
Abstract
Background
Moral distress involves psychological suffering when actions conflict with personal ethical values due to institutional constraints. This distress erodes professional integrity and significantly undermines the quality of nursing work life. Addressing this conflict is essential for clinical workforce sustainability.
Aim
This study aimed to investigate the impact of moral distress on the quality of nursing work life (QNWL) among clinical nurses and to verify the serial mediating effects of compassion fatigue and resilience in this relationship.
Research design
This was a descriptive correlational study.
Participants and research context
We conducted a descriptive survey with 289 clinical nurses with at least 3 years of experience. Data were collected using the Korean version of the Moral Distress Scale-Revised (KMDS-R), the Professional Quality of Life Scale (ProQOL) for compassion fatigue, the 10-item Connor-Davidson Resilience Scale (CD-RISC-10), and the Korean version of the Quality of Nursing Work Life (K-QNWL). Data were analyzed using descriptive statistics, Pearson’s correlation coefficients, and the PROCESS macro (Model 6).
Ethical considerations
This study was approved by the institutional review board. Informed consent was obtained from participants prior to data collection.
Results
Moral distress was positively correlated with compassion fatigue and negatively correlated with resilience and QNWL. Serial multiple mediation analysis revealed that moral distress had a significant direct effect on QNWL. Furthermore, the serial mediation path of moral distress → compassion fatigue → resilience → QNWL was statistically significant (indirect effect = −0.051, 95% CI [−0.081, −0.032]). However, the simple mediation effect through resilience alone was not significant.
Conclusions
The findings demonstrate that moral distress significantly reduces the quality of nursing work life through the sequential mediation of compassion fatigue and resilience. This suggests that moral distress induces compassion fatigue, which subsequently erodes resilience and professional well-being. Organizational strategies should prioritize early intervention and integrated support systems.
Keywords
• It uniquely identifies compassion fatigue as a critical “gateway” mechanism that depletes a nurse’s internal defense system (resilience), moving beyond previous studies that primarily explored fragmented bivariate relationships. • It integrates the theoretical frameworks of Jameton and Corley into a robust statistical model, confirming that the erosion of moral integrity acts as a persistent stressor leading to emotional exhaustion.
• The findings urge healthcare organizations to shift from individual-focused resilience training to systemic ethics interventions, such as implementing “Ethical Grand Rounds” and safe consultation channels for resolving ethical dilemmas. • It highlights the practical necessity of training senior clinical staff, such as charge nurses, as “ethics first responders” equipped with screening tools to detect early signs of emotional depletion in high-risk units.What is original about this work?
What impact is the work likely to have on care practice, leadership, research and/or education?
Introduction
In the current clinical environment, nurses face unforeseen biomedical ethical issues amid rapid advances in medical technology and the expansion of patient rights. 1 These environmental changes increase the demand for improved working conditions and the management of nurses’ physical and mental well-being, highlighting the importance of systematically managing the quality of nursing work life (QNWL). QNWL refers to the degree to which registered nurses satisfy important personal needs through their work experiences while achieving the organization’s goals. 2 This is a multidimensional concept encompassing fair compensation, safe and healthy environments, development opportunities, and social integration, and it is an essential precondition for nurses’ self-actualization and professional growth.3,4
QNWL signifies the sense of accomplishment and subjective satisfaction felt during work and it is closely related to the sustainability of nursing work, turnover rates, job satisfaction, stress levels, organizational commitment, and quality of care.5,6 Despite its importance, clinical nurses’ QNWL is continuously threatened by various ethical and emotional stressors.
Background
A primary factor undermining QNWL is moral distress. As patient advocates who maintain close contact with patients, nurses constantly engage in ethical decision-making in situations where values conflict, such as between patient rights and respect for life. 3 In such cases, the ethical problems nurses face are divided into two categories. One is ethical conflicts, wherein determining the best course of action is difficult due to conflicting moral principles; the other is personal moral distress, which occurs when external constraints prevent individuals from taking what they know to be the right action.7,8 While ethical conflict stems from uncertainty in judgment, personal moral distress is characterized by emotional suffering resulting from a compromise of moral integrity. 9 When a nurse’s ethically motivated actions are systematically obstructed by institutional barriers, they experience severe emotional distress that extends beyond a baseline psychological burden, directly compromising their moral integrity. 10 Moral distress occurs when nurses clearly recognize the correct course of action but cannot execute it due to institutional structures or situational constraints. 8 This distress originates from structural constraints such as unsupportive ethical cultures, resource shortages, or conflicts between tasks and ethical standards,11,12 leading to physical and emotional burnout, decreased job satisfaction, and increased turnover intention. The experience of personal moral distress weakens a nurse’s inner identity and ethical beliefs, negatively impacting job commitment and professional performance 13 and is thus a significant factor affecting overall QNWL.
Unresolved and cumulative moral distress can lead to compassion fatigue. Compassion fatigue is a concept that encompasses both emotional exhaustion experienced during the process of helping individuals suffering from trauma or pain and the secondary traumatic stress resulting from exposure to patient suffering. 14 It is distinguished from general burnout resulting from accumulated job stress and is described as a specific form of psychological exhaustion. 15 While providing compassionate care is essential for high-quality nursing, the resulting compassion fatigue can lead to serious professional challenges, including clinical errors, diminished professional loyalty, and increased turnover intention. This type of fatigue also leads to emotional distancing, cynicism, and indifference, 16 and negatively impacts nursing practice through decreased interpersonal skills, communication barriers, and reduced organizational efficiency.17,18 This vulnerability is particularly pronounced in high-acuity settings; for instance, ICU nurses experience acute trauma and end-of-life dilemmas, while oncology nurses face a cumulative emotional toll from prolonged patient suffering and repeated loss, significantly amplifying their risk of compassion fatigue.17,19,20
The degree and consequences of personal moral distress and compassion fatigue vary depending on an individual’s psychological resources. 20 In particular, resilience has been identified as a protective quality that negatively influences moral distress while simultaneously mitigating the negative effects associated with compassion fatigue. 21 Specifically, resilience is theoretically defined as a dynamic psychological process encompassing the ability of an individual to maintain, adapt, or regain mental health and stable functioning despite experiencing significant adversity or chronic workplace stressors.22,23 Based on this protective mechanism, it can be inferred that resilience plays a crucial role in preventing ethical stressors from eroding the overall quality of nursing work life. Nurses with high resilience demonstrate the capacity to quickly recover their psychological balance and engage in constructive emotional regulation, even when facing severe emotional difficulties. 19 Furthermore, resilience is understood as a multidimensional psychological trait that goes beyond simple stress endurance to encompass emotional regulation, self-efficacy, and optimism. 24 Consequently, resilience acts as a core psychological resource that buffers the negative effects of compassion fatigue, even in complex clinical situations accompanied by moral distress.
Previous studies have mostly explored individual variables, such as the impact of moral distress on QNWL, 25 the impact of compassion fatigue on QNWL, 26 or the relationship between resilience and QNWL. 27 To integrate these fragmented relationships, this study is grounded in the theoretical frameworks of Jameton and Corley.7,28 Jameton initially conceptualized moral distress as the painful psychological imbalance that occurs when institutional constraints prevent a nurse from executing an ethically correct action. 28 Building upon this, Corley’s theory of moral distress posits that such unresolved ethical conflicts progressively erode a nurse’s moral integrity and negatively impact their professional environment. 7
Guided by these frameworks, we hypothesized a sequential cascade of psychological deterioration. Specifically, the initial erosion of moral integrity acts as a persistent stressor that manifests as severe emotional exhaustion, conceptualized here as compassion fatigue. As compassion fatigue accumulates, it gradually depletes the individual’s internal coping resources, wearing down their resilience. Ultimately, this depleted psychological state profoundly diminishes the overall quality of nursing work life.
Accordingly, the purpose of this study is to comprehensively analyze the influence of moral distress on QNWL and to verify this sequential mediation path, demonstrating how moral distress induces compassion fatigue, which subsequently erodes resilience and ultimately reduces QNWL.
Methods
Study design
This is a descriptive correlational study to investigate the relationships among clinical nurses’ moral distress, compassion fatigue, resilience, and quality of nursing work life, and to verify the mediating effects of compassion fatigue and resilience.
Participants
The participants were clinical nurses with at least 3 years of experience. According to Benner, 29 nurses reach the competent stage at approximately 2–3 years of clinical practice, demonstrating stable and skilled performance. Upon successful transition into this stage, nurses develop the capacity to perform their duties consciously and deliberately, guided by long-term goals or plans. Thus, clinical nurses with three or more years of experience were selected for this study to effectively capture variables that are fully formed through accumulated clinical experience. The inclusion criteria consisted of clinical nurses providing direct patient care who voluntarily consented to participate in the study. Nurse managers and nurses in non-hospital institutions were excluded because managers’ moral distress qualitatively differs from that of staff nurses, typically originating from administrative compromises and resource management rather than direct clinical care conflicts.26,30 In this study, charge nurses refer to senior staff nurses who perform shift-level clinical coordination alongside full direct patient care duties, holding no permanent administrative or personnel management authority unlike unit managers; thus, they were appropriately included as direct care providers. A total of 289 participants were included in the final analysis. To examine the multiple mediation effects, we employed a bootstrapping method with 5000 resamples to calculate bias-corrected confidence intervals (CIs). This approach was selected as it provides greater statistical power than traditional methods for a sample size of this magnitude and effectively addresses the non-normal distribution of indirect effects.
Instruments
General characteristics
In this study, the impact of the participants’ general characteristics on the major variables was examined through a literature review. Socio-demographic characteristics consisted of 10 items: gender, age, highest education level, marital status, total clinical career, current hospital type, work schedule, position, current department, and clinical career within the current department. These items were utilized to identify differences based on individual backgrounds and work environments and to analyze their relationships with the main variables.
The Moral Distress Scale-Revised (MDS-R)
The original Moral Distress Scale was developed by Hamric et al. 11 Later, Chae et al. 31 translated and modified it for the clinical environment of Korean nurses in 2016. The MDS-R consists of a total of 21 items across five subscales: futile care (5 items), nursing practice (5 items), institutional and situational factors (4 items), constraints on raising ethical issues (3 items), and physician practice (4 items). Each item requires responses for both the frequency of the situation from 0 (never) to 4 (very frequently) and the intensity of discomfort from 0 (= not uncomfortable at all) to 4 (very uncomfortable), evaluated on a 5-point Likert scale. The score for each item is calculated by multiplying the frequency and intensity, with total scores ranging from 0 to 336; higher scores indicate higher levels of moral distress. The Cronbach’s alpha was .91 in the study by Chae et al. 31 and .97 in the present study. Additionally, the Cronbach’s alpha coefficients for the subscales in this study were as follows: futile care .94, nursing practice .91, institutional and situational factors .84, constraints on raising ethical issues .76, and physician practice .84.
Professional Quality of Life Scale (ProQOL)
Compassion fatigue was assessed using the Korean version of the Professional Quality of Life Scale, Version 5 (ProQOL). 32 This translated instrument and its usage permission were obtained directly from the original author via the official ProQOL website (https://www.proqol.org/). The ProQOL consists of 30 items across three subscales: compassion satisfaction, burnout, and secondary traumatic stress. In this study, a total of 20 items from the burnout (10 items) and secondary traumatic stress (10 items) subscales were used to evaluate compassion fatigue. Each item is rated on a Likert scale from 1 (not at all) to 5 (very much so), with some items in the burnout subscale reverse coded. The score for each subscale ranges from 10 to 50, and compassion fatigue is calculated by summing the scores of burnout and secondary traumatic stress. Higher scores indicate greater levels of compassion fatigue. A Cronbach’s alpha coefficient of 0.95 was obtained in this study, with subscale reliabilities of .93 for burnout and .92 for secondary traumatic stress.
Connor-Davidson Resilience Scale (CD-RISC-10)
We evaluated resilience using the Korean version of the 10-item short form of the Connor-Davidson Resilience Scale (CD-RISC-10), 22 validated by Shin et al. 33 This scale has been validated through factor analysis for both general and clinical populations and is widely used as a concise yet highly reliable tool. It consists of 10 items, with each rated on a 5-point Likert scale from 0 (not true at all) to 4 (true almost always). Total scores range from 0 to 40; higher scores indicate higher resilience. The Cronbach’s alpha of the original scale was .85 and .94 in the present study.
Quality of Nursing Work Life (QNWL)
The quality of nursing work life was assessed using the Korean version of the Quality of Nursing Work Life (K-QNWL), 34 based on the original English version by Brooks and Anderson. 35 The K-QNWL is a 41-item tool consisting of five sub-dimensions: hospital management (10 items), communication and teamwork (7 items), hospital welfare policy (7 items), work design for quality nursing (10 items), and work conditions (7 items). Each item is rated on a 6-point Likert scale from 1 (not at all) to 6 (very much so). Total scores range from 41 to 246, calculated by summing the scores of each item. Cronbach’s alpha was .87 in this study, and the reliabilities for its sub-dimensions were as follows: hospital management .90, communication and teamwork .86, hospital welfare policy .88, work design for quality nursing .87, and work conditions .73.
Data collection
We posted a recruitment notice on “Nurscape,” an online community for nurses, and recruited participants using a snowball sampling method, where participants who viewed the notice shared it with other nurses. To minimize social desirability bias and ensure psychological safety regarding sensitive ethical questions, data were collected via an anonymous online snowball sampling method rather than institutional channels, allowing for a more authentic disclosure of participants’ moral distress. 36 Participants took part in the survey after being fully informed of the study’s purpose and procedures, including the fact that participation was voluntary and that they could withdraw at any time. Data were collected through a self-reported online survey using Google Forms, and all items were set as mandatory to minimize missing responses. Additionally, responses were restricted to one per IP address to prevent duplicate entries.
Data collection was carried out from October 14 to October 18, 2025, and a total of 312 surveys were collected. Of these, 289 surveys were included in the final analysis, excluding 23 responses. These exclusions comprised insincere responses (e.g., extreme completion times under 3 min or continuous straight-lining patterns) and respondents who did not meet the inclusion criteria based on demographic screening questions (e.g., having less than 3 years of clinical experience or holding non-direct care manager positions). The time required to complete the survey was approximately 10–15 min.
Data analysis
We analyzed the collected data using the IBM SPSS Statistics for Windows, Version 28.0, with descriptive statistical methods; for categorical data, the results are presented as frequencies or percentages. The correlations among moral distress, compassion fatigue, resilience, and quality of nursing work life were examined using Pearson’s correlation coefficient. The mediating effects of compassion fatigue and resilience on the relationship between moral distress and the quality of nursing work life were analyzed using PROCESS Macro Model 6. 37 Age and gender were included as covariates, intentionally excluding clinical experience. In the nursing workforce, age and clinical experience are highly correlated; thus, incorporating both into the mediation model simultaneously could introduce multicollinearity, leading to inflated standard errors and unstable coefficient estimates. 37 Controlling for age alone was deemed statistically sufficient to account for both demographic and professional maturity while maintaining model parsimony. All statistical tests were based on a significance level of .05 and a 95% confidence interval (CI).
Ethical considerations
This study was conducted following approval from the Institutional Review Board of Chung-Ang University (Approval No.: 1041078-20250715-HR-227). Before starting the online survey, participants were given sufficient information regarding the study’s purpose, procedures, voluntary nature of participation, the possibility of withdrawal, and measures for personal information protection, including that they could withdraw at any time by simply closing the web browser, ensuring that no partial data would be saved. Collected survey responses were encoded to ensure anonymity so that participants could not be identified, and the data were stored securely on the researcher’s password-protected personal device and in secure cloud storage. Participants’ mobile phone numbers were temporarily collected to prevent duplicate participation and to provide tokens of appreciation; however, this information was not used for any other purpose and was permanently destroyed upon completion of the study. Following the conclusion of the study, the collected survey data will be stored for 3 years according to relevant regulations and then permanently deleted. As a token of appreciation, mobile coffee coupons were provided to the participants.
Results
Participants’ demographic characteristics
Demographic characteristics of participating nurses (N = 289).
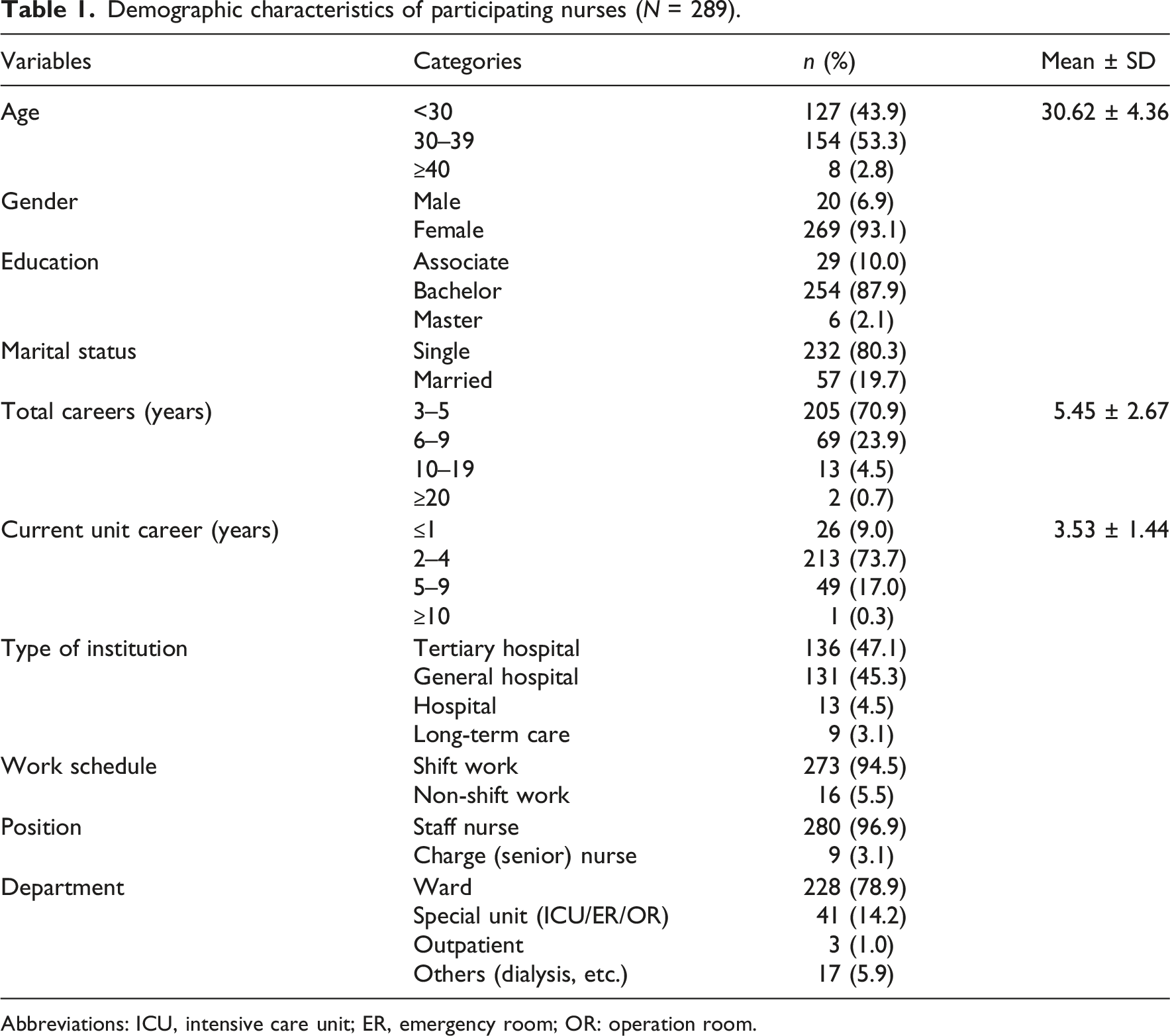
Abbreviations: ICU, intensive care unit; ER, emergency room; OR: operation room.
Degree of moral distress, compassion fatigue, resilience, and quality of nursing work life
Mean and correlation coefficients in study variables.
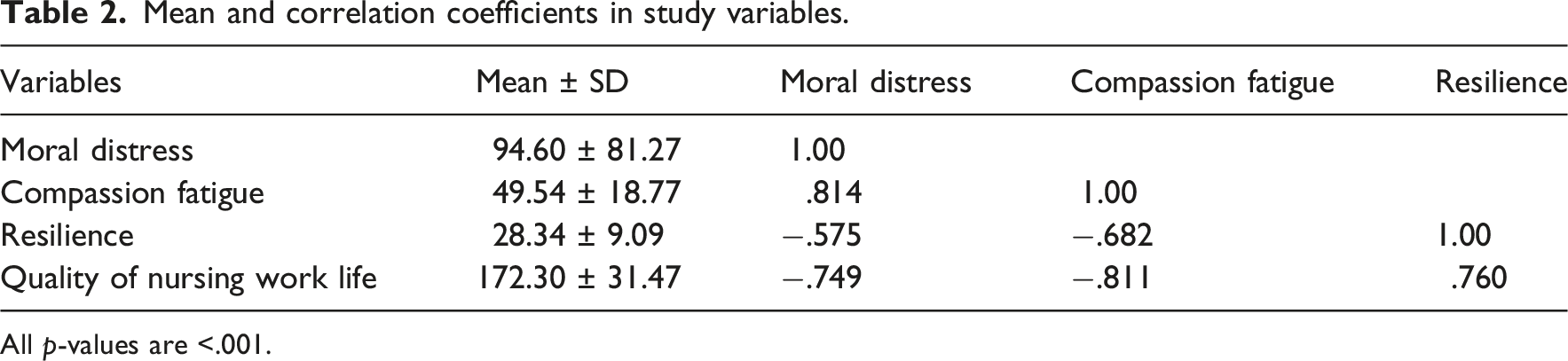
All p-values are <.001.
Moral distress showed a significant positive correlation with compassion fatigue (r = .814, p < .001), indicating that higher levels of moral distress were associated with higher compassion fatigue. Significant negative correlations were observed between moral distress and resilience (r = −.575, p < .001) and between moral distress and QNWL (r = −.749, p < .001), meaning that as moral distress increased, both resilience and QNWL decreased. Compassion fatigue also had significant negative correlations with resilience (r = −.682, p < .001) and QNWL (r = −.811, p < .001). Finally, resilience and QNWL demonstrated a significant positive correlation (r = .760, p < .001), showing that higher resilience was associated with a higher quality of nursing work life (Table 2).
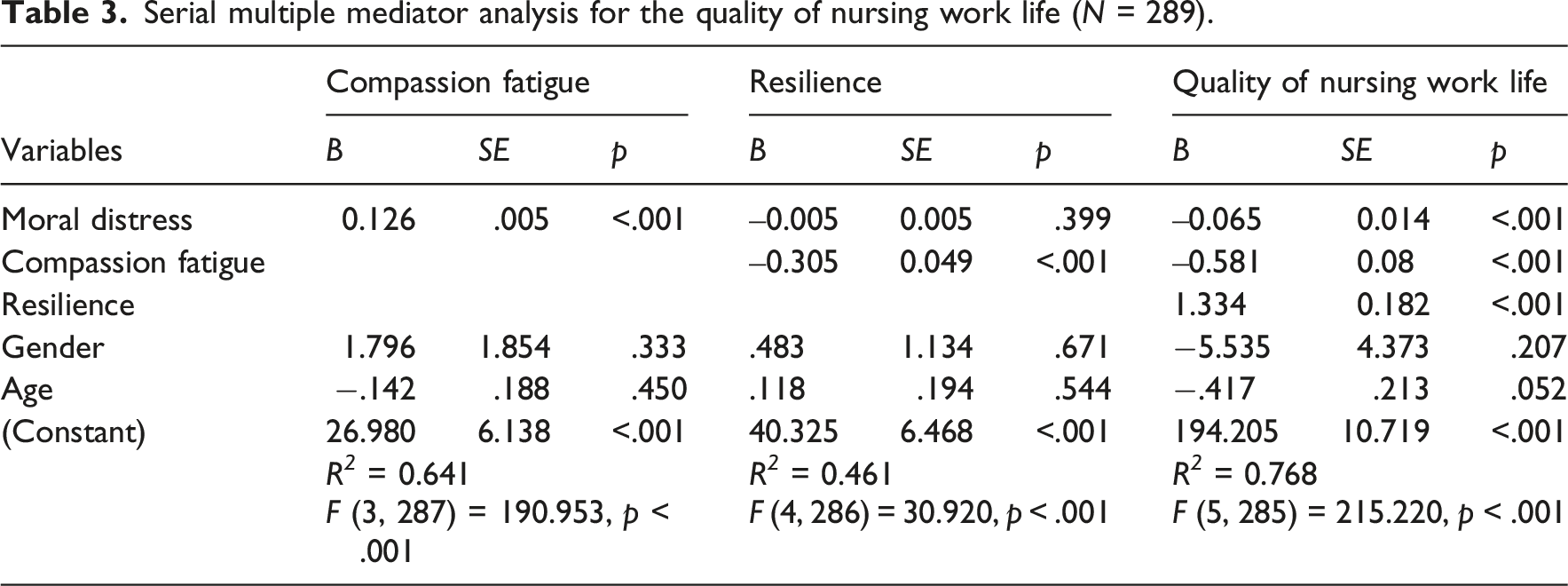
Mediating effects of compassion fatigue and resilience
To verify the mediating effects of compassion fatigue and resilience on the relationship between moral distress and quality of nursing work life, a parallel multiple mediator model was initially applied. The analysis revealed a correlation coefficient of −0.460 between the model residuals, indicating a strong negative relationship where higher compassion fatigue was associated with lower resilience, even after controlling for moral distress. This justified the assumption of a causal path between the mediators. Therefore, a serial multiple mediator model (PROCESS Model 6) was selected as the final analysis model.
The results of the serial multiple mediator analysis showed significant paths from moral distress to compassion fatigue (B = 0.126, p < .001), compassion fatigue to resilience (B = −0.305, p < .001), and resilience to quality of nursing work life (B = 1.334, p < .001). The indirect effect coefficient of the serial mediation path, where moral distress sequentially passes through compassion fatigue and resilience to reach QNWL, was −0.051 (95% CI [–0.081, −0.032]), which was statistically significant. Conversely, the simple mediation effect of moral distress on QNWL through resilience alone was −0.006 (95% CI [‒0.019, 0.008]), which was not statistically significant. The total effect of the model was −0.196 (95% CI [‒0.216, −0.176]), and the direct effect after including all mediators remained significant at −0.065 (95% CI [‒0.093, −0.038]).
Serial multiple mediator analysis for the quality of nursing work life (N = 289).
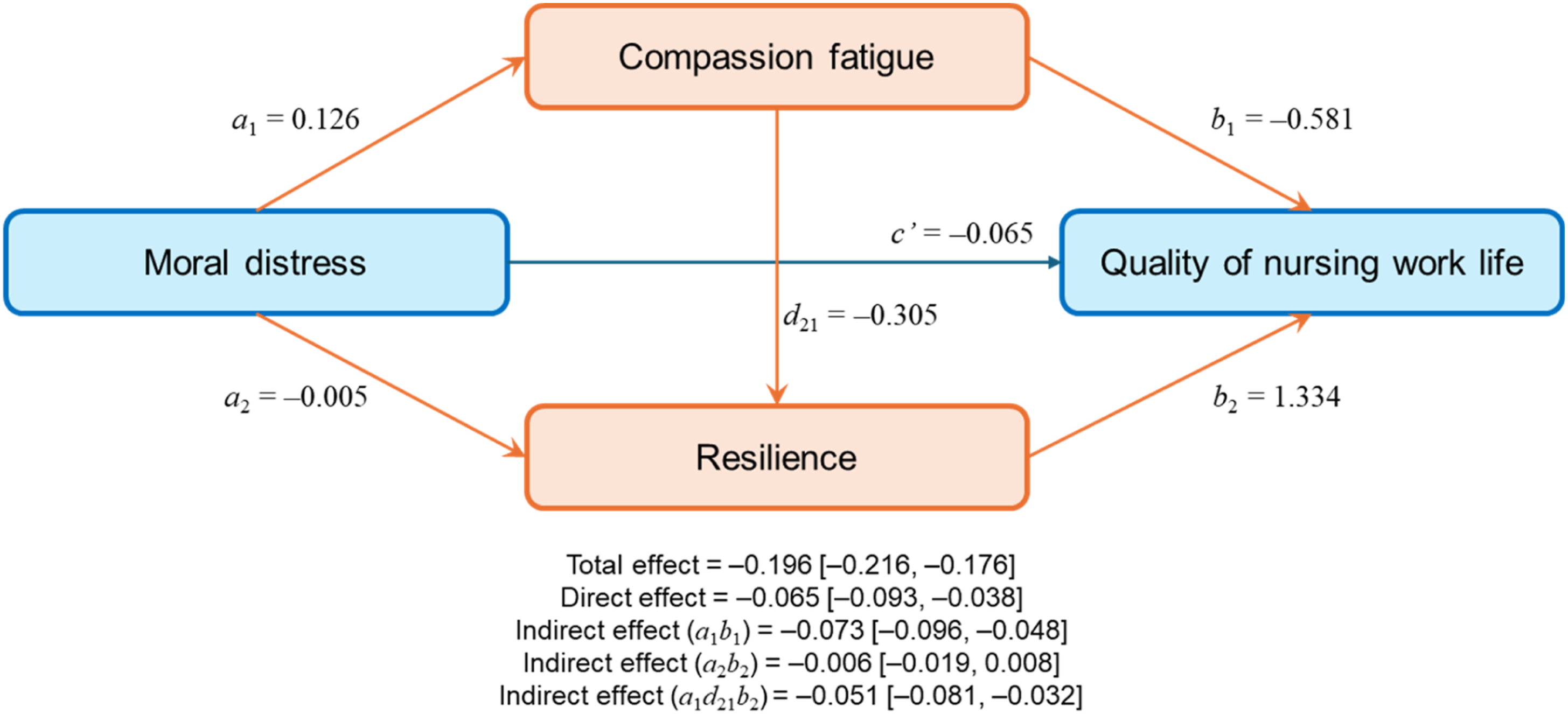
A serial multiple mediation model of the quality of nursing work life, controlling for age and gender.
Discussion
The study, conducted to identify the influence of moral distress among clinical nurses, showed that the participants’ moral distress score averaged 94.60 points, which is an above-average level. This figure is higher than that reported among nurses in Iran and the Netherlands using the same instrument. Oldenmenger et al. 30 stated that open communication within a team and opportunities for structured ethical discussion alleviate moral distress; however, it is suggested that Korean nurses experience relatively higher levels of ethical stress due to heavy workloads, role conflicts, and a hierarchical organizational culture. 38 In particular, the fact that the results of this study are similar to or higher than those of previous domestic studies implies that improving the ethical environment of clinical settings remains an urgent task.
The participants’ compassion fatigue averaged 49.54 points, a moderate level, which is slightly lower than a study targeting nurses in small-to-medium-sized hospitals. 39 This difference appears to be partly influenced by the age and clinical career distribution of the participants in this study. Meanwhile, compassion fatigue is reported to be influenced by multidimensional factors such as the nursing work environment, patient characteristics, and personal factors, and it has been confirmed that levels of compassion fatigue and burnout can vary significantly among individuals even in the same work environment. 40 Considering this, the results of this study suggest that various organizational and contextual factors, in addition to age and clinical career, are important in explaining compassion fatigue levels.
Resilience averaged 28.34 points, an above-average level, which falls within a similar range as studies of nurses in tertiary and general hospitals using the same scale.41,42 This shows that resilience does not differ significantly from the levels generally reported among clinical nurse groups. Previous studies have reported resilience as an important protective factor that helps nurses regulate stress or emotional burdens encountered during the work process and to maintain psychological well-being.43,44 Therefore, the above-average level of resilience found in this study may function as an important protective factor buffering nurses’ stress reactions in clinical situations.
The quality of nursing work life averaged 172.30 points, showing a relatively higher level than reported in previous studies targeting nurses in tertiary and general hospitals.4,39 This difference is consistent with reports from previous studies that contextual characteristics—such as the work environment, staffing, and workload—can affect the level of quality of work life. 45 Furthermore, the quality of nursing work life can vary depending on organizational factors such as the work environment, management system, workload, and interpersonal relationships, and institutional characteristics and staffing have also been reported as factors influencing it. 46 Considering these points, the relatively high level of quality of nursing work life observed in this study may be attributable to the participants’ work environment or organizational characteristics, providing important context for interpreting its relationship with the psychological factors in this study.
According to the mediation path analysis, which is the primary finding of this study, the serial mediation path in which moral distress leads to the quality of nursing work life through compassion fatigue and resilience was statistically significant. The fact that moral distress had a direct effect on the quality of nursing work life, even after controlling for mediating variables, reaffirms that the gap between ethical values and actual practice is a powerful factor hindering nurses’ professional lives.
A notable finding is that moral distress affected resilience indirectly through compassion fatigue rather than directly. This suggests that compassion fatigue may play a “gateway” role in the process by which moral distress weakens resilience. In other words, rather than immediately depleting a nurse’s internal resource of resilience, the external stress of moral distress follows a gradual erosion process in which emotional energy is first exhausted, followed by a decline in psychological defense mechanisms. These results are consistent with those of Zhai et al. 47 and Yin et al., 20 who reported a sequential mediating relationship between compassion fatigue and resilience.
The sequential path identified in this study clearly suggests priorities for nursing interventions. Although resilience is the variable with the strongest positive influence on the quality of nursing work life, the accumulation of compassion fatigue may make it difficult to maintain a high quality of work life even among nurses with high resilience. Therefore, interventions to improve the quality of nursing work life should not be limited to enhancing individual resilience; efforts to alleviate moral distress—a significant antecedent of compassion fatigue—should also be implemented at the organizational level. Organizations should identify the underlying environmental factors associated with moral distress and strengthen early intervention to prevent compassion fatigue from accumulating. Additionally, a balanced approach considering differences in stress sensitivity according to individual tendencies is required in building organizational resilience. 48
In sum, to protect the quality of clinical nurses’ work life, organizational ethical decision support systems should be implemented early, when nurses first experience moral distress. An integrated intervention strategy should be introduced to the clinical field to create an environment of psychological safety where nurses can freely express their opinions during ethical dilemmas and to prevent compassion fatigue from eroding resilience.
Limitations
While this study is significant for identifying the psychological mechanisms involved in protecting the quality of nursing work life among nurses, it has several limitations. First, data were collected using snowball sampling through an online nursing community. Furthermore, setting all survey items as mandatory to prevent missing data may have constrained participants’ item-level autonomy, even though they were informed they could exit the survey at any time.
This may limit the findings to users of a specific platform, making it difficult to represent the entire population of clinical nurses; furthermore, due to the nature of self-reported online surveys, the possibility of social desirability bias cannot be excluded. Future studies should employ stratified sampling to encompass nurses from various regions and hospital sizes. Second, this study adopted a descriptive survey design to confirm the relationship between moral distress and QNWL. Consequently, there are limitations in establishing firm causal relationships based on temporal precedence; therefore, follow-up longitudinal studies are needed to clarify the dynamic causal mechanisms between these variables. Third, the quality of nursing work life is influenced by multidimensional contextual factors, such as hospital policies, staffing, and organizational culture. This study focused primarily on individual psychological mechanisms and did not sufficiently control for or include these organizational and environmental variables as independent variables. Subsequent research utilizing multilevel analysis that incorporates organizational-level variables is suggested. Finally, although professional nursing performance is closely related to the ethical climate within an organization, this study did not fully reflect specific environmental characteristics where the moral voice of nurses might be suppressed. This may act as a limitation in providing an in-depth understanding of the structural obstacles that hinder nurses’ ethical practices.
Implication for clinical practice
Based on the sequential mechanisms identified, healthcare institutions must shift from individual-focused resilience training to structured, systemic ethics interventions. First, organizations should implement “Ethical Grand Rounds” and anonymous consultation channels where bedside nurses can discuss moral dilemmas safely without fear of organizational repercussions. Second, because compassion fatigue acts as a critical gateway eroding psychological defenses, nurse managers and senior clinical leaders (such as charge nurses) should be trained as ethics first-responders. They must be equipped with screening tools to identify early signs of emotional depletion in high-risk units like ICUs and oncology wards. Finally, clinical protocols should incorporate regular, structured debriefing sessions following ethically challenging events—such as life-sustaining treatment decisions—to prevent cumulative distress. Creating a psychologically safe environment that amplifies nurses’ moral voice is an essential prerequisite for preventing compassion fatigue and safeguarding the quality of nursing work life.
Conclusion
This study aimed to investigate the mediating effects of compassion fatigue and resilience on the impact of moral distress on the quality of nursing work life among clinical nurses. The analysis confirmed a sequential mediating path in which moral distress induces compassion fatigue, which in turn weakens resilience and ultimately deteriorates the quality of nursing work life. These results suggest that ethical stress experienced by nurses follows a gradual erosion process, where emotional energy is exhausted first, followed by the gradual undermining of resilience, an individual’s psychological defense mechanism.
Based on these findings, the following suggestions are made to protect and improve the quality of nursing work life. First, active intervention is essential at the early stage when nurses report moral distress. In particular, recognizing that compassion fatigue is a key gateway for the erosion of resilience, systematic psychological support strategies must be established to prevent compassion fatigue and manage compassion satisfaction. Second, rather than relying solely on the enhancement of an individual nurse’s resilience, organizational efforts should be made to inspect and improve the structural and environmental factors that cause moral distress. It is of paramount importance to create an organizational culture in which the moral voice of nurses is respected and psychological safety is guaranteed.
Footnotes
Acknowledgments
The authors would like to thank all the participants for their contribution to this study.
Author contributions
Ha Eun Lee: Conceptualization, data collection and analysis, validation, writing—original draft. Hyejin Kim & Ji-Su Kim: Conceptualization, review—original draft. Eunjung Ryu: Conceptualization, methodology, supervision, visualization, and manuscript writing. We confirm that all authors meet the authorship criteria and are in agreement with the content of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
More data about this study can be requested from the authors on reasonable requests.