
Abstract
Background
Preserving dignity is a core element of nursing care. Older adults admitted to intensive care units (ICUs) are particularly vulnerable to dignity loss due to critical illness, invasive interventions, and limited communication.
Objective
This study examined the status and influencing factors of dignified care practices among ICU nurses in caring for older patients, with the aim of informing quality-improvement strategies.
Design
An explanatory sequential mixed-methods design was employed.
Participants and Setting
A questionnaire survey was completed by 487 ICU nurses from 5 tertiary hospitals in Hunan Province, China. Semi-structured interviews were then conducted with 18 ICU nurses. Qualitative data were analyzed using a descriptive phenomenological approach.
Ethical Considerations
The study was approved by the institutional ethics committee, and informed consent was obtained from all participants.
Findings
Nurses reported moderately high dignified care (79.12 ± 10.40). Scores were higher in absolute dignity (87.05 ± 11.43) than in relative dignity (70.19 ± 12.86). Regression analysis identified six predictors—gender, education, ethics training, work environment, moral sensitivity, and psychological capital—explaining 38.4% of the variance. Qualitative findings revealed four themes: difficulty balancing technical demands with dignity preservation; patient-related barriers such as severe illness and poor adherence; cultural conflicts between traditional respect for older adults and family decision-making; and organizational constraints, including heavy workloads and implicit workplace norms.
Conclusion
ICU nurses generally demonstrate competence in dignity preservation; however, limitations remain in addressing individualized dignity needs. Dignified care is influenced by the interplay of individual, environmental, and cultural factors. Improvement requires optimizing the clinical environment, strengthening ethics education and psychological support, applying dignity-centered standards, and promoting patient-centered cultural transformation through leadership. Coordinated efforts by healthcare administrators are essential to achieve sustainable quality improvement.
Introduction
Compared with other healthcare settings, ICU nurses work in a persistently stressful environment and are burdened with substantial workloads and significant psychological strain 1. Additionally, they frequently encounter unavoidable and complex ethical challenges in their nursing practice. 2 These complexities predispose them to moral distress, 3 and as they struggle to cope with their own burdens, patients’ dignity is often overlooked. Currently, many studies at home and abroad have utilized qualitative research methods to investigate ICU nurses’ practices for safeguarding patients’ dignity. These studies indicate that upholding patients’ dignity in the ICU is highly challenging, and several recommendations have been proposed to address this issue.4–6 However, the practical value of these investigations is limited by their incomplete examination of the multidimensional influencing factors. In China, only one cross-sectional study 7 assessed nurses’ behavioral levels and individual factors in dignity preservation, recommending enhanced dignity-focused training and further exploration of other influencing factors. Meanwhile, although studies have examined dignity-related factors among older adults in nursing homes, 8 general wards, 9 and emergency departments, 10 research specifically focusing on older patients in the ICU remains limited. Collectively, existing research predominantly employs single methodologies, lacks a comprehensive analysis of influencing factors, and is particularly scarce regarding the dignity of older adults in the ICU.
Based on this premise, the present study adopts a mixed-methods approach, in which quantitative and qualitative research complement each other. It aims to comprehensively examine the current status and influencing factors of ICU nurses’ dignity-preserving practices for older patients, thereby providing an empirical foundation for improving the physical and psychological well-being of critically ill older patients.
Background
Dignity, as humanity’s most fundamental human rights principle, constitutes the core essence of nursing professional ethics. 11 Its concept is inherently abstract and multidimensional, encompassing elements such as respect, intrinsic value, sociality, and autonomy. 12 Beyond its universally recognized meaning, dignity carries deeper philosophical significance within nursing ethics. Nordenfelt 13 conceptualizes dignity as two interrelated dimensions: absolute dignity and relative dignity. The former refers to the inherent intrinsic value of every individual, characterized by universality, unconditionality, and inalienability, and serves as the ethical cornerstone of human rights theory. In contrast, the latter refers to a recognition of value constructed within social relationships and cultural contexts, characterized by malleability and variability, and susceptible to being undermined or restored through interpersonal interactions. 14 For nurses, this dual understanding further manifests as a bidirectional professional ethical value: respecting the dignity of others (other-oriented) and upholding one’s own dignity or self-respect (self-oriented), requiring them to strive for ethical equilibrium between self-respect and respect for others. 15 It follows that dignity is not a static attribute but rather a dynamic construct continuously experienced, interpreted, and morally mediated in nursing interactions.
In the Intensive Care Unit (ICU), the ethical challenge of maintaining dignity is particularly prominent. Nyholm’s research 16 indicates that due to reasons such as consciousness disorders, loss of expression ability, or being on the verge of death, ICU patients often find it difficult to maintain their dignity independently, thus requiring nurses to assume the roles of protectors, advocates, and interpreters of patients’ humanistic values. At the same time, the technology-driven and fast-paced environment of the ICU is prone to inducing dehumanization, loss of privacy, forced interventions, and value conflicts surrounding life-sustaining treatments. 17 Under these dual pressures, the depth of nurses’ understanding of the essence of dignity, their vulnerability when facing moral dilemmas, and their ability to make ethical judgments and take action amid multiple value tensions directly determine whether patients’ dignity is maintained or eroded.
The global aging of the population further intensifies this ethical dilemma. According to a report from the United Nations Department of Economic and Social Affairs, 18 9% of the world’s population was aged 65 or older in 2019, a proportion projected to reach 16%—approximately one-sixth of humanity—by 2050. As populations age, the number of older patients admitted to ICUs continues to increase, and this group is gradually becoming a dominant segment of the critically ill population.19,20 These patients are typically frail, burdened with chronic diseases, and because of cognitive decline, heightened dependency, or restricted autonomy, they are particularly susceptible to violations of dignity. 21 In this global context, the ethical responsibility of ICU nurses to safeguard the dignity of older patients has grown increasingly critical and complex.
Methods
Study design
This study employed an explanatory sequential mixed-methods design. In Phase I, a questionnaire survey was administered to examine the current status and influencing factors regarding ICU nurses’ maintenance of the dignity of older patients. In Phase II, ICU nurses were selected for semi-structured interviews based on survey findings, and a descriptive phenomenological approach was used for in-depth exploration. This study followed the reporting standards outlined in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement and Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.
Social Cognitive Theory (SCT) 22 was adopted as the overall theoretical framework. SCT highlighted the reciprocal interactions among the individual, environment, and behavior, focusing on how individuals perceive, process, and respond to information within social contexts while underscoring their agency in behavioral decision-making. This aligned with the construct of moral subjectivity in nursing ethics: in ethical scenarios, nurses were not only shaped by environmental factors but also exercised autonomous judgment to make moral decisions. Guided by this framework, the quantitative phase classified nurses’ demographic characteristics, moral sensitivity, and psychological capital as individual factors, and the nursing work environment as an environmental factor. Dignified care toward older patients was defined as the target behavior and assessed in terms of its overall level and associated influencing factors. The qualitative phase utilized semi-structured interviews to capture practical experiences and contextual nuances that were difficult to obtain through quantitative methods. Ultimately, this study integrated quantitative and qualitative findings through the SCT structure of “person–environment–behavior,” thereby constructing a theoretical framework for the multidimensional influencing mechanisms underlying ICU nurses’ implementation of older-patient dignity care.
Participants and setting
During the quantitative phase, convenience sampling was used to distribute online questionnaires to ICU nurses from 5 tertiary hospitals in Hunan Province. The sample size was determined using Liang’s sample size table, 23 yielding an initial recommended sample size of 384 participants (95% confidence level, 5% margin of error). After accounting for a 10% anticipated invalid questionnaire rate, the final sample size was increased to at least 427. In the qualitative phase, purposive sampling was used, and participants were selected from the preceding quantitative phase sample according to the principle of maximum variation. Selection emphasized diversity in gender, age, years of clinical experience, professional title, educational level, and training history to ensure sample representativeness. The sample size was determined by theoretical saturation; data collection stopped when no new concepts or themes emerged from additional interviews. Eligibility criteria included (1) registered nurses currently in active practice; (2) a minimum of 1 year of ICU experience; exclusion criteria comprised: (1) temporary unavailability due to leave or off-site training commitments; (2) refusal to participate.
Instruments
ICU dignified care questionnaire (IDCQ)—An instrument for evaluating nurses’ dignified care behaviors toward older patients
The IDCQ, 23 developed by Chinese scholar Liang et al., consists of 17 items across two dimensions: absolute dignity (items 1–9) and relative dignity (items 10–17). It employs a 5-point Likert scale, yielding total scores ranging from 17 to 85. Behavioral performance is quantified through standardized scores calculated as (actual score − 17)/(85 − 17) × 100. A score of ≥ 80 indicates good behavior, 60–79 indicates moderate behavior, and <60 indicates poor behavior. The instrument demonstrates rigorous psychometric properties, evidenced by a Cronbach’s α coefficient of 0.94 and test-retest reliability of 0.88.
Nursing work environment scale—An instrument for evaluating environmental factors
The Nursing Work Environment Scale 24 was developed by Chinese scholars Jing Shao et al. This scale comprises seven dimensions totaling 26 items, structured as follows: professional development (items 1–5), leadership and management (items 6–9), nurse-physician relationships (items 10–13), recognition climate (items 14–16), professional autonomy (items 17–20), basic security (items 21–23), and staffing adequacy (items 24–26). Each item is rated on a 6-point Likert scale ranging from 1 (“strongly disagree”) to 6 (“strongly agree”), yielding total scores ranging from 26 to 156. Higher scores indicate more favorable perceptions of the nursing work environment. The full scale demonstrated a Cronbach’s α coefficient of 0.946 and split-half reliability of 0.894, confirming good psychometric properties.
Instruments for evaluating individual factors
Basic information questionnaire for ICU nurses
Developed through literature review, consultations with domain experts, and panel discussions, the questionnaire included items designed to collect nurses’ sociodemographic characteristics and professional practice information.
The moral sensitivity questionnaire-revised Chinese version (MSQ-R-CV)
The MSQ-R-CV 25 is the officially revised Chinese version of the original international scale, adapted for use among Chinese nurses. This scale comprises two dimensions: “ethical responsibility and strength” (5 items) and “sense of moral burden” (4 items). A 6-point Likert scale is employed, where 1 indicates “strongly disagree” and 6 “strongly agree.” Total scores range from 9 to 54, with higher scores reflecting greater moral sensitivity. The full scale demonstrates a Cronbach’s α coefficient of 0.82 and split-half reliability of 0.75, indicating strong reliability for assessing nurses’ moral sensitivity.
Chinese Psychological Capital Questionnaire-Revised for nurses
The questionnaire was developed by Hong Luo 26 based on Chaoping Li’s translation of the Psychological Capital Questionnaire, originally compiled by Luthans, and was further adapted to fit the current nursing context in China. This 20-item questionnaire comprises four dimensions: self-efficacy (6 items), hope (6 items), resilience (5 items), and optimism (3 items). All items employ a 6-point Likert scale (1 = “strongly disagree” to 6 = “strongly agree”), yielding total scores ranging from 20 to 120. Higher scores correspond to greater psychological capital. Subscale Cronbach’s α coefficients range from 0.707 to 0.927, with test-retest reliability values between 0.771 and 0.863, demonstrating high reliability and stability.
Qualitative research tool—semi-structured interview outline
Based on the literature review and discussions within the research team, an initial interview guide was drafted and revised after two pilot interviews. The content includes ① How do you understand the concept of “dignity”? ② What is your view on maintaining the dignity of older patients? ③ What do you think dignity means to older patients? ④ What nursing behaviors do you think would affect the dignity of older patients? ⑤ What facilitating or hindering factors in nursing practice do you think would affect your maintenance of the dignity of older patients? Which factors are the most important? ⑥ Do you have any suggestions regarding maintaining the dignity of older patients in nursing practice? ⑦ Is there anything that was not mentioned in this interview but you think is very important?
Data collection
The questionnaire survey was conducted from January 2025 to June 2025. Electronic questionnaires were developed using Wenjuanxing (a Chinese online survey platform). After obtaining approval from the nursing departments of the participating hospitals, ICU head nurses distributed the questionnaire QR codes through WeChat work groups, explaining the research purpose and inclusion/exclusion criteria for participants. Nurses voluntarily and anonymously completed the questionnaires, which required full completion of all items before submission. A total of 43 pilot questionnaires (10% of the projected sample size) and 533 formal questionnaires were distributed, yielding 487 valid questionnaires, resulting in an effective response rate of 91.37%.
The qualitative interviews were conducted in quiet nurse duty rooms from June 2025 to August 2025. One-on-one, face-to-face, semi-structured interviews were carried out using an interview guide with open-ended questions, accompanied by follow-up probing to facilitate in-depth elaboration. Theoretical saturation was achieved after 18 interviews, when no new themes emerged, and data collection was therefore terminated. All interviews were audio-recorded and lasted approximately 25 min on average.
Data analysis
In the first phase, quantitative data were analyzed using IBM SPSS 27.0. Descriptive statistics were applied to analyze demographic characteristics and questionnaire data. Normality was assessed using the Shapiro-Wilk test and histograms, while homogeneity of variance was evaluated via Levene’s test. The results indicated that the data were approximately normally distributed and that the assumption of homogeneity of variance was satisfied. Therefore, parametric statistical methods were employed, including independent-samples t-test, one-way analysis of variance (ANOVA), Pearson correlation analysis, and multiple linear regression, to examine influencing factors. Statistical significance was set at P < 0.05.
In the second phase, qualitative data were analyzed using Colaizzi’s 7-step phenomenological method 27 in NVivo 12.0. The steps included (1) repeatedly reading the transcripts to gain familiarity with the interview content; (2) identifying and extracting key statements related to maintaining older patients’ dignity; (3) coding and conceptualizing recurring significant viewpoints; (4) developing preliminary themes by comparing and integrating similar concepts; (5) producing detailed descriptions of these themes supported by verbatim quotations; (6) refining and integrating themes into higher-level core themes; and (7) validating the final thematic structure with a subset of participants.
For data integration, the quantitative findings were compared and integrated with the qualitative themes to identify areas of convergence and complementarity. These results were combined within an integrated framework, thereby providing a more comprehensive and multidimensional understanding of the factors influencing ICU nurses’ dignified behaviors toward older patients.
Rigor
All research team members held postgraduate degrees or higher and had received systematic training in questionnaire survey administration and qualitative research methodologies. The following approaches were implemented to ensure methodological rigor: composing reflexive journals to control potential biases; conducting pilot surveys and pilot interviews to assess feasibility; excluding questionnaires with consecutive identical responses, duplicate IP addresses, or completion times under 3 minutes; using probing techniques such as repetition and counter-questioning to encourage participants to express their authentic perspectives; two researchers independently coded the interview data, with a third researcher consulted when necessary to resolve discrepancies; and returning the interview findings to participants for confirmation through member checking.
Ethical considerations
This study was approved by the Ethics Committee of Hunan Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Approval No. 2024-236). In the quantitative phase, the online questionnaire was administered via a non-affiliated external platform, and no personally identifiable information was collected to ensure respondent anonymity. The first page of the questionnaire clearly stated the study objectives, the principle of voluntary participation, and the right to withdraw at any time; completion and submission of the questionnaire were considered to constitute informed consent. Prior to the qualitative interviews, all participants provided written informed consent. Interview data were anonymized and used exclusively for research analysis to ensure participant privacy and confidentiality.
Results
Quantitative results
Participants’ characteristics
This study included 487 ICU nurses from Changsha, Hunan Province. The participants were predominantly female (77.4%), with a mean age of 29.70 ± 4.54 years, of whom 49.3% were in the 26–30 age group. They had an average of 7.91 ± 4.29 years of ICU working experience, a monthly night-shift frequency of 6.69 ± 2.92 days, and a mean monthly income of ¥9416.84 ± ¥2933.28. The cohort comprised 62.4% married individuals, 73.3% with a bachelor’s degree or higher, and 70.5% holding primary professional titles. Regarding professional training, 68.4% of nurses had received education in geriatric nursing, and 66.7% had studied nursing ethics.
ICU nurses’ dignified care behaviors toward older patients
Scores of IDCQ (n = 487).

Univariate analysis
Demographic characteristics and univariate analysis of geriatric dignified care behaviors among ICU nurses (n = 487).
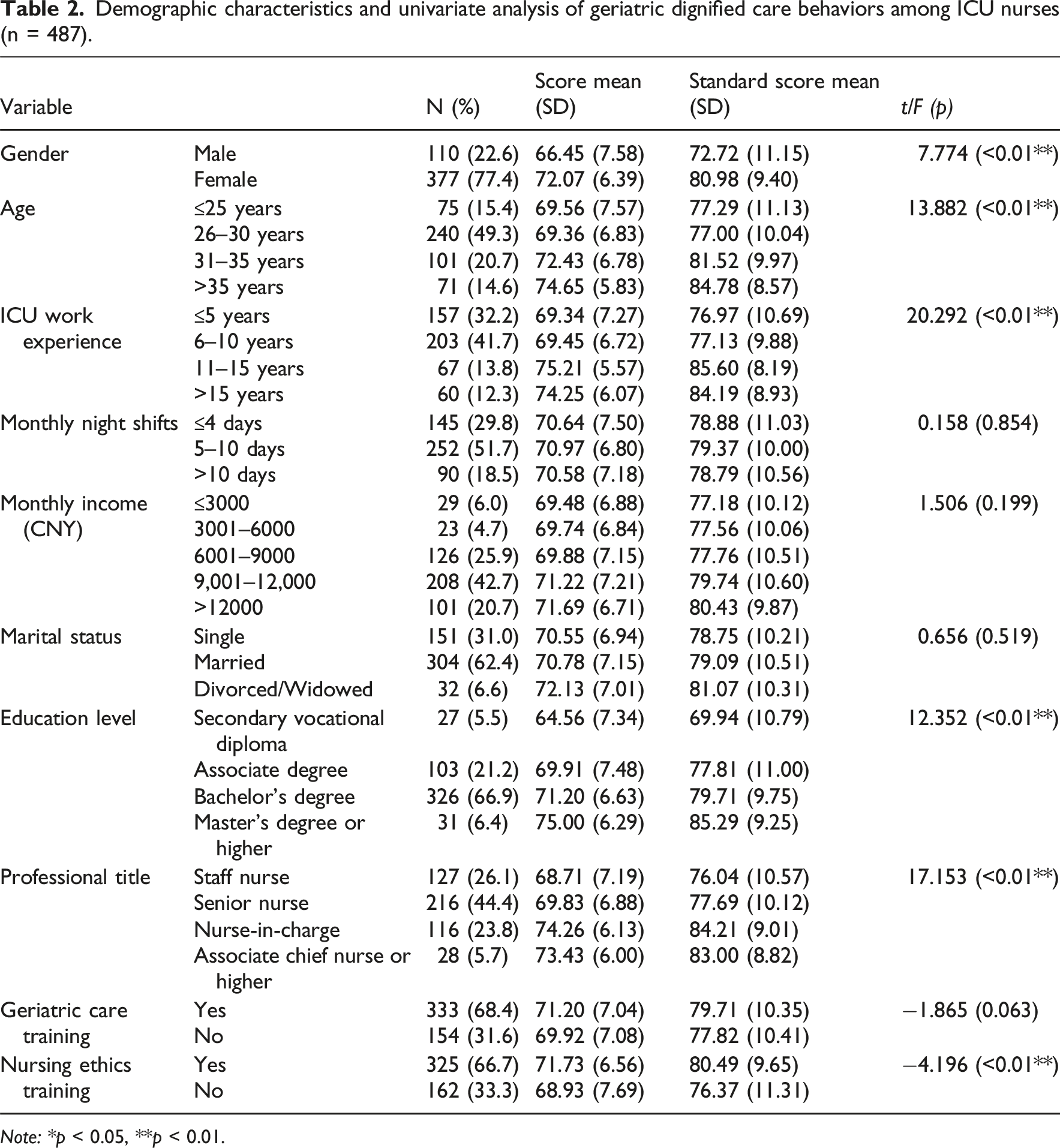
Note: *p < 0.05, **p < 0.01.
Pearson correlation analysis
Pearson correlation analysis revealed significant positive correlations between nursing work environment, moral sensitivity, psychological capital, and the dignified care behaviors of ICU nurses toward older adults (r = 0.492, 0.447, 0.392; P < 0.01).
Multiple linear regression analysis
Multiple linear regression analysis of geriatric dignified care behaviors among ICU nurses (n = 487).
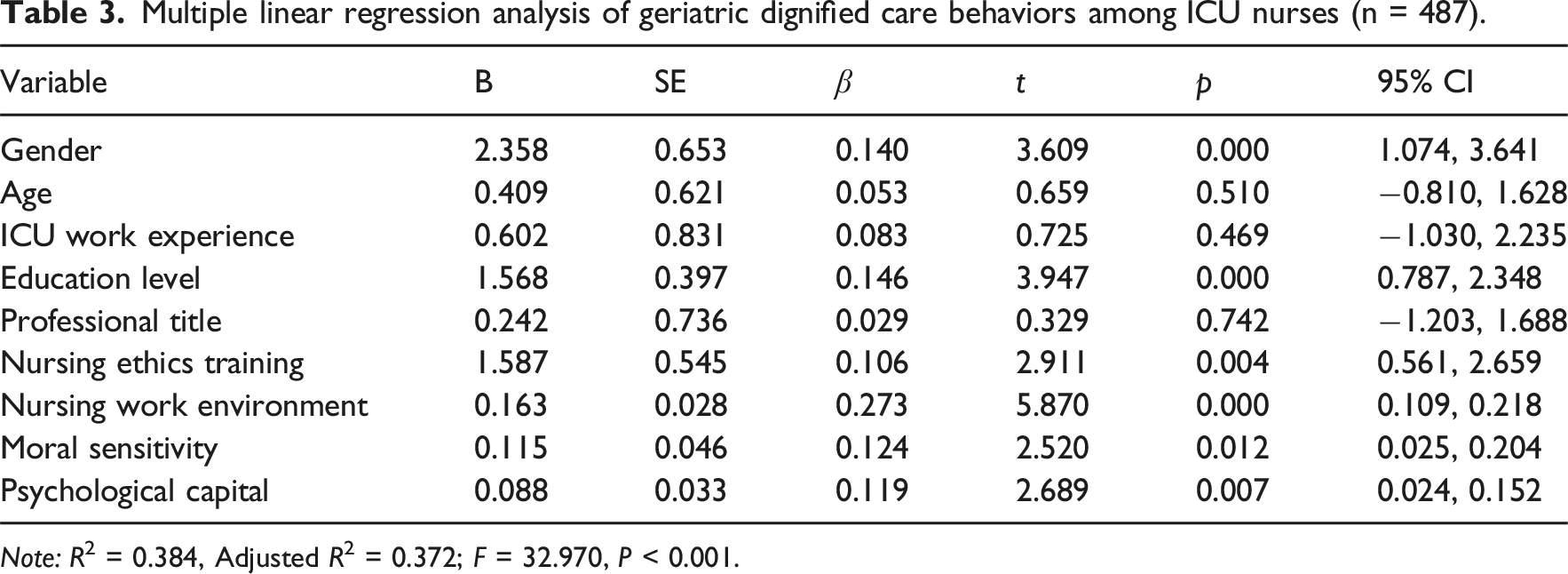
Note: R2 = 0.384, Adjusted R2 = 0.372; F = 32.970, P < 0.001.
Qualitative results
Theme 1: Nurse factors
Dilemma between technical procedures and dignity preservation
ICU nurses constantly face value choices between standardized procedures and protecting older patients’ dignity during clinical procedures. This conflict is particularly prominent in the care of private areas, and the practical need for operational convenience often leads to the simplification of privacy protection measures. Especially in emergency medical situations, this contradiction is further magnified, creating an intractable practical dilemma.
N17: “Some older patients attach great importance to personal dignity, but for the convenience of nursing tubes, we just drape the clothes over the patients.”
N1: “When caring for patients, there will inevitably be conflicts with maintaining their dignity. For instance, procedures such as perineal care and bed baths may make patients feel that their privacy is exposed. These concerns become a lower priority during emergency resuscitation, as saving lives always comes first.”
Individual differences in nurses’ emotional investment
Research findings suggest that nurses’ personality traits directly impact their sensitivity in dignified care. Nurses with keen observational skills demonstrate a heightened awareness of the dignity needs of older patients, whereas colleagues with less meticulous dispositions may overlook these critical details.
N4: “Some nurses are naturally meticulous, while others may be careless and pay less attention to dignity. Certain individuals might also think it does not matter and do not care so much. As a result, older patients’ dignity needs are often unmet in many cases.”
As clinical experience accumulates and age advances, nurses’ empathetic capacity toward older patients tends to strengthen. However, prolonged exposure to high-intensity work environments may lead to job burnout among experienced nurses, fostering emotional numbness toward human life. This state of emotional exhaustion weakens their inherent drive to preserve the dignity of older patients.
N17: “When I started working, I was nervous about caring for older patients. They have multiple chronic conditions and poor veins, which made me anxious about giving them injections. However, as I gained more experience and aged, I came to understand their emotional needs more deeply.”
N6: “After working in this field for too long, some colleagues have indeed become numb, developing a sense of indifference toward life and older patients.”
Theme 2: Patient factors
Moderating role of disease severity
Within the ICU’s clinical decision-making framework, the medical primacy principle places patients’ physiological stability above all other concerns. This illness-centered care paradigm often results in reduced attention to the dignity of older patients. ICU nurses adjust their care strategies based on patients’ levels of consciousness, creating a tiered pattern of dignity-related attention.
N10: “ICUs focus primarily on older patients’ medical conditions, with no specific focus on their dignity.”
N17: “Sometimes we have to restrain delirious older patients. (sighs) I know this might harm their dignity, but if we let them pull out their tubes, it could cause life-threatening consequences. So ultimately, we prioritize their medical needs above all else.”
N4: “If the patient is conscious, we tend to afford him more dignity. For patients with confused consciousness, we pay less attention to maintaining their dignity. Firstly, they have less space for expression and choice. Secondly, they are less aware of many things.”
Constraining effects of low therapeutic adherence
Low treatment adherence among older patients creates multifaceted constraints on dignified care practices in ICUs. Some older patients develop negative perceptions of nurses based on societal stereotypes before their first clinical encounter, and these preconceived biases can hinder the implementation of dignity-preserving care.
N9: “The perception of our profession by the entire society also affects my dignified care for patients, because respect is mutual. Some older people have a prejudice against nurses. As soon as they enter the ICU, they say we are unreliable and think our attitude is bad, but in fact, we have not even interacted with them yet.”
The moment-to-moment compliance issues during treatment are even more intricate. When there is a discrepancy between older patients’ treatment expectations and the actual medical circumstances, they often exhibit more overt resistance, making it difficult for nurses to deliver care that fully aligns with the patients’ intentions.
N14: “Some older patients want to be discharged or transferred to a general ward, but their physical condition has not yet met the discharge criteria, and they cannot be moved out of the ICU. At this time, the patients may refuse to cooperate with treatment and nursing operations to express their dissatisfaction, which in turn makes it impossible for us to respect their opinions.”
Theme 3: Cultural factors
Cultural logic of familial decision-making
In the ICU, older patients are in a doubly disadvantaged position, both physiologically and socially. As a result, decision-making authority often shifts to family members, leading to a surrogate decision-making model. Under this model, hospital protocols usually require family members, rather than the patients themselves, to sign the consent forms. This situation inevitably shifts the focus of nursing care toward meeting family members’ expectations, potentially overlooking older patients’ individual will.
N3: “When older patients lose communication capacity or face unaffordable medical costs, their decision-making authority diminishes significantly within family structures. They become passive observers, following their children’s arrangements without expressing personal preferences.”
N8: “Even when patients are fully lucid, we have never sought their signatures. Instead, we always ask the family members to sign. Moreover, when determining the treatment approach for patients, we generally follow the opinions of the family members rather than those of the patients.”
However, family members’ considerations may encompass multiple factors, and may even involve mutually conflicting ones. Some family members, motivated by a desire to safeguard the patient’s dignity, are reluctant to see their relatives sustained in a highly medicalized state surrounded by medical equipment. Conversely, others may be inclined to continue life-sustaining treatment for practical reasons, including economic considerations.
N15: “For some patients, their family members prefer to maintain the patient’s dignity and do not want to see them lying there with various tubes inserted. They ask us to try to keep the patient’s skin clean and intact.”
N1: “For such retired senior cadres, as long as their hearts are still beating, they will receive a high pension. At this stage, their families may not necessarily give up treating them.”
Professional internalization of elder-respecting values
Traditional Chinese values such as “extending familial reverence to all elders” have been integrated into nursing behavioral guidelines. This cultural consciousness orients ICU nurses in China to prioritize older patients as the primary recipients of compassionate care, thereby forming a humanistic care foundation rooted in an elder-respecting culture.
N17: “I firmly believe in the truth of China’s ancient teaching: ‘Respect the elderly in your family as well as others; cherish the young in your home as well as those beyond’. Our cultural heritage continues to influence how we honor the dignity of older patients positively.”
N7: “In our country, there has long existed a prevailing concept that people should respect the older and care for the young. This value is deeply ingrained in the national psyche and is widely recognized and practiced by the public.”
Theme 4: Organizational factors
Objective constraints of workload
In the high-pressure environment of the ICU, a heavy nursing workload often limits nurses’ ability to fully attend to the psychosocial needs of older patients. Particularly when managing multiple critically ill patients concurrently, the preservation of patient dignity often becomes secondary to the provision of more immediate, life-sustaining medical care.
N10: “ICU patients really need someone to stay with them, but we are always so busy with work that we often cannot take full care of their mental state.”
N11: “I think being busy itself is a problem. Sometimes nurses care for four patients at the same time. Some aspects may not be done well when all the patients need help, especially when conscious patients are among them.”
Implicit construction of working atmosphere
The distinctive work climate within ICUs exerts a subtle yet profound influence on nurses’ awareness of preserving patient dignity. Prolonged exposure to this specific professional environment leads to the unconscious internalization of shared behavioral norms and value orientations within clinical teams. Such cultural conditioning often operates beyond individual cognitive awareness.
N8: “I believe that neglecting to safeguard patients’ dignity is an unfavorable phenomenon. However, it may be the case that each of us approaches patient care in this manner. Over time, such practices become habitual, leading to a diminished focus on the issue of patients’ dignity.”
N12: “When I was newly practicing, how to specifically preserve patients’ dignity was mainly shaped by my clinical preceptor’s example. The impact would have been different if their professional conduct had been more standardized.”
N14: “Our head nurse treats every patient equally, regardless of their emotional state. During busy shifts when we cannot comfort patients, she steps in to calm them, ensuring treatment cooperation.”
Results of the integrated data
Guided by the triadic reciprocal determinism of SCT, this study identified the factors influencing ICU nurses’ dignified care toward older patients and integrated the quantitative and qualitative findings into a comprehensive theoretical framework (Figure 1). Integrated analysis revealed that the two strands of evidence were directionally consistent and complementary. The quantitative phase identified key individual and environmental factors influencing dignified care, while the qualitative phase further illuminated how these factors operate in clinical contexts and revealed additional contextual influences not captured quantitatively. Taken together, the integrated findings demonstrate that dynamic interactions between the “environmental system” and the “individual system” shape ICU nurses’ dignified care toward older patients. Conceptual framework of factors influencing ICU nurses’ dignified care for older patients.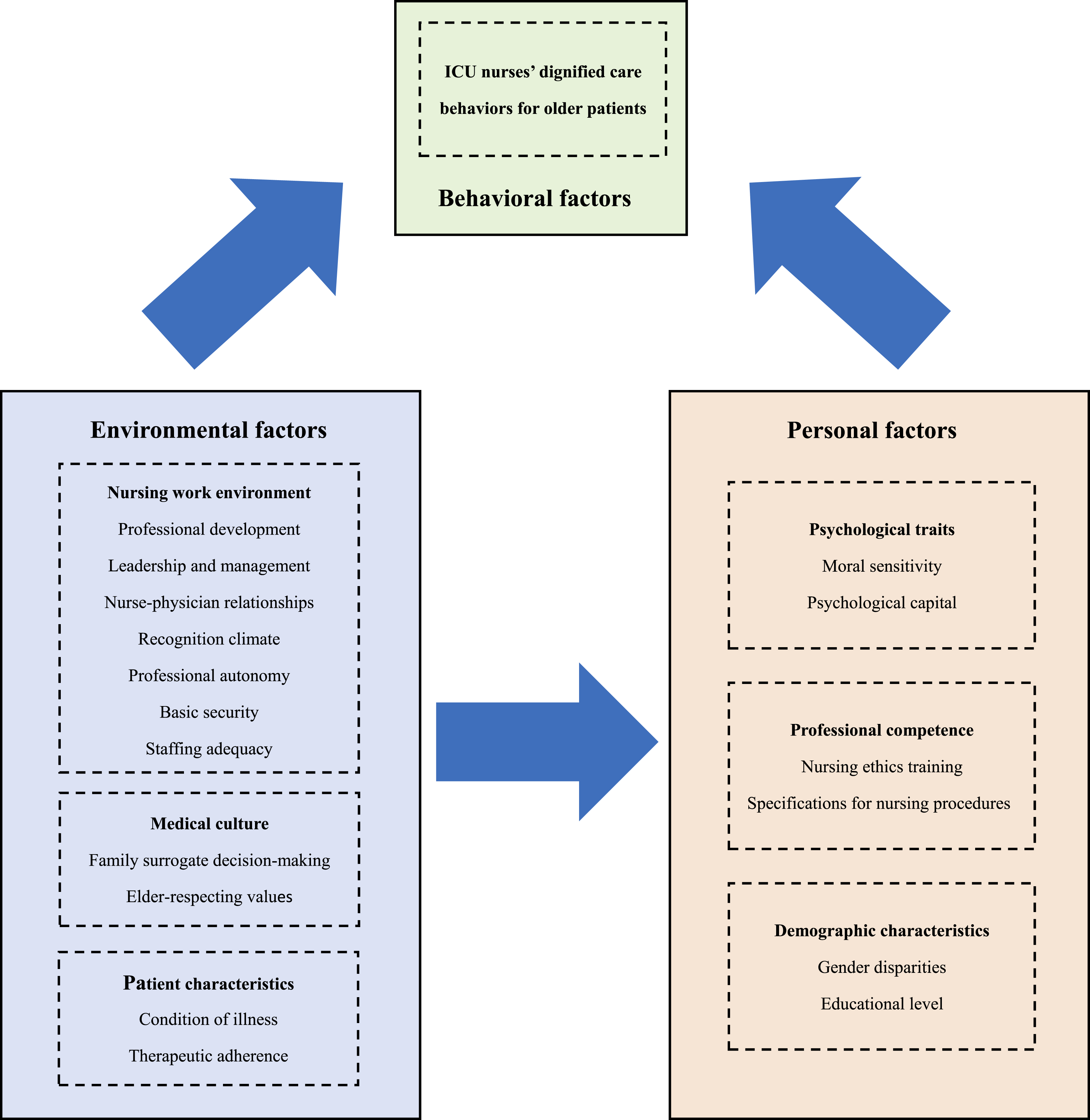
Discussion
The results of this study indicated that ICU nurses’ overall performance in maintaining the dignity of older patients was at an upper-mid level, approaching a generally positive standard. This study systematically identified key factors influencing dignity-focused care behaviors through a mixed-methods approach. The quantitative findings demonstrated that the nursing work environment, psychological capital, ethical sensitivity, and nursing ethics training constituted the primary influencing factors, while individual characteristics such as gender and education also exerted significant effects. The qualitative analysis further uncovered multiple challenges in clinical practice, including ethical tensions between technical procedures and dignity preservation, varying influences of patient characteristics, the profound impact of medical culture, and structural constraints within organizational systems.
The specific data showed that ICU nurses’ average total score in maintaining older patients’ dignity-related behaviors was 70.80 ± 7.07 points, with a converted standardized score of 79.12 ± 10.40 points, indicating that current ICU nursing practices generally meet the dignity needs of older patients, although there remained room for improvement in certain aspects. Notably, the results of this study were slightly better than those reported by Liang et al., 23 which may be related to the increasing emphasis on humanized care in ICUs in recent years and the ongoing implementation of relevant training programs.28,29 The study further revealed that ICU nurses performed relatively better in maintaining “absolute dignity” (e.g., fundamental and life-sustaining care), while their performance in preserving “relative dignity” was comparatively weaker. According to Edlund’s ontological theory of dignity, 4 absolute dignity derives from the inherent worth of the human being and is more easily upheld in ICUs, where life-sustaining interventions and fundamental care predominate. In contrast, relative dignity depends on understanding, responsiveness, and respect within interpersonal interactions and is shaped by factors such as patients’ life histories and social identities. In the highly technologized and physiologically driven ICU environment, opportunities for individualized communication and relational care are often limited, which may hinder the realization of relative dignity. For older patients, equal treatment, the avoidance of age-related bias, and respect for individual rights are considered more important than “assistance with activities of daily living”, 30 and these needs form the core elements of relative dignity. Therefore, ICU nurses should ensure the quality of fundamental care while paying greater attention to identifying and responding to the individualized dignity needs of older patients.
Regarding nurses’ individual characteristics, this study found that female ICU nurses with advanced educational attainment demonstrated superior performance in preserving the dignity of older patients. Female nurses, through socialization processes that foster empathy and interpersonal connectedness, often develop strong interpersonal communication skills; meanwhile, higher education enhances nurses’ theoretical competence, critical thinking, and communication abilities.31,32 These attributes facilitate the identification of older patients’ individualized needs and the management of complex ethical situations. Previous research 33 similarly observed that female nurses and those with graduate-level education in ICUs typically exhibit stronger empathic capacities and humanistic care competencies. Beyond educational background and gender, ICU nurses’ professional literacy and ethical awareness were also identified as critical individual factors. Professional ethics, as foundational requirements for nursing practice, provide essential guidance for establishing effective nurse-patient relationships 34 —a core element in delivering dignity-centered care. Gherman et al. 35 noted that nurses with heightened ethical sensitivity demonstrate a greater ability to adopt older patients’ perspectives and maintain professional standards when confronting ethical dilemmas, findings that align with ours. Simultaneously, empathy serves as a crucial intrinsic motivator for ICU nurses, enabling older patients to feel valued. Compassionate nurses demonstrate heightened attentiveness to patients’ needs and distress, thereby enabling them to deliver more individualized and clinically appropriate care. 36 However, the ICU nurses in this study were vulnerable to compassion fatigue, which may lead to disrespectful behavior. This finding aligns with Xie et al.’s systematic review, 37 suggesting that ICU nurses are more predisposed to such a psychological state than nurses in other departments.
Within the domain of external environmental influences, patient characteristics, medical culture, and workplace conditions collectively constitute a complex interactive system. ICU nurses commonly perceive that impaired health status and advanced age render geriatric ICU patients more vulnerable than other populations, predisposing them to loss of situational control and communication exclusion, 38 thereby jeopardizing their dignity. Our findings demonstrated that the observable characteristics of older ICU patients that predispose them to dignity impairment often lead nurses to prioritize physical care while providing comparatively less emotional support. Concurrently, older patients’ preconceived biases toward nurses substantially reduced treatment adherence, thereby hindering the implementation of dignity-centered care. Relevant studies 39 have indicated that patients’ preconceptions about nurses pose formidable barriers, and addressing this challenge requires “understanding the world through others’ perspectives” by focusing on individual characteristics rather than relying on prejudices and stereotypes. Within the cultural dimension, gerontological respect, as an important traditional value, encourages nurses to prioritize the dignity of older patients. 40 Nevertheless, the currently prevalent family-dominated decision-making model is rooted in collectivist and filial piety cultures. While this model emphasizes family responsibility, it may inadvertently limit older patients’ ability to express their preferences and marginalize their autonomous decision-making. 41 The present study indicated that, within such a cultural context, ICU nurses must simultaneously respond to societal expectations that prioritize filial duty and the professional ethical mandate to respect patient autonomy, creating pronounced value tensions and ethical dilemmas in the provision of dignified care. Concerning workplace environmental factors, ICU-specific structural constraints—particularly staffing shortages and excessive workloads 42 —compelled nurses to make triage decisions in resource-scarce environments. These pressure-driven prioritization patterns frequently compromised patient autonomy and psychosocial needs, constituting major barriers to the quality of dignified care. Conversely, environments characterized by collegial collaboration and sufficient resource allocation can significantly enhance nurses’ professional satisfaction and identity, thereby fostering more favorable conditions for dignity-centered care practices.
Based on the findings above, it is recommended to implement multidimensional and systematic improvement strategies: First, in team development, a “dignity-care mentorship system” should be established under the guidance of managers with ethical leadership qualities, and highly educated female nurses may be encouraged to assume an exemplary role in humanistic care, thereby enhancing the team’s overall capacity for dignified care through value modeling and moral guidance. Concurrently, stratified training is recommended, with a focus on strengthening junior nurses’ ethical decision-making capabilities and communication skills. Second, regarding the educational system, medical ethics and geriatric dignity care courses should be integrated into continuing education, with the adoption of interactive teaching methods to strengthen nurses’ moral sensitivity and cultural competence. Third, for mental health support, it is necessary to establish a routine psychological intervention mechanism, such as screening for compassion fatigue, providing psychological counseling, and organizing stress-relieving activities, to enhance nurses’ psychological capital. Fourth, in terms of management systems, dignity care quality indicators should be incorporated into performance evaluations, supported by positive incentive mechanisms. Additionally, optimizing the ICU work environment, staffing allocation, and nursing processes will provide structural support for dignity care practices. Finally, regarding cultural development, cultivating a dignity-confirming care culture enables respect for patients’ subjectivity and life histories to become a shared team ethic. On this basis, traditional elder-respect values and family decision-making models should be harmonized, and a multi-stakeholder communication mechanism involving patients, families, and medical teams should be established to promote value alignment. These strategies require sustained policy and resource support from management, as well as strengthened interdepartmental collaboration, to systematically enhance the quality of dignity care for geriatric ICU patients.
Strengths and limitations
This study demonstrates three key strengths. First, the mixed-methods design enhances methodological rigor by allowing for mutual corroboration of quantitative and qualitative findings, with the qualitative component providing deeper contextual interpretation. Second, the development of a multilevel analytical framework systematically integrates environmental and individual factors, elucidating the mechanisms underlying nurses’ dignity-preservation practices and establishing a theoretical foundation for future research. Third, the explicit focus on culturally specific dynamics within the Chinese healthcare context, particularly the tension between traditional elder-respect norms and family decision-making patterns, strengthens the cultural relevance of the findings.
However, limitations must be acknowledged. First, the sample sources are relatively concentrated with limited geographical coverage, which may compromise the external validity of the findings. Second, the study relies primarily on self-report measures derived from a single data source, which may be subject to social desirability bias and common-method bias. Third, the research is conducted mainly from the nurses’ perspective, lacking a systematic investigation of patients, their families, and members of the multidisciplinary team, thereby limiting a comprehensive understanding of dignified behaviors in relational contexts. Future research could employ multi-center and longitudinal designs to enhance sample representativeness. It may also combine observational methods and multi-informant assessments to reduce self-report and method biases. In addition, incorporating patients’ and their families’ experiential data would help more fully explore factors influencing dignified care and provide more targeted recommendations for clinical practice.
Conclusion
This study systematically investigates the current status and influencing factors of ICU nurses’ dignity-preservation practices for older patients. The findings reveal that while nurses demonstrate a moderate to high overall level of dignity maintenance, there remains considerable room for improvement in preserving “relative dignity.” The dignity-preserving behaviors of ICU nurses are shaped through a dynamic interplay between individual characteristics and environmental factors. Professional competencies, psychological traits, and demographic characteristics constitute the internal foundation for nurses to implement dignity-centered care. The clinical work environment not only directly influences nursing practices but also indirectly affects behaviors by shaping psychological capital and other individual attributes. Traditional cultural values of respect for older adults, family decision-making patterns, and patient-specific factors (including clinical status and treatment adherence) collectively mediate nurses’ behavioral choices to varying degrees. Based on these findings, we propose three key improvement strategies: optimizing clinical environments, enhancing continuing education programs, and establishing comprehensive support systems. These measures require systematic planning and sustained implementation by hospital management to continuously improve the quality of dignity-centered care and achieve excellence in geriatric critical care services.
Footnotes
Acknowledgments
We gratefully acknowledge the financial support from Hunan University of Chinese Medicine, the Department of Science and Technology of Hunan Province, and the Hunan Provincial Health Commission. Our sincere thanks extend to all researchers, participating institutions, and study participants for their invaluable contributions to this work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Innovation Project for Postgraduate Students of Hunan University of Chinese Medicine (Grant number: 2024CX184), the Natural Science Foundation of Hunan Province (Grant number: 2024JJ8200), and the Scientific Research Project of the Hunan Provincial Health Commission (Grant number: 20257723).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.