
Abstract
Background
The COVID-19 pandemic has posed unprecedented challenges for nurses, including resource shortages, heavier workloads, and ethical decision-making pressures, putting them at high risk for moral injury. This threatens their physical and mental health, job stability, and the quality of care.
Aim
The aim was to systematically assess the level of moral injury among nurses during the COVID-19 pandemic.
Methods
A comprehensive search was conducted on 12 databases (PubMed, Web of Science, MEDLINE, ProQuest, Embase, CINAHL, Scopus, PsycINFO, CBM, CNKI, VIP, WanFang Data) for cross-sectional studies published up to 20 July 2025, that reported the level of moral injury among nurses using the Moral Injury Symptoms Scale—Health Professionals Version. A systematic review and meta-analysis were conducted. Two researchers independently screened the literature, extracted data, and assessed methodological quality. The pooled mean score was calculated using random-effects or fixed-effects models, with subgroup analysis to explore heterogeneity.
Ethical considerations
Ethical approval was not required as the review synthesized publicly available data.
Results
This study included 16 articles, involving 5824 participants. The meta-analysis showed that the pooled mean total MISS-HP score for nurses was 42.12 (95% CI: 40.70–43.53). Among the dimensions, the pooled mean score for Loss of religion/spiritual faith was the highest at 5.68 (95% CI: 4.61–6.74), while the pooled mean score for religious struggles was the lowest at 2.26 (95% CI: 1.13–3.40). Subgroup analysis results indicated significant differences in moral injury levels among nurses based on Survey year and department (p < .001).
Conclusions
Under the context of the COVID-19 pandemic, nurses experienced moderate to high levels of moral injury, particularly during the early stages of the pandemic in 2020, with emergency department nurses being most affected. To support nurses’ well-being and mental health, healthcare institutions should strengthen ethical support systems, improve management, and consider the role of religion/spiritual faith in alleviating moral injury.
Introduction
Nurses, as the core force in the healthcare system, play a crucial role in determining the quality of healthcare services and public health. 1 The International Council of Nurses has made promoting nurse well-being one of its key missions. 1 The National Academy of Medicine in the United States also called for attention to the impact of COVID-19 on healthcare workers, particularly the overall well-being of nurses. 2 With the global spread of the COVID-19 pandemic, the professional challenges faced by nurses have significantly increased. 3 This public health crisis, with its unprecedented scale and uncertainty, forced nurses to make difficult decisions under extreme pressure. 4 These challenges not only include issues such as shortages of medical resources, increased workloads, and ethical decision-making pressure, 3 but also deeper ethical dilemmas, such as patients dying in isolation due to visiting restrictions, balancing personal safety with caregiving responsibilities in the absence of adequate protective equipment, and making resource allocation decisions in the face of overwhelming numbers of patients. 5 These unique challenges have made nurses a high-risk group for moral injury, 6 increasing compassion fatigue and burnout, 7 making moral injury (MI) a core issue threatening the physical and mental health and professional stability of nurses.
Moral injury was originally used in military contexts. 8 Litz et al. 9 defined it as the experience of committing, failing to prevent, witnessing, or knowing about actions that violate one’s deeply held moral beliefs. In healthcare systems, nurses are more vulnerable to moral injury due to the nature of their work. 10 Especially during the COVID-19 pandemic, the surge in patients caused nurses to frequently face ethical dilemmas such as emergency triage, resource allocation, and end-of-life care. 10 When nurses are unable to act according to their moral beliefs, they may experience feelings of shame, guilt, and betrayal,11,12 along with emotional conflict and loss of trust. 13 Moral injury is associated not only with emotional disorders, substance abuse, and self-harm, 14 but also often coexists with depression, suicide, and post-traumatic stress disorder (PTSD).15–17 Its harm lies in weakening nurses’ trust in themselves, their colleagues, and the healthcare system, leading to intense feelings of betrayal and guilt, undermining moral integrity and self-efficacy,12,18 further triggering burnout, 19 and ultimately affecting nurse well-being and the quality of care. 20
Currently, the commonly used assessment tool for moral injury in healthcare workers is the Moral Injury Symptom Scale–Healthcare Professionals Version (MISS-HP). 21 This scale was developed by Mantri et al. 21 in 2020 and has been validated in several studies as a reliable and effective tool for assessing moral injury in healthcare workers.10,22–36 The scale includes 10 dimensions: Sense of Betrayal, Guilt, Shame, Moral Concerns, Loss of Trust, Loss of Meaning/Goals, Difficulty in Forgiving, Self-condemnation, Religious Struggles, and Loss of Religion/Spiritual Faith, with a total of 10 items. Each item is scored from 1 to 10, with a total score range of 10 to 100, where higher scores indicate more severe moral injury. 21 Mantri et al. 21 noted that a score of 36 or above indicates at least moderately distressing moral injury. The tool has been validated for good reliability and validity and has undergone cross-cultural validation in multiple languages.21,36 It has been widely used among healthcare workers during the pandemic and in different countries.10,22–36
However, existing studies are mostly single-center or regional surveys, with limited sample sizes and significant result variability. Moreover, most of these studies are cross-sectional designs,10,22–36 lacking comprehensive and systematic integrated analyses. In light of this, this study conducts a systematic review and meta-analysis based on the literature related to the MISS-HP scale, aiming to assess the overall level of moral injury among nurses worldwide. Given that the COVID-19 pandemic is a dynamic and evolving process, involving viral mutations, vaccine distribution, and adjustments to preventive policies,37,38 this study integrates cross-sectional data from different years for subgroup analysis to explore the temporal trends in moral injury levels during the pandemic. The findings of this study could provide insights for multi-level practice: at the institutional level, it could help improve psychological support systems to enhance nursing team stability; at the policy level, it could inform the development of ethical plans and resource allocation during public health crises; and at the educational level, it could provide a basis for optimizing professional training and strengthening nurses’ moral decision-making and psychological adjustment skills. Overall, this study aims to enrich the evidence base in this field and offer new ideas for developing more precise intervention measures and systemic support strategies.
Methods
Design
This review was conducted following the Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 39 and has been registered on the PROSPERO website (registration number: CRD420251118389).
Search strategy
Databases including PubMed, Web of Science, MEDLINE, ProQuest, Embase, CINAHL, Scopus, PsycINFO, Chinese Biomedical Database (CBM), China National Knowledge Infrastructure (CNKI), Chinese Scientific Journal Databases (VIP), and WanFang Data were searched to collect studies related to the level of moral injury among nurses during the COVID-19 pandemic, with the search covering the period from database inception to 20 July 2025. A combined search strategy using both subject headings and free terms was applied, along with manual searches through reference lists. The search terms included: Nurses, Nursing Staff, Nurse Practitioners, moral injury, etc. The complete search strategy is provided in Supplemental Table 1.
Eligibility criteria
Inclusion criteria: (1) Study type: Cross-sectional studies (The theoretical basis for selecting cross-sectional design in this study is as follows: First, since the study aims to assess the level of moral injury among nurses during the COVID-19 pandemic rather than causal relationships, 40 cross-sectional surveys are a classic design more suited for evaluating health status at a specific point in time. 41 Second, this design has become the mainstream research method in public health emergencies due to its timeliness. 41 Existing literature provides sufficient data support for this review.10,22–36 Finally, limiting to a single study design helps reduce methodological heterogeneity, 42 which improves the stability and representativeness of the meta-analysis results. 43 ); (2) Study population: Nurses practicing during the COVID-19 pandemic (if the study includes mixed samples, data for the nurse group must be extracted separately); (3) Measurement tool: Moral Injury Symptoms Scale—Health Professionals Version (MISS-HP) 21 ; (4) Outcome indicators: MISS-HP mean total score (or) mean score of the 10 dimensions.
Exclusion criteria: (1) Duplicate publications, conference abstracts, and review studies; (2) Studies with incomplete or incorrect data; (3) Non-Chinese or non-English studies.
Study selection and data extraction
Two researchers independently conducted literature screening, data extraction, and verification based on the inclusion and exclusion criteria. In case of disagreement, a third party was consulted. During literature screening, the titles of the articles were read first. Articles meeting the inclusion criteria were then further examined by reading the abstracts and full texts. Data extracted included: First author (year), Survey year, Country, Sample size, Department, MISS-HP mean total score, and the mean scores of dimensions ①-⑩.
Quality appraisal
The methodological quality assessment of the included studies was conducted by two researchers based on the cross-sectional study evaluation criteria recommended by the Agency for Healthcare Research and Quality (AHRQ). 44 The AHRQ criteria consist of 11 items, with each item scoring 1 point for a “yes” answer, and no points for a “no” or “unclear” answer. A total score of 8–11 points indicates high-quality studies, 4–7 points indicate moderate-quality studies, and 0–3 points indicate low-quality studies.
Statistical analysis
Stata software (version 15.0; StataCorp) was used to perform pooled analyses of the mean scores and standard deviations of the MISS-HP survey and its dimensions. All pooled means were presented as weighted effect sizes with corresponding 95% CIs. Heterogeneity among studies was assessed using Cochrane’s Q test and the I2 index. If significant heterogeneity was observed (P < .05 and I2 ≥ 50%), random-effects models were applied for the meta-analysis; otherwise, fixed-effects models were used. 45 To explore potential sources of heterogeneity and evaluate their impact on nurses’ moral injury during the COVID-19 pandemic, subgroup analyses were conducted by survey year, department, and country. A leave-one-out sensitivity analysis was performed to assess the robustness of the results. Funnel plots and Egger’s test were used to evaluate publication bias. A two-sided p < .05 was considered statistically significant for all analyses.
Results
Search results
A total of 1144 relevant articles were initially retrieved, of which 732 duplicates were removed. Titles and abstracts were screened, resulting in the exclusion of 339 articles. Full texts were reviewed for further screening, leading to the exclusion of 57 articles. Finally, 16 articles were included,10,22–36 15 in English and 1 in Chinese. The literature screening process and results are shown in Figure 1. PRISMA flow diagram of the literature search process.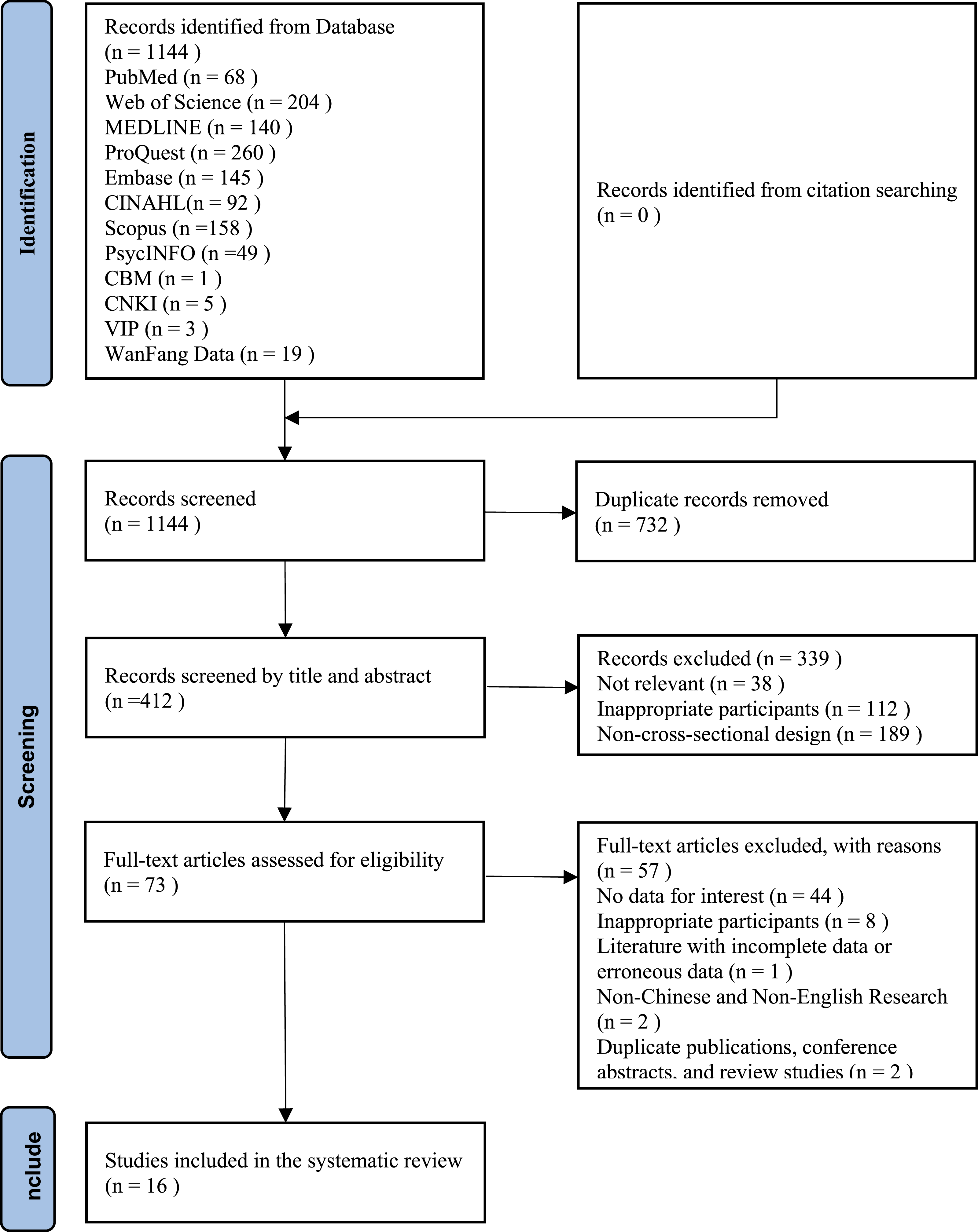
Study characteristics
Characteristics of included studies (n = 16).
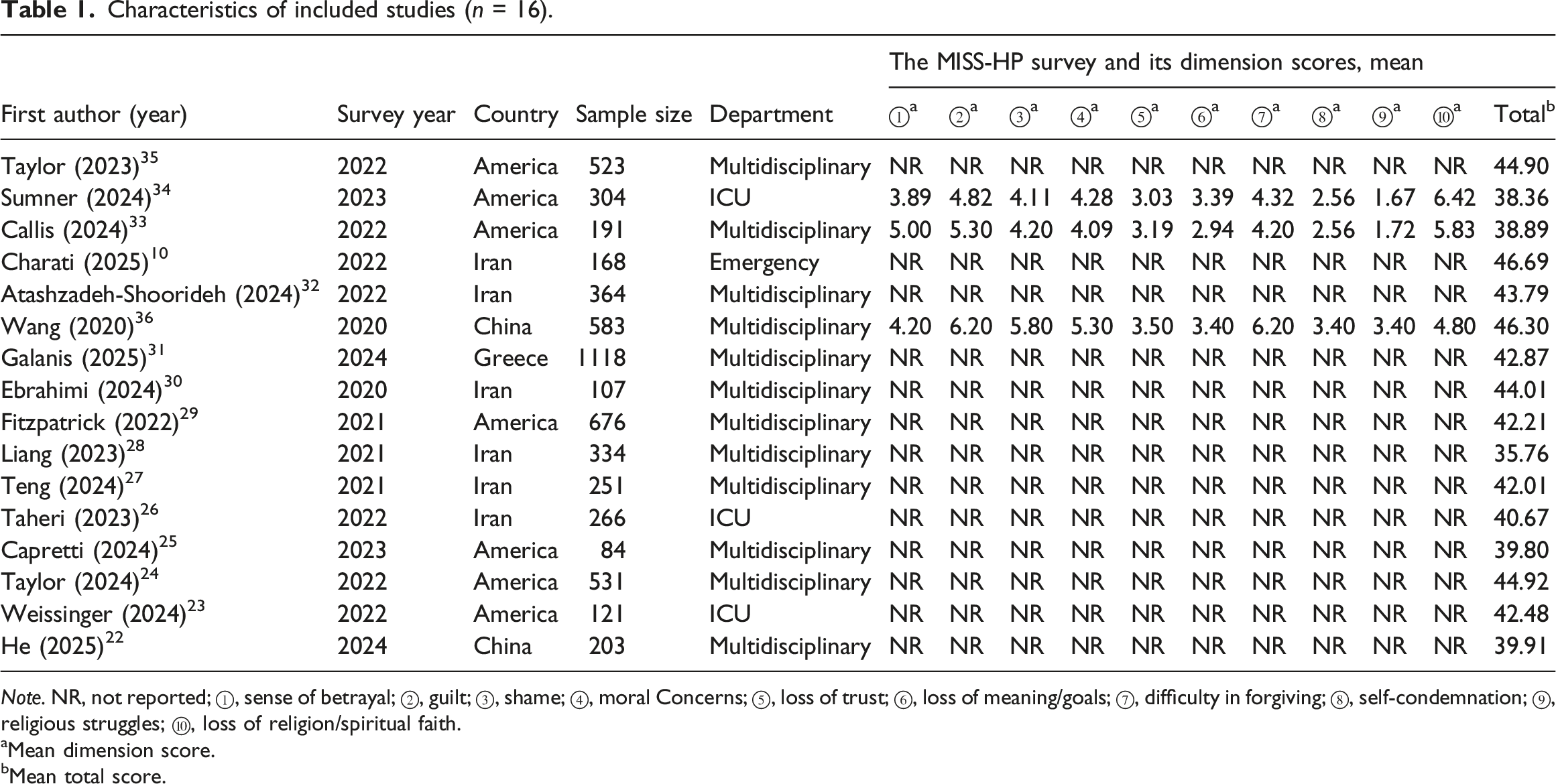
Note. NR, not reported; ①, sense of betrayal; ②, guilt; ③, shame; ④, moral Concerns; ⑤, loss of trust; ⑥, loss of meaning/goals; ⑦, difficulty in forgiving; ⑧, self-condemnation; ⑨, religious struggles; ⑩, loss of religion/spiritual faith.
aMean dimension score.
bMean total score.
Quality assessment
All 16 included studies10,22–36 were assessed for methodological quality using the AHRQ scale, with good inter-rater consistency (Cohen’s kappa = 0.85).
The quality assessment results showed that 1 study (6.25%) was of high quality (8 points), while the remaining 15 studies (93.75%) were of moderate quality (4–7 points).
The main methodological limitations of the studies were: (1) failure to adequately describe or control for confounding factors; (2) lack of clear explanation regarding the handling of missing data. Detailed assessment results are provided in Supplemental Table 2.
Nurses’ MISS-HP scores
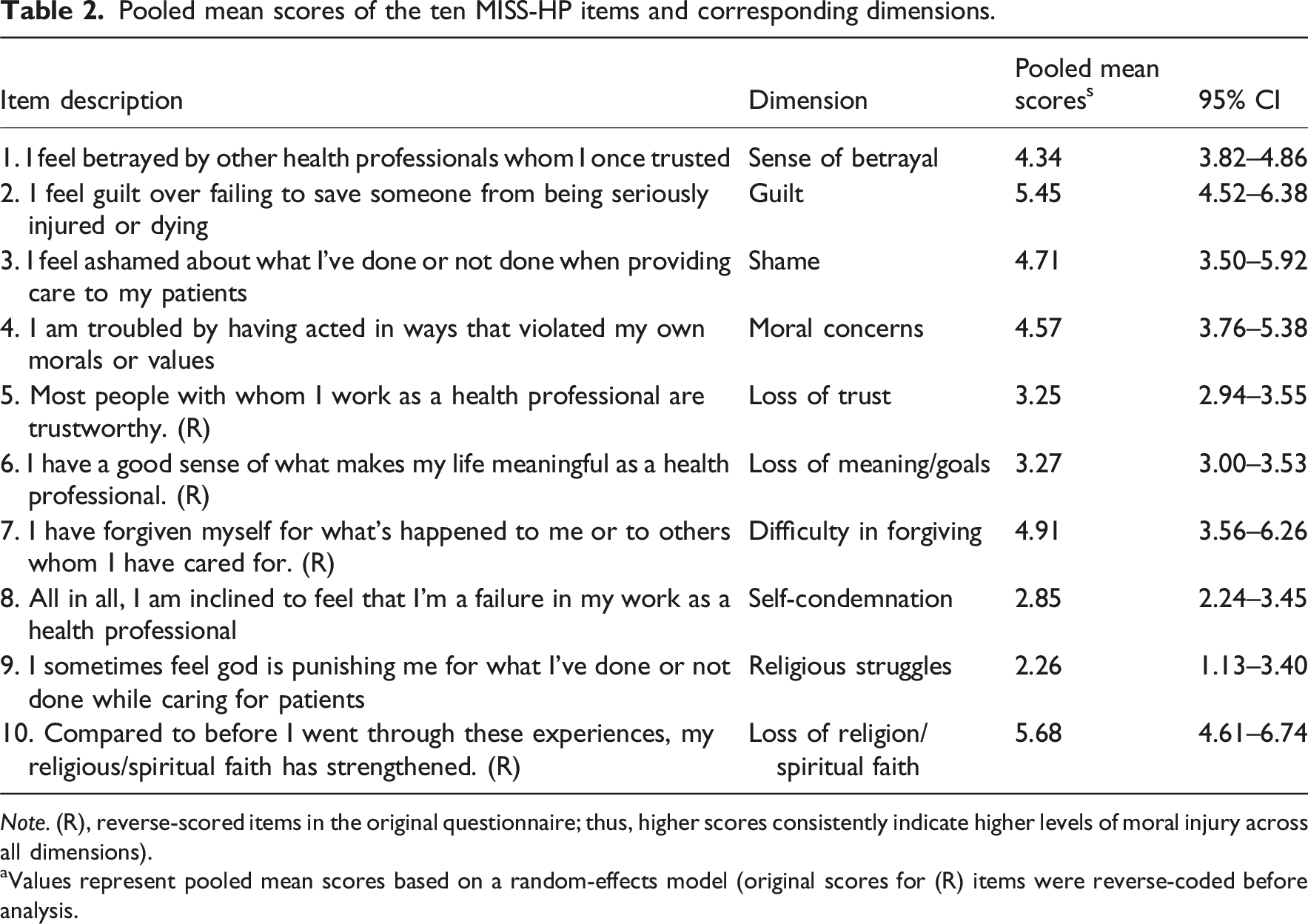
The mean total MISS-HP score was reported in 16 studies.10,22–36 Due to high heterogeneity between studies (I2 = 95.3%, p < .001), a random-effects model was used to calculate the pooled mean total score. The results showed that the pooled mean total MISS-HP score for nurses was 42.12 points (95% CI: 40.70–43.53), as shown in Figure 2. Three studies33,34,36 reported the mean scores for the 10 dimensions of the MISS-HP scale, with high heterogeneity within each dimension (I2 range: 67.4%–98.9%, all p < .05, see Supplemental Figures 1–10). The pooled mean scores for the 10 dimensions ranged from 2.26 to 5.68. Specifically, the pooled mean score for the loss of religion/spiritual faith dimension was the highest, at 5.68 (95% CI: 4.61–6.74), while the religious struggles dimension had the lowest pooled mean score, at 2.26 (95% CI: 1.13–3.40). Detailed scores for all dimensions are shown in Table 2. Forest plot of pooled mean total score of MISS-HP among nurses. Pooled mean scores of the ten MISS-HP items and corresponding dimensions. Note. (R), reverse-scored items in the original questionnaire; thus, higher scores consistently indicate higher levels of moral injury across all dimensions). aValues represent pooled mean scores based on a random-effects model (original scores for (R) items were reverse-coded before analysis.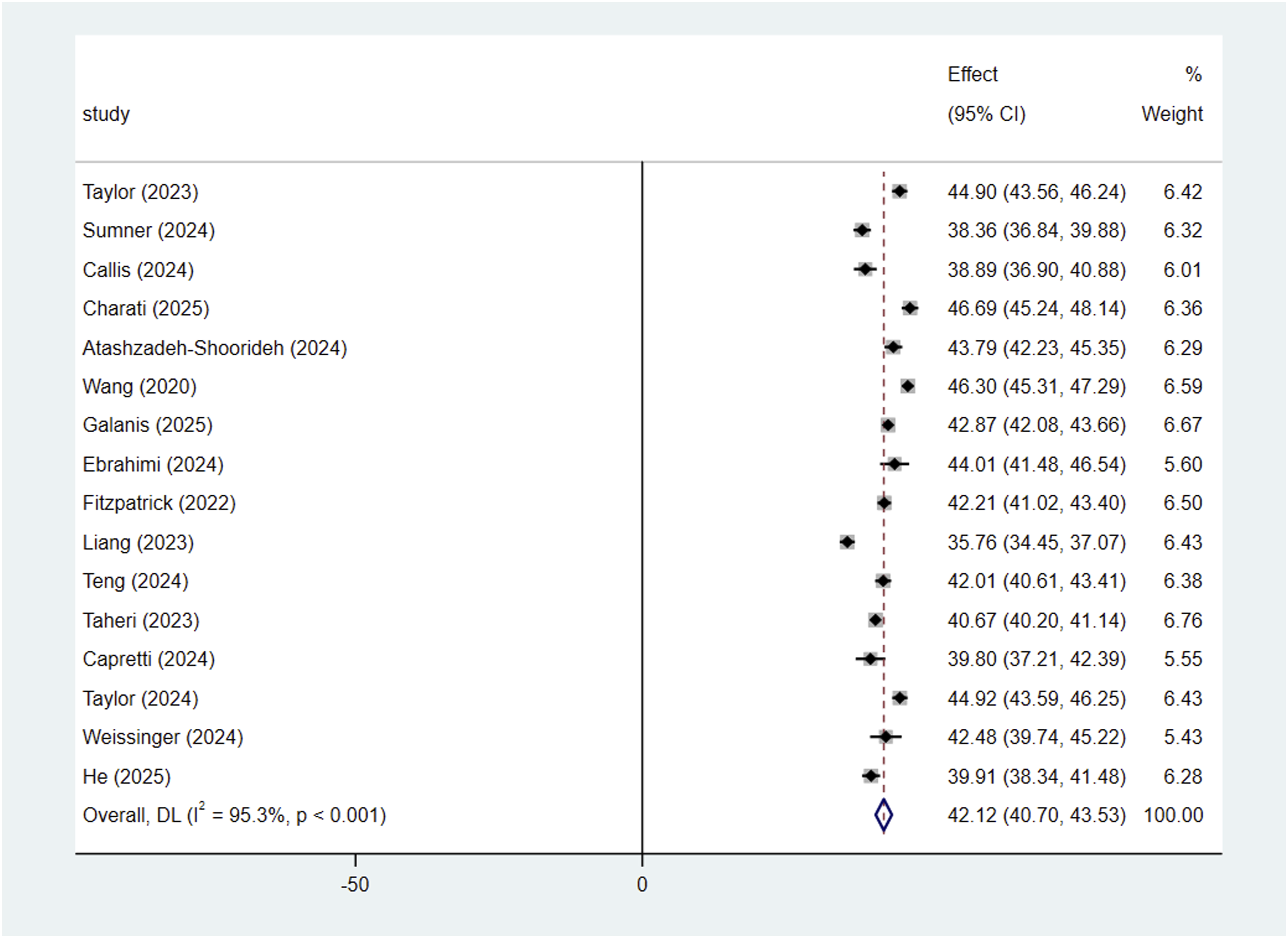
Subgroup analyses of pooled mean total MISS-HP score
Subgroup analyses of pooled mean total MISS-HP scores.
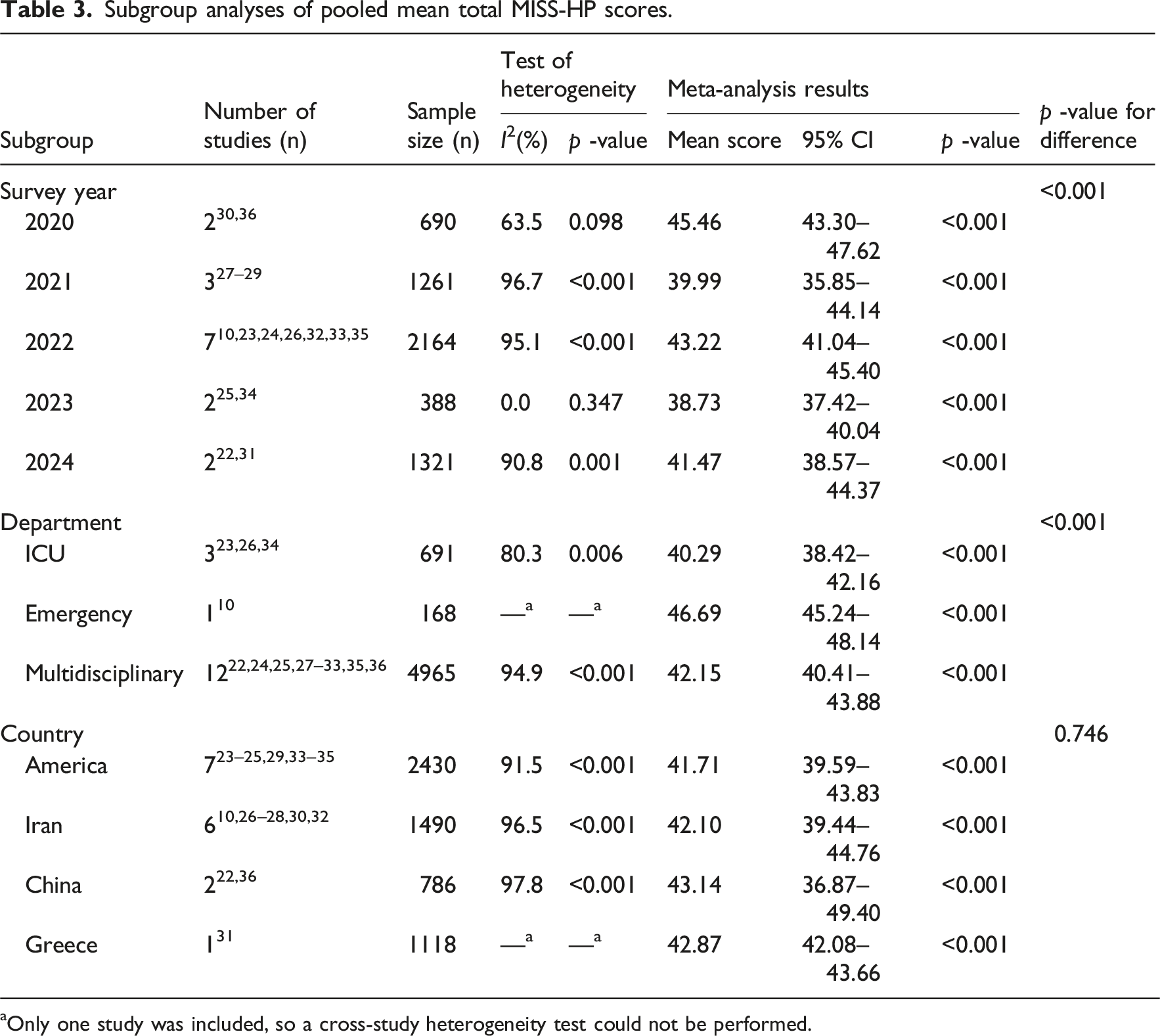
aOnly one study was included, so a cross-study heterogeneity test could not be performed.
Sensitivity analysis and publication bias
In the sensitivity analysis, each study included was removed one by one. After pooling, the nurses’ moral injury level ranged from 40.70 to 43.53, showing no significant change, indicating the stability of the study results (Supplemental Figure 12). The pooled mean total MISS-HP score Egger test showed t = 0.49, p = .632. The funnel plot of the studies was mostly symmetric (Figure 3), with no significant publication bias observed. Funnel plot of pooled mean total score of MISS-HP among nurses.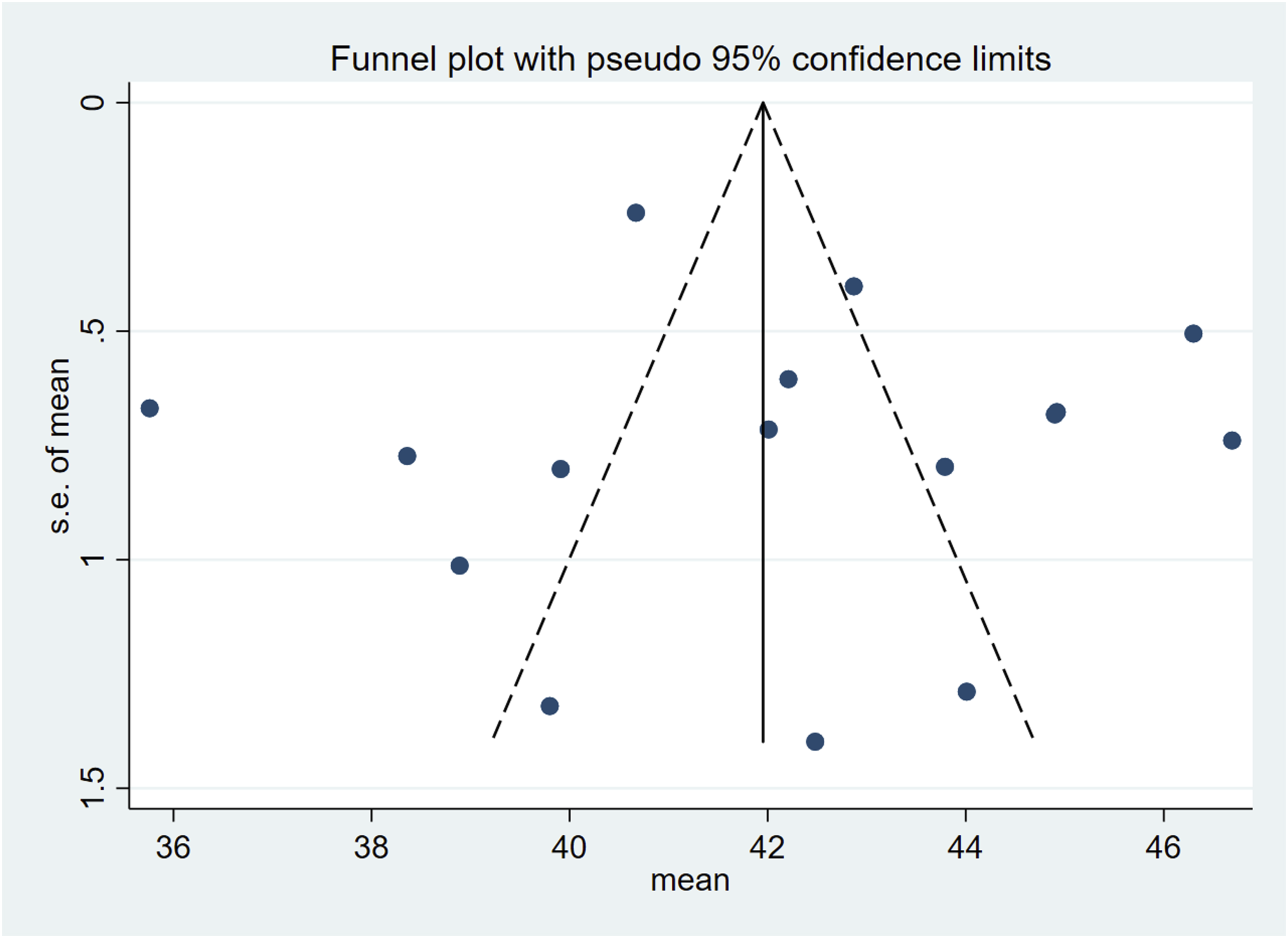
Discussion
This study included 16 studies on moral injury among nurses in the context of the COVID-19 pandemic. The studies reported the pooled mean total MISS-HP score or the pooled mean scores for its 10 dimensions, and subgroup analyses were performed based on survey year, department, and country.
The results of this study show that the pooled mean total MISS-HP score among nurses during the COVID-19 pandemic was 42.12 (95% CI: 40.70–43.53), higher than the optimal cutoff value of 36 established by Mantri et al. 21 and the mean score of 36.8 reported among U.S. healthcare workers. This indicates that nurses have experienced a moderate to high, and more pronounced, burden of moral injury. This burden is not merely an individual psychological issue, but an external manifestation of a dysfunctional or resource-constrained healthcare system affecting individual practitioners. 46 Its origins can be analyzed at both the systemic and organizational levels: At the systemic level, the pandemic worsened structural barriers such as shortages of healthcare workers, inadequate protective equipment, and excessive workloads, 47 forcing nurses to make prioritization decisions under resource constraints that conflicted with ethical standards, thereby triggering moral distress. 48 This experience of being unable to act according to moral judgment due to external constraints is the core source of moral injury. 49 At the organizational level, the lack of supportive leadership, rigid hierarchies, and inconsistent policies weakened nurses’ professional autonomy and voice, causing their ethical concerns to be overlooked. 50 The resulting sense of disillusionment due to insufficient organizational support may be an important contributor to moral injury. 51 In conclusion, external constraints at both the systemic and organizational levels hinder nurses’ moral actions, leading to an accumulation of moral burden, 49 which becomes more pronounced under the high-pressure context of the COVID-19 pandemic.
Regarding the scores of different dimensions (based on three studies), the pooled mean score for the loss of religion/spiritual faith dimension was the highest, at 5.68 (95% CI: 4.61–6.74). This suggests that, under significant traumatic stress such as the pandemic, some nurses’ existing religious or spiritual beliefs may have been cognitively impacted, reflecting the complexity of the role that religion and spirituality play in nurses’ coping with professional challenges. 52 Although religion and spirituality are typically seen as protective resources that provide comfort and inner strength, 53 in extreme ethical dilemmas or when traumatic experiences sharply conflict with personal belief systems, they may become risk factors that exacerbate moral distress. 54 This is particularly true for nurses who strongly associate their moral principles with spiritual beliefs. 55 Under resource constraints, difficult decisions or witnessing unnecessary patient suffering can trigger profound moral and spiritual conflicts, leading to cognitive dissonance between belief and practice. 56 Such conflicts are more prominent among nurses who adhere to higher moral standards, 57 as they are more likely to experience moral injury when faced with unavoidable negative outcomes and the gap between ideals and reality. 58 Moreover, if nurses adopt negative religious coping strategies, such as attributing their suffering to divine punishment or abandonment, it may further intensify moral distress. 59 Therefore, some nurses with strong faith and a sense of moral responsibility may experience a sense of powerlessness and frustration when they cannot achieve their ideal goals under the constraints of real-world conditions. This internal conflict may become one of the key triggers for their psychological issues and moral injury. 46
The pooled mean score for the religious struggles dimension was the lowest, at 2.26 (95% CI: 1.13–3.40). This may be because, during major crises such as the COVID-19 pandemic, individuals are more likely to view religion as a positive psychological resource rather than experience struggles with their faith.53,60 According to psychological theories, individuals assign different religious meanings to challenging events, which form either positive or negative coping patterns. 61 This trend may be more pronounced among frontline nurses facing immense physical and mental pressure, as well as ethical dilemmas during the pandemic. 62 Studies have shown that healthcare workers tend to adopt positive religious coping strategies to manage stress, and this approach is associated with lower levels of anxiety. 63 Consistent with this study’s findings, it suggests that the participants may view religious faith as a source of resilience, helping to maintain professional commitment and moral integrity, thus reducing inner religious conflict. 63 From an ethical perspective, such faith-based positive coping strategies may help nurses maintain empathetic care under extreme pressure and potentially alleviate moral distress caused by witnessing significant suffering. 64 This phenomenon also aligns with the broader social context, where the demand for religious support globally increased during the pandemic, reflecting a general reinforcement of religious solace in collective adversity. 65 Therefore, seeking religious support and adopting positive religious coping strategies during major crises may be a more common psychological and behavioral tendency than experiencing religious struggles. 66
Based on the above findings, future research and practice should focus on developing a multi-level, systematic ethical support framework to address the moderate to high levels of moral injury within the nursing population. Since its roots primarily lie in systemic challenges, interventions need to go beyond the individual level, with a focus on optimizing the macro-level practice environment and improving organizational support systems. 67 At the systemic level, policymakers and healthcare institution managers should prioritize addressing the long-standing structural shortages in healthcare resources 68 and establish clear, fair ethical guidelines for resource allocation to reduce the moral burden on nurses when making triage decisions during crises. 69 At the organizational level, fostering supportive and transparent leadership is crucial. 70 Open communication channels should be established to ensure that nurses’ ethical concerns are effectively addressed, and greater clinical decision-making autonomy and voice should be granted, thereby reducing their moral distress.47,71 At the educational level, integrating ethics education and reflective practice into nursing school curricula and continuing education programs may enhance nurses’ and nursing students’ moral resilience and their ability to navigate complex ethical scenarios. 72 This could contribute to creating a practice environment that better supports their moral integrity and professional well-being.
The subgroup analysis of this study revealed that from 2020 to 2024, the pooled mean total MISS-HP score among nurses showed significant annual fluctuations, with scores of 45.46, 39.99, 43.22, 38.73, and 41.47, respectively. The differences between groups were statistically significant (p < .001), which may be closely related to the varying impacts of the COVID-19 pandemic on the healthcare system at different stages. 73 The peak in 2020 may have resulted from the extreme challenges during the early phase of the pandemic, 74 such as severe shortages of personal protective equipment (PPE) 75 and the lack of effective treatment strategies, 76 which forced nurses to make resource allocation decisions conflicting with their professional values while facing personal safety risks, leading to intense moral dilemmas. 77 The decrease in 2021 may have benefited from improved PPE supply and the introduction of ethical decision-making support tools, such as multi-principle care allocation frameworks, which partially alleviated the acute ethical stress faced by nurses. 78 However, the spread of the Omicron variant in 2022 imposed another wave of pressure on an already overburdened nursing workforce, 79 where ongoing staff shortages and insufficient organizational support further intensified moral dilemmas.80,81 The decline in 2023 may be attributed to the lifting of the global public health emergency 82 and the resumption of regular healthcare services. 83 The slight rebound in 2024 suggests the lasting impact of the pandemic and persistent systemic issues. On one hand, previous traumatic ethical experiences may continue to affect nurses’ mental health in the form of moral residue. 84 On the other hand, the worsening global nursing shortage in the post-pandemic era 85 and sustained heavy workloads have caused moral distress among nurses unable to provide ideal care. 86 This indicates that even after the peak of the crisis, chronic moral injury caused by systemic deficiencies remains a key factor affecting nurses’ professional well-being. 87 It also suggests that future ethical interventions should address both acute crisis responses and chronic injury recovery, and develop long-term strategies targeting systemic deficiencies to ensure the ongoing protection of nurses’ professional well-being.
The subgroup analysis of this study showed that the pooled mean total MISS-HP score was highest for emergency department nurses (46.69), followed by multidisciplinary nurses (42.15), while ICU nurses had the lowest score (40.29). The differences between groups were statistically significant (p < .001). This may be because the emergency department, as the frontline of the hospital, has a highly unpredictable work environment and continuously limited resources. 88 Additionally, frequent ethical dilemmas during the pandemic 75 may have contributed to the higher level of moral injury among nurses in this department. Notably, ICU nurses had relatively lower scores, which contrasts with the common perception of the ICU as a high-conflict ethical area. 89 One possible explanation is that ICU nurses, due to their prolonged exposure to complex ethical challenges such as end-of-life decisions, may have developed more mature coping mechanisms, such as perspective-taking, which reflects higher moral resilience. 90 The intermediate scores of multidisciplinary nurses suggest that systemic issues, such as resource limitations and inadequate organizational management, are prevalent across various departments. 91 Although the data from the emergency department comes from a single study, which may affect the generalizability of this result, this study preliminarily indicates that the impact of different clinical environments on nurses’ moral injury is heterogeneous, suggesting that future research should develop context-sensitive organizational support strategies tailored to the ethical challenges of specific departments.
The subgroup analysis of this study showed that the pooled mean total MISS-HP scores for nurses in China, Greece, Iran, and America (43.14, 42.87, 42.10, and 41.71, respectively) did not differ significantly (p = .746), indicating that moral injury may have been a common challenge faced by nurses in these countries during the COVID-19 pandemic. However, this statistical similarity may mask the heterogeneity of the ethical dilemmas experienced by nurses in each country. 74 The same level of injury could stem from vastly different pandemic outbreak timelines, healthcare system capabilities, and socio-economic contexts across these nations. Specifically, the pressures faced by nurses in China were mainly related to the ethical stress of dealing with an unknown virus and severe shortages of medical resources during the early stages of the pandemic, as China was the initial epicenter. 92 In Iran, moral injury among nurses was uniquely shaped by political and economic factors, arising from the resource challenges under long-standing international sanctions, which led to a sense of helplessness due to the inability to provide adequate care to all patients. 93 In the United States, moral distress was more closely related to the persistent systemic pressures under the large scale and multiple waves of the pandemic, 94 including resource allocation disputes, inadequate organizational support, and societal divisions triggered by public health measures. 95 In Greece, based on a single study, the situation reflected the challenges arising from the inherent vulnerabilities of the healthcare system due to prolonged economic austerity measures. 96 In summary, nurse moral injury is not only a psychological issue but also a product of the complex interplay of healthcare, social, political, and economic contexts in each country’s nursing ethics practice. 97 Future research should go beyond simple quantitative comparisons and explore the specific mechanisms behind moral injury in different contexts to provide a basis for developing localized support strategies.
Limitations
First, the number of studies included in this meta-analysis was relatively small, which may affect the representativeness of the research. In the subgroup analysis, some subgroups included a small number of studies, which could influence the stability of the results. Second, all studies included in this research were cross-sectional designs, which may not allow for causal inferences. Furthermore, the high heterogeneity in the results may increase the uncertainty of the conclusions, and the interpretation of the findings should be more cautious. Additionally, only studies published in Chinese and English were included, which may introduce language bias. Finally, this study only included research that used the MISS-HP scale to assess nurses’ moral injury, excluding studies that used other moral injury measurement tools.
Implications for practice and research
At the practical level, healthcare institutions should establish a systematic ethical support system, develop fair resource allocation principles, and optimize staffing arrangements to reduce nurses’ decision-making pressure. At the same time, identifying and addressing moral injury should be integrated into routine nursing management, with improved mechanisms for psychological counseling, ethical consultation, and peer support to help nurses maintain mental well-being in high-stress environments. In nursing education and training, ethical reflection skills should be strengthened, and the introduction of spiritual care based on religious beliefs may be explored as a supplementary approach to psychological support.
At the research level, future studies could explore the manifestations and mechanisms of moral injury from cross-cultural and interdisciplinary perspectives, use longitudinal designs to reveal its dynamic changes and long-term impacts, and combine qualitative and quantitative methods to build evidence-based assessment and intervention models that support nurses’ occupational health and ethical practice.
Conclusion
Under the context of the COVID-19 pandemic, nurses’ moral injury was at a moderate to high level, particularly during the early stages of the pandemic in 2020, with emergency department nurses experiencing especially high levels of moral injury. The main causes include systemic issues and inadequate organizational management, especially resource shortages and heavy workloads, which exacerbated ethical dilemmas. The role of religious/spiritual beliefs in strengthening nurses’ ability to cope with moral injury should be emphasized. At the same time, healthcare systems and organizational support should be improved, and more targeted ethical support strategies should be developed to reduce nurses’ moral injury and enhance their professional well-being.
Supplemental Material
Supplemental Material - Moral injury in nurses during COVID-19: A systematic review and meta-analysis
Supplemental Material for Moral injury in nurses during COVID-19: A systematic review and meta-analysis by Zhehui Yang, Hong Yan, Shijin Wang, Yan Liu, Yuling Luo, Yuanyuan Tang, and Tingting Zhang in Nursing Ethics
Footnotes
Acknowledgments
We gratefully acknowledge all nurses who participated in the studies included in the meta-analysis, and the authors who provided the original data for their help in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing is not applicable as no data was generated or analyzed in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.