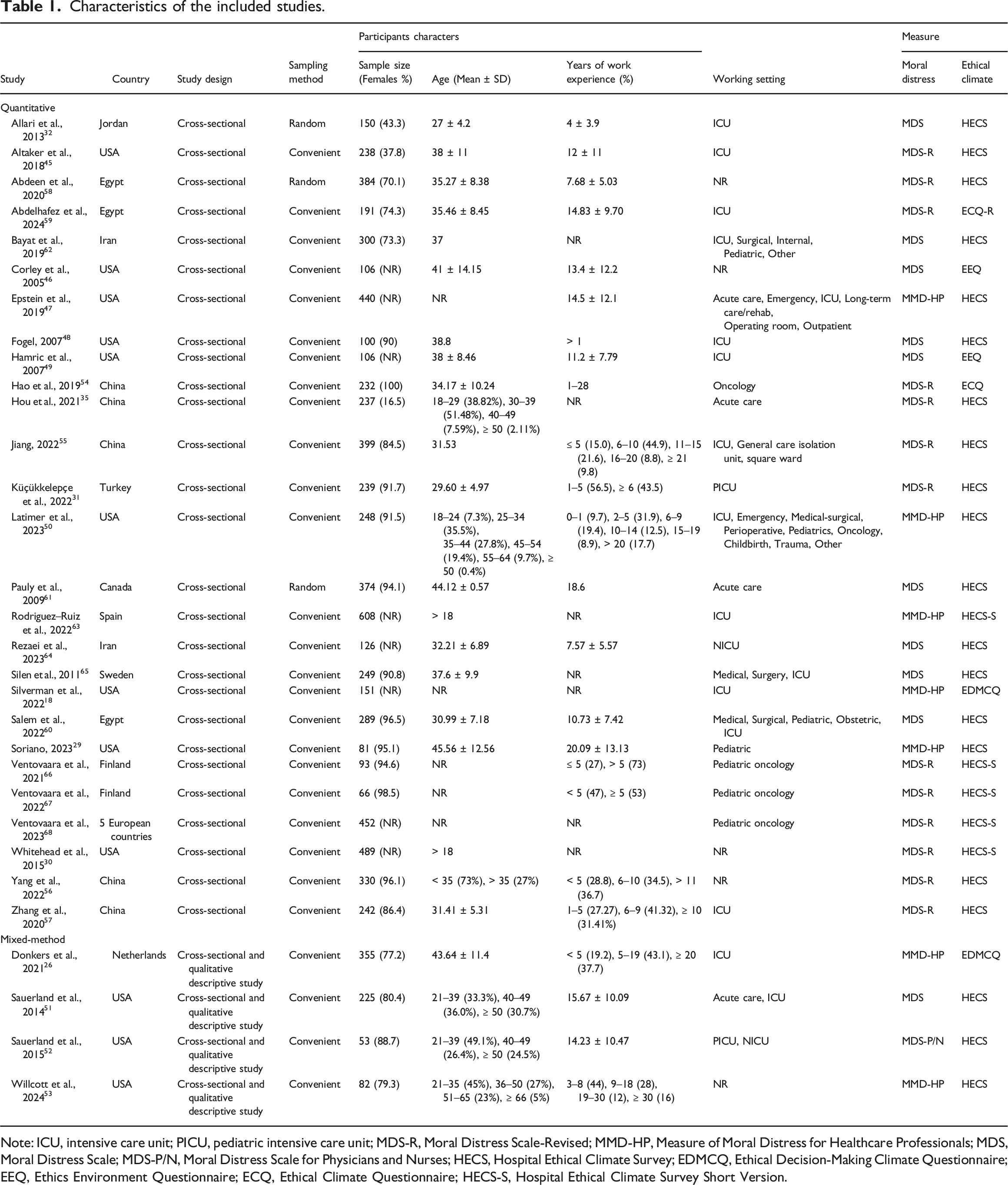
Note: ICU, intensive care unit; PICU, pediatric intensive care unit; MDS-R, Moral Distress Scale-Revised; MMD-HP, Measure of Moral Distress for Healthcare Professionals; MDS, Moral Distress Scale; MDS-P/N, Moral Distress Scale for Physicians and Nurses; HECS, Hospital Ethical Climate Survey; EDMCQ, Ethical Decision-Making Climate Questionnaire; EEQ, Ethics Environment Questionnaire; ECQ, Ethical Climate Questionnaire; HECS-S, Hospital Ethical Climate Survey Short Version.
Quality assessment
The methodological quality of all 31 studies was assessed. The average Cohen’s kappa was 0.82 for the AHRQ checklist and 0.91 for the JBI checklist, indicating very good agreement.
Among the quantitative studies, 18 (66.7%) were rated as moderate quality, while 931,32,45,48,50,55,59,66,68 achieved high-quality ratings. The 4 mixed-methods studies were rated as moderate quality.
For the quantitative studies, the most frequent methodological limitations were the failure to control for confounding variables and inadequate handling of missing data. In the mixed-methods studies, the main concern was the failure to identify and address confounding factors. Detailed results are provided in Supplemental Tables 2a and 2b.
Meta-analysis
Among the 31 studies included in this review, 25 examined the association between overall moral distress and ethical climate, while 10 studies further analyzed the relationships of ethical climate with either the frequency or intensity of moral distress.
Of the 12 studies that explicitly investigated the directionality of this relationship, 10 conceptualized ethical climate as an exogenous variable influencing moral distress. These studies consistently reported that a more positive ethical climate was associated with lower levels of moral distress. In contrast, 2 studies48,56 proposed a reverse relationship, indicating that higher levels of moral distress may negatively shape nurses’ perceptions of the organizational ethical climate.
Association between overall moral distress and ethical climate
Twenty-five studies, involving a total of 6696 participants, reported correlations between overall moral distress and ethical climate. The pooled analysis showed a moderate negative association, with r = −0.49 (95% CI: −0.59 to −0.38, p < .0001) (Figure 2). Forest plot of the association between moral distress and ethical climate among nurses.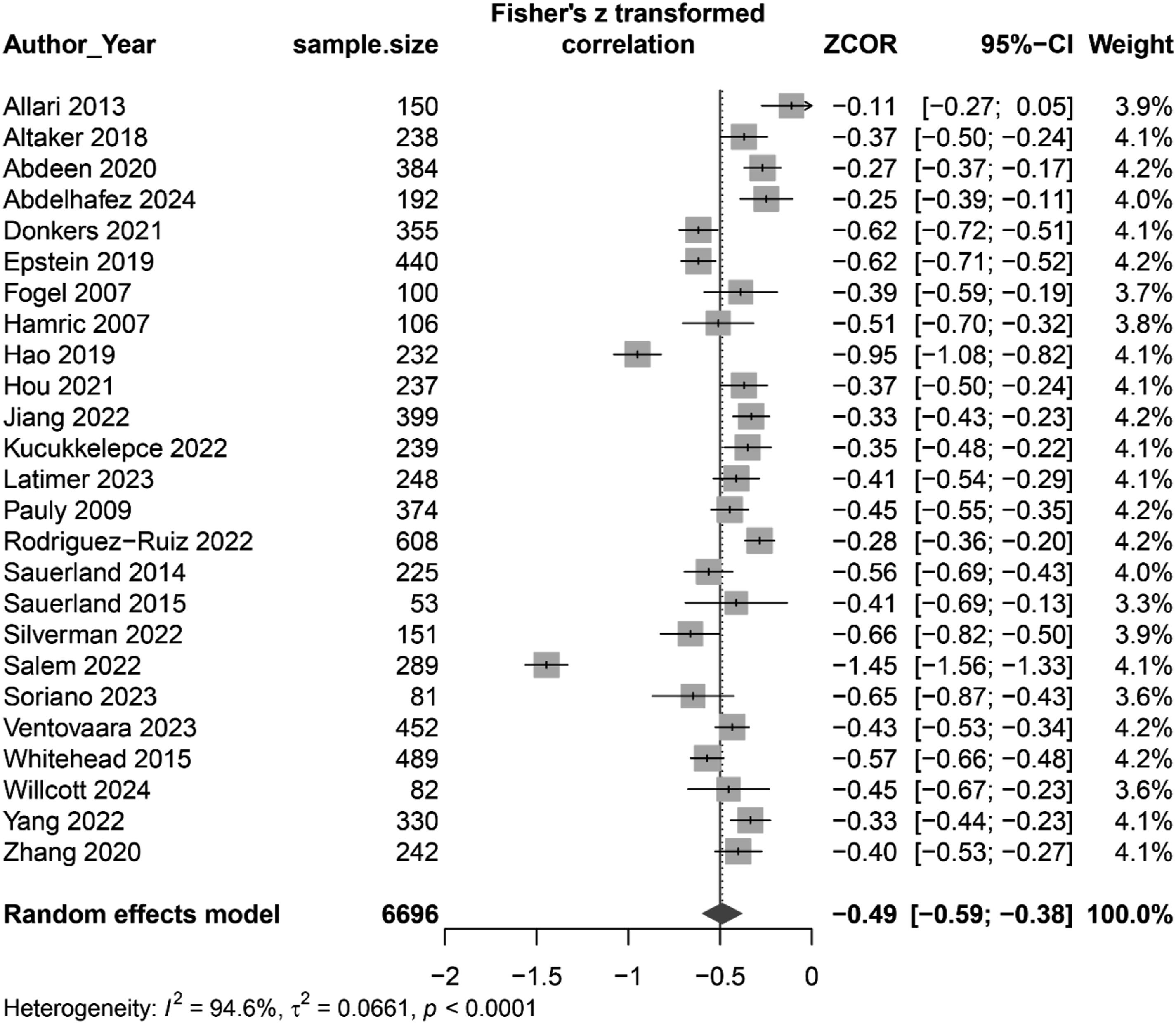
Associations of moral distress frequency and intensity with ethical climate
Ten studies, comprising 2105 participants, reported associations between moral distress frequency and ethical climate. The meta-analysis revealed a moderate negative association (r = −0.37, 95% CI: −0.45 to −0.28, p = .001) (Supplemental Figure 1).
Regarding moral distress intensity, no significant association with ethical climate was observed (r = −0.15, 95% CI: −0.21 to −0.10, p = .78) (Supplemental Figure 2).
Moderator analysis of the association between overall moral distress and ethical climate
Moderator analysis of the association between overall moral distress and ethical climate among nurses.
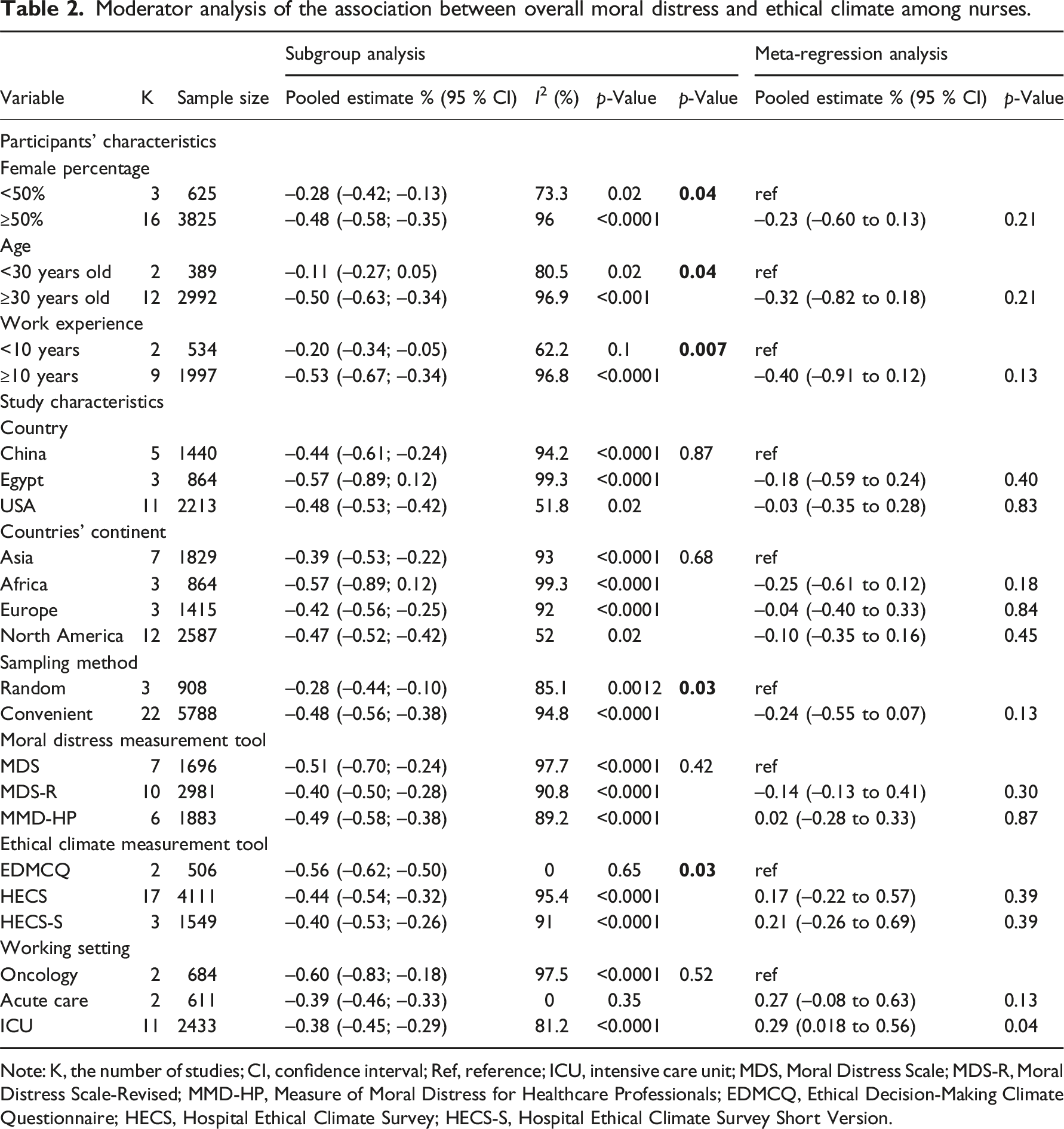
Note: K, the number of studies; CI, confidence interval; Ref, reference; ICU, intensive care unit; MDS, Moral Distress Scale; MDS-R, Moral Distress Scale-Revised; MMD-HP, Measure of Moral Distress for Healthcare Professionals; EDMCQ, Ethical Decision-Making Climate Questionnaire; HECS, Hospital Ethical Climate Survey; HECS-S, Hospital Ethical Climate Survey Short Version.
Concerning participant characteristics, three variables significantly moderated the strength of the association: (1) Gender composition: Studies with a female proportion ≥50% showed a stronger negative correlation (r = −0.48, 95% CI: −0.58 to −0.35). (2) Mean age: A stronger association was observed in studies with a mean participant age ≥30 years (r = −0.50, 95% CI: −0.63 to −0.34). (3) Work experience: Studies with average years of work experience ≥10 reported a stronger correlation (r = −0.53, 95% CI: −0.67 to −0.34).
Regarding study characteristics, no significant moderation was found for country, continent, or the specific moral distress measurement tool. Conversely, sampling method and ethical climate assessment tool significantly moderated the relationship. Concretely, stronger correlations were found in studies using convenient sampling (r = −0.48) compared to random sampling (r = −0.28), and in studies using the EDMCQ (r = −0.56) compared to those using HECS (r = −0.44) and HECS-S (r = −0.40).
Working settings did not demonstrate a significant moderating effect in subgroup analysis. However, meta-regression indicated that studies conducted in intensive care units showed a weaker correlation compared to those in oncology settings.
Sensitivity analysis and publication bias
Sensitivity analyses confirmed the stability of the results across studies. Funnel plots and Begg’s test indicated no significant publication bias for overall moral distress and ethical climate (t = −0.22, p = .83) or for moral distress frequency and ethical climate (t = 0.14, p = .89) (Supplemental Figures 12–16).
Discussion
This systematic review and meta-analysis included 31 studies, encompassing 7635 participants across 14 countries. It provides a comprehensive examination of the associations between overall moral distress, moral distress frequency, intensity, and ethical climate among nurses.
Key findings
The association between overall moral distress and ethical climate
Our meta-analysis revealed a moderate negative correlation between overall moral distress and ethical climate among nurses, stronger than that observed in other healthcare professionals.26,69 This discrepancy likely reflects the interplay of organizational and individual factors.
At the organizational level, entrenched hierarchies often relegate nurses to subordinate roles, limiting their involvement in clinical decision-making. 70 The absence of effective ethical support mechanisms exacerbates this issue, leaving nurses without adequate guidance or decision-making resources. Hospitals should prioritize strengthening ethics education, establishing clear ethical frameworks, developing advanced practice nurse teams, providing decision support tools, and fostering interdisciplinary collaboration.71,72
At the individual level, nurses’ continuous emotional and physical labor, coupled with frequent interactions with patients and healthcare teams, increases psychological strain, burnout, absenteeism, and even turnover intentions.73,74 Given that the nursing workforce is predominantly female, gender-specific coping mechanisms, such as emotional suppression or avoidance, may also amplify moral distress. 75 Additionally, poor interprofessional communication and overreliance on physicians’ decisions may cause conflicts between nurses’ professional values and role identity.76,77 Organizational interventions should include strengthening psychological support, offering regular ethics seminars, and providing communication skills training. 78
Associations between moral distress frequency and ethical climate
We also found a moderate negative correlation between moral distress frequency and ethical climate. However, no significant correlation emerged between moral distress frequency and ethical climate, contrasting with some prior studies. 69 These inconsistencies may stem from variations in sample characteristics, clinical settings, and assessment tools.
Moderator analysis of the association between overall moral distress and ethical climate
Participants’ characteristics
Demographic factors, particularly gender composition and age, significantly moderated the relationship. Subgroup analysis indicated that a higher proportion of female participants strengthened the negative association between moral distress and ethical climate, possibly reflecting women’s greater moral sensitivity and empathy.79,80 Age also acted as a moderator; nurses aged 30 and above showed a stronger negative correlation, potentially due to heightened professional responsibilities, career expectations, and work-life balance pressures.35,81
Work experience further influenced the association. Nurses with more than 10 years of experience exhibited a stronger negative correlation, likely due to greater exposure to ethical dilemmas, professional disillusionment, and interpersonal conflicts. 82
Study characteristics
Sampling methods significantly impacted the findings. Studies using convenience sampling reported a stronger negative correlation compared to those32,58,61 using random sampling, suggesting potential selection bias. 83
Measurement tools for ethical climate also contributed to heterogeneity. Studies utilizing the EDMCQ and HECS-S scales reported stronger negative correlations than those using the HECS-S, highlighting the need for future research to employ standardized, psychometrically robust instruments and potentially integrate mixed-methods approaches for greater measurement consistency. 84
Work settings
Meta-regression revealed setting-specific differences: ICU nurses showed a weaker negative association compared to oncology nurses. This may reflect differences in ethical challenges: ICU nurses often face urgent decisions, whereas oncology nurses confront chronic value conflicts regarding quality of life and resource allocation.22,85,86
Strengths and limitations
This review has several strengths. First, it systematically examined both the direction and magnitude of the associations between nurses’ overall moral distress, moral distress frequency, moral distress intensity, and ethical climate. Second, a comprehensive search across 10 databases ensured a wide scope. Third, moderator analyses and meta-regressions provided valuable insights into sources of heterogeneity.
Nonetheless, several limitations must be acknowledged. First, restricting the search to English and Chinese publications may have led to language bias. Second, all included quantitative and the quantitative components of mixed-method studies used cross-sectional designs, which preclude causal inference.
Implications for practice and research
Healthcare administrators must recognize the detrimental impact of moral distress and foster policies aimed at cultivating a positive ethical climate. Enhancing ethical support can improve nurses’ moral decision-making, nursing quality, and retention rates. Future research should prioritize longitudinal, qualitative, and interventional studies to establish causal links between moral distress and ethical climate and to deepen understanding of underlying mechanisms.
Conclusion
This systematic review and meta-analysis identified a moderate negative association between nurses’ overall moral distress, moral distress frequency, and ethical climate. Moderator analyses highlighted that gender composition, age, work experience, sampling methods, and ethical climate measurement tools contribute to heterogeneity in overall association.
Our findings emphasize the urgent need for future research employing larger, more diverse samples and methodologically rigorous designs. Building a positive ethical climate remains essential for mitigating nurses’ moral distress and enhancing organizational effectiveness.
Supplemental Material
Supplemental Material - Nurses’ moral distress and ethical climate: A systematic review and meta-analysis
Supplemental Material for Nurses’ moral distress and ethical climate: A systematic review and meta-analysis by Kexin Xue, Jingxian Shang, Chaochao Yang Liping Pan, Huijing Shi, and Yanli Zeng in Nursing Ethics.
Footnotes
Acknowledgments
We gratefully acknowledge all nurses who participated in the studies included in the meta-analysis, and the authors who provided the original data for their help in this study.
Authors’ contributions
Kexin Xue: Conceptualization, methodology, software, visualization, and writing—original draft. Jingxian Shang: Conceptualization, methodology, software, visualization, and writing—original draft. Chaochao Yang: Conceptualization, methodology, software, visualization, and writing—original draft. Liping Pan: Methodology, data curation, and visualization. Huijing Shi: Methodology, data curation, and visualization. Yanli Zeng: Conceptualization, methodology, supervision, writing—reviewing and editing, and funding acquisition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the “Primary Health Development Research Center of Sichuan Province Program” [grant numbers SWFZ23-Z-16] and the “Sichuan Hospital Management and Development Research Center program” [grant number SCYG2024-3].
Data Availability Statement
Data sharing is not applicable as no data was generated or analyzed in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.