
Abstract
Background
Ethical dilemmas in pediatric oncology represent a major challenge for nurses, significantly impacting their well-being and motivation at work.
Research aim
The objective of this study was to identify the ethical dilemmas experienced by nurses through a sample recruited from two pediatric cancer treatment units.
Research design
This study adopts an interpretative phenomenological qualitative approach based on interviews conducted with nurses working in pediatric oncology.
Ethical considerations
The study adhered to ethical principles. Institutional authorization was obtained prior to data collection, and participants’ confidentiality and anonymity were strictly ensured.
Findings
The findings revealed that nurses face ethical dilemmas on a daily basis, structured around four main thematic domains: communication and decision-making, pain and care practices, professional integrity and safety, and systemic and contextual constraints. These dilemmas encompass issues such as truth-telling, treatment refusal, pain management, medication errors, resource allocation, confidentiality, and end-of-life decisions, including treatment futility. These situations have a significant impact on nurses’ well-being and on the quality of care provided.
Discussion and conclusion
Our findings align with international literature, highlighting that poor service management, institutional conflicts, heavy workloads, and unrealistic expectations from some families also contribute to the psychological and moral distress of nurses. This study underscores the need to implement support mechanisms to help nurses navigate ethical dilemmas. Improving healthcare organization, providing continuous training, and ensuring appropriate supervision could reduce moral distress among caregivers and enhance the quality of care for children with cancer.
Introduction
Cancer is one of the leading causes of death among children and adolescents worldwide. According to the World Health Organization (WHO), more than 1000 children are diagnosed with cancer every day, illustrating the scale of this pediatric disease. 1 In Morocco, the Greater Casablanca Cancer Registry recorded 566 new cases of pediatric cancer between 2018 and 2021, representing 2.6% of all cancers of all ages. 2 These figures highlight the importance of this public health issue and the challenges it poses for healthcare structures.
Thanks to advances in diagnostic techniques and multimodal therapeutic strategies, survival rates for pediatric cancers have risen considerably in recent decades. However, caring for these children exposes healthcare professionals, particularly pediatric oncology nurses, to complex situations, both medically and ethically. Among these complexities is nurses’ ability to identify and manage the ethical dilemmas they encounter daily in their practice.3,4
Pediatric oncology is widely recognized as a field in which ethical conflicts are frequent and often particularly complex. These dilemmas arise from tensions between several fundamental ethical principles, such as respect for autonomy, beneficence, non-maleficence and justice. They can involve complex decisions about treatment, communication with families, pain management and end-of-life issues. These tensions affect not only the quality of care, but also the psychological and moral health of nurses, who have to juggle professional obligations with personal values.
In addition, ethical tensions are particularly salient in the context of clinical procedures performed on children. Many pediatric oncology interventions are invasive, repetitive, and potentially distressing, raising important concerns regarding children’s rights, including the right to be informed, to express their views, and to be protected from unnecessary harm. Evidence shows that inadequate preparation and insufficient information can increase children’s anxiety and negatively affect their experience of care.5,6 Furthermore, situations in which children are physically held during procedures highlight the ethical complexity of balancing clinical necessity with respect for the child’s dignity and autonomy. 7 In this context, ensuring appropriate procedural preparation and support is increasingly recognized as a fundamental component of ethical pediatric oncology care. 8
Building on these considerations, the literature suggests that ethical challenges in pediatric oncology arise in a wide range of clinical situations. These may include issues related to communication with children and families, decision-making processes, pain management, invasive procedures, and end-of-life care. While these situations have been described in previous studies, the way in which nurses experience, interpret, and manage these ethical tensions in their daily practice remains complex and context-dependent. Rather than representing fixed categories, these dilemmas often overlap and evolve within clinical interactions, highlighting the need for an in-depth exploration of nurses’ lived experiences.9–14
However, despite the growing international body of research, little is known about how these ethical dilemmas are experienced in specific socio-cultural and healthcare contexts such as Morocco. In particular, the organizational constraints, resource limitations, and cultural dynamics that shape pediatric oncology care may influence both the nature of ethical dilemmas and the ways in which nurses respond to them. Therefore, the present study aims to explore the ethical dilemmas experienced by nurses working in two facilities caring for children with cancer within a university hospital in Morocco. The aim is to identify the nature of the dilemmas encountered, to analyze their impact on nursing practice, and to suggest ways in which nurses can be better supported in managing these complex situations.
Methods
Type of study
This study adopts an interpretative phenomenological qualitative approach (IPA). 15 This approach is particularly suited to exploring how individuals make sense of their lived experiences, especially in complex and emotionally charged contexts such as pediatric oncology. It enables an in-depth understanding of nurses’ perceptions, meanings, and interpretations of the ethical dilemmas they encounter in their daily practice.
Study participants
The study population consisted of nurses working in two pediatric oncology departments in Morocco. Their involvement in daily care positions them as key informants for exploring ethically challenging situations in this context.
The inclusion criteria were as follows 1 : nurses working directly in pediatric oncology departments, and 2 having at least 2 years of professional experience in these services, in order to ensure sufficient familiarity with the clinical context.
The study adopted an exploratory approach, focusing on nurses’ lived experiences and perceptions of ethically challenging situations in their practice.
Sampling and data analysis were conducted concurrently until data saturation was reached.
Data collection
Data were collected between November and December 2024 through semi-structured, face-to-face interviews with the participants. The interviews were conducted by H.T. Each interview took place in a quiet and private environment within the hospital, at a time convenient for the participants and with their prior agreement. In total, 20 interviews were carried out with pediatric oncology nurses. The interviews enabled an in-depth exploration of nurses’ lived experiences of ethically challenging situations in their daily practice.
An interview guide was developed based on the study objectives and informed by existing literature, while remaining open-ended to allow new themes to emerge inductively. It included the following: • Sociodemographic characteristics of participants • Open-ended questions exploring experiences of ethically challenging situations • Probing questions to deepen understanding of emotions, perceptions, and coping strategies • Reflective questions inviting participants to suggest improvements in managing ethical dilemmas
Each interview lasted between 60 and 90 min. All interviews with the permission of the participants were audio-recorded. Each participant was given a code including N1, N2, and so on.
Data analysis
Data analysis followed a rigorous and systematic approach, aimed at identifying the major themes emerging from the interviews. It took place in several key stages:
Pre-analysis, transcription and playback
Interviews were recorded using a digital audio device to ensure secure data storage. Immediately after each interview, the recordings were replayed and transcribed verbatim using Microsoft Word to ensure an accurate representation of participants’ accounts. All transcripts were anonymized by removing any identifying information.
In addition to verbal data, field notes were taken during and immediately after the interviews to capture contextual and non-verbal elements (e.g., pauses, tone, and emotional expressions). These elements were not formally coded but were used to support the interpretation of the data.
An initial immersive reading was conducted to gain a comprehensive understanding of the data, followed by a more detailed analysis to identify emerging themes.
Initial and thematic coding
This stage identified minimum meaning units (MSUs), classified according to themes emerging from the verbatim. The initial coding was conducted by H.T. J.O, based on several iterative readings of the transcripts to ensure a comprehensive and consistent analysis. The coding process was subsequently reviewed and discussed with H.A, M.O and N.G., allowing for refinement and validation of the emerging themes. Each meaning unit was then associated with a specific thematic category.
Categorizing and linking data
The thematic categories were progressively refined through discussions among the research team (H.T., J.O., H.A., M.S., and N.G.) to establish links between main and secondary themes. These collaborative exchanges enabled the identification of thematic relationships, including oppositions and complementarities, thereby enhancing the depth and credibility of the analysis. A classification grid, initially developed from early interviews, was iteratively enriched throughout this phase.
Researcher reflexivity
The researchers acknowledge that their professional background in healthcare, particularly in oncology and nursing practice, may have influenced data interpretation. Their familiarity with the clinical context facilitated access to the field and a deeper understanding of participants’ experiences, while also requiring careful reflexivity to minimize potential bias.
Throughout the research process, reflexive discussions were conducted within the team to critically examine assumptions and interpretations. The researchers remained attentive to participants’ meanings, aiming to stay as close as possible to their lived experiences while engaging in an interpretative process consistent with IPA.
Presentation of results
The main themes were clearly identified as being directly related to the research question, while secondary themes enriched and contextualized certain aspects of the findings. The results are presented as themes organized into sub-themes in a structured manner.
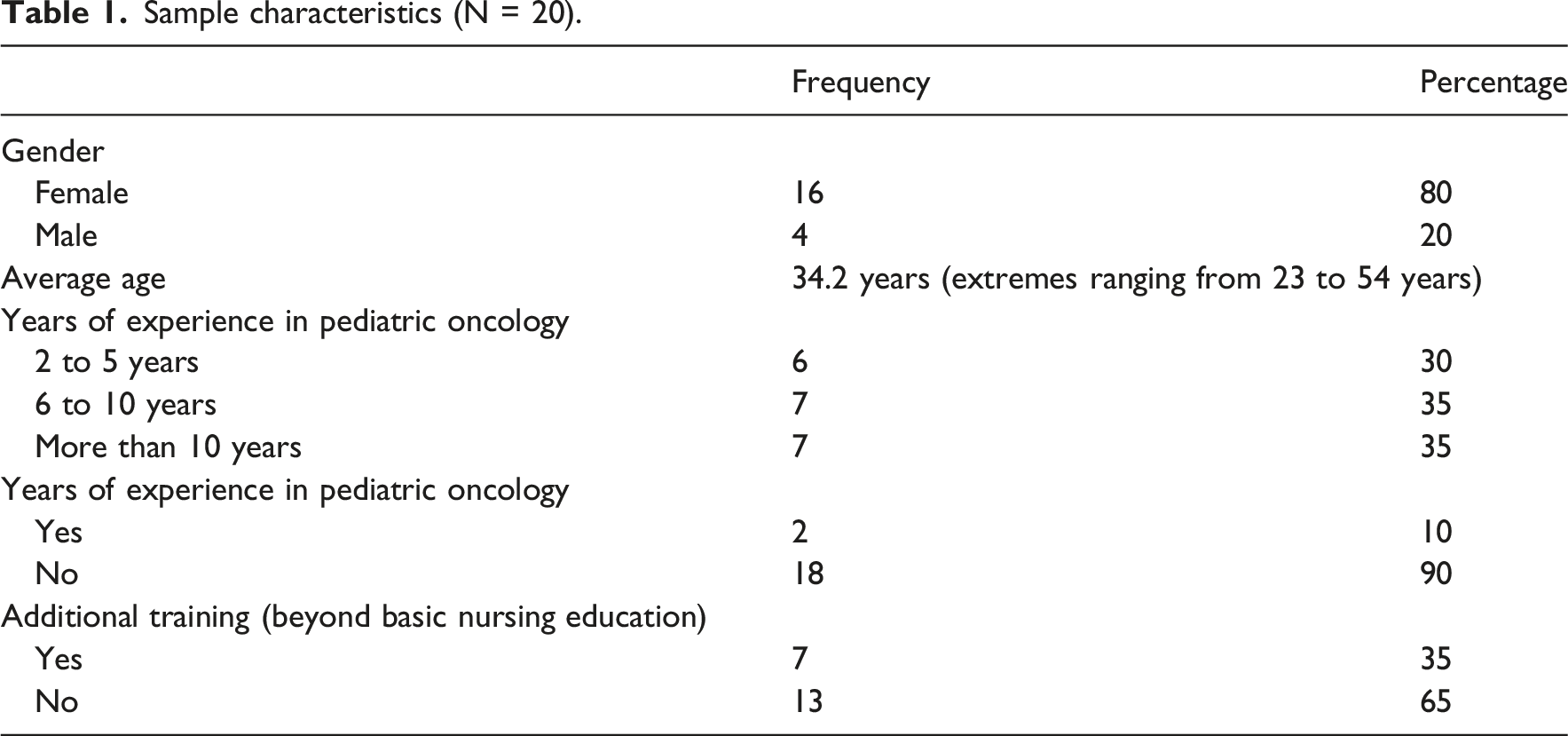
Participants’ characteristics, such as age and years of experience, were summarized using descriptive statistics (numbers and percentages) to provide an overview of the study sample.
Rigor
The analysis followed the principles of interpretative phenomenological analysis, moving from detailed examination of individual accounts to the identification of shared patterns across participants. Coding was performed independently by two researchers (H.T and J.O), followed by discussions to reach consensus and ensure consistency. Discrepancies were resolved through iterative review of the data.
To enhance the credibility of the findings, several strategies were employed, including double coding, triangulation between researchers, and regular discussions within the research team to refine the themes.
This study was conducted and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines.
Ethical consideration
The study complied with ethical standards for research involving human subjects. Formal approval from an ethics committee was not required in accordance with local regulations. Institutional permission to conduct the study was obtained prior to data collection.
Participation was voluntary, and informed consent was obtained from all participants prior to the interviews. To ensure confidentiality and anonymity, no identifying information was included in the transcripts. Each participant was assigned a unique code, and all data were stored securely on password-protected devices accessible only to the research team. Audio recordings were anonymized during transcription and were not shared outside the research team. Participants were informed of their right to withdraw from the study at any time without any consequences.
Results
Sample characteristics (N = 20).
Ethical dilemmas
The analysis revealed four interrelated themes reflecting nurses’ lived experiences of ethical dilemmas in pediatric oncology: (1) ethical tensions in communication and decision-making, (2) pain and care practices, (3) professional integrity and safety, and (4) Systemic and Contextual Constraints (Figure 1). Overview of the thematic structure of ethical dilemmas experienced by pediatric oncology nurses.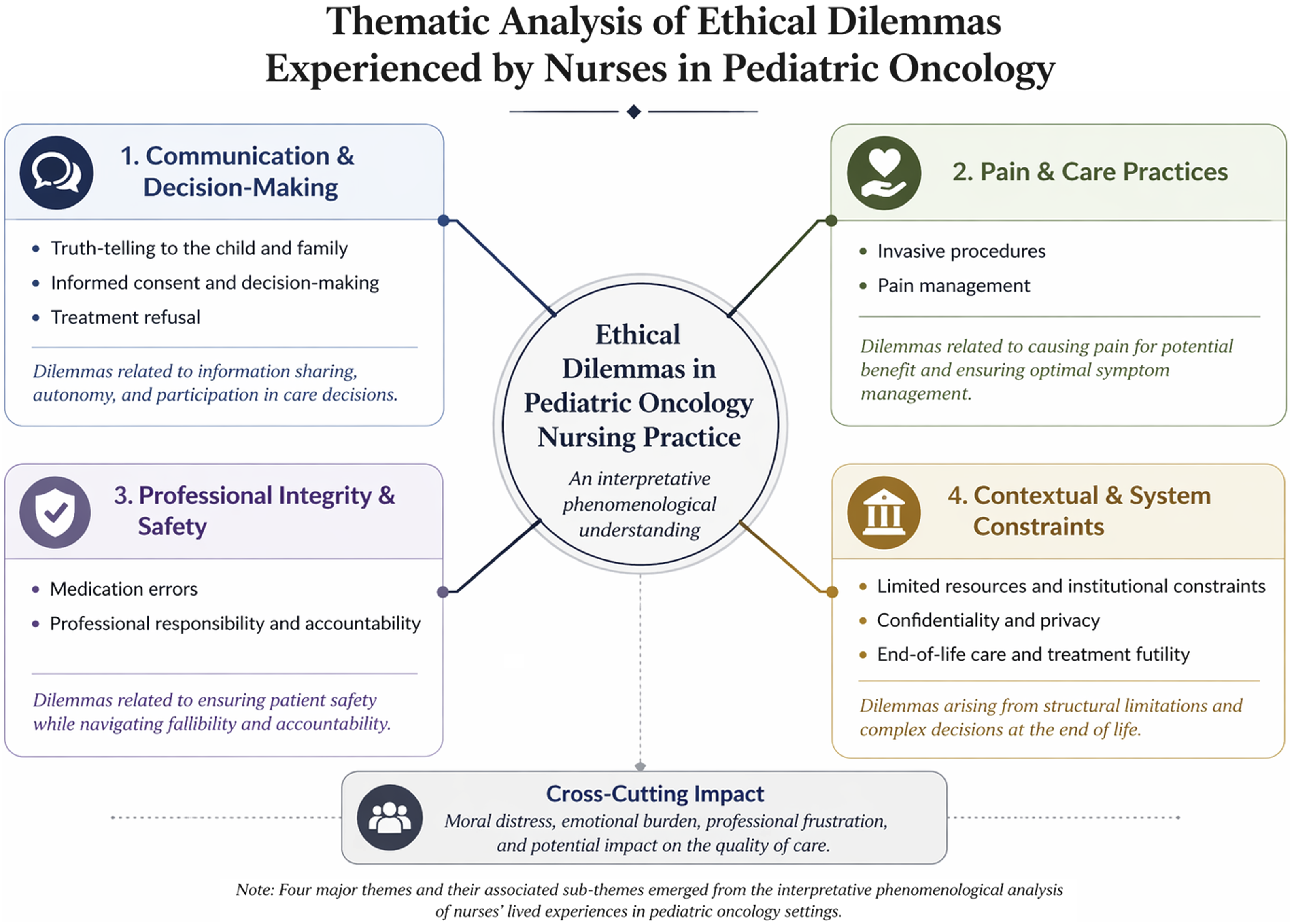
Ethical tensions in communication and decision-making
Participants described communication with children and families as a major source of ethical tension. Nurses frequently found themselves caught between respecting the child’s right to information and the perceived need to protect them from psychological harm.
Some participants highlighted physicians’ reluctance to disclose difficult information directly to children, which placed nurses in an intermediary and often uncomfortable position: “We still have a problem with the announcement of a diagnosis, especially when it involves therapeutic failure or a move to palliative care. Doctors are unable to communicate this to families” (N5)
This lack of transparency generated feelings of discomfort and ethical ambiguity among nurses, who felt complicit in withholding information: “Not informing patients puts us in a delicate situation. We feel like thieves during care” (N11)
Informed consent was also perceived as ethically problematic. Participants described it as a formal process that often failed to ensure genuine understanding, particularly in contexts marked by limited health literacy: “It’s just a signature without enough information to make a decision” (N8)
The child’s “There are many families who totally refuse to inform the child… but we respect their decision” (N17)
Similarly, situations of “I force them to have the treatment because it’s in their best interest” (N1)
Parental refusal was often perceived as beyond the nurses’ scope of action, leading to frustration and a sense of powerlessness: “We make every effort to convince them, but if they don’t agree, there’s nothing we can do” (N10)
These situations generated significant emotional distress, as nurses struggled to reconcile respect for family decisions with their professional commitment to protect the child.
Pain and care practices
A central theme emerging from the analysis was the ethical tension associated with “Yes, we’re going to generate pain, but it’s temporary and negligible compared to the benefits of the treatment” (N19)
Despite this rationalization, many nurses reported feelings of guilt and emotional discomfort: “You feel guilty, and I can’t forgive myself for having caused this child pain” (N5)
This tension was particularly pronounced among nurses who identified strongly with the children, especially those who were parents themselves: “Since I’ve had children, I can’t do this kind of care anymore” (N7)
“We don’t even assess pain” (N5) “Sometimes, we don’t even have paracetamol” (N15)
Participants also highlighted physicians’ reluctance to prescribe strong analgesics, contributing to inadequate pain control: “Doctors have a morphinophobia” (N12)
These factors contributed to a profound sense of moral distress, as nurses witnessed children’s suffering without being able to adequately relieve it Figure 1: “You see the child suffering, and you can’t calm him down… it wears on me morally” (N11)
Professional integrity and safety
“If an error occurs, I immediately inform the doctor” (N13)
However, errors were often attributed to structural factors such as workload and prescribing issues: “If you have ten patients, the quality of care decreases” (N18)
Beyond practical considerations, these situations were associated with intense emotional and moral suffering. Nurses described feelings of guilt and psychological distress, particularly when errors involved children: “I became mentally ill; I couldn’t accept the fact that I’d made a mistake” (N6)
“The child’s interest is paramount, even if it creates conflict” (N12)
Others hesitated due to fear of conflict, loyalty, or hierarchical pressures: “It’s not easy… you can’t disclose if the person in charge hasn’t said anything” (N13)
These tensions illustrate the complex interplay between professional responsibility, team dynamics, and moral distress.
Systemic and contextual constraints
Participants emphasized that ethical dilemmas were not only individual but also deeply shaped by structural and contextual constraints. “We prioritize according to the severity of the patients” (N2)
In some cases, economic considerations influenced access to treatment, raising concerns about equity: “We give the treatment to the poorest first” (N5)
These situations generated feelings of injustice, frustration, and moral burden: “It’s unfair to have to choose… you feel guilty” (N17)
“We’re just prolonging pain… why not let the child go in peace?” (N11) Participants also reported feeling excluded from decision-making processes, despite their close relationship with patients: “We’re not part of the decision-making” (N12)
Finally, issues related to “The rooms are often overcrowded, which makes it difficult to have private conversations” (N8)
These structural limitations reinforced nurses’ sense of powerlessness and contributed to the ethical complexity of their daily practice.
Discussion
Pediatric oncology is a complex field where ethical dilemmas are deeply embedded in everyday clinical practice. While these dilemmas have been widely documented in international literature, they remain insufficiently explored in the Moroccan context, where nursing research is still emerging. In this study, using an interpretative phenomenological approach, we sought to understand how nurses experience and make sense of these dilemmas in their daily practice.
The analysis highlights four major dimensions: ethical tensions in communication and decision-making, pain and care practices, professional integrity and safety, and the impact of structural constraints on ethical practice.
Ethical tensions in communication and decision-making
The findings reveal that communication-related dilemmas are central to nurses’ experiences, particularly in relation to truth-telling, informed consent, and treatment refusal. Nurses are frequently positioned at the intersection of competing ethical principles: respect for autonomy, beneficence, and non-maleficence.
Consistent with previous studies, 16 participants described the difficulty of balancing the child’s right to information with the need to protect them from psychological harm. However, our findings go further by highlighting the mediating role of nurses, who often become the primary interlocutors for families while lacking decision-making authority. This creates a form of ethical vulnerability, where nurses feel both responsible and powerless.
The issue of informed consent further illustrates this tension. In the Moroccan context, structural factors such as limited health literacy and communication practices contribute to a form of “symbolic consent,” where formal procedures do not necessarily ensure true understanding. This challenges the ethical principle of autonomy and places nurses in a morally uncomfortable position, as also reported by McLennon et al. 12
Treatment refusal—whether from the child or the parents—intensifies these dilemmas. Nurses oscillate between persuasion, respect, and, in some cases, coercion, reflecting a tension between protecting the child and respecting family authority. While similar findings have been reported in the literature, 17 our study highlights the limited involvement of nurses in decision-making in the Moroccan setting, which amplifies their frustration and sense of powerlessness.
Pain and care practices
A key contribution of this study lies in the identification of a profound ethical tension related to the experience of causing harm while providing care. Nurses described invasive procedures and pain management as situations where they are required to inflict suffering for therapeutic benefit.
This paradox—“causing pain to relieve suffering”—is a central source of moral discomfort. While participants often rationalized these actions in terms of medical necessity, they simultaneously reported feelings of guilt, particularly when procedures were repeated or when the child’s distress was intense. This finding echoes existing literature on procedural pain in pediatric oncology but adds an experiential dimension, emphasizing the emotional burden carried by nurses.
Moreover, systemic factors such as inadequate pain assessment, limited access to analgesics, and morphinophobia among physicians exacerbate this dilemma. As highlighted by Flowers & Birnie, 8 effective procedural preparation and pain management are considered a standard of care in pediatric oncology. However, our findings suggest a gap between recommendations and practice, which intensifies nurses’ moral distress and reinforces their sense of professional inadequacy. 8
Professional integrity and safety
Medication errors represent another significant source of ethical tension, revealing the interplay between individual responsibility and systemic constraints. Participants expressed a strong sense of accountability and a commitment to patient safety, consistent with previous studies.18–20 However, they also highlighted the role of workload and organizational factors in the occurrence of errors.
Beyond the technical dimension, our findings underscore the emotional and moral impact of errors, particularly in a pediatric context. Feelings of guilt, anxiety, and self-blame were frequently reported, illustrating the concept of moral distress, where nurses are unable to act according to their ethical values due to external constraints.
Witnessing colleagues’ errors further complicates this dynamic. Nurses must navigate between loyalty to their peers and their duty to protect the patient, leading to ethical conflicts that are not purely individual but relational and organizational. This highlights the need for supportive institutional cultures that promote transparency and shared responsibility.
Systemic and contextual constraints
Finally, this study emphasizes that ethical dilemmas are not solely the result of individual decision-making but are deeply shaped by structural and contextual constraints. Resource limitations, organizational shortcomings, and socio-economic inequalities significantly influence ethical practice.
Resource allocation emerged as a major concern, particularly in a context where financial constraints directly affect access to care. Nurses are often required to prioritize patients, leading to experiences of moral tension, injustice, and emotional burden. These findings resonate with existing literature,16,21 while illustrating the lived and emotional dimensions of such decisions in resource-limited settings.
End-of-life care represents another area where structural and relational factors intersect. The persistence of treatments perceived as futile, often driven by family expectations or institutional norms, generates significant moral distress among nurses. Participants expressed a desire to prioritize comfort over aggressive interventions, yet their limited involvement in decision-making processes intensifies their sense of frustration and ethical tension, as also reported in previous studies.13,22,23
Issues related to confidentiality and privacy further reflect the influence of organizational constraints. Overcrowding, lack of infrastructure, and cultural perceptions limit the ability to ensure confidentiality, challenging ethical standards and reinforcing nurses’ sense of powerlessness. These findings echo prior research,21,24 while underlining the importance of context-sensitive approaches to ethical practice. 25
Limitations
Despite the relevance of these findings, several limitations should be acknowledged. First, the qualitative design does not allow for generalization to all Moroccan nurses. In addition, voluntary participation may have introduced selection bias, as nurses more sensitive to ethical issues may have been more inclined to participate. Furthermore, participants’ varying levels of familiarity with the concept of ethical dilemmas may have influenced how their experiences were articulated. The use of a semi-structured interview guide helped to provide direction while preserving the exploration of lived experiences; however, a more open-ended approach might have allowed for the emergence of additional nuanced perspectives.
Conclusion
Ethical dilemmas in pediatric oncology represent a central and unavoidable dimension of nurses’ daily practice, with significant implications not only for their psychological well-being but also for the quality and ethical integrity of care provided to children. Through an interpretative phenomenological approach, this study offers a deeper understanding of how these dilemmas are experienced, highlighting the complex interplay between communication challenges, decision-making tensions, the experience of causing harm, professional responsibility, and structural constraints.
While the types of dilemmas identified are consistent with those reported in the literature, this study brings forward important contextual insights, particularly regarding the Moroccan healthcare setting. It underscores the pivotal yet often under-recognized role of nurses, who operate at the intersection of children, families, and physicians, while remaining insufficiently involved in therapeutic decision-making processes. This limited involvement contributes to feelings of powerlessness and intensifies moral distress.
The findings also point to the importance of adopting a more explicit children’s rights perspective in pediatric oncology care. Recognizing children as active participants in their care—according to their developmental capacities—could help address ethical tensions related to truth-telling, consent, and end-of-life decisions, while promoting more respectful and person-centered practices.
From a practical standpoint, several avenues for improvement emerge. Integrating ethical reflection and the management of ethical dilemmas into both initial and continuing nursing education appears essential. In addition, fostering interdisciplinary communication, promoting the inclusion of nurses in decision-making processes, and strengthening competencies in pain management are key priorities. Addressing structural challenges—such as resource limitations, organizational constraints, and inequalities in access to care—is also crucial to reducing ethically problematic situations.
Finally, given the extent of moral distress expressed by participants, future research could aim to further explore and quantify this phenomenon, as well as to evaluate interventions designed to support nurses in coping with ethical challenges. Such efforts are essential not only to improve nurses’ well-being, but also to enhance the overall quality and humanity of care provided to children with cancer.
Footnotes
Acknowledgments
The authors have no acknowledgments to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The dataset is not publicly available due to the sensitive nature of the data.