
Abstract
Background
Home-based end-of-life palliative care presents unique ethical challenges that differ fundamentally from those in institutional settings. Healthcare professionals navigate the complex role of being both clinical experts and guests in patients’ domestic environments, operating in a context where professional authority is continuously negotiated rather than institutionally established.
Research aim
This study examines the ethical tensions healthcare professionals encounter in home-based end-of-life palliative care and explores the strategies they employ to balance and negotiate competing ethical values within patient-family relationships.
Research design
A qualitative study using thematic content analysis conducted through focus groups and semi-structured interviews.
Participants and research context
Thirty-three multidisciplinary healthcare professionals from Israeli home-based hospice care participated, all employed by a national organization specializing in home-based medical services. Data was collected through three profession-specific focus groups (physicians, nurses, social workers) and nine semi-structured interviews with organizational leaders.
Ethical considerations
The study was approved by the Institutional Review Board. All participants provided written informed consent, were assured confidentiality and anonymity, and informed of their right to withdraw without consequences.
Findings
Two interrelated themes were identified. “From Guest to Clinician” describes how professionals balance clinical authority with domestic sovereignty, manage involuntary exposure to private patient information, and develop “protective witnessing,” a deliberate ethical practice of selective attention preserving patient dignity. “Distributed Responsibility in Multi-Stakeholder Care” reveals the paradox of accountability without control: professionals bear clinical responsibility without institutional oversight while working alongside family members as untrained care partners with competing priorities.
Conclusions
Home-based palliative care places professionals at the intersection of clinical responsibility and domestic sovereignty, a position for which existing frameworks offer insufficient guidance. Addressing these structural and relational challenges requires both individual-level preparation, including training in ethical decision-making in low-control environments, and systemic policy reform.
Keywords
Introduction
Home-based end-of-life care positions clinicians as “professional guests” who must deliver expert care within patients’ sovereign domestic spaces. This study examines how interprofessional teams manage the ethical tensions arising from this dual position and from distributed responsibility among patients, families, and providers. We conducted a qualitative study using focus groups and interviews with physicians, nurses, and social workers in an Israeli home hospice organization, identifying key tensions and the practical strategies clinicians adopt to balance competing ethical values in patient-family relationships.
Background
End-of-life care, defined as care provided in the final months or weeks of life, represents a particularly ethically intensive phase of palliative care, characterized by heightened emotional, relational, and clinical complexity.1,2 In home settings, this intensity is compounded by the absence of institutional structures that ordinarily support professionals through this demanding phase. 3
By 2021, approximately 30 home hospice programs were operating nationwide in Israel, providing services through multidisciplinary teams with Health Maintenance Organization coverage, including regular home visits and 24/7 availability. 4 Despite this institutional coverage, significant gaps persist, including inconsistent professional training across providers, unclear delineation of responsibility among care teams, and the absence of standardized protocols for end-of-life discussions in home settings. 5
Contemporary home hospice care relies on multidisciplinary teams of physicians, nurses, social workers, and volunteers who collaborate to address the complex needs of patients and their families.6–8 The home setting can expose staff to professional isolation and moral distress, underscoring the importance of interprofessional collaboration in maintaining ethical sensitivity and enhancing the quality of care.9,10
Ethical tensions arise when competing values or obligations create uncertainty about the appropriate course of action. 3 In home-based palliative care, such tensions are amplified by the absence of institutional structures that ordinarily help professionals manage conflicting responsibilities, including balancing patient autonomy with appropriate care 3 and managing family-centered decision-making. 11 Healthcare professionals in this setting are also vulnerable to moral distress, defined as the negative experience that arises when one knows what the right course of action is but feels constrained from acting on that belief.12,13 The home setting, with its limited institutional oversight and distributed decision-making, is particularly likely to generate such distress, as professionals bear clinical responsibility while lacking the environmental controls available in institutional care.
Family involvement in home care introduces further ethical complexity, particularly when family members request that information be withheld, creating tensions between honest communication and the risk of causing distress.3,14 These communication tensions may also reflect deeply held cultural values: in many cultural contexts, withholding prognostic information from a seriously ill patient is understood as an act of protection and familial care rather than deception, and family members may assume primary decision-making responsibility as an expression of loyalty and duty. 15 In the Israeli context, where diverse cultural and religious communities hold varying orientations toward illness disclosure and family authority, professionals must manage not only individual family dynamics but culturally embedded norms that resist resolution through standardized clinical protocols. 5
The home setting blurs the boundaries between professional and personal relationships, requiring healthcare providers to balance their “professional position” with a “guest position” within a “de-institutionalized” relationship, while maintaining therapeutic effectiveness.3,16 This environment paradoxically exposes patients to greater observation of their living conditions and personal circumstances by visiting professionals, creating tensions around privacy, confidentiality, and dignity.8,17
The relational and contextual nature of ethical challenges in home-based care has been examined within the ethics of care tradition,18,19 which foregrounds responsiveness to relationships over abstract principles and their application. Yet existing studies have predominantly explored these challenges from single-profession perspectives or within non-palliative contexts,3,20 leaving underexamined how professionals actively develop strategies to manage competing values across an interprofessional team. The present study addresses this gap by examining ethical tensions among physicians, nurses, and social workers within a single home hospice organization, while attending to the need to balance relational responsiveness with professional accountability and patient beneficence.
Research aim
This study examines the ethical tensions that healthcare professionals encounter in home-based end-of-life palliative care, exploring the strategies they employ to balance and negotiate competing ethical values within patient-family relationships.
Research design
This study employed a qualitative approach, using thematic content analysis 21 to examine the ethical challenges and concerns encountered by healthcare professionals providing end-of-life care in home settings.
Participants and research context
Participant characteristics (N = 33).
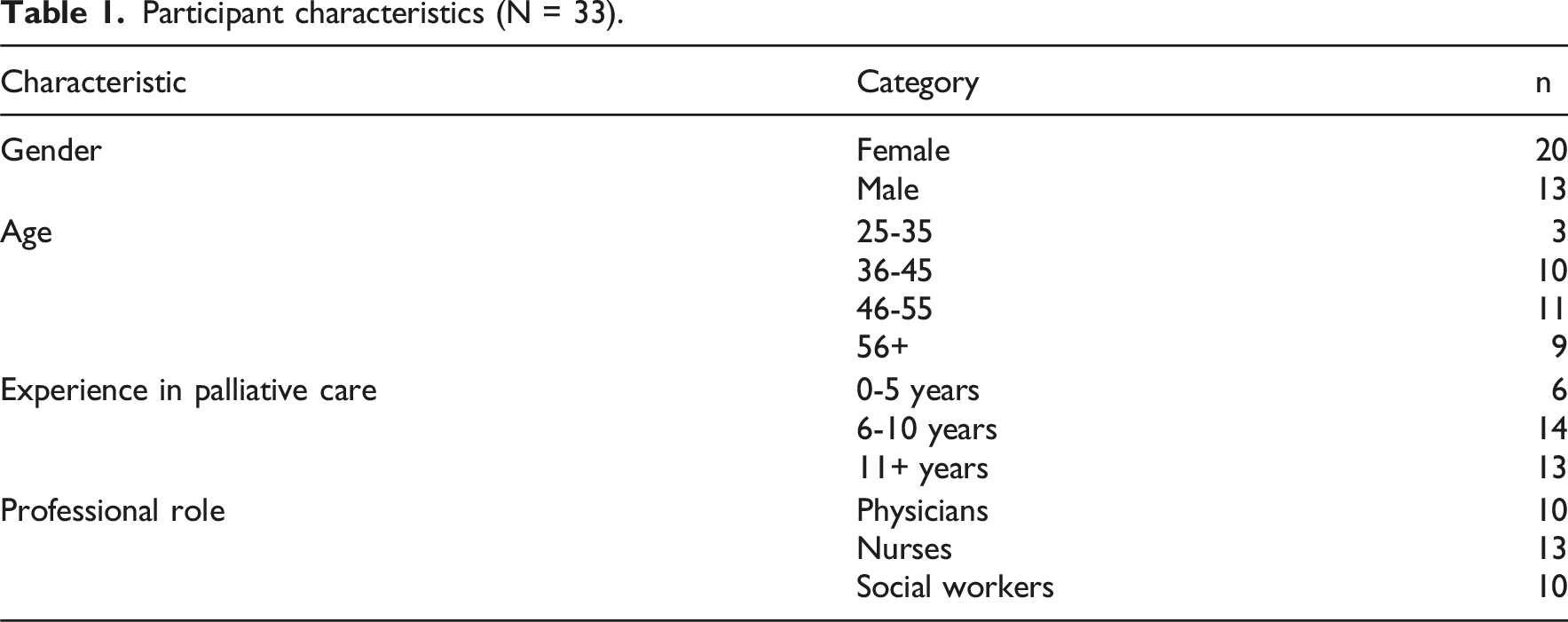
All participants had received formal palliative care training prior to the study. Physicians completed a minimum 80-h in-house palliative care training program; one holds specialist certification in palliative medicine, and two are practicing hospital-based oncologists. Two nurses are certified specialists in supportive care; all remaining nurses completed the 80-h organizational training and hold additional post-basic certifications. Social workers completed both the 80-h organizational program and a structured 60-h advanced training in palliative social work. This level of formal preparation demonstrates that the challenges described reflect structural conditions of domestic care rather than deficits in professional competence. Demographic data is reported in aggregated form to protect participant anonymity.
Data collection
Both interviews and focus groups were conducted via Zoom for logistical reasons related to participants’ availability and accessibility. Each focus group was conducted separately by profession to enable candid within-profession dialogue. Interviews lasted 45-70 min (averaging 55 min); focus groups lasted 70-90 min. An experienced qualitative researcher facilitated all sessions in a conversational, unhurried manner.
Focus groups opened with the framing: “We would like to learn about the ethical challenges, concerns, and deliberations you encounter in your work with people in home-based care.” The term “ethical dilemma” was deliberately avoided in favor of “ethical challenges” to encourage open, experiential description. All sessions were audio-recorded and transcribed verbatim; probing questions were used to deepen understanding. 23 In practice, the ethical concerns described across the three professional groups were notably consistent, reflecting the strong interprofessional collaboration characteristic of home hospice teams.5,10 At the end of each focus group, participants were invited to contact the research team for further support. No participants made contact.
Data analysis
Data analysis was conducted by three researchers with expertise in nursing ethics, end-of-life care, qualitative methodology, and palliative care professional training. This interdisciplinary composition enabled both methodological rigor and contextual sensitivity.
Analysis followed Braun and Clarke’s 21 thematic content analysis, proceeding from familiarization with data through coding, theme identification, and refinement. Researchers independently coded transcripts, then compared and discussed results; interpretive differences were resolved through structured dialogue until full agreement was reached on all themes and sub-themes. Member checking was conducted with a subset of participants to verify interpretive accuracy. Verbatim quotes supported every interpretive claim. 24
Ethical considerations
The Institutional Review Board approved the study [2023-98YVC EMEK]. All participants provided written informed consent, were assured of confidentiality and anonymity, and were informed of their right to withdraw without consequences. The study adhered to the principles of the Declaration of Helsinki and local ethical guidelines for research involving healthcare professionals.
Findings
The analysis identified two primary themes, each with three sub-themes (see Figure 1). These themes address the study’s aim by revealing how domestic settings reshape the ethical landscape of end-of-life care, and how professionals develop strategies to balance and negotiate competing values within patient-family relationships. Thematic framework showing the two main themes and six sub-themes identified in the analysis of ethical challenges in home-based end-of-life care.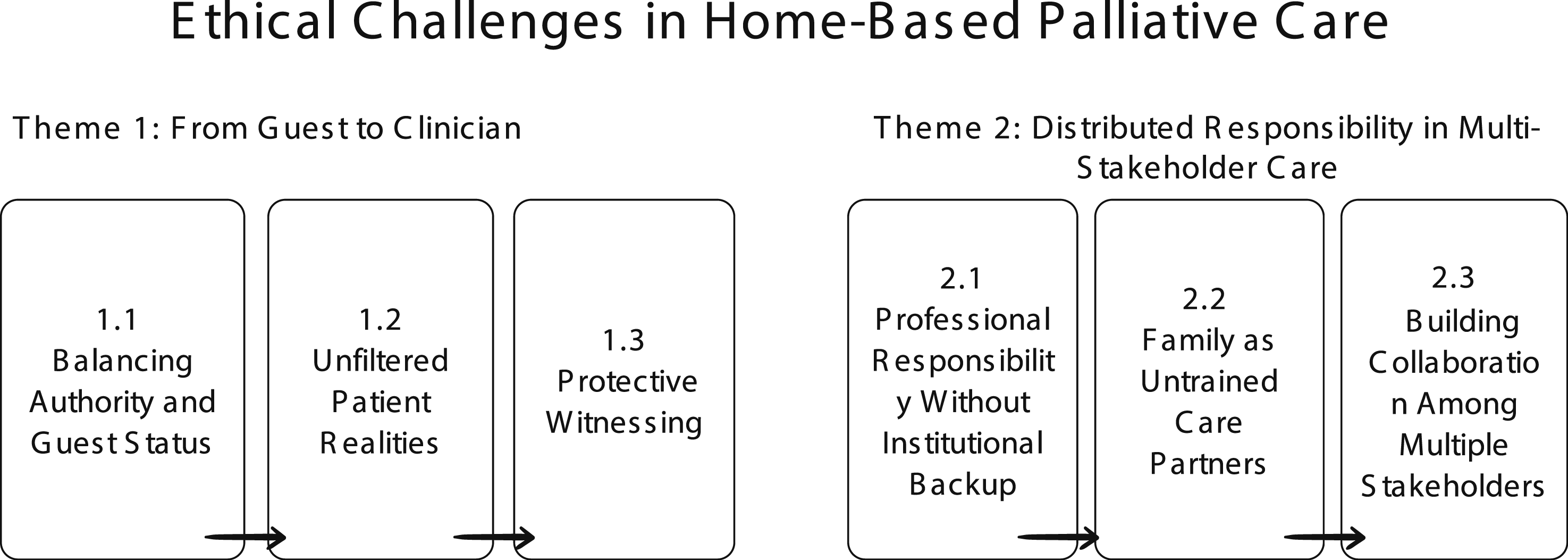
Theme 1: From guest to clinician: Ethical tensions of professional authority in domestic spaces
The first theme, “From Guest to Clinician,” follows a progression from entry into domestic space, where professional authority must be continuously negotiated, through exposure to unfiltered patient realities, to the development of protective witnessing as a deliberate ethical strategy for maintaining patient dignity. Healthcare professionals consistently described operating as “professional guests” in spaces they do not control, creating ongoing ethical tensions about asserting clinical expertise while deferring to patient preferences. Three interconnected sub-themes reflect this unfolding ethical progression: from negotiating permission and presence in domestic spaces, through encountering unavoidable access to private patient information, to developing protective witnessing as a deliberate ethical strategy that maintains therapeutic effectiveness while protecting patient dignity.
Balancing authority and guest status
Participants described the ethical tension of maintaining clinical responsibility while operating as guests in spaces they do not control. One physician explained, “We are guests in this situation… we need to be very, very humble in this place.” This position requires ongoing negotiation between professional expertise and patient autonomy, raising tensions about when clinical authority should take precedence over patient preferences.
Unlike institutional settings, where professional presence is established through organizational structures, home-based care requires seeking permission explicitly at each encounter. A social worker noted, “It is not our space. This means we need to respect, first, the patient’s wish and ask whether he wants us to come, whether he wants us to enter the house.” Interviewees described this continuous consent process as creating distinct responsibilities regarding professional presence and intervention in private spaces.
Participants reported that behavioral practices help maintain awareness of guest status throughout therapeutic relationships. One nurse explained, “I am always a guest in someone’s home. Even if I have been treating them for one, two, or 3 months, I am a guest, not family. For example, I will knock on the door first. I will ask permission again where to sit.” These practices demonstrate that professional authority in home settings depends on ongoing patient consent rather than institutional mandate.
Exposure to unfiltered patient realities
Participants described acquiring “embodied knowledge” in home settings—information obtained through sensory and environmental cues that exceeds standard clinical boundaries, creating ethical tensions between therapeutic benefits and privacy concerns. One social worker explained: “I have much more information about the person when I come to their home, and they do not always want to show me that information… when we come to their home, we see everything.”
This unfiltered access was characterized as “entering the truth.” One nurse noted: “When they come to the hospital, they are dressed and even wear lipstick. However, at home, there is a smell of urine, unchanged diapers, messy hair, and tired eyes. I enter the truth.” Such access enables more accurate clinical assessment, yet creates ethical tensions about witnessing patients’ vulnerability that they might prefer to conceal.
Environmental observations also provide immediate clinical information about cognitive functioning and safety risks. A physician explained: “I see piles of newspapers, a mess. I will not leave written instructions because they will get lost. When everything is organized, I can leave the guidebooks. This lets me personalize the plan.” Similarly, personal items facilitate relationship-building unavailable in institutional settings. One nurse stated, “I enter the house and see a first-place trophy in a bowling competition; I see a picture on the wall with the patient’s family name, and immediately I can create closeness and trust. This is not possible in the hospital. Only at home.”
Complex home environments require continuous professional adjustment. One social worker described: “Pit bulls without muzzles; parrots; seven people in a room and a half apartment all running around… a one-room apartment where I had to talk with the patient outside on chairs in the rain.” A nurse added, “I arrived with a plan, but there is reality, and that requires me to move. You cannot come rigid.”
Protective witnessing through selective attention
Participants described developing “protective witnessing”—a deliberate ethical practice of selective attention that manages exposure to patients’ unfiltered realities while maintaining dignity. One physician explained: “I see it, but I do not show that I see it. I show that I am with them, and these are two very different things.” This practice requires ongoing ethical judgment about what warrants professional attention and what should be respectfully overlooked.
Professional humility emerged as central to this practice. One social worker noted: “The issue of absolute knowledge humility is very strong with me. I come not knowing… I come understanding, I come knowing, but I do not come knowing about that specific Levy or Cohen family.” This humility reflects recognition that clinical expertise does not encompass each patient’s unique circumstances, life history, and domestic context.
Selective attention - choosing what to address and what to respectfully ignore, represents a core ethical skill in home-based care. One nurse stated: “What I choose to address in the home, what I choose to ignore in the home… that is also a choice… how I protect them there.” These decisions create ethical tensions between the need for thorough clinical assessment and respect for aspects of patients’ lives they may wish to keep private, while maintaining patient dignity amid the unavoidable exposure characteristic of domestic care.
Theme 2: Distributed responsibility in multi-stakeholder care: Family-focused ethical tensions
Home-based palliative care introduces a critical additional dimension beyond the professional-patient relationship: the active involvement of family members in care delivery and decision-making. Participants consistently described how this creates “distributed responsibility”—clinical accountability shared among professionals, patients, and family caregivers, each holding different types of authority without institutional structures to coordinate them. Three interconnected patterns were identified, reflecting an unfolding ethical process: the absence of institutional backup first exposes professionals to moral uncertainty without collegial support; this vacuum draws family members into active roles they are unprepared for; and professionals must consequently engage in continuous negotiation among multiple stakeholders with competing priorities.
Professional responsibility without institutional backup
Participants experienced ethical tensions when bearing clinical responsibility without the institutional support structures available in hospital-based care. One physician explained: “What is unique about the home is that you do not have the team around you, the equipment, you enter the patient’s home.” Interviewees described this not as a logistical challenge but as a source of moral uncertainty, when clinical responsibility persists but collaborative consultation and resource access are unavailable.
Medication management emerged as a key context for this tension. A physician noted: “The issue of medications is very problematic. They do whatever they want with the medications… We cannot control this.” The ethical tension arose not from inability to control patient behavior, which participants recognized as appropriate patient autonomy, but from a sense of moral unease: feeling answerable for patient safety while lacking the environmental oversight that hospital settings provide to identify and respond to risks.
Participants reported that this responsibility requires sustained emotional vigilance beyond clinical assessment. One nurse stated: “It requires much more effort from the doctor, emotional effort mainly… to check whether the patient is doing the treatment.” A physician described a further tension: “A patient receiving sedative treatment is asked not to drive… Then what happens when we leave the house, and he takes the keys?”
One nurse articulated the fundamental tension: “In the home, my responsibility continues, but my authority ends when I walk out the door. I can recommend, document, and explain the risks, but I cannot ensure they follow through. That’s just how it is in home care.” This recognition, that professional accountability persists despite limited ability to ensure implementation, creates ongoing moral deliberation about the scope and limits of responsibility when care delivery depends on patient and family actions beyond professional oversight.
Family members as untrained care partners
Home-based care significantly expands family members’ roles in implementing clinical decisions without professional training. Family caregivers’ continuous presence and responsibility for daily care tasks create ethical tensions distinct from institutional settings. One nurse explained: “The patient does not want to eat or drink. His wife offers him water, ‘No’. ‘Okay, then do not drink’. That is where the intervention ends. Then blood pressure drops.” Home settings position family members as primary care implementers whose moment-to-moment decisions significantly affect outcomes when professional oversight is intermittent.
Communication patterns within families emerged as a further source of ethical tension, intensified by the privacy of home settings. Participants described experiencing profound professional discomfort when family members prevented honest conversations about prognosis and treatment realities. A physician noted: “The family refused to talk about the end of life… always saying no, no, everything will be fine… but we know she will not recover.” Unlike hospital settings, the home environment grants families territorial control, enabling them to decline visits or terminate conversations, making professional intervention more complex.
Cultural variations in family communication norms create additional ethical tensions regarding the disclosure of illness. One social worker stated: “Family systems are so different from house to house… sometimes families at home do not warn us, for example, do not tell them about the illness.” When such tensions escalate to threaten patient welfare, professionals must assert clinical authority despite their guest status. A physician explained: “I went according to your wishes, but here I am entering your home as a doctor who says, enough, stop… we need a proper conversation.”
Building collaboration among multiple stakeholders
Participants identified ethical tensions between duties to individual patients and obligations to family-centered decision-making. Unlike institutional settings where professional authority operates through established hierarchies, domestic environments require collaborative decision-making among family members, patients, and healthcare providers.
Maintaining patient-centered care requires active professional effort when family dynamics threaten individual autonomy. One nurse stated, “I insist that as long as there is a cognitively intact patient, he be part of the conversation. I do not conduct conversations behind his back.” A physician described, “Sometimes you see the dominant family member who manages all the conversation… and you see the patient himself kind of shrinking.”
Patient and family resistance frequently arises as a natural response to changing care circumstances. One social worker explained: “One prominent characteristic in home relationships is resistance. ‘I did not want to be at home, I wanted rehabilitation’, ‘I do not understand what you offer’. Anger.” Participants described how resistance can transform into collaboration when professionals set clear boundaries and persistently advocate for patients’ needs. One nurse explained: “When I entered the home, a big man screamed at me terribly… he was taking out his frustration because they promised a doctor, not a nurse. I told him I was a nurse, but I would not leave until his wife received an answer. We became best friends afterward.”
Professional humility emerged as essential for gaining family acceptance of clinical recommendations. One nurse stated, “For them to accept my recommendations, I need much patience… to listen, to ask, with humility, with gentleness, to gain trust.” Transparency also emerged as crucial for maintaining professional integrity while balancing competing demands. One social worker explained: “My role is to honestly put all information on the table, with transparency and fairness, and let them choose what is right for them.”
These findings reveal two mutually reinforcing ethical dimensions: the guest status and limited institutional footing described in Theme 1 amplify the ethical weight of distributed responsibility described in Theme 2. Together, these dimensions place professionals in a state of ethical liminality, operating at the boundary between clinical responsibility and intimate relational contexts, a condition examined further in the Discussion.
Discussion
Home-based palliative care has been consistently identified as an ethically demanding practice environment, shaped by the intersection of professional responsibility, patient autonomy, and intimate domestic contexts.3,20 Yet existing literature has largely documented the challenges professionals face without adequately examining the adaptive ethical strategies they develop in response. This study addressed that gap by exploring how healthcare professionals balance and negotiate competing ethical values in patient-family relationships within home-based end-of-life care, revealing two interrelated dimensions: ethical tensions within the professional-patient relationship (Theme 1) and the complexities of distributed responsibility among multiple stakeholders (Theme 2). Together, these dimensions illuminate what we characterize as ethical liminality, a state in which professionals operate at the boundary between clinical responsibility and intimate relational contexts that institutional frameworks inadequately address. We use the term “ethical tensions” rather than “ethical dilemmas” deliberately: not all challenges described constitute dilemmas in the strict sense of two irresolvable moral imperatives in conflict. Rather, they reflect tensions arising from structural conditions of domestic care that resist resolution through protocol or clinical skills alone.
Participants consistently described their position as both insider and outsider, welcomed into the private space of families yet acutely aware of their status as guests. Prior research has underscored how professional authority can be diminished in home settings.16,25 Our findings extend this by demonstrating how guest status functions as an active ethical condition: professionals must seek permission not only for treatment decisions but for physical presence itself, knocking despite months of familiarity, asking where to sit, and requesting re-entry at each visit. This extends Emanuel and Emanuel’s 26 models of the professional-patient relationship and aligns with relational autonomy frameworks, 27 suggesting that continuously requesting permission is itself constitutive of patient autonomy rather than a constraint upon it.
This guest positioning inevitably exposes professionals to involuntary information about patients’ lives that was not consciously disclosed. Participants described “entering the truth” by witnessing unchanged diapers, cognitive disorganization, and living conditions that patients can conceal in institutional settings. This aligns with documented privacy concerns in home care20,28 yet differs in an important respect: this exposure is not the violation of a boundary but its structural absence. Traditional informed consent frameworks, which assume patients control information disclosure, inadequately address the involuntary exposure inherent to domestic care environments.
In response, professionals develop “protective witnessing,” a purposeful, ethically guided practice of selective attention that emphasizes dignity-preserving responses over exhaustive clinical disclosure.29,30 Our findings specify how this operates through “seeing but not showing I see,” choosing what to address professionally versus what to respectfully overlook. This practice sits between care ethics, which advocates full presence to patient experience,18,19 and the thoroughness principle of clinical ethics, which treats comprehensive assessment as a virtue. 31 Protective witnessing represents neither a compromise nor a failure of either framework, but an adaptive ethical practice shaped by conditions unique to domestic care, where visibility is total, yet intervention must remain selective.
The Israeli context illuminates why such strategies emerge informally rather than through institutional protocol. Despite palliative care training and multidisciplinary support, 22 Israeli home care services operate with limited structured protocols for end-of-life discussions and lack systematic documentation of patient preferences 5. In the absence of formal guidelines, professionals develop informal practices that bridge clinical responsibility and relational sensitivity, making the ethical exercise of selective attention not merely preferable but necessary.
The professional guest role complicates the balance between respecting autonomy and ensuring safety. Participants frequently recounted situations in which patients’ or family decisions appeared to compromise well-being, particularly regarding medication management and adherence to clinical recommendations. Such tensions are well-documented in the home-based care literature.3,28,32 Notably, while Heggestad et al. 3 emphasize patients’ right to autonomy as a central value, our participants experienced autonomy as a source of tension when it constrained their ability to ensure safe care delivery. This divergence may reflect cultural differences in the Israeli context, where family-centered decision-making and collective orientations toward illness can complicate individualistic autonomy frameworks.5,15
However, our findings emphasize the intensity of moral distress that arises when clinicians bear responsibility without having the means to control the environment. We characterize this as the paradox of “accountability without control”: professionals remain ethically accountable for outcomes, yet depend on families’ willingness, capacity, and domestic constraints to implement care plans. Brazil et al. 33 identified moral distress among home-based palliative care providers as arising precisely from this gap between responsibility and control. Our findings extend this by demonstrating how the gap is structural rather than incidental, embedded in the domestic setting itself. This structural dependence is further supported by Sabar et al., 16 who found that home-hospice professionals relied on family caregivers as a defining feature of the care context. As Nissanholtz-Gannot et al. 5 demonstrated in the Israeli context, gaps between professional accountability and practical control are compounded by systemic factors, including inconsistent palliative care training, unclear division of responsibilities among care providers, and the absence of standardized protocols for home-based end-of-life care. In response to this structural gap, evidence-based support mechanisms such as ethics reflection groups 34 and home-based advance care planning 35 have shown promise in helping professionals manage moral uncertainty in community care settings.
Family involvement emerged as a central and ambivalent force in end-of-life home palliative care. Families often function as indispensable partners providing continuity, cultural stability, and everyday care, yet can also be sources of conflict when emotional decision-making or protective instincts clash with professional assessments.36–38 Participants described managing authority with family members who asserted their own preferences or who were internally divided, leaving clinicians to mediate conflicting priorities without clear institutional backing.33,39 These dynamics position professionals not merely as intermediaries but as ethical mediators who must simultaneously advocate for patient autonomy and respect for family sovereignty, often in direct tension with one another. In home settings, families exercise a degree of control over the care environment that differs fundamentally from that in institutional settings, 3 thereby intensifying the moral weight of this mediating role. 16
Communication patterns within families further complicated clinical decision-making, as families often adopt protective strategies, softening or withholding prognostic information to shield loved ones from distress. While these practices can foster cohesion, they hinder transparent shared decision-making and place clinicians in the position of balancing disclosure with family loyalty.36,37 Importantly, such communication strategies are not merely emotional responses but may reflect deep cultural values: in collectivist family structures, withholding prognostic information is often understood as an act of protection and care rather than deception. 15 In the Israeli context, where diverse cultural and religious communities hold varying orientations toward death, disclosure, and family authority, this dynamic is particularly pronounced. 5 What participants described is not a structural loss of authority but a perceived expansion of moral obligation: professionals understood themselves as ethically responsible not only for clinical decisions but for the relational dynamics among all parties. The outcome is an ongoing negotiation of authority that contrasts with institutional hierarchies: in domestic settings, ethical decision-making should be collaborative, context-sensitive, and relational rather than principle-based.40,41
The two themes identified in this study are not parallel or independent. They are mutually constitutive. Theme 1 reveals how the domestic setting reconfigures professional identity and authority: professionals enter patients’ homes as invited experts yet also as guests, involuntarily exposed to private realities and required to exercise deliberate, selective attention in their ethical responses. Theme 2 builds directly upon this: it is precisely because professionals lack institutional footing and environmental control that the distribution of responsibility across multiple parties, patients, families, and systems becomes ethically charged.
Notably, within each theme, the sub-themes reflect an unfolding ethical process rather than independent categories. In Theme 1, professionals move from managing entry into domestic space, through unavoidable exposure to unfiltered patient realities, toward the development of protective witnessing as an adaptive ethical strategy. In Theme 2, the absence of institutional control creates moral uncertainty, drawing family members into active care roles they are unprepared for and requiring professionals to engage in ongoing negotiations among multiple stakeholders with competing priorities. This processual structure suggests that ethical competence in home-based palliative care is not simply a matter of applying principles but of working through a dynamic sequence of challenges that unfold within each clinical encounter.
Together, these themes illuminate a dynamic ethical cycle: the domestic environment destabilizes professional authority, and this destabilization is compounded by the diffusion of responsibility across multiple stakeholders without adequate institutional scaffolding. This layered vulnerability, relational, structural, and ethical, is a distinctive feature of home-based palliative care that existing ethical frameworks have not adequately mapped.
Implications for practice and policy
The following implications are offered in relation to the specific organizational and cultural context studied and should be understood as context-sensitive propositions rather than generalizable prescriptions. These findings carry concrete implications for professional preparation and organizational support. Clinicians working in home-based palliative care would benefit from training that goes beyond clinical competency to include ethical decision-making in low-control environments, communication strategies for managing family authority, and awareness of how domestic spaces shape professional identity and judgment. Reflective supervision and peer consultation structures, adapted to the distributed nature of home care, could help professionals process the moral distress arising from accountability without institutional support. Evidence-based ethics support structures, including ethics reflection groups 34 and home-based advance care planning, 35 provide additional mechanisms to support professionals managing moral uncertainty in community care settings.
At the organizational level, the structural nature of these ethical challenges suggests that individual-level solutions are insufficient. Policies governing home-based palliative care should explicitly address the reallocation of responsibility that occurs when care moves into domestic settings, including clearer protocols for managing family disagreements, defining thresholds for professional intervention, and ensuring that professionals are not left to manage complex ethical terrain in isolation.
Future studies should examine how patients and families experience and construct ethical authority in home care contexts, to complement the professional perspective presented here.
Limitations
This study is subject to several limitations. The sample was drawn from a single home care organization in Israel, which may limit transferability to other healthcare systems or cultural contexts. Nevertheless, the structural features identified, the reconfiguration of professional authority in domestic spaces, the paradox of accountability without control, and the development of protective witnessing as an adaptive ethical strategy are likely to resonate beyond the Israeli context, as home-based palliative care systems worldwide share the fundamental challenge of delivering clinical care within patients’ sovereign domestic environments. As with all qualitative research, findings reflect participants’ interpretations and subjective experiences rather than objective outcomes.
The study captured only the perspectives of healthcare professionals; patient and family voices, including their own frustrations and experiences of the ethical tensions described, are absent, and their inclusion in future research would provide a more complete understanding of the distributed relational dynamics at play. Additionally, because past experiences were involved, some retrospective bias cannot be excluded. The use of Zoom for data collection, while enabling broad participant access, may have limited the depth of non-verbal communication characteristic of in-person focus groups; this is acknowledged as a limitation of the current study.
Transferability is further limited by the absence of systematic data on participants’ socioeconomic and cultural backgrounds. To strengthen trustworthiness, we followed Belotto’s 42 recommendations, maintaining transparent coding procedures, interrater reliability checks, and member checking with participants; nonetheless, the interpretive nature of thematic analysis may have introduced variability in coding and categorization. Finally, all focus groups were conducted within separate professional groups; a mixed-profession design could offer additional interprofessional perspectives and should be considered in future research.
Conclusions
Home-based palliative care places healthcare professionals at the intersection of clinical responsibility and domestic sovereignty, an intersection where existing ethical frameworks offer insufficient guidance. This study demonstrates that the ethical challenges of this setting are structural and relational rather than incidental: the professional guest dynamic and the paradox of accountability without control are features of a system that has expanded into domestic spaces without adequately reconceptualizing the support required.
Competence in this context extends beyond clinical skill to encompass relational sensitivity, cultural awareness, and the capacity to navigate moral uncertainty. Addressing these challenges will require both individual-level preparation and systemic policy reform to ensure that dignity, autonomy, and safety can be sustained in the intimate space of the home. Although rooted in the Israeli context, the structural challenges identified in this study are relevant to nurses working in home-based palliative care across diverse cultural settings, particularly where such care is expanding and formal ethical guidance remains limited. Further research incorporating patient and family perspectives would deepen understanding of the distributed ethical dynamics identified here.
Footnotes
Acknowledgments
The authors thank the healthcare professionals who generously participated in this study and shared their experiences. We acknowledge the Sabar Health Hospital at Home organization that facilitated access to participants while maintaining confidentiality. Portions of this manuscript were supported by language and style assistance using artificial intelligence tools (e.g., ChatGPT, OpenAI). All AI-generated content was reviewed and edited by the authors to ensure accuracy and integrity. The authors take full responsibility for the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request. Data cannot be shared publicly due to ethical restrictions and privacy concerns arising from the sensitive nature of healthcare professional interviews.