
Abstract
Background
Psychiatric inpatients in China may experience threats to dignity and self-expression within ward environments shaped by stigma, safety concerns, and institutional routines. However, how they navigate these challenges and restore dignity through everyday interactions during hospitalization remains underexplored in psychiatric nursing.
Aim
To develop a substantive theoretical framework explaining how Chinese psychiatric inpatients experience dignity challenges and navigate pathways toward dignity empowerment and restoration during hospitalization, and what role therapeutic relationships with mental health nurses play in facilitating this process.
Research design
Constructivist grounded theory following the Charmaz tradition, informed by relational autonomy theory.
Participants and research context
11 psychiatric inpatients were recruited from the psychiatric ward of a tertiary general hospital in China between March and June 2025, using maximum variation purposive sampling to ensure demographic diversity.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine (Reference 2025-2245-01).
Findings
The theoretical model “Finding Voice in Vulnerability” suggests that psychiatric inpatients may navigate dignity challenges through four interconnected relational processes: Cognitive Liberation and Conceptual Reconstruction, Relational Dignity Empowerment, Relational Reconstruction of Valued Identity, and Participatory Treatment Negotiation. The model further suggests that vulnerability may become a relational resource through dignity-affirming interactions that support autonomy and participation in treatment decisions.
Conclusions
Dignity empowerment may emerge through relational recognition rather than individual autonomy, suggesting a potential reorientation toward relationally informed psychiatric care. The findings suggest that everyday nursing interactions may be important contexts for empowerment, with implications for relational competency training and future longitudinal research across diverse psychiatric settings.
Introduction
Mental illness encompasses a broad spectrum of conditions that substantially impair cognitive, emotional, and behavioral functioning, 1 profoundly disrupting social identity and exposing patients to stigmatization, discrimination, and social exclusion that progressively erode self-worth, dignity, and agentic capacity. 2 In Chinese psychiatric contexts specifically, these dignity challenges are distinctively configured by mianzi (face) culture, Confucian filial piety obligations, and family-centered care models, factors that collectively generate a particularly severe form of dignity vulnerability systematically constraining patients’ capacity for autonomous participation. Mental health nurses are uniquely positioned to address these challenges through therapeutic relationships that foster dignity empowerment, 3 yet the relational and institutional mechanisms enabling this process within culturally specific contexts remain insufficiently theorized.
To address these theoretical and empirical gaps, this study employed constructivist grounded theory methodology4,5 informed by relational autonomy theory6,7 to develop a substantive theoretical framework explaining how Chinese psychiatric inpatients experience dignity challenges and navigate pathways toward dignity empowerment and restoration during hospitalization. The resulting theoretical model elucidates the dynamic relational processes through which patients reconstruct dignity within institutional care, thereby informing more humanistic, culturally responsive, and empowerment-oriented psychiatric nursing practice. This study sought to address the question of how Chinese psychiatric inpatients experience dignity challenges and navigate pathways toward dignity empowerment and restoration during hospitalization, and what role therapeutic relationships with mental health nurses play in facilitating this process; this paper accordingly presents the study’s theoretical and methodological foundations, reports the conceptual model of dignity empowerment developed from participants’ lived experiences, and discusses implications for person-centered psychiatric nursing practice in Chinese institutional contexts.
Background
Mental illness profoundly disrupts social identity, exposing patients to misconceptions that construct them as “abnormal” or “dangerous” and thereby precipitate stigmatization, discrimination, and social exclusion. 2 These socially produced devaluations progressively deprive patients of meaningful social roles and opportunities for active, autonomous participation, fundamentally eroding self-worth and dignity. When institutional practices and cultural frameworks fail to recognize patients’ humanity and personhood, dignity, understood as a multifaceted construct encompassing both inherent value and relational dimensions, becomes compromised. 8 The progressive erosion of self-worth, social belonging, and agentic capacity that follows constitutes a dignity crisis that mental health nurses are uniquely positioned to address through therapeutic relationships that foster dignity empowerment. 3 Yet this endeavor is itself ethically demanding, as nurses must balance genuine ethical conviction for patient well-being against the procedural moral obligations imposed by medical institutional frameworks, 9 while recognizing patients not merely through a biomedical lens but as relationally constituted persons whose humanity is inherently open, incomplete, and agentive. 10 In psychiatric contexts, where naturalist reduction of patients to diagnostic categories routinely eclipses recognition of their personhood, these tensions are particularly acute. Understanding how nurses facilitate dignity empowerment within institutional and cultural constraints has therefore become a critical priority for advancing person-centered psychiatric care.
Within the Chinese context, these dignity challenges present a configuration markedly distinct from those documented in other cultural settings. Although collectivist values broadly characterize East Asian societies, comparative studies on mental health stigma across countries indicate that the mechanisms driving stigma in China are particularly severe in scope and distinct in form. 11 The Chinese configuration is specifically shaped by the pervasive mianzi (face) culture, Confucian filial piety obligations, and folk attributions of mental illness to moral failings or supernatural causes—factors that, in combination, generate a particularly family-mediated form of stigma implicating entire kinship networks. 12 These culturally specific meanings foster relational marginalization, as patients become peripheral within family hierarchies, healthcare encounters, and wider social networks. 13 The culturally valued family-centered decision-making model frequently supplants individual patient voices with collective determinations by relatives and professionals, effectively silencing patients’ authentic needs and relegating them to passive recipients of care. 14 Patients’ capacity to assert agency and maintain dignity becomes constrained not merely by individual limitations but through the complex interplay of hierarchical family structures, cultural norms prioritizing collective face-saving over individual expression, and institutional practices reflecting these collectivist orientations. 15 In this context, dignity and agency emerge not as individual attributes requiring protection, but as relational capacities continuously shaped by family dynamics, cultural expectations, and healthcare environments. Mental health nurses must therefore navigate tensions between these collectivist cultural norms and commitments to foster patient dignity and active, autonomous participation in care.
Contemporary psychiatric nursing practice operates within health systems that privilege clinical efficiency, risk management, and symptom control over dignity-centered, relationally oriented care, positioning patients as objects of intervention rather than as subjects with legitimate voices in decision-making. 16 Standardized protocols and resource pressures further compromise patient dignity and participatory autonomy. 17 Existing scholarship has advanced understanding by documenting structural barriers to patient participation across diverse healthcare systems 18 and identifying communication approaches that enhance engagement 19 ; however, prevailing conceptualizations predominantly treat dignity as a static, individually held attribute to be protected through systemic reforms (e.g., perceived rights violations, satisfaction with care environments, and adherence to institutional standards) rather than as a dynamic, relationally constructed outcome of therapeutic interactions, 20 thereby obscuring the transformative potential of everyday nursing encounters. Limited attention has been directed toward how patients actively negotiate institutional and cultural constraints to maintain dignity, how therapeutic encounters shape patients’ evolving capacity for agency, or what relational mechanisms enable transitions from passive recipients to active, autonomous participants. This gap is particularly pronounced in Chinese psychiatric contexts, where collectivist values and family-centered care models create unique challenges for fostering individual patient empowerment. 15
Relational autonomy theory6,7 addresses these limitations by conceptualizing autonomy as fundamentally relational, emerging from and shaped by social relationships, cultural contexts, and institutional structures—enabling examination of how patients’ capacity for autonomous participation develops through interactions with nurses within culturally specific contexts. Constructivist grounded theory methodology4,5 provides a complementary analytical approach, enabling inductive generation of substantive theory directly from participants’ lived experiences while prioritizing patient voices and examining social processes as they naturally unfold. Together, these frameworks direct analytical attention to the dynamic interplay of individual actions, therapeutic relationships, cultural norms, and institutional structures through which dignity and agency are relationally constituted, providing the theoretical and methodological foundation for the present investigation.
Methodology
Aim
This study aimed to develop a substantive theory through constructivist grounded theory methodology (Charmaz tradition) to investigate how Chinese psychiatric inpatients experience dignity challenges and navigate pathways toward dignity empowerment and restoration during hospitalization, and what role therapeutic relationships with mental health nurses play in facilitating this process.
Study design
This study employed constructivist grounded theory methodology following the Charmaz tradition.4,5 Constructivist grounded theory was selected for its inductive approach enabling theoretical insight generation directly from empirical data and its focus on understanding social processes through participants’ meanings and perspectives.4,5 The theoretical analysis was informed by Mackenzie’s relational autonomy theory, 6 which reconceptualizes autonomy as emergent through social relationships rather than isolated individual capacity.
The research design implemented concurrent data collection and analysis following constant comparative method and theoretical sampling principles. The study maintained researcher reflexivity throughout the analytical process, acknowledging the co-construction of knowledge between researchers and participants while allowing concepts to emerge from the data.4,5 Eleven participants completed three-stage interviews without attrition.
Sample and setting
This investigation was conducted in the psychiatric ward of a tertiary general hospital in China between March and June 2025, a care model of growing prevalence in urban China wherein psychiatric units are embedded within broader general medical systems. These wards constitute an institutionalized care environment operating under the concurrent governance structures of psychiatric care and broader hospital administration. 21 Participants were recruited using initial maximum variation purposive sampling to ensure demographic diversity across gender, age, education, diagnosis, illness duration, and ward type.
Inclusion criteria encompassed (1) psychiatric diagnoses meeting ICD-11 22 or DSM-5 23 criteria; (2) ages 18–65 years 24 ; (3) educational attainment ≥6 years; (4) clear consciousness and adequate communication abilities; (5) voluntary participation with signed informed consent. Drawing on the constructivist grounded theory premise that participants embedded within a shared institutional context possess experiential access to its operative social processes,4,5 the sampling strategy prioritized functional eligibility and demographic variation as the primary bases for selection, without pre-identification of participants on the basis of specific experiential categories. Exclusion criteria included (1) acute episodes with absent insight or expression capabilities 23 ; (2) hospitalization <5 days; (3) vulnerable populations beyond psychiatric patients/minors. Theoretical sampling guided subsequent recruitment after initial analysis identified conceptual gaps.4,5
Data collection
Data collection employed three-stage semi-structured interviews with iteratively refined interview guides based on emerging theoretical requirements (Supplement File 1). Each successive stage was designed to deepen participant engagement and generate progressively richer data for grounded theory construction.4,5 The initial stage explored hospitalization experiences. Analysis revealed theoretical gaps in cognitive transformation processes, prompting the second stage to incorporate targeted exploration of dependency redefinition and dignity preservation strategies. The third stage addressed remaining gaps around relational identity reconstruction and participatory treatment engagement.
Prior to data collection, all researchers and participants were unacquainted. Stage one interviews (average 25 min) established baseline understanding, stage two (average 45 min) targeted cognitive liberation processes, and stage three (average 55 min) focused on relational identity reconstruction. All interviews occurred in private ward locations with participant consent for audio recording. At each interview session, participants were reminded that involvement was voluntary, that withdrawal at any point would not affect their care, and that any question causing discomfort could be declined or deferred, thereby reducing participant burden within the inherently asymmetric researcher-patient relationship; the potential inconvenience of three-stage participation was weighed against the anticipated benefit of advancing understanding of inpatient psychosocial experiences, and no adverse events were reported. Verbatim transcription was completed within 24 h by professional transcriptionists trained in qualitative data management. Interview transcripts were returned to participants within 1 week alongside preliminary analytical interpretations, and participants were invited to verify, clarify, or expand upon both their accounts and the researcher’s interpretive summaries to ensure accurate representation of their experiences. All 11 participants confirmed the accuracy of their transcripts and preliminary interpretations, with three participants providing clarifications that informed refinements to the emerging analytical categories.
Data analysis
Data analysis commenced immediately after completion of the first interview, following constructivist grounded theory’s concurrent data collection and analysis principle.4,5 NVivo 12.0 software facilitated systematic data management and coding while preserving theoretical sensitivity. 25 The iterative analytical process (Supplement File 2-Figure 1) progressed through initial coding, focused coding, and theoretical integration, with constant comparison and memo writing maintained throughout to ensure emergent categories remained grounded in participant narratives. When theoretical saturation was not yet achieved, the process returned to data supplementation through additional interview stages, ensuring iterative refinement of interview guides and continued conceptual development until all participant narratives demonstrated clear fit within Mackenzie’s relational autonomy framework.
During initial coding, line-by-line coding employed gerund-based labels to capture participants’ actions, strategies, and meaning-making processes as they navigated dignity challenges within institutional contexts. Mackenzie’s relational autonomy framework 6 provided a sensitizing lens directing analytic attention toward how dignity and agency emerge through relational networks, guiding examination of how patients experience dignity challenges and navigate pathways toward restoration within institutional care contexts, while maintaining reflexivity regarding how theoretical concepts shaped interpretation.4,5 Through focused coding, the most significant initial codes were synthesized into sub-categories representing thematic dimensions within each main category. An illustrative example demonstrating the progression from line-by-line codes through focused coding to main categories is provided in Supplement File 2-Table 1, which shows how seven gerund-based codes extracted from a participant’s narrative about vulnerability were consolidated into the sub-category “Transformation of Vulnerability into Strength” within the main category “Cognitive Liberation and Conceptual Reconstruction.” For the purposes of systematic constant comparison, participants were organized into demographic subgroups (defined by gender, age range, educational attainment, and ward placement) and into subclinical subgroups (defined by psychiatric diagnosis category and illness duration). Constant comparison was applied within transcripts, across interview stages for each participant, across these demographically and clinically constituted participant subgroups, and between emergent categories and the relational autonomy framework to identify both convergent patterns and dimensional variations across these clinically and sociodemographically distinct participant groups.
Theoretical saturation was systematically monitored across 33 interview transcripts (Supplement File 2-Table 2). Stage 1 interviews (n = 11) generated 127 substantive codes reflecting varied participant experiences across diagnoses, illness durations, and ward contexts, with analytical memos identifying conceptual gaps in cognitive transformation and relational dignity processes that necessitated interview guide refinement. Stage 2 interviews revealed conceptual consolidation as only eight new codes emerged as dimensional variations within existing sub-categories, though gaps in identity reconstruction mechanisms (e.g., how patients re-narrate self-worth through therapeutic relationships; how relational dynamics facilitate meaningful participation in treatment decisions) prompted further interview guide adjustments targeting these dimensions in Stage 3. Saturation was confirmed at Stage 3 when final interviews generated zero new codes and exclusively mapped to the four main categories, with analytical memos documenting that category properties sufficiently explained variations across all demographic and clinical subgroups.
Theoretical integration centered on “Relational Dignity Empowerment” (the core category), examining connections between four main categories: Cognitive Liberation and Conceptual Reconstruction, Relational Dignity Empowerment, Relational Reconstruction of Valued Identity, and Participatory Treatment Negotiation. Literature review was integrated iteratively throughout the analytical process to situate emerging findings within existing scholarship while maintaining sensitivity to participants’ perspectives.4,5
Analytical rigor was maintained through systematic memo-writing, weekly multidisciplinary team meetings, reflexive journaling, comprehensive audit trails, and member checking.
Ethical considerations
Ethical approval (Reference 2025-2245-01) was obtained from the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine. Information sheets and consent forms were provided to participants prior to participation. 26 Participant records were deidentified and stored securely.
Results
Participant characteristics
Participant demographic characteristics.
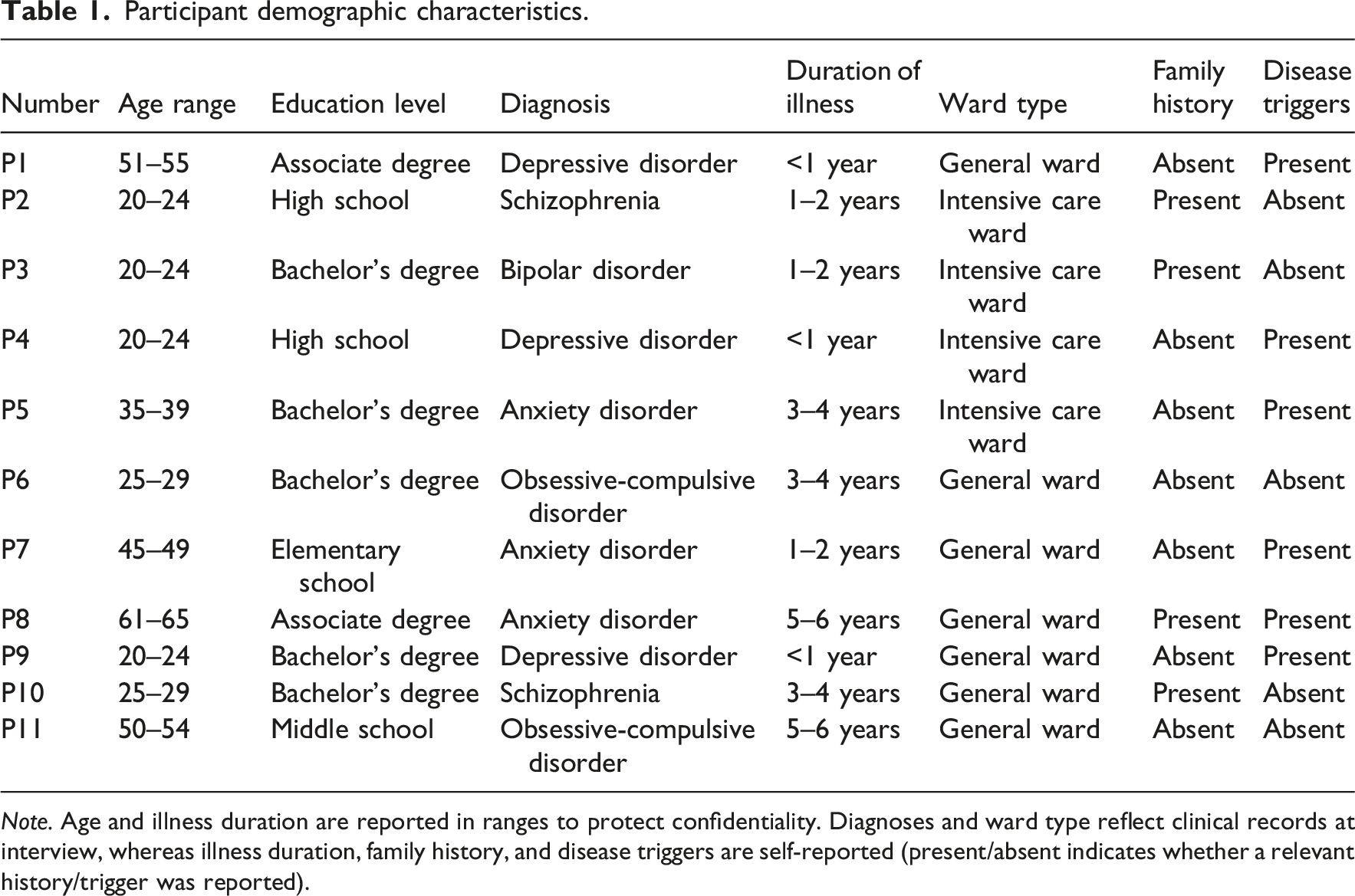
Note. Age and illness duration are reported in ranges to protect confidentiality. Diagnoses and ward type reflect clinical records at interview, whereas illness duration, family history, and disease triggers are self-reported (present/absent indicates whether a relevant history/trigger was reported).
Finding voice in vulnerability
The emergent theory “Finding Voice in Vulnerability” elucidates how psychiatric inpatients described experiencing dignity empowerment during hospitalization through relational interactions (Figure 1). This process comprises four interconnected main categories: Cognitive Liberation and Conceptual Reconstruction, Relational Dignity Empowerment, Relational Reconstruction of Valued Identity, and Participatory Treatment Negotiation. Finding voice in vulnerability.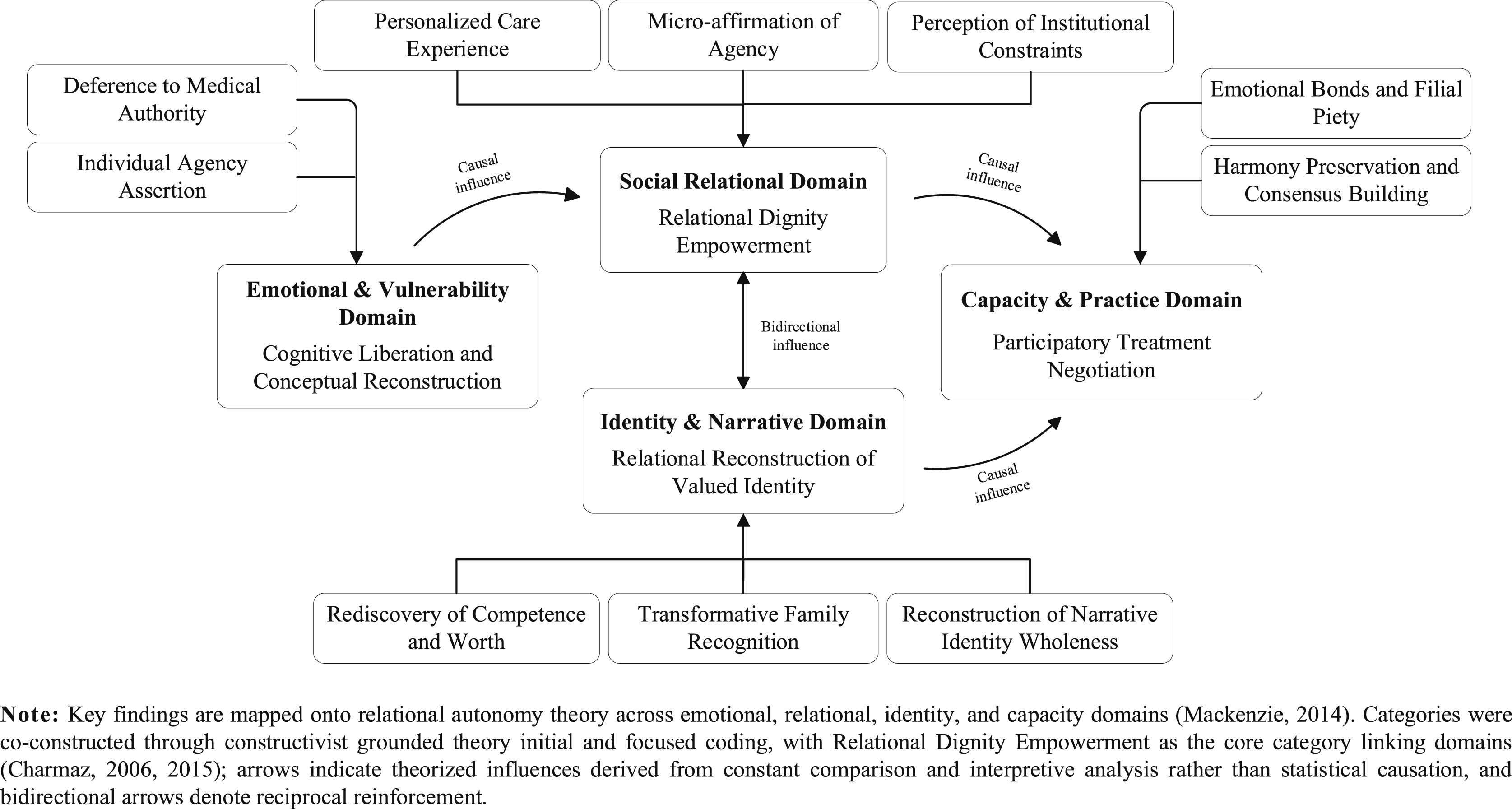
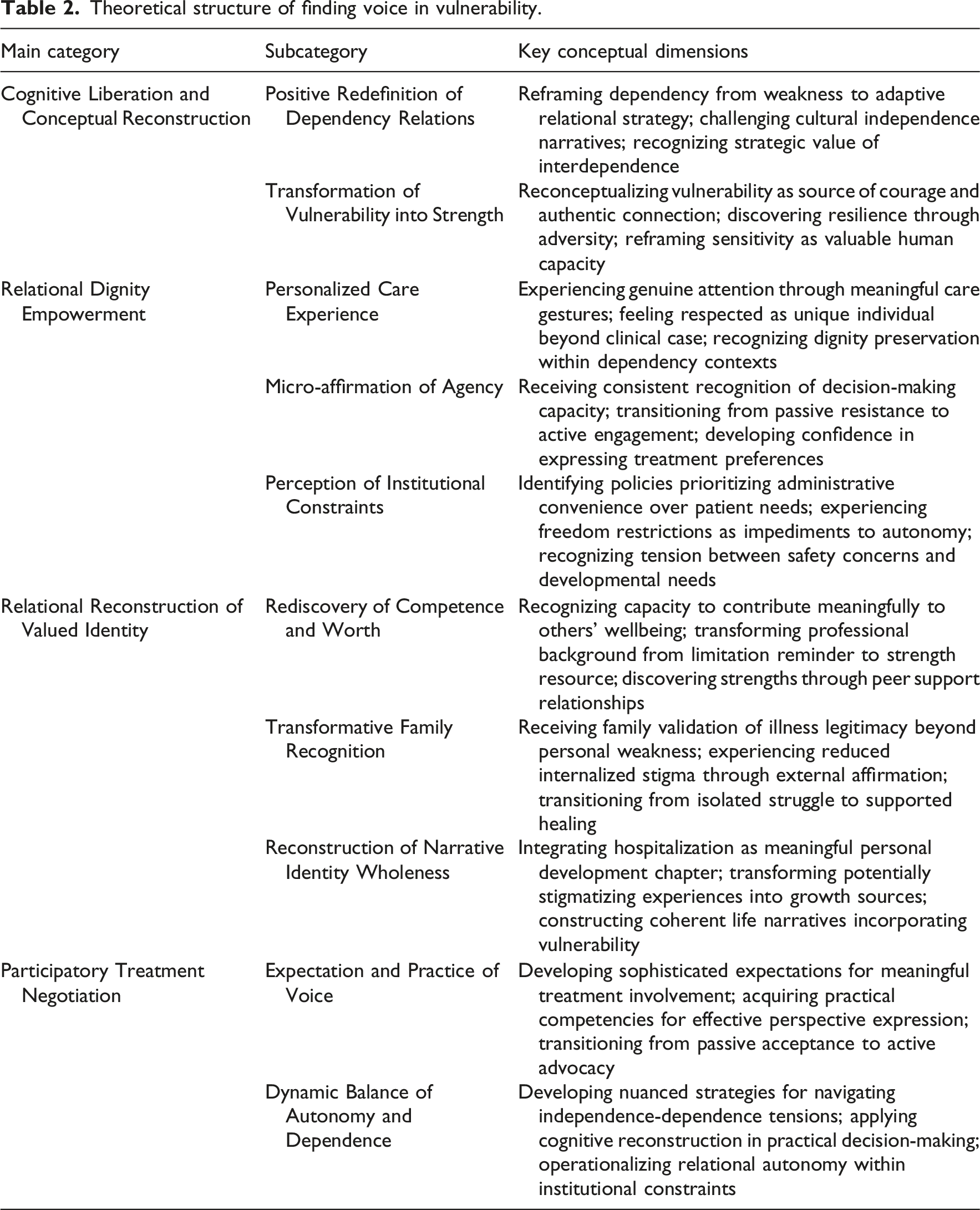
Theoretical structure of finding voice in vulnerability.
The relative salience of these processes varied across participant profiles. Participants with shorter illness durations and intensive care placements engaged more prominently with Cognitive Liberation and Conceptual Reconstruction, while those managing conditions for four or more years demonstrated more differentiated Participatory Treatment Negotiation strategies. Older participants with established family roles showed particularly active Transformative Family Recognition processes, with all four main categories identifiable across diagnostic groups, illness durations, and ward placements.
Relational Dignity Empowerment and Relational Reconstruction of Valued Identity appeared to function reciprocally: dignity-affirming relational encounters appeared to furnish the experiential foundation for identity reconstruction, while progressively restored self-worth appeared to enhance patients’ capacity to sustain such interactions. This dynamic was facilitated by consistent nursing recognition and parallel peer and family validation, and hindered by rigid ward routines, restricted autonomy, or impersonal clinical interactions disrupting relational continuity.
The sections that follow elaborate each main category through analysis and illustrative participant narratives demonstrating how these theoretical dimensions manifested in actual hospitalization experiences.
Cognitive liberation and conceptual reconstruction
This category represents the cognitive transformation participants described, through which they reframed understanding of dependency, vulnerability, and strength, enabling challenges to conventional independence paradigms.
Positive redefinition of dependency relations
Participants described fundamental cognitive shifts from viewing dependency as weakness to recognizing it as adaptive strategy through repeated positive support experiences. This reconceptualization challenged, in participants’ accounts, cultural narratives equating independence with self-sufficiency. One participant articulated this transformation: “I used to think [independence] meant not bothering others. Now, I believe true independence is being able to take good care of yourself while also being able to accept care from others” (P3). This account reflects a reported shift from binary conceptualizations toward relational models recognizing the strategic value of appropriate dependency.
Transformation of vulnerability into strength
Participants described reconceptualizing vulnerability from inherent weakness to source of courage and authentic connection through positive vulnerability expression experiences. This transformation was associated with participants’ recognition that acknowledging vulnerability required considerable courage and with their discovery of previously unrecognized strengths. As one participant reflected: “Vulnerability taught me to engage in deeper self-exploration. When I admitted my vulnerability, I began to face my inner world more honestly… I now see vulnerability as a necessary part of the path to growth. It makes us more authentic and gives us more depth” (P9). These reframing positions vulnerability as fundamental to authentic human connection rather than evidence of inadequacy in participants’ accounts.
Relational dignity empowerment
This category encompasses interpersonal mechanisms through which patients reported experiencing affirmation of inherent worth and agency within healthcare relationships, illustrating how dignity may emerge through relational recognition in daily interactions.
Personalized care experience
Personalized care experiences represent moments when healthcare providers demonstrated genuine attention to patients as unique individuals through small but meaningful gestures communicating respect and care. One participant described: “Once, my hands were shaking so much I couldn’t hold a cup of water steadily. A nurse saw this and didn’t just grab it from me. She first asked, ‘Would you like some help?’ and only helped after I agreed. This respect made me feel like my dignity was being protected” (P8). This illustrates how dignity preservation may occur through recognition of patient agency even within dependency contexts.
Micro-affirmation of agency
The term “micro” designates the granular, moment-level scale of discrete interactional events rather than their subjective significance 27 ; participants described such encounters as transformative precisely because small acts carried disproportionate meaning within institutional care settings. Micro-affirmations represent consistent recognition of patient capacity for decision-making within institutional constraints. One participant noted: “I am now more proactive in expressing my own views, unlike before when I was resistant. For example, regarding my treatment plan, I’ll ask why it’s arranged this way and what other options there are” (P5). This reported shift from passive resistance to active engagement illustrates how agency affirmation may transform treatment participation.
Perception of institutional constraints
This subcategory addresses hospital-level institutional constraints on patient agency and dignity, encompassing ward regulations, clinical protocols, and administrative practices. While participants also described structural pressures in familial and broader sociocultural domains, including stigmatizing conceptualizations of mental illness and cultural expectations of self-sufficiency, this subcategory focuses specifically on the institutional environment of inpatient care. Participants recognized that policies often prioritized administrative convenience over patient needs. One participant observed: “I think when the rules were made, they were probably thinking more about management convenience and safety, and not enough about the actual needs of us young people” (P2). These experiences suggest institutional dynamics that can either support or undermine relational autonomy development.
Relational reconstruction of valued identity
This category represents the process through which patients described rebuilding self-worth and capability through supportive relationships and recognition of continued value, encompassing restoration of positive self-regard and integration of hospital experiences into coherent life narratives.
Rediscovery of competence and worth
Through interactions with other patients and opportunities to provide support, participants described rediscovering capacity to contribute meaningfully to others’ wellbeing within the hospital environment. One participant reflected: “Sometimes I would use my professional knowledge to help others, which gave me a great sense of accomplishment” (P6). Professional backgrounds were described as becoming sources of strength rather than reminders of limitations.
Transformative family recognition
Family recognition of participants’ experiences as legitimate illness rather than personal weakness was reported as providing crucial external validation supporting participants’ reframing and reducing internalized stigma. One participant described this change: “My family is more patient with me now. They used to always say, ‘Just look on the bright side’, but now they know it’s an illness that needs treatment…These changes make me feel understood and have helped me rediscover my own worth. I don’t feel weak; I feel brave for facing my illness” (P10). Participants indicated that this validation facilitated integration of hospital experiences into positive self-narratives.
Reconstruction of narrative identity wholeness
Participants engaged in active reconstruction of biographical narratives to incorporate hospitalization experiences as meaningful personal development chapters rather than disruptions. One participant articulated: “...Compared to before, my story now includes more about courage and growth. I used to think I was very fragile, but now I know that being able to face difficulties is itself a form of courage” (P4). This narrative reconstruction illustrates participants’ reported transformation of potentially stigmatizing experiences into sources of personal growth.
Participatory treatment negotiation
This category represents the evolving process through which patients described transitioning from passive recipients to active treatment collaborators, encompassing development of expectations for meaningful involvement and acquisition of practical participation skills.
Expectation and practice of voice
Participants described developing sophisticated expectations for being heard alongside practical competencies for expressing perspectives effectively, representing a reported movement from passive acceptance to active advocacy. One participant stated: “I believe we should have more of a say throughout the entire treatment process because we are the subject of our own treatment, and our thoughts and feelings are very important” (P5). Professional participants particularly sought recognition of their expertise and capacity to contribute meaningfully to treatment planning.
Dynamic balance of autonomy and dependence
Participants described developing sophisticated strategies for navigating contradictory needs for independence and appropriate dependence, representing what they perceived as practical application of cognitive reconstruction regarding dependency relationships. Participants described their approaches: “I felt I needed to rely on medical professionals for medical matters and on family and friends for emotional support. But for personal hygiene, daily activities, and expressing my emotions, I hoped to handle them independently. I balanced these two needs by not being shy about asking for help when I needed it and not being dependent when I could be independent” (P3). This balance appeared to require nuanced assessment of when to seek support versus assert independence, reflecting complexity of operationalizing relational autonomy within institutional contexts.
Discussion
This study applies constructivist grounded theory methodology4,5 to explicate the dynamic process of Relational Dignity Empowerment among Chinese mental health inpatients, culminating in the theory “Finding Voice in Vulnerability.” The theory illuminates how patients, through relational interactions, may cognitively reframe the meaning of dependence and vulnerability, experience personalized care and affirmation of agency, and reconstruct competence and self-worth while increasingly seeking participation in treatment decisions. At a conceptual level, Relational Dignity Empowerment positions dignity as co-constructed through interpersonal recognition, rather than as an inherent characteristic that merely requires protection. This formulation operationalizes Mackenzie’s relational autonomy framework by demonstrating that autonomy in inpatient psychiatry is sustained by social relationships, institutional structures, and cultural contexts that can either enable or constrain self-determination.6,7 Accordingly, the process model challenges emphases on individual self-sufficiency 28 and reconceptualizes vulnerability and interdependence as potential sources of strength, diverging from therapeutic paradigms that prioritize individualized resilience building 29 while converging with Asian mental health nursing evidence emphasizing relational engagement, reciprocity, and family involvement in recovery. 30
While certain dominant empowerment frameworks have historically emphasized individual autonomy and self-assertion, emerging scholarship across diverse cultural contexts challenges this binary framing. Person-centered care literature, grounded in the Gothenburg model, reconceptualizes patients as partners with capacities rather than passive recipients, prioritizing the co-construction of health plans through sustained therapeutic partnerships. 31 A constructivist grounded theory study of community mental health recovery similarly found that building genuine therapeutic relationships with care providers, rather than fostering independence from them, was the central mechanism enabling participation and personal recovery, with participants describing such support as an “invisible hand” that empowered rather than constrained agency. 32 The present framework, emerging from a distinctly Chinese relational-Confucian context in which interdependence is understood as foundational to human existence and personal cultivation is achieved through meaningful relationships, thus converges with an increasingly relational turn within international person-centered care literature, rather than contrasting with frameworks that privilege individualistic self-sufficiency. By foregrounding the micro-interactional quality of everyday nursing encounters, the framework recasts therapeutic relationships as sites of dignity co-creation. 33
Cognitive Liberation and Conceptual Reconstruction clarify how empowerment may begin with interpretive change, as stigmatizing understandings of hospitalization give way to meanings that may position vulnerability as a legitimate site of therapeutic growth and authentic therapeutic engagement. Rather than casting dependency as an obstacle to autonomy, the category depicts an epistemic shift in which interdependence may be recognized as an adaptive way of sustaining agency within conditions of acute distress, thereby aligning with relational autonomy’s claim that self-determination is exercised through, not against, supportive relationships.6,7 Recognition practices within wards, including nonjudgmental responses to disclosure and moral reframing of help-seeking as responsibility, appear to supply the social conditions under which patients may reinterpret vulnerability as relational courage rather than personal failure, a pattern consistent with the constitutive role of recognition in autonomy development across diverse cultural contexts. 34 This reconstruction is particularly consequential in Chinese contexts where mental illness stigma is tightly interwoven with family honor and social reputation, intensifying shame narratives that can render admission a source of familial disgrace. 13 Within such cultural conditions, agency may be enacted through relational negotiation that preserves face while enabling selective openness in relationally safe contexts, an interactional strategy that connects emotional restraint norms with culturally situated pathways toward voice and therapeutic relationship. 35
The present data suggest that dignity may be experienced as an interpersonal achievement embedded in everyday care, a pattern that extends relational autonomy theory into observable nursing mechanisms. In this account, dignity appears to emerge through recognition conveyed in ordinary encounters, such as respectful address, attentive listening, and clear procedural explanations, which may soften hierarchical asymmetries without destabilizing culturally appropriate deference to professional authority. 33 Within this framework, each nursing interaction may be understood as what Holopainen et al. term a caring encounter, 36 characterized by mutuality between nurse and patient, the nurse’s authentic presence, and attunement to the patient’s subjective lifeworld beyond mere task completion. This distinction carries analytical significance: personalized care denotes the tailoring of interventions to individual needs, person-centeredness describes a broader philosophy of therapeutic partnership, and the caring encounter captures the micro-interactional quality of each discrete nursing interaction as the operative site of dignity co-construction, a conceptualization that resonates with Scandinavian nursing philosophy, suggesting that such micro-interactional quality may constitute a fundamental unit through which dignity is experienced across cultural contexts.
Personalized care may function as more than a courteous style because it may signal sustained acknowledgment of personhood and agency within contexts that otherwise risk reducing patients to clinical cases, a dynamic widely emphasized in person-centered nursing scholarship.20,37 At the same time, the category maintains analytic sensitivity to institutional constraints, since ward routines and risk-oriented rules can inadvertently communicate that administrative convenience outweighs patient needs, thereby narrowing the relational space in which voice can be safely expressed. Taken together, these tensions underscore that autonomy-supportive care in inpatient psychiatry requires institutional environments that permit recognition practices to be enacted consistently, rather than episodically, if dignity is to be reliably co-created.
Relational Reconstruction of Valued Identity suggests how self-worth may be rebuilt through mutual recognition and relational contribution, challenging accounts of identity that privilege solitary self-appraisal. 28 Within this trajectory, opportunities to support peers and be recognized as helpful may allow competence to be re-experienced as socially consequential, creating a bridge between suffering and a restored sense of value that is consonant with Japanese evidence on the recovery significance of interpersonal contribution, 38 suggesting that social recognition may constitute a culturally transcendent mechanism of competence restoration. Family recognition may constitute a parallel pathway of validation, particularly salient in settings where family interpretations can either intensify internalized stigma or legitimate illness as deserving of professional care, thereby reshaping moral narratives of weakness that are often attached to psychiatric diagnoses in China. 13 Confucian commitments to self-cultivation may further condition this reconstruction by providing culturally intelligible grammar for interpreting recovery as continuous improvement while resisting stigmatizing reductions of illness to character deficiency. As narrative coherence is gradually reestablished, hospitalization may be integrated as a meaningful chapter in a broader life story, allowing vulnerability to be held alongside competence rather than treated as a permanent identity rupture.
Participatory Treatment Negotiation suggests a progressive movement from passive compliance to collaborative engagement, in which expectations for involvement may develop alongside practical capacities for articulating preferences within hierarchical contexts. This account aligns with the procedural dimensions of relational autonomy, since participation is not a simple expression of rational capacity but a relational accomplishment supported by validation, invitation, and opportunities for meaningful contribution. 7 As patients develop confidence through earlier recognition experiences, participation in care planning may become more feasible, a pattern that converges with scoping review evidence and a Swedish community mental health study that engagement is enabled by both relational support and context-specific communication conditions.32,39 Within Chinese settings, voice may be expressed through indirect, face-saving communication and in consultation with family members, suggesting culturally adapted shared decision-making that preserves relational obligations while potentially advancing patient agency. 40 Consequently, empowerment may be better conceptualized as the capacity to negotiate contextually appropriate positions along a continuum of autonomy and reliance, rather than as a linear transition toward maximal independence, thereby reinforcing the proposition that dependence within therapeutic relationships can facilitate, rather than undermine, agential capacity. 41
Relevance for clinical practice
Dignity empowerment emerges fundamentally through relational nursing interactions wherein patients experience personalized care and recognition of worth. Nurses should establish structured routines dedicating uninterrupted time for meaningful conversations with each patient daily, maintaining eye contact and sitting at eye level during interactions. Documentation systems should capture personal details about patients’ lives, family contexts, and communication preferences to facilitate continuity across nursing shifts. Incorporating patients’ preferred forms of address and remembering family details demonstrates sustained attention to patients as unique persons. 20
Within such relational contexts, patients may cognitively reconstruct vulnerability as strength through validation from nurses and opportunities to exercise agency. Nurses should normalize help-seeking through explicit verbal affirmation, responding to patient requests with statements such as “Asking for help shows you understand what you need.” Modeling collaborative problem-solving by verbalizing consultations with colleagues demonstrates that professional competence encompasses recognition of limitations. 42 Ward activities should facilitate peer support interactions wherein patients both receive and provide assistance to fellow inpatients, enabling them to experience accumulated wisdom as sources of strength.
Facilitating these transformative processes requires communication competencies attuned to Chinese cultural contexts and hierarchical healthcare relationships. Training programs should incorporate role-playing exercises teaching nurses to balance professional authority with patient partnership, facilitate patient disclosure while protecting mianzi (face), involve families appropriately without marginalizing patient voices, and navigate guanxi (relationship network) dynamics while fostering collaborative decision-making. Core competencies include active listening, reflective responses validating patient emotions, open-ended questioning, and transparent explanation of treatment rationales.13,19
Beyond individual nursing competencies, environmental structures and family involvement patterns emerge as critical for supporting patient agency development. Ward modifications should include designated private spaces for nurse-patient conversations, patient input mechanisms for daily routine adjustments such as meal times and activity participation, and visual displays of individual patient preferences. Visiting hour flexibility should accommodate family involvement while maintaining patient-centered focus. Family involvement protocols must specify when families participate in care planning, with explicit guidelines ensuring family presence supports rather than overrides patient participation in treatment decisions.13,43
Limitations and prospects
This study acknowledges several important limitations. (1) Data collection was conducted within a single tertiary general hospital whose psychiatric unit, embedded within a general medical organizational structure, may not reflect the staffing arrangements, resource availability, or patient acuity profiles characteristic of specialized psychiatric hospitals, community mental health facilities, or lower-tier settings, thereby constraining the resonance and usefulness of the theoretical model when applied across these varied contexts. (2) The study design captured experiences during specific hospitalization periods, potentially missing temporal evolution of nursing-facilitated dignity empowerment and long-term sustainability beyond immediate inpatient contexts. (3) The sample (n = 11) was compositionally concentrated toward mood and anxiety spectrum diagnoses, younger age, and higher educational attainment, potentially shaping the analytical prominence of particular theoretical processes as situated constructions and constraining the resonance and usefulness of the emergent theoretical model, with the research team’s prior clinical familiarity with psychiatric nursing potentially introducing interpretive predispositions despite sustained reflexive engagement throughout the analytical process.
Future research should pursue several directions: (1) longitudinal designs tracking relational autonomy development from acute care through community reintegration to identify critical transition points; (2) multi-site replication across diverse psychiatric settings to establish the theory’s scope conditions and necessary contextual adaptations; (3) focused investigations within specific diagnostic subgroups to assess whether current categories adequately capture diagnosis-specific manifestations of relational dignity empowerment.
Conclusion
This grounded theory study generated the theoretical framework “Finding Voice in Vulnerability,” which proposes an explanatory account of how Chinese psychiatric inpatients may navigate dignity challenges through four interrelated relational processes: Cognitive Liberation and Conceptual Reconstruction, Relational Dignity Empowerment, Relational Reconstruction of Valued Identity, and Participatory Treatment Negotiation. The findings suggest that dignity and agency may emerge through interpersonal recognition within therapeutic relationships rather than through the protection of individual autonomy, a pattern that appears consistent with Chinese emphases on relational interdependence and with implications for independence-oriented psychiatric care models. The framework indicates that everyday nursing interactions may serve as meaningful empowerment mechanisms, suggesting that clinical practice, institutional environments, and nursing education could benefit from prioritizing recognition-based relational competencies, safeguarding patient voice within family involvement, and supporting culturally appropriate shared decision-making, while future research should examine dignity trajectories across care transitions, test transferability in multi-site studies, and develop systematic assessment measures across diverse psychiatric contexts.
Supplemental material
Supplemental Material - Finding voice: Grounded theory of dignity among psychiatric inpatients
Supplemental Material for Finding voice: Grounded theory of dignity among psychiatric inpatients by Kehua Yang, Wenyu Yue, Shuting Zhang, Qunyan Shen, Xinghui Lv, Zhongmei Yan, Lingling Cheng, Wei Chen, and Xiaoqin Ma in Nursing Ethics.
Supplemental material
Supplemental Material - Finding voice: Grounded theory of dignity among psychiatric inpatients
Supplemental Material for Finding voice: Grounded theory of dignity among psychiatric inpatients by Kehua Yang, Wenyu Yue, Shuting Zhang, Qunyan Shen, Xinghui Lv, Zhongmei Yan, Lingling Cheng, Wei Chen, and Xiaoqin Ma in Nursing Ethics.
Footnotes
Author contributions
Kehua Yang: Conceptualization, methodology, software, formal analysis, investigation, data curation, and writing—original draft; Wenyu Yue: Conceptualization, methodology, software, formal analysis, investigation, data curation, and writing—original draft; Shuting Zhang: Investigation and data curation; Qunyan Shen: Investigation and data curation; Xinghui Lv: Investigation and data curation; Zhongmei Yan: Investigation and data curation; Lingling Cheng: Investigation and data curation; Wei Chen: Supervision, project administration, and funding acquisition; Xiaoqin Ma: Supervision, project administration, and funding acquisition.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Zhejiang Provincial Medical and Health Science and Technology Project (Grant No.: 2025717397).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation. We confirm that the dataset used in this manuscript has not been used in any other papers (in progress, under review, or published). There is nothing to declare regarding data overlap.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.