
Abstract
Background
Obstetric violence is a significant ethical and human rights concern in maternity care that undermines women’s dignity, autonomy, and respectful care during childbirth. Although women’s experiences of mistreatment are widely documented, less attention has focused on factors that enable midwives to prevent obstetric violence and provide respectful maternity care, particularly in low-resource settings.
Research aim
This study explored midwives’ perspectives on facilitators of respectful maternity care for the prevention of obstetric violence in maternity centres in South-West Nigeria.
Research design
A qualitative descriptive design was adopted, and data were analysed using Braun and Clarke’s reflexive thematic analysis.
Participants and research context
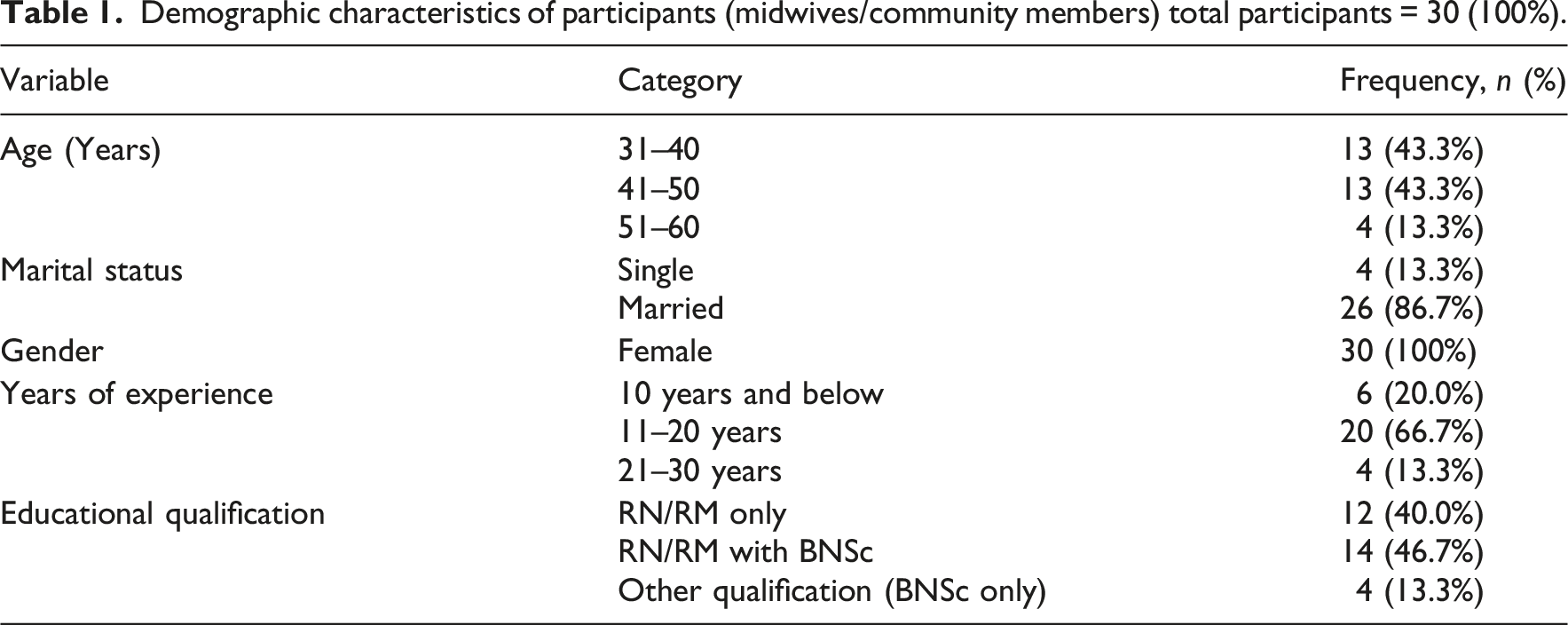
Thirty registered midwives with at least 5 years of maternity care experience participated in three focus group discussions conducted in three state-owned secondary health facilities in Oyo State, South-West Nigeria.
Ethical considerations
Ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee and the Oyo State Ministry of Health Research Ethics Review Committee. Written informed consent was obtained from all participants.
Findings/results
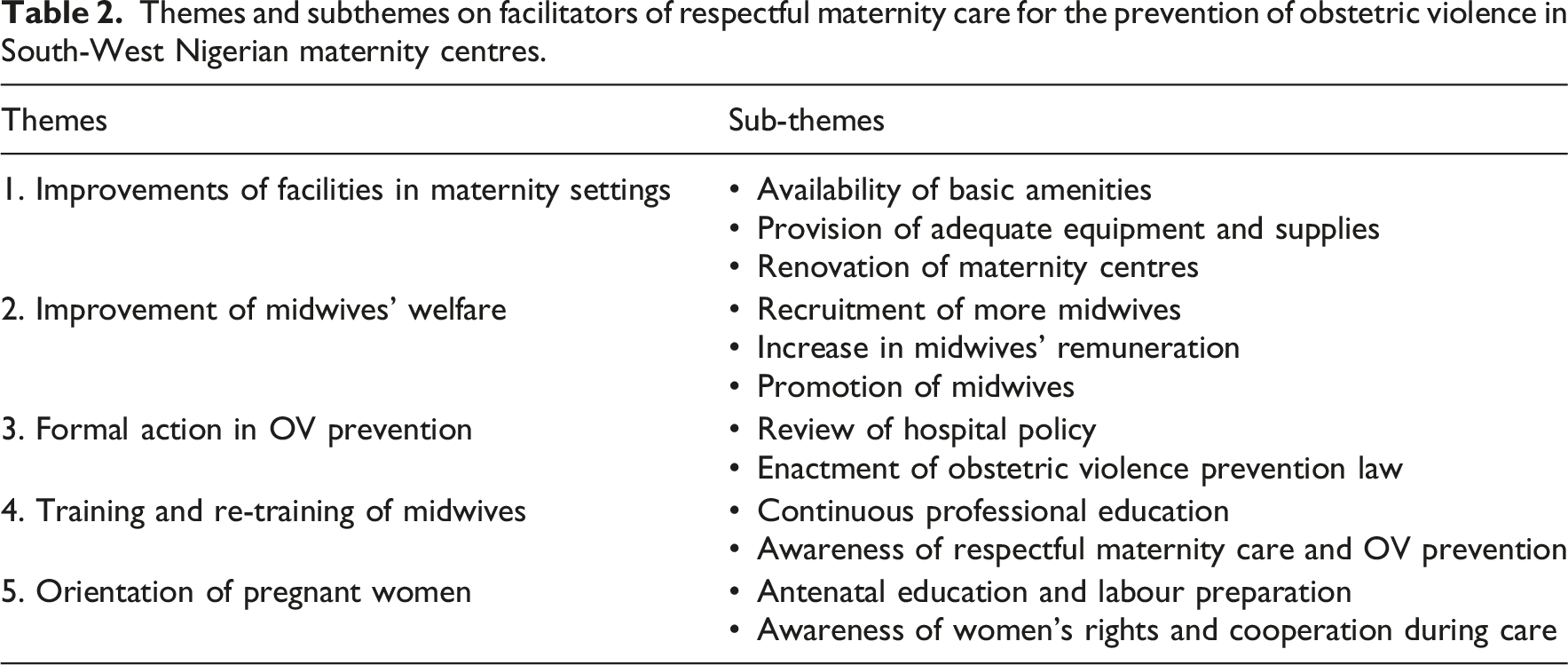
Five themes were identified as facilitators of respectful maternity care and obstetric violence prevention: improvements in maternity facilities; improvement of midwives’ welfare; formal institutional and legal actions; training and re-training of midwives; and orientation of pregnant women. Midwives described how supportive infrastructure, staffing, remuneration, institutional policies, legal accountability, continuous professional education, and women’s awareness contribute to respectful and ethical maternity care practices.
Conclusions
Preventing obstetric violence requires supportive health systems that strengthen midwives’ capacity to provide dignified and respectful maternity care. Addressing structural, institutional, legal, and educational facilitators is essential for promoting ethical childbirth care and protecting women’s rights.
Keywords
Introduction
Respectful maternity care (RMC) is a fundamental ethical obligation in nursing and midwifery practice, grounded in the principles of dignity, autonomy, beneficence, non-maleficence, justice, and respect for human rights. RMC encompasses compassionate communication, informed consent, privacy, and women’s meaningful participation in decision-making throughout pregnancy, childbirth, and the postpartum period. The White Ribbon Alliance Charter on Respectful Maternity Care further recognises respectful childbirth as a universal human right and emphasises women’s entitlement to dignified, confidential, and non-discriminatory care throughout maternity services. 1 In contrast, obstetric violence, including verbal abuse, neglect, coercion, non-consented care, discrimination, and violations of privacy, constitutes a serious ethical breach that undermines women’s reproductive rights and professional nursing values. 2
This study explores the facilitators to respectful maternity care and explores how these factors may contribute to the prevention of obstetric violence from the perspectives of practising midwives in South-West Nigerian maternity centres.
Background
The concept of obstetric violence has gained increasing international attention following foundational work of Bowser and Hill. 3 , who identified multiple forms of disrespect and abuse experienced by women during childbirth, including physical abuse, non-consented care, non-confidential care, discrimination, abandonment, and detention in facilities. Subsequent global evidence has demonstrated that mistreatment during childbirth occurs across diverse healthcare systems and socioeconomic settings. 4 Recent qualitative and integrative reviews show that maternity care providers may witness or engage in practices that compromise women’s dignity, frequently rationalized by clinical urgency, resource scarcity, or entrenched routines.5,6 From a nursing ethics perspective, these patterns reflect systemic moral shortcomings rather than individual ethical failures alone.
In low- and middle-income countries, particularly within sub-Saharan Africa, ethical challenges surrounding obstetric violence are further intensified by structural constraints such as inadequate infrastructure, staffing shortages, limited material resources, and weak accountability mechanisms. Empirical studies from African maternity settings consistently show that overcrowded wards, lack of privacy, and excessive workloads create conditions in which disrespectful care becomes normalized.7,8 Such environments raise critical ethical concerns related to justice and equity, while also contributing to moral distress among midwives who are unable to consistently practice in accordance with professional standards.
Midwives occupy a central ethical position in maternity care as primary caregivers during labour and childbirth and as major advocates for women’s rights. Evidence indicates that midwives generally recognize the importance of respectful maternity care and ethical practice; however, their capacity to uphold these values is shaped by institutional policies, working conditions, access to training, and legal protections. 9 The International Confederation of Midwives (ICM) competencies for midwifery practice emphasise that respectful, woman-centred, and rights-based care constitutes a core professional responsibility of midwives globally. 10 Similarly, the World Health Organization (WHO) standards for improving maternal and newborn care identify effective communication, dignity, emotional support, and respectful care as essential components of quality maternity services. 11 Contemporary nursing ethics scholarship therefore increasingly calls for attention not only to acts of mistreatment, but also to the institutional and systemic conditions that enable ethical and respectful maternity care practices.
Within the Nigerian context, challenges such as high patient volume, resource limitations, workforce shortages, and inconsistent institutional policies may further complicate efforts to provide respectful and ethically grounded maternity care. Although studies in Nigeria have documented women’s experiences of disrespectful care and barriers to maternal health service utilisation, considerably less attention has been paid to the perspectives of midwives regarding factors that facilitate respectful maternity care and prevent obstetric violence. This gap is ethically significant because professional conduct is shaped not only by individual attitudes but also by organisational structures, health system support, and governance frameworks. 5
Nursing Ethics emphasises moral agency, social justice, and the conditions that support ethical nursing practice. Examining facilitators of respectful maternity care therefore offers a constructive and ethically grounded approach that moves beyond attributing blame to individual providers and instead highlights the systemic and organisational conditions necessary for ethical maternity care. Focusing on facilitators shifts the discourse toward shared responsibility and health system reform, highlighting how healthcare institutions can support midwives to practice in ways that uphold dignity, justice, and professional integrity. 12
Research aim
Therefore, this study explored midwives’ perspectives on the facilitators of respectful maternity care to prevent obstetric violence in maternity centres in South-West Nigeria.
Methods
Study design
This study adopted a qualitative descriptive design to explore midwives’ perspectives on facilitators of respectful maternity care and the prevention of obstetric violence in South-West Nigeria. A qualitative descriptive approach is appropriate for obtaining rich, practice-oriented accounts of participants’ experiences and professional insights without imposing pre-existing theoretical interpretations. 13 This design was considered suitable because the study aimed to provide a comprehensive description of institutional, professional, and contextual factors that support respectful maternity care within real-world maternity settings. The study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) to enhance transparency, rigour, and ethical accountability throughout the research process.
Study setting
The study was conducted in three state-owned secondary health facilities located in Oyo State, South-West Nigeria. Each facility is situated in an urban centre and provides maternity services to a diverse population of pregnant women. These settings were purposively selected due to their accessibility, patient volume, and role in maternal healthcare delivery, allowing for a broad exploration of midwives’ experiences across different institutional contexts. The selected facilities also represented busy maternity environments where midwives routinely managed labour and childbirth care, thereby providing information-rich contexts for exploring facilitators of respectful maternity care and obstetric violence prevention.
Participants and recruitment
Participants comprised 30 registered midwives employed in the maternity units of the three selected hospitals, with ten midwives recruited from each facility using purposive sampling. Eligibility criteria included registration with the Nursing and Midwifery Council of Nigeria and a minimum of 5 years’ experience in maternity care, ensuring participants had sufficient professional exposure to respectful maternity care and obstetric violence prevention practices.
The decision to recruit ten participants per focus group was guided by recommendations for focus group research, which suggest that groups of 6–10 participants are adequate for generating diverse perspectives while still allowing meaningful interaction and manageability of discussion dynamics. 14 Recruitment continued until sufficient informational depth and thematic redundancy were achieved across the three focus groups.
Midwives currently undergoing disciplinary proceedings related to professional misconduct were excluded to minimise ethical sensitivity and potential distress during group discussions. This exclusion criterion was determined through consultation with nursing unit managers and confirmation during participant recruitment to ensure consistency in participant selection.
Recruitment was facilitated through the Chief Nursing Officers of the respective hospitals. Eligible midwives received an information sheet detailing the study aims and procedures and were given the opportunity to ask questions. Written informed consent was obtained prior to participation.
Data collection
Data were collected between February and April 2022 through three focus group discussions (FGDs), one conducted in each hospital, with ten participants per group. FGDs were chosen to encourage interaction and shared reflection among midwives on institutional practices and professional experiences. Discussions were conducted in English, Nigeria’s official language and the working language of all participants.
Each session lasted approximately 45–60 min and took place in a private room within the hospital to ensure confidentiality and minimise interruptions. Although the duration of the discussions was relatively moderate, participants were highly experienced midwives familiar with the study topic, and the focused nature of the discussion guide enabled rich and detailed exploration of the issues within the available time.
A semi-structured FGD guide with open-ended questions was used to explore facilitators of respectful maternity care and obstetric violence prevention. The guide was refined following a pilot FGD conducted in a non-participating hospital. The pilot process helped improve clarity, sequencing, and wording of selected questions, while also confirming the appropriateness of the discussion prompts for eliciting detailed participant responses.
Discussions were facilitated by the primary researcher, supported by a trained note-taker who documented non-verbal cues, group dynamics, and contextual observations. During the FGDs, participants were encouraged to interact freely, respond to one another’s comments, and elaborate on shared experiences to enhance the depth and richness of the data generated. All FGDs were audio-recorded with participants’ consent, and detailed field notes were maintained.
Data analysis
Data were analysed using Braun and Clarke’s reflexive thematic analysis approach, which is methodologically consistent with qualitative descriptive research and suitable for analysing focus group data 15 . Audio recordings were transcribed verbatim within 24–48 h of each discussion to preserve contextual accuracy.
The researcher engaged in repeated reading of transcripts and field notes to achieve familiarity and immersion in the data. Initial codes were then generated inductively by identifying meaningful segments of text related to facilitators of respectful maternity care and prevention of obstetric violence. Coding was conducted manually and included attention to both individual participant accounts and interactional dynamics within the focus groups, such as agreement, shared concerns, and collective emphasis on institutional issues.
Codes with conceptual similarities were subsequently grouped into preliminary categories, which were reviewed and refined into broader themes and sub-themes through iterative comparison across transcripts. Themes were continuously reviewed against the original dataset to ensure they accurately reflected participants’ perspectives and the overall context of the discussions.
To enhance analytic rigour, emerging themes and interpretations were discussed with the research supervisor to minimise subjective bias and strengthen consistency in coding and theme development. Member checking was conducted with six participants selected across the three facilities, who reviewed summaries of the preliminary findings and confirmed that the themes reflected their experiences and perspectives. Minor clarifications relating to wording and interpretation were incorporated following participant feedback.
Trustworthiness
Trustworthiness was ensured using Lincoln and Guba’s criteria of credibility, transferability, dependability, and confirmability. 16 Credibility was supported through prolonged engagement during FGDs, member checking, and reflexive practice. Transferability was enhanced by providing rich descriptions of the study context and participant characteristics. Dependability was addressed through consistent data collection procedures and documentation of analytic decisions. Confirmability was maintained through reflexive journaling, audit trails, and supervisory review. Participant anonymity and confidentiality were preserved by assigning pseudonyms and using generic identifiers for study sites.
Researcher reflexivity
The primary researcher is a nurse/midwife scholar with professional and research interest in maternal health, respectful maternity care, and nursing ethics. The researcher’s clinical background provided familiarity with maternity care practices and sensitivity to issues surrounding obstetric violence and respectful care. Recognising that prior professional experiences and assumptions could influence data interpretation, reflexive journaling was maintained throughout data collection and analysis to critically examine personal perspectives, assumptions, and potential biases. Regular discussions with the research supervisor also supported reflexive engagement and analytic transparency throughout the study.
Ethical considerations
Ethical approval was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (Approval Number: BREC/00003411/2021) and the Oyo State Ministry of Health Research Ethics Review Committee (Approval Number: AD13/479/44134B). Written informed consent was obtained from all participants, and they were informed of their right to decline participation or withdraw at any point without penalty. Confidentiality and privacy were strictly maintained, and all data were securely stored and accessible only to the research team.
Results
Demographic characteristics of participants (midwives/community members) total participants = 30 (100%).
Themes and subthemes on facilitators of respectful maternity care for the prevention of obstetric violence in South-West Nigerian maternity centres.
Theme 1: Improvements of facilities in maternity settings as a facilitator to OV prevention
This theme comprised three sub-themes: availability of basic amenities, provision of adequate equipment and supplies, and renovation of maternity centres.
Sub-theme 1: Availability of basic amenities
Participants described how the presence of basic amenities such as electricity, water, lighting, and ventilation made the working environment more conducive and enabled calm, respectful interactions with women during labour. Midwives reported that adequate amenities reduced stress and improved their ability to provide care without resorting to shouting or negative reactions. “…another thing is the provision of amenities like a constant supply of electricity, especially at night. This will make work easier, especially for the nurse, and make the patient receive adequate care. The environment will be conducive, and the midwives will not be shouting at pregnant women” (Foluso, P010, FGD 1, 37 years, 15 years of work experience). “Creating a good working condition is a facilitator to OV prevention; for example, there should be the provision of adequate lighting, especially at night, and there should be the provision of water and other necessary things that make working by the midwives conducive. Even if the patients provoke us, if the working condition is okay, we won’t react negatively as midwives.” (Rebecca, P007, FGD 2, 31 years, 8 years of work experience). “We need light at all times. There should be adequate supply of water to work with. When there is electricity, the fan can blow and the environment will be cool and conducive to work, especially in the dry season when everything is hot.” (Gabriella, P004, FGD 1, 48 years, 18 years of work experience).
Sub-theme 2: Provision of adequate equipment and supplies
Midwives reported that the availability of essential equipment and emergency drugs enabled them to perform their duties effectively and reduced frustration during care provision. Participants emphasized that adequate supplies supported quality care delivery and reduced the likelihood of aggressive responses toward patients. “…there must be the provision of enough equipment to carry out our duty so that we will not be aggressive to patients. To provide quality care, we need equipment to work with.” (Abibat, P006, FGD 2, 37 years, 11 years of work experience). “I think the government should make provision for emergency drugs. Some things are needed that will not be available on the ward; that should not be. There should be the provision of emergency drugs.” (Caroline, P008, FGD 1, 45 years, 18 years of work experience). “Provision of amenities and equipment needed is important because it makes the work to be easier.” (Faith, P002, FGD 1, 47 years, 16 years of work experience).
Sub-theme 3: Renovation of maternity centres
Participants described how overcrowded wards and lack of demarcation limited privacy and confidentiality, which affected women’s cooperation during care. Midwives emphasized that renovation, expansion, and structural improvements would enable confidential interactions and enhance respectful care. “Provision of adequate maternity building and facilities for patients to enhance privacy so that confidential care can be given to patients is a factor that can facilitate the prevention of OV.” (Eugena, P001, FGD 3, 35 years, 10 years of work experience). “The labour ward that is not demarcated by the hospital should also be worked on to provide privacy and confidential care to patients.” (Clara, P008, FGD 2, 34 years, 7 years of work experience). “There can be an extension of the maternity centre to accommodate other needed units, for example isolation or septic wards.” (Racheal, P001, FGD 1, 38 years, 10 years of work experience). “…curtains can be provided to provide privacy for patients in open wards so that there will be confidentiality and they too will feel that midwives are keeping their privacy.” (Susan, P004, FGD 3, 45 years, 12 years of work experience).
Theme 2: Improvement of midwives’ welfare as a facilitator to OV prevention
Participants described improvement in midwives’ welfare as an important facilitator of respectful maternity care and obstetric violence prevention. Midwives emphasized that welfare-related factors influenced their emotional wellbeing, motivation, and capacity to interact calmly and respectfully with women during maternity care. Three sub-themes emerged under this theme: recruitment of more midwives, increase in midwives’ remuneration, and promotion of midwives.
Sub-theme 1: Recruitment of more midwives as a facilitator to OV prevention
Participants consistently reported that the recruitment of more midwives reduced workload, physical exhaustion, and emotional strain during service delivery. Midwives explained that adequate staffing allowed them to perform their duties effectively and reduced the likelihood of transferring work-related stress or aggression to patients. “There is a need to recruit competent midwives in taking care of patients because if we have enough qualified midwives on the duty, we will not be transferring aggression of too much workload to the patients.” (Caroline, P008, FGD 1, 45 years, 18 years of work experience). Adjusting her seat. “Government should recruit more midwives to relieve the workload. This will lessen the work done by the midwives and there will not be transfer of aggression to the patients by the midwives.”(Feyisara, P005, FGD 2, 41 years, 14 years of work experience). “Also, there is need to employ enough midwives to relieve work burdens related to increased workload that may lead to OV.”(Rebecca, P007, FGD 2, 31 years, 8 years of work experience). “Employment of more midwives is needed to help reduce workload that can serve as an obstacle to OV. This is because when there are enough midwives on duty, the cases of OV will be reduced.” (Linda, P004, FGD 2, 40 years, 16 years of work experience).
Sub-theme 2: Increase in midwives’ remuneration as a facilitator to OV prevention
Participants described adequate and timely remuneration as an important factor that enhanced motivation, job satisfaction, and positive attitudes toward patient care. Midwives indicated that fair compensation encouraged them to remain committed to their roles and engage more positively with women during childbirth. “There should be remuneration for a job well done to the midwives. Increased remuneration is a way of motivating and encouraging midwives to do more for their patients.” (Oluwatoyin, P007, FGD 1, 51 years, 29 years of work experience). “Correct remuneration for the midwives as and when due will be a motivational factor for the midwives to do more and help prevent OV.” (Foluso, P010, FGD 1, 37 years, 15 years of work experience).
Sub-theme 3: Promotion of midwives as a facilitator to OV prevention
Participants emphasized that promotion and recognition were closely linked to morale, professional fulfilment, and workplace satisfaction. Midwives reported that delayed or missed promotions contributed to frustration, whereas timely promotion encouraged commitment and positive interactions with patients. “Correct remuneration for the midwives and promotion of midwives as and when due will be a motivational factor for the midwives to do more and will help prevent OV.” (Foluso, P010, FGD 1, 37 years, 15 years of work experience). “The management needs to promote us as and when due. This can facilitate OV prevention; we will be happy to work, and things can go on smoothly at work even with our patients.” (Salome, P005, FGD 3, 33 years, 11 years of work experience). “We desire to be promoted and recognised in our workplace. Many of us are due for promotion, and that has not been done. It can be frustrating leading to OV unknowingly, but if our promotion is done, it will encourage us and we can be motivated to prevent OV.” (Antoniette, P003, 44 years, 19 years of work experience).
Theme 3: Formal action in OV prevention as a facilitator of OV prevention
Participants described formal institutional and legal actions as important facilitators of obstetric violence prevention in maternity settings. Midwives emphasized that clear policies and enforceable laws influenced professional conduct and guided respectful maternity care practices. Two sub-themes emerged under this theme: review of hospital policy and enactment of obstetric violence prevention laws.
Sub-theme 1: Review of hospital policy as a facilitator to OV prevention
Participants reported that certain existing hospital policies contributed to practices perceived as obstetric violence, particularly policies related to the detainment of women unable to pay medical bills. Midwives emphasized the need for policy review to address financial barriers, improve access to essential resources, and support respectful care practices. “Good hospital policy should be put in place to put in place things needed to prevent OV like availability of equipment and things to be used in the hospital. When all of these are put in place, it will be possible to prevent OV.” (Rachabel, P006, FGD 1, 41 years, 20 years of work experience). “There should be a review of the institutional policy to identify the aspects that can be improved. Institutional policy that states that women should be detained if unable to pay up for medical bills should be investigated.” (Clara, P008, FGD 2, 34 years, 7 years of work experience). “The hospital policy can be reviewed about how to source funds to prevent detainment of patients that are unable to pay and essentials of what can be used for them in case of emergency. When this is done, and there are enough funds, it can be made accessible for those that need it.” (Reminiscence, P003, FGD 3, 36 years, 11 years of work experience).
Sub-theme 2: Enactment of obstetric violence prevention law as a facilitator to OV prevention
Participants consistently emphasized the absence of formal legal frameworks regulating obstetric violence and described the enactment of specific laws as necessary for accountability and behaviour regulation. Midwives reported that legal backing would deter abusive practices and reinforce adherence to respectful maternity care standards. “I am recommending putting rules and regulations including adding the legislative aspect on preventing the act of OV. Once people are aware, there will be an improvement as regards OV prevention.” (Olorunyomi, P007, FGD 3, 35 years, 13 years of work experience). “…midwives tend to do what they like when there is no law to put them in check. Therefore, there is a need for obstetric violence prevention law to prevent OV.” (Oluwatoyin, P007, FGD 1, 51 years, 29 years of work experience). “When there is no formal law backing up the prevention of OV, people can do anything and go away with it.” (Abibat, P006, FGD 2, 37 years, 11 years of work experience). “If truly we want to facilitate the prevention of OV, let there be a law on it and ensure that anyone found guilty will be punished according to the law.” (Agness, P001, FGD 2, 38 years, 15 years of work experience). “To regulate something in our society, the law has been seen to help. Therefore, I think putting laws on OV prevention in place should be done and enforced. Once people know there is a law on that and that they can be punished if they are caught, things will change in the war we are putting against OV.” (Mattah, P003, FGD 1, 36 years, 8 years of work experience).
Theme 4: Training and re-training of midwives as a facilitator to OV prevention
This theme comprised two sub-themes: continuous professional education and awareness of respectful maternity care and obstetric violence prevention.
Sub-theme 1: Continuous professional education
Participants described training and re-training as essential to improving midwives’ knowledge, awareness, and professional conduct in relation to obstetric violence prevention. Midwives emphasized the need for continuous education to keep them informed about respectful maternity care practices and evolving professional standards.
Participants reported that ongoing training, in-service education, seminars, and conferences enhanced their understanding of obstetric violence and reinforced appropriate care practices. Midwives described training as a means of updating knowledge, improving skills, and maintaining awareness of respectful maternity care standards. “There should be more training and retraining for midwives on preventing OV. This will enhance updating the midwife’s knowledge and skills and the issues of OV prevention.” (Feyisara, P005, FGD 2, 41 years, 14 years of work experience). “Continuous education is needed for the midwives to keep updating them. There should be frequent seminars about OV and its prevention.” (Abibat, P006, FGD 2, 37 years, 11 years of work experience). “To facilitate OV prevention, I think government and hospital management should sponsor midwives to attend conferences and seminars where they can learn about OV and its prevention.” (Bamidele, P005, FGD 1, 55 years, 23 years of work experience).
Sub-theme 2: Awareness of respectful maternity care and OV prevention
Participants further emphasized that training was important for improving awareness of behaviours and practices that constitute obstetric violence beyond obvious forms such as verbal and physical abuse. Midwives described the need for reflective learning that would continually remind healthcare professionals about respectful maternity care principles and ethical conduct during childbirth care. “Midwives should be trained and for them to be aware of what constitutes OV, and its prevention is another factor that can facilitate the prevention of OV. There should be increased awareness about other practices that constitute OV among midwives and not just focusing on verbal and physical abuse alone.” (Eugenia, P008, FGD 3, 49 years, 20 years of work experience). “Training will go a long way to keep reminding midwives and other healthcare professionals of practices that constitute OV and how to prevent it.” (Salome, P005, FGD 3, 33 years, 11 years of work experience).
Theme 5: Orientation of pregnant women as a facilitator to OV prevention
This theme comprised two sub-themes: antenatal education and labour preparation, and awareness of women’s rights and cooperation during care.
Participants described the orientation of pregnant women as an important aspect of respectful maternity care and obstetric violence prevention. Midwives emphasized that adequate antenatal education prepared women for labour and childbirth, reduced misunderstandings during care, and supported cooperation between women and care providers.
Sub-theme 1: Antenatal education and labour preparation
Participants reported that consistent antenatal education and orientation helped pregnant women understand what to expect during labour and what was expected of them during maternity care. Midwives described the need for repeated health education at each clinic visit, particularly on labour processes, communication, and preparation for childbirth. “Though the midwives in antenatal clinic educate pregnant women, they should intensify more on health education of what patients will expect on the ward and what the midwives will expect from them because, at times when you are telling them to do something, for instance at the verge of delivery when the cervix is not fully dilated, teaching them to be panting, some will tell you that they don’t know it. When you ask them to be panting, they will tell you ‘Ki lo n je baun,’ meaning what is the meaning of what you are saying? The health education should be intensified and should be re-emphasized at each visit.” (Foluso, P010, FGD 1, 37 years, 15 years of work experience). “Adequate information or orientation should be given to pregnant women right from the antenatal period so that they will understand what they are to experience during labour.” (Tolulope, P002, FGD 2, 39 years, 14 years of work experience). “Pregnant women should be enlightened on what to expect, especially the underage, during labour, delivery, and postpartum period. The signs and stages of labour should be explained to them, and what pregnant women should do during pregnancy and childbirth. This will make them cooperate with the midwives.” (Faderera, P010, FGD 3, 43 years, 18 years of work experience).
Sub-theme 2: Awareness of Women’s rights and cooperation during care
Participants also emphasized the importance of educating women about respectful maternity care, their rights during childbirth, and the need for effective communication and cooperation between women and midwives. Midwives perceived that informed women were more likely to participate actively in care processes and advocate for respectful treatment during childbirth. “Women should be informed about what constitutes OV and know about their rights by educating them so that they can insist on their rights.” (Eugenia, P008, FGD 3, 49 years, 20 years of work experience). “Pregnant women’s cooperation is essential. So, pregnant women should be encouraged to work together and cooperate with the midwives at all times.” (Victoria, P002, FGD 3, 33 years, 9 years of work experience).
Discussion
This study explored midwives’ perspectives on facilitators of respectful maternity care and the prevention of obstetric violence in South-West Nigerian maternity centres. Collectively, the findings suggest that respectful maternity care is not solely dependent on individual midwives’ behaviour or professional intentions, but is strongly shaped by institutional conditions, organisational support, legal frameworks, and health system responsiveness. The study therefore highlights obstetric violence as both an ethical and structural concern, requiring interventions that support midwives’ moral agency and ability to practice in ways consistent with professional nursing and midwifery value.
This current study found that the availability of basic amenities such as constant electricity, water supply, ventilation, and adequate lighting facilitates respectful maternity care and prevents obstetric violence. Midwives explained that a conducive working environment reduces stress, improves comfort, and enables them to provide calm and supportive care, even in challenging situations. This suggests that basic amenities help regulate provider emotions and interactions, thereby reducing tendencies toward shouting or negative reactions. Similar studies report that functional amenities promote dignity, reduce tension in labour wards, and support respectful communication between providers and women.9,17 From an ethical perspective, these findings demonstrate how structural inadequacies can constrain compassionate care and undermine midwives’ capacity to uphold women’s dignity, privacy, and emotional wellbeing during childbirth. This aligns with the World Health Organization (WHO) Standards for Improving Quality of Maternal and Newborn Care in Health Facilities, which recognise a safe, supportive, and respectful care environment as fundamental to women’s rights and quality maternity care. 11
The findings revealed that the provision of adequate equipment and supplies, including emergency drugs and essential delivery tools, facilitates the prevention of obstetric violence by enabling midwives to provide timely and quality care. Participants indicated that when necessary materials are readily available, care becomes easier and less frustrating, reducing the likelihood of aggressive or rushed interactions. This implies that material readiness supports respectful maternity care by allowing midwives to focus on clinical and emotional support rather than improvisation. Consistent evidences from Ghana and Rwanda shows that well-equipped maternity units enhance respectful practices and reduce neglect and mistreatment during childbirth.7,18 The findings further suggest that respectful maternity care cannot be separated from broader questions of distributive justice and health system investment. Where essential resources are lacking, midwives may experience frustration, emotional exhaustion, and moral distress arising from the inability to provide care consistent with ethical and professional standards.
This study also demonstrated that renovation and expansion of maternity centres facilitate obstetric violence prevention by enhancing privacy, confidentiality, and organization of care spaces. Midwives noted that demarcated labour wards, curtains, and additional units reduce overcrowding and promote cooperative behaviour among women during labour. This suggests that improved physical structures foster respectful interactions and protect women’s dignity by minimizing exposure and unwanted disclosure. Supporting literature indicates that well-designed maternity spaces promote confidentiality, improve provider–woman relationships, and reduce disrespectful care practices.5,8 Within nursing ethics, privacy and confidentiality are central components of ethically grounded care. The present findings therefore reinforce the importance of healthcare environments that protect women’s bodily integrity, autonomy, and dignity during labour and childbirth.
This study found that recruitment of more midwives facilitates the prevention of obstetric violence by reducing workload and work-related stress among midwives. Participants explained that having adequate staffing prevents fatigue and frustration, thereby reducing the likelihood of transferring aggression to women during labour. This suggests that sufficient staffing enables midwives to provide individualized, calm, and respectful care even in high-pressure situations. Similar evidence from low- and middle-income settings shows that adequate staffing levels improve respectful maternity care and reduce incidents of mistreatment during childbirth.7,18 These findings are particularly important within the context of moral distress theory, which suggests that healthcare professionals may experience psychological and ethical strain when organisational constraints prevent them from providing the quality of care they believe is morally appropriate. Adequate staffing therefore not only improves service delivery but also supports midwives’ moral agency and ethical practice.
The current study findings revealed that adequate and timely remuneration serves as a facilitator to obstetric violence prevention by motivating midwives and enhancing job satisfaction. Participants noted that fair pay encourages commitment, positive attitudes, and willingness to provide compassionate care to women. This implies that financial motivation plays an important role in shaping provider behaviour and emotional responses during maternity care. Supporting literature indicates that improved remuneration is associated with increased morale, reduced burnout, and better quality of respectful maternity care.5,19 Similarly, timely promotion and professional recognition were perceived as important institutional mechanisms that reinforce workplace value, motivation, and professional fulfilment. These findings suggest that respectful maternity care is closely linked to how healthcare systems value, support, and recognise midwives themselves.
This current study also demonstrated that timely promotion and recognition of midwives facilitate obstetric violence prevention by improving motivation and workplace satisfaction. Participants explained that promotion acknowledges professional effort and reduces frustration, which in turn promotes positive interactions with women during childbirth. This suggests that career progression strengthens midwives’ sense of value and commitment to respectful maternity care. Evidence from recent studies indicates that professional recognition and supportive management practices enhance respectful care behaviours and reduce provider-related mistreatment.6,9 The International Confederation of Midwives (ICM) Essential Competencies for Midwifery Practice emphasise the importance of supportive professional environments that enable midwives to provide safe, respectful, woman-centred, and evidence-based care. 10 The present findings reinforce the argument that institutional support systems are essential for sustaining ethical maternity care practices.
This study revealed that reviewing hospital policies that inadvertently promote obstetric violence facilitates respectful maternity care and OV prevention. Midwives highlighted policies such as detainment of women unable to pay medical bills as practices that contribute to disrespect and rights violations. This suggests that policy reforms addressing financial barriers and institutional procedures can protect women’s dignity and reduce coercive practices. Evidence from recent studies indicates that unclear or punitive hospital policies contribute to normalization of obstetric violence, while rights-based institutional policies promote respectful care.2,5 Similarly, a study identified that mistreatment during childbirth is frequently driven by broader health system failures, including poor institutional conditions, inadequate staffing, and weak accountability structures rather than isolated provider behaviour alone. 20 These findings demonstrate how institutional policies may either enable or undermine ethical care practices.
The findings also showed that enactment and enforcement of obstetric violence prevention laws facilitate OV prevention by providing formal accountability mechanisms for care providers. Midwives indicated that legal backing would regulate behaviour, deter abusive practices, and promote adherence to respectful maternity care standards. This implies that laws serve as protective frameworks that reinforce professional ethics and women’s rights during childbirth. This finding further supports the foundational work of Bowser and Hill (2010), who argued that disrespect and abuse during childbirth are closely linked to structural deficiencies, institutional practices, and failures in accountability within maternity care systems. 3 Supporting literature demonstrates that legal recognition of obstetric violence strengthens accountability, shifts institutional culture, and improves respectful maternity care practices.5,12 The findings therefore support growing international calls for legal and policy frameworks that explicitly recognise respectful maternity care as a human rights and ethical issue rather than solely a clinical concern.
This study revealed that continuous training and re-training of midwives facilitates the prevention of obstetric violence by improving knowledge, awareness, and professional conduct during maternity care. Participants emphasized that regular in-service training, seminars, and conference attendance help midwives understand the full scope of practices that constitute obstetric violence beyond verbal and physical abuse. This suggests that ongoing education reinforces respectful maternity care principles and promotes reflective practice. Supporting evidence indicates that continuous professional education improves midwives’ attitudes, communication skills, and adherence to respectful care standards.21,22 Evidence further shows that sustained training fosters ethical sensitivity and reduces normalized disrespectful practices in maternity settings. 6 Continuous ethics-focused education may therefore strengthen reflective practice, ethical awareness, and midwives’ capacity to navigate complex interpersonal and institutional challenges during childbirth care.
This study revealed that proper orientation of pregnant women facilitates obstetric violence prevention by improving cooperation, communication, and mutual understanding between women and midwives during childbirth. Participants emphasized that consistent antenatal education helps women understand labour processes, expected behaviours, and clinical instructions, thereby reducing fear, confusion, and resistance during care. This suggests that informed women are better prepared to participate actively in childbirth and engage positively with care providers. Evidence indicates that adequate antenatal orientation enhances women’s confidence, promotes informed decision-making, and supports respectful maternity care practices.9,17 Additionally, studies show that educating women about their rights and what constitutes obstetric violence empowers them to advocate for respectful care and contributes to OV prevention. 2 This finding highlights the ethical importance of women’s autonomy, participation, and informed decision-making within maternity care. The White Ribbon Alliance Charter for Respectful Maternity Care recognises women’s rights to dignity, information, informed consent, privacy, and equitable care throughout childbirth, reinforcing the importance of empowering women within maternity services. 1 Respectful maternity care therefore requires not only ethically competent providers but also empowered women who are informed about their rights, care processes, and available support systems during childbirth.
Taken together, the findings of this study suggest that respectful maternity care and prevention of obstetric violence depend on interconnected structural, professional, educational, and legal facilitators. The findings move beyond explanations that locate obstetric violence solely within individual provider behaviour and instead demonstrate how healthcare systems, institutional cultures, and organisational conditions shape ethical maternity care practices. Supporting midwives through adequate resources, fair workplace conditions, continuous professional development, and rights-based institutional policies may therefore strengthen their ability to act as moral agents and provide care that upholds women’s dignity, autonomy, and reproductive rights.
Conclusion
This study demonstrates that the prevention of obstetric violence is fundamentally an ethical issue that extends beyond individual conduct to encompass institutional responsibility, professional support, and legal accountability. Facilitators identified by midwives, such as supportive infrastructure, improved welfare, policy reform, continuous education, and women’s orientation, highlight the conditions required for ethical practice in maternity care. Addressing obstetric violence therefore demands system-level interventions that enable midwives to uphold professional values of dignity, justice, and respect for persons, consistent with the ethical commitments of nursing and midwifery practice.
Recommendations
Healthcare policymakers should prioritize investment in facility upgrades and midwives’ welfare to create a supportive work environment. Regular training and re-training on respectful maternity care should be institutionalized. Government should enact and enforce laws addressing obstetric violence. Maternity centres should also intensify antenatal education to empower pregnant women. Collaboration between midwives and management is essential for sustainable change.
Limitation of the study
This study was limited to midwives working in three selected public maternity centres in Oyo State, which may not fully represent the experiences of midwives in private or rural settings. Additionally, since data were collected through focus group discussions, some participants may have withheld sensitive opinions due to social desirability bias or the presence of colleagues. The qualitative nature of the study also limits the generalizability of findings to other regions or healthcare systems.
Footnotes
Acknowledgements
The author wishes to acknowledge all the midwives who participated in the study for their time, openness, and valuable insights. Special thanks also go to the management of the selected hospitals in Oyo State for granting access and supporting the data collection process.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to ethical restrictions and the need to protect participant confidentiality but are available from the corresponding author on reasonable request.
Anonymity statement
All identifying information related to participants and study sites has been anonymised to protect confidentiality. No information that could compromise the anonymity of participants or institutions is included in this manuscript.