
Abstract
In elder care, “safety” is frequently accorded overriding moral priority. As a result, restrictive measures introduced under the banner of risk prevention are readily treated as “reasonable protection,” while, under the guise of care, they can encroach on older persons’ freedom, privacy, and dignity. The expansion of digital care technologies reinforces logics of continuous monitoring and alerting, thereby intensifying this tension. Existing debates often remain confined to an “autonomy versus beneficence” framing or to compliance-oriented privacy governance, and thus struggle to specify clear boundary conditions. Grounded in care ethics and relational autonomy, this article conceptualizes such practices as “benevolent coercion” and develops a Relational Legitimacy Framework (RLF). The RLF treats restrictive measures as normative actions that carry a burden of justification and requires that they meet, simultaneously, risk-grounded necessity and proportionality; relationally defined, minimally intrusive alternatives; relational procedural legitimacy, including the identification of false consent and the possibility of withdrawal; and non-negotiable baseline protections for dignity and privacy. It further emphasizes time-limited reassessment and viable exit mechanisms. The Chinese context serves as a setting in which underlying mechanisms become especially visible, allowing assessment of the risk that key conditions may fail in practice. This article contributes a reusable normative braking system for safety-based justifications and offers a theoretical foundation and practical guidance for nurses and institutions to integrate restrictive measures into actionable ethical decision-making procedures and governance rules.
Keywords
Introduction
In contemporary elder care practice, “safety” is increasingly treated as a moral responsibility that is rarely questioned. Measures introduced to prevent falls, wandering, medication errors, or acute health incidents often, to varying degrees, restrict older adults’ mobility, privacy, and capacity for self-determination. The spread of digital care technologies, such as in-home cameras, GPS tracking, wearable and ambient sensors, passive remote monitoring, and platform-mediated management, further reinforces a care logic centered on continuous visibility and anticipatory intervention. As a result, restrictive practices can more readily shift from occasional responses to routine arrangements.1,2 The Chinese context offers an analytically revealing site for examining this problem. Within a structural configuration shaped by the intersection of family responsibility ethics and organized risk governance, “safety” is more likely to be granted moral priority. This, in turn, makes restrictive arrangements more readily taken as self-evidently justified and further narrows the space for contestation. 3
Although scholarship on elder care has expanded around autonomy, consent, privacy, and risk management, the normative standing of safety-oriented restrictions still lacks clear conceptual delineation and explicit boundary conditions. Two tendencies are especially common in existing discussions. The first reduces care dilemmas to a straightforward tension between autonomy and beneficence.4–6 The second approaches privacy and consent primarily as matters of compliance and disclosure, thereby tacitly assuming that the presence of risk permits safety to override other values.7–10 Such approaches can obscure central structural features of care settings, including who defines risk, whose anxieties are being managed, and how older adults’ preferences are reframed as “cooperation” under relational pressures and institutional accountability. Felber et al. observe that this zone of ambiguity is particularly pronounced in contexts of digital monitoring. Restrictions are often articulated through benevolent language of “for your own good,” appearing mild in form yet persisting over time, which makes them harder to recognize, challenge, and rectify. 11
Accordingly, this paper centers its analysis on the ethical legitimacy of benevolent coercion, namely, restrictive practices that are enacted, or gradually routinized, in the name of protection and care within caring relationships. The theoretical contribution of this paper is twofold. First, it explicitly conceptualizes such safety-oriented restrictions as normative actions that involve an initial infringement, thereby placing them under a stringent requirement of justification. Second, grounded in care ethics and relational autonomy, it proposes a Relational Legitimacy Framework for evaluating safety-oriented restrictive measures. Rather than treating “safety” as an automatically overriding good, the framework specifies a set of relational conditions under which restrictions may be considered acceptable. These conditions include risk-based necessity and proportionality, the prioritization of relationally less intrusive and adequate alternatives, relational procedural legitimacy and revocability, including the identification of apparent consent that is not genuinely voluntary, and a non-negotiable baseline for dignity and privacy. At the level of nursing practice, the paper aims to provide nurses and institutions with an operational ethical decision-making rationale. It seeks to shift restrictive measures from a default option to an exceptional practice that requires explicit justification, and to establish reviewable and revisable normative safeguards for safety governance.
Problem origin: From safety as a care goal to benevolent coercion
In elder care, “safety” is often more than a practical objective. It is frequently mobilized as a morally overriding justificatory discourse. Once an intervention is framed as “preventing harm” or “avoiding risk,” it tends to be accorded priority in normative reasoning, thereby displacing values such as autonomy, privacy, dignity, and choices about one’s way of life. 12 Crucially, risk is not a purely objective given. It is co-produced under specific institutional arrangements, affective pressures, and resource constraints. Prior studies show that in long-term care settings and nursing facilities, risk is repeatedly defined, amplified, and prioritized through organizational accountability and performance imperatives, heightened sensitivity to adverse events and legal liability, and the emotional and moral burdens borne by caregivers, including family members and professionals.13,14 At the same time, older adults’ designation as “high risk” is not attributable solely to age, physical decline, or cognitive change. It may also reflect upstream conditions, including inadequate income security, limited community support, uneven access to health and long-term care services, staffing shortages, and insufficient accessible environments.15,16 If risk governance focuses narrowly on controlling individual behavior and preventing immediate incidents, it can obscure these institutional sources of vulnerability. Problems that could be addressed through environmental modifications, resource support, or adjustments in care arrangements may instead be translated into restrictive interventions directed at older adults. Under such conditions, “safety” can readily shift from a value that requires balancing to a rationale presumed to require no further justification. Restrictive measures then acquire default legitimacy as matters of taken-for-granted necessity, while older adults’ objections are reinterpreted and labeled as “irrational,” “non-cooperative,” or “lacking risk awareness.” 17
Within this structural context, the present study focuses on benevolent coercion. Benevolent coercion does not denote overt oppression centered on violence or punishment. Rather, it refers to a family of practices that invoke protection and care as justificatory grounds within caring relationships and that, through restricting movement, narrowing the scope of choice, instituting default guardianship, applying moral persuasion, or routinizing institutional procedures, generate substantive curtailments of older adults’ freedom, privacy, and autonomy. 18 Its normative complexity lies in the fact that it is often accompanied by care-laden language and a moral self-understanding on the part of interveners. They may sincerely believe they are acting responsibly and providing care. Yet precisely because coercion is framed as care, it is more easily taken as self-evidently right and can quietly become routine within caring relationships marked by power asymmetries. 19 An opinion issued by the German Ethics Council on benevolent coercion underscores that coercion motivated by benevolence is not uncommon in professional care relationships. Any form of coercion, however, entails serious infringement of the care recipient’s core normative interests and personal freedoms and therefore must meet a more stringent burden of justification and standards of scrutiny. 20 In parallel, debates in nursing ethics on consentless care highlight that when caregivers substitute benevolent interpretations for the person’s consent and participation, coercion may occur in a mild yet persistent manner within a zone of ambiguity in everyday practice.21,22
Moreover, benevolent coercion is not merely an occasional individual choice. It reflects a practice logic that can be analyzed in terms of mechanisms. When “safety” is established as the primary moral objective, caregivers become more inclined to convert uncertainty into manageability, to translate preference differences into standardized arrangements, and to replace “allowing choice” with “deciding on behalf of the person.” This conversion can proceed through multiple pathways. It may appear as physical restrictions, such as limiting outdoor activities and tightening medication management and activity control. 23 It may also take the form of emotional and moral constraints, for example by invoking “making the family worry” or accusing the person of being “thoughtless” in order to exert pressure. 24 It can also be realized through institutional routines, such as standardized schedules and risk-oriented disciplinary practices, and, with the introduction of digital monitoring, become further embedded in the temporal and spatial organization of everyday life.25,26 The ethical risks at stake extend beyond abstract questions such as whether privacy is violated or autonomy is harmed. More fundamentally, such practices may produce an ongoing erosion of personhood and agency. Older adults may be placed in circumstances where they are made visible by default and continually assessed. Over time, they may learn to exchange compliance for relational equilibrium and access to care resources, thereby cultivating self-discipline and silence. 27 At the same time, caring relationships may be reorganized into a managerial arrangement in which some manage and others are managed, with dignity and meaning in life increasingly marginalized within safety-centered discourse. 28
Digitalization renders this problem more urgent not simply because it introduces an additional tool, but because it reshapes how restrictive practices operate and under what conditions they can be contested. As monitoring becomes routine and preventive, restrictions are less readily recognized as restrictions and are correspondingly harder to challenge as excessive. For example, location wristbands or GPS tracking devices may initially be introduced to address a clearly defined risk of wandering. Yet when their use expands to round-the-clock location logging, real-time access by family members, and alerts for atypical activity, protection aimed at a specific risk can shift into ongoing management of everyday life through continuous visibility. Similarly, bed-exit alarms or bedside monitoring sensors may be ethically intelligible when night-time fall risk is elevated. However, when records are retained over extended periods, used to judge compliance with care routines, or employed to trigger broader restrictions on activity, the practice can exceed its original safety rationale and raise concerns about dignity, privacy, and agency.29,30 Review studies likewise identify privacy, informed consent, autonomy, intrusiveness, accessibility, and fairness as co-present core issues. They indicate that the normative difficulties of digital care are often multidimensional structural tensions, rather than problems that can be resolved through a single compliance or disclosure procedure.31,32
Against this backdrop, the normative problem targeted in this study is as follows. When “safety” is granted overriding moral priority, restrictive measures cease to be merely technical options for risk control and inevitably become ethical judgments concerning personal freedoms, dignity, and the distribution of relational power. As digital surveillance becomes increasingly normalized, restrictions are more easily naturalized as reasonable protection, while their erosive effects on autonomy and dignity are more likely to be justified through discourses of care and responsibility. This creates an urgent need for a normative analysis that articulates clear boundary conditions. Such an analysis should acknowledge vulnerability and the realities of risk in care settings, while also imposing explicit constraints on restrictions advanced under safety-based justification. Doing so enables a clear and defensible distinction between necessary protection and benevolent coercion.
Provenance and limitations of existing ethical frameworks
Ethical discussions of safety-justified restrictive measures in elder care can be broadly organized into three approaches. The first is a clinical bioethics approach grounded in autonomy and principlism. The second is a risk governance approach centered on identifying and controlling risk. The third is a privacy and technology ethics approach focused on data protection, informed consent, and compliance-oriented regulation. Together, these approaches offer important resources for understanding value conflict, risk management, and the governance of digital care. Yet when restrictive measures enter care relationships through care-laden justification and generate substantive effects on power under the banners of protection, responsibility, and risk prevention, these frameworks often struggle to specify sufficiently granular and practicable normative boundaries.
First, autonomy-focused principlism is rooted in the tradition of clinical bioethics and relies on a normative vocabulary of respect for autonomy, beneficence, nonmaleficence, and justice. A key contribution of this approach is that it evaluates restrictive care practices through conflicts among basic ethical principles, highlighting how mobility restrictions, substituted decision-making, physical restraint, and continuous monitoring can infringe older adults’ autonomy.33,34 It therefore brings the question of whether safety may override autonomy to the center of ethical analysis. Its main limitation, however, is a tendency to treat autonomy as an overly abstract, atomistic capacity. In everyday elder care, autonomy does not primarily appear as the rational choosing of an isolated individual. It is co-shaped by relations of dependency, care needs, institutional arrangements, and affective pressures. On the one hand, older adults may display autonomy that is context specific and temporally variable in the presence of functional decline, fluctuating cognition, or reliance on care. 35 On the other hand, even when decision-making capacity is intact, choices can be steered toward compliance through family expectations, institutional disciplinary routines, or caregivers’ moral exhortation. 36 More importantly, when restrictions are advanced in the caring language of “for your own good,” autonomy cannot be reduced to a simple yes or no of consent. What matters is whether older adults possess a genuine and practicable capacity to refuse, and whether they can voice disagreement without incurring relational penalties. 22 If analysis continues to rely on formal consent or a categorical separation between capacity and incapacity, it becomes easy to mistake dense relational pressures for voluntariness. In turn, this prevents recognition of the mild yet persistent curtailment of rights that can unfold within everyday care.
Second, the risk governance framework is largely shaped by patient safety initiatives, long-term care management, and institutional accountability practices. It emphasizes identifying, assessing, documenting, and controlling risks such as falls, wandering, medication errors, and acute health events. This framework is practically valuable in elder care because organizations and nursing staff must address preventable harms and use standardized processes to improve quality and strengthen accountability.13,37 Its central limitation, however, is a tendency to treat risk as neutral and objective, and as something that can be managed through technical and administrative control. This can obscure how risk is defined, amplified, and prioritized within concrete institutional arrangements and affective dynamics. Yet in long-term care, risk is rarely determined solely by probability and magnitude of harm. It is also shaped by organizational accountability, compliance audits, anticipated legal liability, and performance cultures oriented toward zero incidents.38,39 In parallel, family members’ worry and caregivers’ moral anxiety can elevate low-probability events into consequences perceived as intolerable, thereby encouraging the selection of more restrictive responses. Within this configuration, restrictive measures can be framed as responsible prudence, whereas less intrusive alternatives may be dismissed as insufficiently safe or insufficiently responsible. 40 Risk governance can therefore explain why care systems tend to intensify safety. It is less well equipped, however, to answer a more fundamental normative question: under what conditions does risk reduction provide adequate justification for restricting freedom, privacy, and dignity under safety justification? Put differently, it explains why restrictions emerge, but it offers fewer clear ethical thresholds for constraining the expansion of safety-based rationales.
Third, the compliance-style privacy and technology ethics framework is largely shaped by digital health governance, data protection, information security, and norms of informed consent. It is particularly salient in digital care settings involving monitoring technologies, remote care, smart home systems, sensors, and platform-mediated care. A key contribution of this framework is that it directs care organizations to attend to data collection, authorization and consent, access control, information retention, purpose limitation, and security safeguards, thereby resisting the tendency to treat digital care as merely a question of technical efficiency41–43 However, when the framework is reduced to compliance, ethical evaluation is often narrowed to procedural checklists, such as whether disclosure has been provided, whether authorization has been obtained, whether encryption and access controls are in place, and whether regulatory requirements are satisfied. 44 The difficulty is that privacy in elder care is not merely a matter of control over personal information. It also concerns bodily boundaries, domestic space, everyday routines, and personal dignity. Moreover, authorization is often vulnerable under conditions of care dependence and relational pressure. Procedural completion does not necessarily mean that older adults understand the implications or possess a genuine ability to refuse, withdraw, and reverse arrangements in practice. 45 Beyond this, many of the ethical harms associated with restrictive practices do not primarily take the form of data breaches. Instead, they manifest as experiential changes, including self-discipline induced by continual observation, contraction of the scope of choice, shame, and the condition of being rendered passively transparent. 25 If ethical questions are framed solely in terms of compliance and procedure, substantive infringements of rights can be misrecognized as having been consented to or as having been adequately addressed through governance.
In sum, each of these three approaches captures an important dimension of the problem. Autonomy-oriented bioethics foregrounds rights and choice. Risk governance highlights prevention and responsibility. Compliance-oriented privacy and technology ethics stresses procedure and data security. Their shared limitation, however, is the difficulty of articulating clear justificatory conditions in contexts where care-laden justification, power asymmetries, and restrictive consequences are tightly intertwined. The ethical problem of benevolent coercion is therefore not reducible to whether autonomy is infringed, whether risk is reduced, or whether compliance steps have been completed. It concerns how safety justification acquires an excessively moralized priority, how relational pressure is mistaken for voluntary consent, how accountability demands are treated as objective necessity, and how privacy and dignity are gradually eroded through ongoing care practices. For these reasons, a relational framework is needed that can better address dependency, relational pressure, and normative boundary setting, thereby engaging the core ethical questions of how safety justification can warrant restrictions and how such restrictions ought to be constrained.
Theoretical reframing: A relational legitimacy framework for benevolent coercion
A normative appraisal of restrictive care advanced under safety justification should begin from a basic presumption. Such restrictions are not value-neutral instruments of management. They can constitute a prima facie infringement on older adults’ mobility, bodily boundaries, privacy, the capacity to express preferences and refusals, and personal dignity. They therefore carry a stringent burden of justification. This claim also implies that coercion in care cannot be treated as a matter of professional judgment confined to the nurse–patient relationship. It also engages minimum requirements for protecting personal liberty and human rights. Put differently, “safety” should not be treated as a value with lexical priority. At most, it provides a reason in favor of intervention. It is not a warrant that automatically displaces other rights and values. The “rights” at stake refer to the core normative interests implicated by restrictive care, including mobility, bodily boundaries, participation and voice, private life, and self-determination. Although legal formulations and protection mechanisms for these interests vary across institutional settings, such variation does not undermine the paper’s central ethical claim. Any restriction advanced under safety justification should be required to account for and substantiate its potential harms to freedom, privacy, dignity, and agency.
This paper adopts care ethics and relational autonomy as its theoretical foundation not simply because they are widely used in nursing ethics scholarship, but because they speak directly to the relational conditions under which benevolent coercion arises. Restrictive measures often occur within care relationships marked by dependence, care-laden justification, family responsibility, and institutional accountability. Care ethics helps illuminate how care can, under claims of benevolence, become a vehicle for domination. Relational autonomy helps clarify how older adults’ consent, refusal, and participation can be supported or suppressed within relations of dependence. On this basis, care ethics and relational autonomy jointly impose two key constraints. First, the legitimacy of care does not rest on professed benevolence, but on whether responses to vulnerability sustain dignity and avoid producing domination and silencing within relations of dependence.46,47 Second, autonomy is not an abstract capacity of an isolated individual. It is a practice formed, expressed, and sometimes suppressed within relationships and care contexts. Accordingly, consent cannot be reduced to a single procedural event. It should be understood as an ongoing expression that is open to challenge, withdrawal, and revision.35,48 Together, these considerations yield a shared normative requirement. When restrictive measures enter care relationships on the grounds of protection, ethical evaluation must examine relational consequences, including whether dignity and agency are weakened, procedural quality, including whether the person has meaningful opportunities to speak and object, and power effects, including whether coercion is obscured by care-laden language.
Within this theoretical position, this paper conceptualizes benevolent coercion as a practice that is especially demanding to justify. It is typically initiated through the language of care and thereby gains moral acceptability, yet under conditions of power asymmetry it can systematically curtail older adults’ freedom, privacy, and scope of choice. Avoiding a simplistic good or bad verdict requires a justificatory structure that differentiates necessary protection from overreaching control. On this basis, the paper proposes the Relational Legitimacy Framework (RLF). The framework treats restrictive measures as interventions that can affect older adults’ core normative interests and minimum protections, rather than as value-neutral instruments of management. Ethical acceptability does not hinge on the pursuit of “safety” as such. It depends on whether an interlocking set of justificatory conditions is satisfied at the same time. Safety does not automatically enjoy overriding priority. Instead, restrictive measures must be defended as relationally defensible, procedurally defensible, and consistent with the minimum ethical boundaries required by dignity, privacy, and integrity of the person.
First, risk-grounded necessity and proportionality. Restrictive measures should be anchored in concrete and identifiable risks supported by adequate evidence, and the risk should be sufficiently serious to provide a moral rationale for intervention. The degree of restrictiveness, the duration of the measure, and the extent of intrusion should be proportionate to both the severity of potential harm and the likelihood of occurrence. 49 Proportionality does not become unstable in relational contexts. Rather, relational analysis helps identify the relevant factors that properly belong in proportionality judgments. These include how risk is defined, how restrictions are experienced by older adults in practice, and whether family pressure, caregivers’ anxiety, or organizational accountability is inflating perceived risk and prompting excessive restriction. The normative function of this condition is to prevent moral slippage produced by risk generalization. In practice, accountability pressures, caregiver anxiety, managerial convenience, or avoidable risks created by insufficient care resources may be framed as “objective risk,” thereby enabling restrictive measures to expand under safety justification. Proportionality review should therefore examine not only whether a restriction can reduce risk, but also whether the risk is real, specific, and directly relevant to the older person’s interests, whether risk reduction could instead be achieved through non-restrictive pathways such as environmental modification, resource enhancement, or additional care support, and whether the harms imposed on freedom, privacy, dignity, and agency have been fully considered. Restrictive measures should proceed to further ethical scrutiny only when the evidentiary threshold for the risk rationale is met and the level of restriction is proportionate to that risk.
Second, relationally less intrusive and adequate alternatives. The existence of real risk does not warrant immediate recourse to highly restrictive measures. Before adopting restrictions, this condition requires identifying and comparing alternatives that are less intrusive and still adequate to address the relevant risk. Less intrusive should not be understood only as fewer constraints on mobility. It also includes reducing harm to privacy boundaries, everyday agency, capacity for self-organization, and meaning in life. 4 Moreover, alternatives are not any options that might exist in theory. They are options that are reasonably feasible in the specific care context, address the primary risk, and align as far as possible with the older person’s values and preferences. For example, for an older adult who has experienced night-time fall risk, environmental lighting, bedside grab rails, night-time accompaniment, bed-exit alerts, and round-the-clock video monitoring may all be described as safety measures. This condition does not require a mechanical search for an absolutely least intrusive option that fails to address the risk. Nor does it imply that intrusiveness must always override health benefits or the person’s expressed preferences. It requires that when a more restrictive measure is selected, the care team must explain why less intrusive options are insufficient for addressing the specific risk. Restrictive measures are therefore potentially justifiable only when reasonably feasible and less intrusive alternatives cannot achieve the care aim.
Third, relational procedural legitimacy. Because elder care relationships are intrinsically marked by dependence and power asymmetries, restrictive measures that lack procedural legitimacy can be advanced through care-laden language in ways that are difficult to contest. Justification therefore cannot rest solely on outcomes. It must include procedural constraints. The person should be included in decision-making and have meaningful opportunities to express preferences, raise objections, and negotiate. Their wishes should be documented and substantively addressed rather than merely acknowledged in a symbolic manner. Especially where family obligations are strong and bargaining power is weak, consent can slide into pseudo-consent, meaning that apparent compliance is driven by relational pressure, emotional burdens, or dependence on resources rather than by adequate understanding and free expression. 5 Relational procedural legitimacy is designed to render such pressures visible and to mitigate them through institutional arrangements. It attends not only to whether consent is present, but also to how consent is formed, whether it can be withdrawn, and whether refusal triggers relational penalties. For older adults with impaired cognition or constrained expressive capacity, this condition does not rely on a simple dichotomy of capacity versus incapacity. Instead, it emphasizes supported decision-making and transparent proxy arrangements. Proxies should state the grounds for their judgments, rely as far as possible on the person’s prior preferences and currently expressible wishes, and remain subject to review in an auditable manner, thereby reducing the risk that substituted decision-making becomes arbitrary control.
Fourth, non-derogable dignity and privacy thresholds. Care ethics acknowledges the realities of vulnerability and dependency. Yet this does not imply that dignity and privacy may be fully instrumentalized under safety justification. The ethical aim of care is not limited to reducing adverse events. It is to respond to vulnerability while sustaining the care recipient’s standing as a person, including voice, dignity, and integrity of everyday life. Accordingly, when practices involve intimate bodily exposure, humiliating disclosure, denigration of personhood, or unbounded monitoring, the harm is not confined to ordinary privacy interests. Such practices undermine basic ethical conditions on which caring relationships depend. Similarly, in digital care, indefinite data retention, unrestricted access, or repurposing care data for managerial control, punishment, or responsibility shifting can constitute a structural erosion of personal dignity. 45 The point of this condition is to place a rigid constraint on the claimed moral priority of safety. It prevents ethical evaluation from collapsing into purely utilitarian balancing and ensures that care, even when framed as protection, does not cross non-negotiable limits.
Taken together, these four conditions specify the burden of justification for benevolent coercion. Any restrictive measure that fails to satisfy these relational conditions simultaneously remains difficult to defend ethically, even if intentions are benevolent and safety benefits are plausible. At the same time, the RLF includes an indispensable temporality clause. The legitimacy of restrictions is not conferred once and for all. It is a continuing obligation. Any restriction should include scheduled review points, mechanisms for updating evidence, and clear exit conditions. When risks diminish, capacities improve, or expressed wishes change, restrictions should be reduced, replaced, or withdrawn.
9
For example, location wristbands or bed-exit alarms should not continue indefinitely on the basis of a single episode of wandering risk or fall risk. When environmental modifications, rehabilitation, or accompaniment arrangements have reduced risk, or when the person persistently expresses distress, the nursing team should reassess necessity and consider limiting the time window of use, narrowing data access, or discontinuing the measure. The temporality clause turns justification from a static judgment into an ongoing responsibility. It helps prevent restrictions from hardening into permanent arrangements through institutional inertia and risk aversion, thereby converting temporary protection into enduring control. The overall logic of the framework is presented in Figure 1. Relational legitimacy framework for safety-justified restrictions in elder care.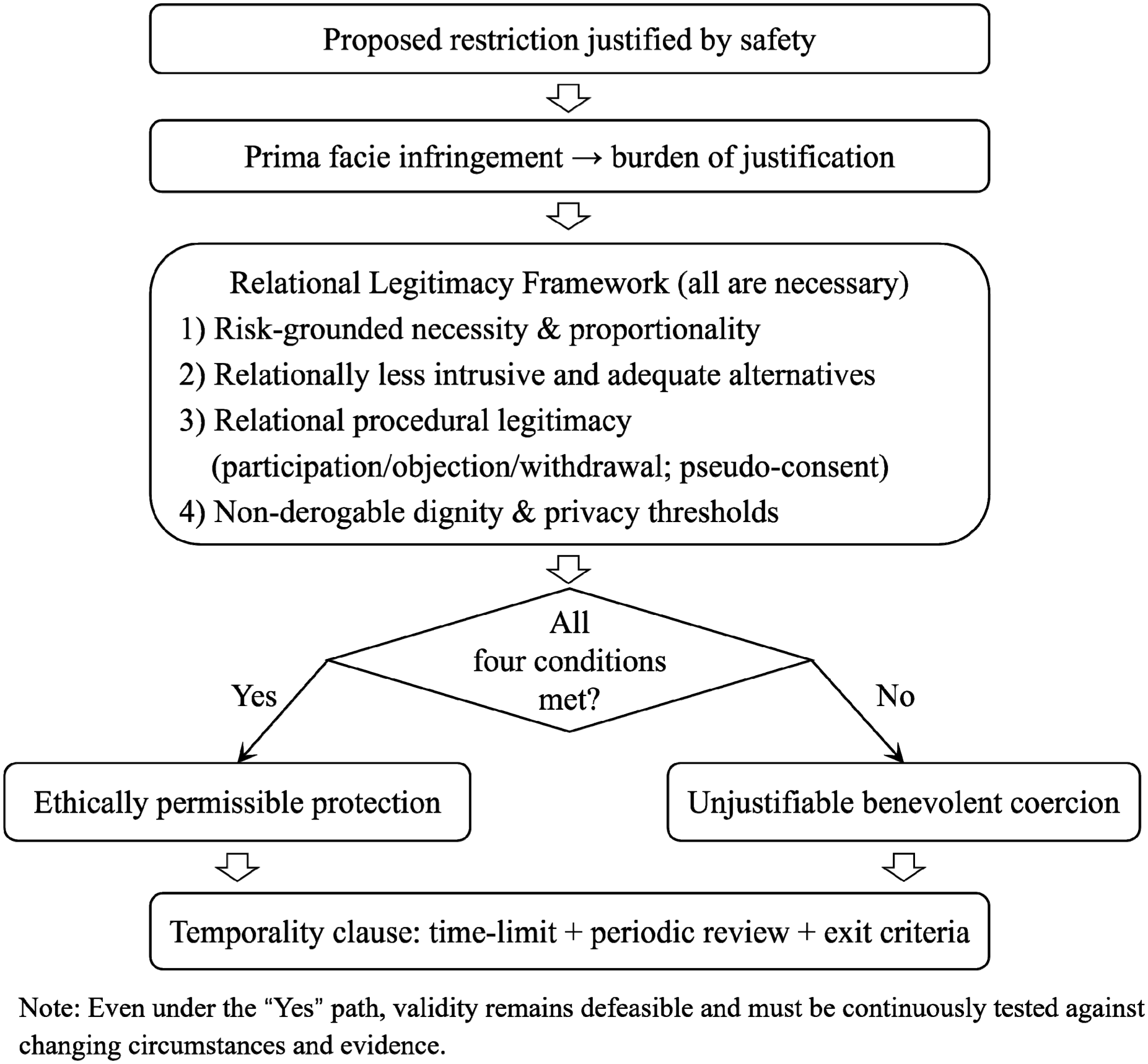
The Chinese context: An analytical field as mechanism revealing and framework calibration
The RLF advances a set of justificatory conditions with cross-contextual potential, yet its normative force must be examined under concrete care institutions and moral environments. The analytic value of the Chinese context does not lie in presenting a culturally exceptional case. Rather, it brings into sharp relief the ambivalence of relational norms. Family responsibility, filial obligations, and traditions of honoring older people can support intergenerational care, reinforce responsibilities to protect vulnerable older adults, and offer ethical resources for sustaining dignity. At the same time, when combined with risk anxiety, escalating care burdens, and institutional accountability, these norms can enable protection to be converted into control. Compliance can be framed as consideration, while dissent may be interpreted as being inconsiderate, immature, or as “adding trouble to the family.” 3 China is therefore not merely an illustration of the problem addressed in this paper. It is a particularly instructive context for showing why safety justification must be subject to relational scrutiny.
First, moral intensification can grant safety restrictions a moralized priority that weakens relational procedural legitimacy. In settings shaped by family responsibility and filial norms, adverse events may be interpreted not only as risk occurrences but also as familial dereliction and moral failure. At the same time, traditions of honoring older people are not simply resources for control. They can also support the protection of older adults’ voice, dignity, and integrity of everyday life. The difficulty arises when these traditions intersect with care pressure, risk anxiety, and accountability mechanisms. Under such conditions, honoring older people can be reinterpreted as a mandate to protect them from all risk, making restrictive measures appear as self-evident responsibilities rather than as options requiring explanation and negotiation. Moral narratives such as not letting one’s children worry, acting for the good of the family, and protecting the older person can generate strong pressure. Restrictions then cease to appear as choices open to deliberation and instead are presented as the only responsible course of action.50,51 Dissent is correspondingly recast as willfulness, selfishness, or a failure to consider the burdens borne by one’s family. In this setting, the RLF requirement of relational procedural legitimacy is not satisfied by formally soliciting views. It requires that older adults be able to refuse without incurring relational penalties and that refusal be treated as a moral stance warranting response rather than as an error to be corrected. The ethical potential of honoring older people norms should not be denied, yet it should not be equated with ever stronger protection. Its proper normative meaning lies in supporting dignity, participation, and non-humiliating care, not in providing moral authorization for non-refusable safety control.
Second, responsibility shifting turns safety-oriented logic into a conduit for offloading responsibility and for performance-driven care, thereby distorting judgments about necessity and relationally less intrusive and adequate alternatives. Under conditions of constrained resources, escalating care burdens, and insufficient formal care and community support, families are more readily expected to absorb risk. Technologies and institutional arrangements can likewise be mobilized to legitimate forms of substitute care. Care is reframed as indicators, records, and auditable managerial targets, and responsibility shifts from relational practice to quantifiable completion.26,52 In this context, invoking safety is not only a rationale for protecting the care recipient. It can also function as strategic language for distributing responsibility and deflecting accountability. Restrictions may be selected not because they are proportionate and less intrusive for the person, but because they are easier to control within organizational governance, easier to attribute in responsibility assignments, and easier to defend in subsequent audits and accountability processes. 53 This mechanism indicates that the first and second RLF conditions require stricter enforcement. Risk-grounded necessity must distinguish reasons genuinely directed toward the care recipient’s risk from reasons driven by accountability pressures. Relationally less intrusive and adequate alternatives must require not only comparisons of risk reduction benefits across options, but also identification of pseudo alternatives whose implicit motives are managerial convenience or responsibility shifting, so that organizational rationality is not mistaken for ethical legitimacy. This analysis also shows that the Chinese context is not a cultural exception that relaxes proportionality requirements. On the contrary, it makes visible how proportionality judgments can be distorted by family responsibility narratives, caregiver anxiety, insufficient resource provision, and institutional accountability logics. It therefore strengthens the case for requiring necessity, proportionality, and less intrusive alternatives to be articulated in ways that are open to scrutiny.
Third, consent fragility increases the likelihood of pseudo-consent, requiring consent to be redefined as a relational procedure rather than a one-time authorization. In the Chinese context, the digital divide intersects with dependency structures. Older adults may be disadvantaged in technological comprehension, access to information, and bargaining power, while their access to care resources depends heavily on families or institutions. 54 At the same time, moral expectations tied to filial piety and responsibility make refusal more likely to carry relational costs. 55 As a result, formal consent does not necessarily amount to normative authorization. Consent may reflect compliance motivated by a desire not to burden one’s family, a concession to moral pressure, or passive acceptance under information asymmetries.56,57 This mechanism implies that the third RLF condition must incorporate a clearer structure for resisting pseudo-consent. Procedural legitimacy should not be reduced to disclosure and signatures. It should include identifying and mitigating relational pressures. For example, it should require context-sensitive assessment of how consent is formed, including whether moral exhortation, shaming language, or threats to withdraw resources are present. It should require withdrawal mechanisms that do not trigger relational penalties. It should also provide older adults with an independent voice channel in family or institutional deliberations and treat dissent as legitimate input requiring response rather than as an error to be corrected. 58
Under these mechanisms, two points of calibration for the RLF can be specified as normative reinforcements. First, assessments of necessity and proportionality must distinguish real risk from accountability anxiety. Any restrictive measure should therefore specify its evidentiary basis for the relevant risk, articulate its proportionality reasoning, and document its assessment of alternatives, rather than substituting broad just-in-case claims for ethical justification. Second, assessments of relational procedural legitimacy must treat relational pressure and pseudo-consent as expected structural risks rather than as isolated exceptions. Dissent should therefore be protected through independent voice channels, withdrawal mechanisms that are feasible and non-punitive, and proxy decision-making procedures that are transparent and subject to review. It can thus be seen that the theoretical significance of the Chinese context does not lie in claiming that any particular culture is more prone to benevolent coercion. It lies in showing how relational norms can function simultaneously as resources for care and as pathways to control. Family responsibility, filial obligations, and traditions of honoring older people can support intergenerational care and sustain dignity. Yet under the combined effects of risk anxiety, escalating care burdens, and institutional accountability, they can also be converted into a logic of protection that is difficult to refuse. Compared with autonomy-centered frameworks that emphasize individual choice and formal consent, this context more clearly illustrates that older adults’ consent, refusal, and participation often take shape within family obligations, emotional burdens, and institutional responsibilities. Similar relational tensions may arise, in different forms, in other societies that emphasize intergenerational responsibility, multigenerational care, or professionalized risk governance. China is therefore not a cultural exception to the RLF. It is an analytic site for testing and refining its justificatory conditions. Across cultural and institutional settings, the enduring questions concern how safety justification acquires moral authority, who is entitled to define risk, and when relational care shifts from support to control.
Implications for nursing practice and organizational policy: Embedding justificatory conditions in decision processes
Accordingly, the key task for nursing practice and organizational policy is not simply whether technologies are adopted or whether safety is prioritized. It is to subject restrictive measures to scrutiny within a framework of personal liberty, minimum human rights protections, and organizational ethical governance. Once coercion in care involves mobility restriction, continuous monitoring, physical restraint, substituted decision-making, or arrangements that cannot be freely withdrawn, it can no longer be treated as professional judgment confined to the nurse–patient relationship. It implicates core normative interests, including mobility, bodily integrity, privacy, dignity, and opportunities for voice and participation. The practical contribution of the RLF is to translate safety justification into justificatory procedures that are implementable, reviewable, and withdrawable. In doing so, restrictive measures no longer take effect by default under labels such as usual care or for safety. They become subject to rights-attentive organizational review. For nursing ethics, this implies a shift from reliance on individual nurses’ moral sensitivity to the development of organized, rights-attentive ethical governance. The burden of justification for safety-oriented restrictions should be made explicit and procedural, and nurses should carry corresponding professional responsibilities for identifying risk, documenting reasons, safeguarding expression, prompting withdrawal, and triggering reassessment.
First, relational justification protocol: translating the four conditions into ex ante review and documentation duties. In everyday practice, restrictions are often initiated quickly under the banner of risk prevention and then become routine. A primary pathway for implementing the RLF is therefore to establish an anticipatory justificatory protocol that converts the four conditions into core steps of clinical and ethical decision-making and generates an auditable record. At a minimum, the protocol should include: clarification of the risk rationale, specifying risk type, severity, likelihood, and evidentiary sources and indicating whether risk could be reduced through less restrictive routes such as environmental modification, adjustment of staffing, strengthening community support, improving access to nutrition and medical care, or supporting digital capabilities; proportionality reasoning, explaining why the intensity, duration, and extent of intrusion are commensurate with the risk and whether the costs imposed on freedom, privacy, dignity, and agency have been considered; systematic comparison of alternatives, explaining why less intrusive options cannot reasonably achieve the care aim; documentation of relational procedural legitimacy, recording whether the person participated, whether dissent was expressed, and how dissent was addressed; and documentation of non-derogable dignity and privacy thresholds, clarifying which spaces and practices are excluded and how relevant data will be governed. For example, if a facility proposes to introduce a location wristband for an older adult with a history of wandering, the record should not stop at stating prevention of wandering. It should specify the evidence for the risk, whether less intrusive options such as accompanied outings, environmental cues, or adjustments in activity planning have been attempted, who has access to location data and the retention period, and whether the older person can request suspension or limitation of use to specific time windows. Where risk primarily arises from remediable resource gaps or deficient care environments, turning immediately to continuous monitoring, mobility restriction, or substituted decision-making is unlikely to constitute a sufficiently justified response under safety justification. Documentation here is not merely administrative. It is normative accountability. It compels teams to convert safety claims from intuitive slogans into arguable reasons and places restrictive measures on a reviewable ethical trajectory rather than allowing them to rest on self-validating claims of for your own good. For organizations, such documentation also supports quality governance by making the initiation, continuation, and withdrawal of restrictive measures objects of internal review and ethical deliberation, rather than reducing performance assessment to incident rates alone.
Second, relational consent and withdrawal mechanisms: reconstructing consent from one-time authorization into an ongoing practice of expression. In practice, the RLF requirement of relational procedural legitimacy is easily reduced to formal compliance centered on disclosure and signatures. Institutionalized mechanisms for consent and withdrawal are therefore needed to counter relational pressure and power asymmetries. For nurses, this means treating consent as a continuing process. It requires not only ensuring that the person understands the content and implications of the intervention, but also assessing whether expressed preferences are shaped by moral exhortation, shaming language, or dependence on resources, thereby identifying risks of pseudo-consent. For example, an older adult may initially agree to wear a location-tracking device to reduce the risk of wandering during outings. If location information is later expanded to round-the-clock access by family members, use in organizational activity management, or logging of atypical activity, the original consent cannot automatically be assumed to cover the expanded use. Relational procedural legitimacy therefore requires ongoing confirmation of monitoring purposes, data pathways, and workable withdrawal options, rather than treating one-time authorization as a substitute for continuing review. At the organizational level, consent quality can be incorporated into procedures. For example, an independent voice channel can be required for the person in family conferences or organizational decision processes. Withdrawal should be feasible and non-punitive, and responses to dissent should be documented and revisited. For people with cognitive impairment, the practical focus should not be a simple dichotomy of capacity versus incapacity. It should emphasize supported decision-making and transparent proxy arrangements. Nursing teams should prioritize communication support, preference elicitation, and stepwise decisions in order to preserve the ethical weight of the person’s wishes. When proxy decision-making is unavoidable, reasons should be stated in a traceable and explainable manner and grounded as far as possible in prior preferences and currently expressible wishes, rather than allowing claims of safety necessity to substitute for the person’s own value judgments.
Third, privacy by default thresholds: embedding non-derogable dignity and privacy thresholds in organizational rules and care environments. The fourth RLF condition treats dignity and privacy thresholds as a threshold constraint rather than as variables open to discretionary balancing. The policy implication is that organizations should elevate privacy protection from case-by-case negotiation to default rules that predefine the permissible scope and intensity of intrusion. The RLF does not require treating all privacy interests as absolute and non-adjustable. It requires identifying in advance the high-risk settings most likely to produce humiliation, denigration of personhood, and unbounded visibility and placing them within the default zone of protection. In practice, at least three categories of thresholds should be specified. First, spatial thresholds. Areas with heightened risks of intimate exposure and humiliation, such as bathing, toileting, and changing, should be governed by a default non-monitoring principle, with explicit criteria for any exceptions. Second, access thresholds. The field of visibility and access permissions should be limited so that safety justification does not produce unbounded expansion of visibility. Third, data thresholds. Data retention periods, purpose limitations, and prohibitions on secondary use should be clearly specified so that purpose drift does not convert care data into instruments of management or punishment. For nursing organizations, the significance of privacy by default thresholds is that refusing certain practices becomes an institutional obligation rather than a demand for individual nurses’ moral courage. This reduces the ethical burden on frontline staff under accountability pressure and makes dignity protection a system-level arrangement.
Fourth, periodic review and exit criteria: transforming restrictions from one-time decisions into temporary measures that can be withdrawn. A common ethical risk of restrictive measures is entrenchment. Once introduced, restrictions can persist through risk aversion, institutional inertia, and convenience. The RLF temporality clause requires the legitimacy of restrictions to be treated as defeasible and makes that defeasibility operational through periodic review and clear exit criteria. Organizations can require that any restrictive measure specify a time limit, a review schedule, and exit conditions, such as reduced risk, feasible alternatives, changes in expressed wishes, or adjustments in environment and staffing. Reviews should again assess necessity and proportionality and re-examine alternatives. For nurses, review should not be a procedural formality. It is continuing ethical governance of the relationship among risk, freedom, and dignity. When necessity no longer holds or less intrusive alternatives become available, withdrawal becomes an ethical responsibility rather than a discretionary option. At the policy level, this also entails shifting from treating safety as a single outcome metric to treating it as a process governance metric. Initiation rates, duration, withdrawal rates, and documented reasons for restrictive measures should all be core indicators in quality management and ethical review.
Conclusion
This paper does not deny the value of safety, nor does it reject digital technologies as such. Its central claim is that when “safety” is granted overriding moral priority in elder care, restrictive measures can readily expand under the shelter of care-laden justification and drift toward benevolent coercion that becomes difficult to recognize and contest. Safety therefore should not be treated as a warrant that automatically displaces autonomy, privacy, and dignity. Instead, any restriction advanced under safety justification should be treated as a prima facie infringement and should carry a corresponding burden of justification. This also implies that coercion in care cannot be reduced to routine professional judgment confined to the nurse–patient relationship. It should be examined within a broader framework of personal liberty, minimum human rights protections, and organizational ethical governance.
Against this background, the paper’s theoretical contribution is twofold. First, through conceptual clarification, it locates benevolent coercion as a structural and routinized ethical risk in nursing practice, thereby avoiding its mischaracterization as a small number of extreme cases or as merely a problem of intentions. Second, grounded in care ethics and relational autonomy, it develops the Relational Legitimacy Framework. The framework specifies a shared set of conditions for ethical acceptability, including risk-grounded necessity and proportionality, relationally less intrusive and adequate alternatives, relational procedural legitimacy, including safeguards for identifying pseudo-consent and ensuring revocability, and non-derogable dignity and privacy thresholds. These conditions are coupled with a temporality clause, yielding a reusable justificatory structure for distinguishing defensible protective interventions from unjustified forms of controlling intervention.
The Chinese context further serves as an analytic site for mechanism elucidation and framework calibration. It shows how safety discourse can acquire heightened moral authority through the intersection of family responsibility ethics and institutionalized risk governance. It also shows how consent can become especially vulnerable under relations of dependence, informational asymmetries, and resource constraints, making relational procedural legitimacy and the burden of justification easier to hollow out in practice. For this reason, the normative structure proposed here addresses boundary questions at the level of theory while also offering clear directions for nursing practice and organizational governance. It calls for institutionalizing safety justification as an ethical process that is reviewable, withdrawable, and subject to periodic reassessment so that restrictive measures no longer take effect by default under labels such as “usual care” or “for your own good” but are instead subject to rights-attentive organizational scrutiny. Only under such conditions can care avoid becoming an ongoing erosion of older adults’ personal liberty, dignity, and autonomy under claims of protection.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Social Science Fund of China (No. 22BSH023) and SEU Innovation Capability Enhancement Plan for Doctoral Students (No. CXJH_SEU 26247).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analyzed during this study.