
Abstract
Digital infrastructures such as platforms, algorithms, and artificial intelligence (AI) are rapidly reshaping the conditions under which nursing care is enacted, raising ethical concerns that extend beyond efficiency. Indeed, as nursing becomes increasingly embedded within platformized and AI-mediated ecosystems, the discipline is confronted with new forms of harm arising from the disruptions to the relational foundations that make ethical nursing possible. Despite this, the discipline lacks a coherent conceptual framework capable of naming, analysing, and responding to the relational injuries produced by digital infrastructures and platformization. This paper introduces the concept of digital-relational harm. Drawing on six philosophical and theoretical traditions: African relational ontology, Western phenomenology and care ethics, Eastern relational philosophies, relational ethics, Labour Process Theory, and digital professionalism, the paper demonstrates that digital-relational harm arises when digital infrastructures disrupt person becoming, displace embodied and intersubjective presence, disturb relational harmony, erode trust and mutuality, fragment labour and continuity, and destabilise professional identity. These disruptions are structural, relational, and ontological. By naming digital-relational harm, the paper reframes digital transformation as an ethical and relational challenge, not merely a technical one, and argues that safeguarding relational integrity must become a central concern in the design, governance, and evaluation of digital health systems. Digital-relational harm offers nursing ethics a new analytic lens for understanding how digital environments shape moral life and provides a foundation for future empirical, theoretical, and policy-oriented work.
Introduction
Nursing has entered a pivotal era in which digital infrastructures such as algorithms and artificial intelligence (AI) are rapidly reshaping the conditions under which care is delivered, relationships are formed, and professional identity is enacted. 1 Across diverse health systems, nurses increasingly work within environments mediated by digital platforms that structure visibility and govern behaviour through algorithmic systems. 2 These technologies promise efficiency and flexibility to fluctuating workforce demands, yet they also introduce disruptions to the relational foundations that remain at the core of nursing practice. 3 By shifting attention to data-driven efficiency, digital systems risk interfering with presence and interfering with relational continuity. Thus, as nursing becomes embedded within platformized and AI-mediated ecosystems, the discipline is confronted with potential emerging forms of harm that remain conceptually unrecognized and ethically unaddressed. 3
While existing frameworks of harm in healthcare such as physical injury, psychological distress, moral distress, and moral injury remain essential,4–6 they are grounded in philosophical accounts that conceptualize harm primarily as a setback to individual interests, wellbeing, or moral agency. What remains missing is a concept capable of explaining how digital mediation alters recognition, continuity, relational presence, and the communal processes that make ethical nursing possible. This conceptual gap provides the rationale for introducing digital-relational harm as a distinct category of injury in nursing ethics. For this paper, digital-relational harm is operationally defined as ‘the ontological, ethical, and relational injuries that arise when digital infrastructures disrupt the relational conditions necessary for personhood, care, and professional identity in nursing’. Digital-relational harm does not replace traditional accounts but extends them by naming a form of injury that arises when digital systems fragment the relational conditions that make ethical nursing practice possible.
Platformization which refers to the reorganization of work, relationships, and governance through digital intermediaries exemplifies this transformation.7,8 Digital labour platforms can automate scheduling and use behavioural metrics to influence labour availability. For example, instead of a nurse being scheduled by a unit manager who knows their skills and team relationships, an automated digital platform takes on the role. Rather than continuity being built through repeated interactions with the same team, nurses may be dispatched to different facilities or clinical units each day according to real-time demand signals. Documentation, communication, and performance visibility are similarly mediated through platform dashboards rather than through relational knowledge within a ward.
Within the platformization landscape, a clear hierarchy of labour forms emerges: digital platform work as the broad global phenomenon 9 ; platform-mediated work as the subset of labour allocated, coordinated, or governed through digital platforms 10 ; and gig work as the most specific category, characterized by on-demand, short-term job arrangement. 11 This stratification underscores how platformization reshapes not only the organization of labour but also the relational and ethical conditions under which nursing care unfolds. Algorithmic governance employed in platformized work introduces opaque forms of control that shape the visibility of nurses and how they are valued, and granted access to work. 12 What is more, algorithmic governance further introduces what has been described as a ‘responsibility gap’, (p. 175) 13 wherein moral accountability becomes diffused or displaced when digital systems act as primary decision-makers. As algorithms increasingly prioritise patients, flag risks, or structure clinical choices, nurses may come to view themselves as passive executors of system outputs rather than autonomous ethical agents. 14 This dynamic creates a risk of moral disengagement, where responsibility is subtly shifted from the nurse to the digital system, weakening ethical intention and diminishing the sense of moral presence that underpins relational practice. 15 Together, AI-mediated systems may increasingly filter recognition, communication, and decision-making, altering the relational texture of clinical encounters. 12 These transformations can potentially erode moral agency and generate harms that are neither purely technical nor purely interpersonal: they are digital-relational harms.
The rise of platformized nursing illustrates the depth of this transformation and nature of this unique type harm.3,12 Unlike traditional agency work, platformization is continuous, data-driven, and embedded within the economic logics of platform capitalism. 3 Nurses experience new forms of algorithmic oversight, taskification, and mobility that disrupt the relational continuity and contextual grounding central to safe and ethical nursing practice. These structural shifts are further intensified by AI-enabled triage tools, 16 automated documentation systems, 17 and predictive analytics that mediate how patients are seen and how nurses are evaluated.18,19 Indeed, AI-supported triage tools can misclassify urgency when contextual cues are absent, narrowing the relational space for clinical judgement. Electronic health records may redirect nurses’ attention toward documentation interfaces, reducing opportunities for embodied presence. Predictive analytics used in staffing systems can inadvertently prioritise efficiency over continuity, while telehealth encounters often limit the subtle intersubjective cues that support relational attunement. Routine interactions with electronic health records, barcode medication systems, automated vital sign monitors, and clinical decision support tools all mediate how nurses perceive, interpret, and respond to patients.
Background
From the perspective of African relational ontology, wherein personhood is understood as a communal and relational achievement, disruptions to relational integrity represent more than operational challenges: they constitute injuries to the very processes through which persons come into being.20,21 In this context, an operational challenge refers to a disruption in workflow or task performance, for example, when a digital documentation system is slow or unintuitive. By contrast, an injury to person becoming concerns a break in the continuity of relational and communal processes through which nurses and patients come to be recognised as persons when digital systems mediate practice.20,21 In African relational ontology emerging from philosophical foundations such as Ubuntu, Ukama, and Consciencism, personhood is cultivated through sustained presence, mutual recognition, and shared moral accountability.20,21 When platformized staffing models prevent nurses from forming ongoing relationships with patients or colleagues, the harm is not merely operational; it undermines the relational conditions through which personhood is enacted. This distinction helps clarify why digital-relational harm is ontological rather than simply technical.
Similar concerns emerge across other philosophical traditions. In much of Western thought, particularly in phenomenology and care ethics, the self is formed through embodied intersubjectivity, mutual recognition, and the moral texture of human encounters.22,23 When digital systems fragment these encounters through platformized care, they erode the conditions necessary for continuous, authentic presence, and ethical responsiveness.24,25 Eastern philosophies likewise emphasize relationality, interdependence, and the co-arising nature of persons within a web of social and moral obligations. From Confucian ren and li, which ground personhood in harmonious relational conduct, to Buddhist notions of dependent origination, which understand the self as constituted through interconnected processes, relational disruption is not a peripheral inconvenience but a disturbance of the moral and ontological order.26,27 Similarly, relational ethics emphasizes that ethical practice emerges through relationships characterised by trust, mutuality, and attentiveness: conditions that may be increasingly mediated or eroded by digital systems. 28 Taken together, these philosophical and theoretical traditions reveal a shared insight: digital infrastructures do not merely alter workflows or communication patterns but contribute to reorganizing the relational, ethical, and ontological conditions that make nursing practice possible. While each tradition emphasizes different dimensions: communal person-becoming, embodied presence, interdependence, ethical responsiveness, structural organization, or professional identity; they converge in showing that digital systems reshape how nurses and patients encounter one another as persons. Thus, digital-relational harm is not an incidental by-product of technological change but a structural and relational injury that emerges when digital systems distort the conditions under which relational care is enacted.
Digital-relational harm is worth nursing’s attention because the discipline is grounded in relational presence, embodied attunement, and the moral texture of human encounters.29,30 Unlike other professions where digital mediation primarily affects workflow or efficiency, nursing practice depends on the ability to form, sustain, and act within relationships characterized by trust, mutual recognition, and contextual understanding. These relational capacities are not peripheral to nursing; they are the very conditions under which safe, ethical, and person-affirming care becomes possible. 31 Thus, digital-relational harm is not simply one category of harm among many; it is a form of injury that directly targets the relational, communal, and ontological foundations of nursing. Naming this vulnerability is essential for understanding why digital transformation poses unique risks to nursing practice and why a concept such as digital-relational harm is necessary to guide ethical, organizational, and technological responses. For instance, when a nurse is required to complete extensive digital documentation during a palliative care conversation, the shift of attention toward the screen can interrupt the relational presence that patients rely on for emotional support. In acute care, algorithmic early-warning systems may prioritise numerical thresholds over the nurse’s embodied sense that a patient ‘does not look right’, narrowing the space for intuitive judgement. In community settings, telehealth platforms may limit the subtle relational cues such as changes in gait, affect, or home environment that nurses use to assess wellbeing.
In fact, platformization does more than reorganize workflows or redistribute labour in nursing; it reshapes the ontological conditions under which nurses and patients come to be recognized as persons. Digital infrastructures redefine what counts as a ‘person’, ‘worker’, or ‘professional’ by simplifying and translating complex relational identities into data profiles, behavioural metrics, and algorithmic categories.32,33 Through this process of datafication, nurses and patients may become what is conceptualized as thin persons (digitally legible representations that capture only fragments of their relational, moral, and contextual existence). For example, a nurse’s professional identity may be reduced to punctuality scores, shift acceptance rates, or patient-generated star ratings, while a patient may be represented primarily through risk scores or algorithmically generated acuity categories. When recognition is mediated by algorithms rather than by relational presence, the processes of person becoming are disrupted.30,31 Platformization thus produces ontological harm not because digital systems malfunction, but because they reorganize the very conditions through which persons are encountered, valued, and held within relational and communal life.
Although platformized nursing represents the most concentrated and visible site of digital-relational harm, the concept may apply across the broader landscape of digital health. 8 Automated documentation systems may reshape how nurses perceive and respond to patients by filtering clinical information through predefined, standardized templates. Algorithmic scheduling tools determine visibility and access to work, often without transparency. Telehealth platforms mediate communication through screens that flatten affective nuance. Standardized digital tools such as automated documentation systems, dropdown menus, and templated assessments also reshape the epistemic landscape of care. From a Buddhist perspective, these systems may erode Sati (mindfulness) 34 by diverting attention away from the patient’s embodied presence toward rigid screen-based inputs. They may also constrain Yonisomanasikāra (analytical reflection), 35 limiting the nurse’s ability to explore in-depth and interpret subtle contextual cues. These constraints may impact care, wherein the patient’s holistic narrative is flattened into predefined categories and the nurse’s experiential knowledge is devalued by the system’s epistemic priorities.
Despite these emerging challenges, the discipline of nursing lacks a coherent conceptual framework capable of naming, analyzing, and responding to the relational injuries produced by digital infrastructures and platformization. For example, Turley’s Nursing Informatics Model frames digital systems as tools that support data, information, and knowledge processes which positions digital disruption as a workflow and information-management problem, not a relational concern. 36 While eight distinct theories have been highlighted in a recent scoping review as representing how nurses can enact caring in a digital world, 37 they remain insufficiently integrated to address the deeper structural and relational consequences of digital transformation. The concept of digital-relational harm is therefore needed to illuminate the ontological, ethical, and socio-technical consequences of platformization and AI-mediated practice in nursing. It provides language for understanding how digital infrastructures interrupt the processes of relational becoming emphasized in African ontology, undermine the intersubjective presence central to Western phenomenology and care ethics, and destabilize the interdependent moral order foregrounded in Eastern philosophies. By articulating this concept, the discipline gains an analytic tool necessary to see how digital systems reconfigure the relational foundations of nursing and to develop strategies that safeguard relational integrity, moral agency, and personhood in an increasingly digital world. Given the foregoing, this paper aims to introduce and theorize the concept of digital-relational harm as a distinct form of injury in contemporary nursing.
Theoretical and philosophical basis of digital-relational harm in nursing
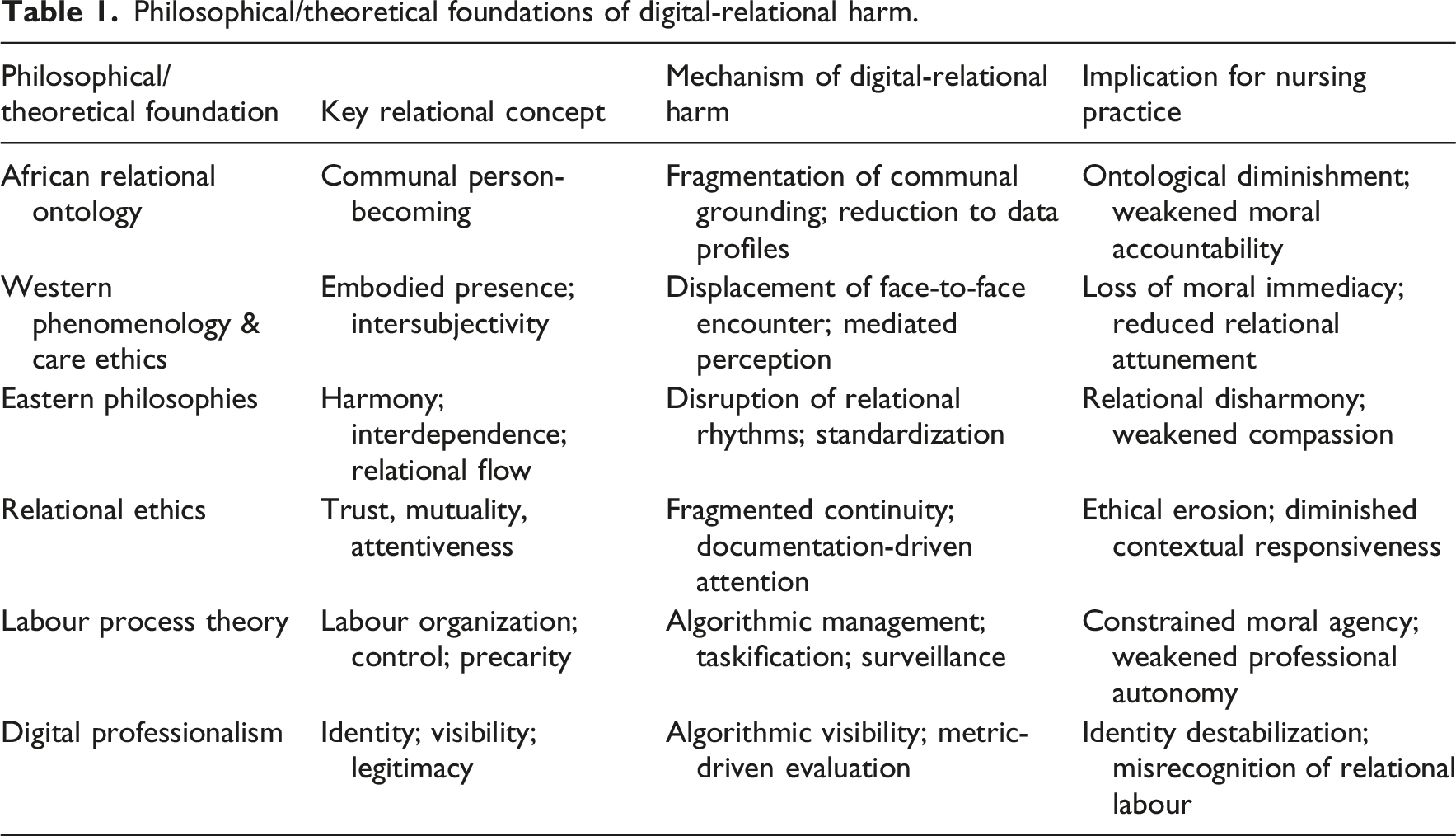
The concept of digital-relational harm is grounded in a synthesis of philosophical and theoretical traditions that illuminate how digital infrastructures reshape the relational foundations of nursing practice. Six bodies of thought: African relational ontology, Western phenomenology and care ethics, Eastern relational philosophies, relational ethics, Labour Process Theory, and digital professionalism provide the core intellectual scaffolding. The selection of these six philosophical and theoretical traditions is intentional and necessary for developing a concept as complex and multi-layered as digital-relational harm. Each tradition illuminates a different dimension of how digital infrastructures reshape the relational, ethical, and ontological foundations of nursing practice, albeit together, they offer a holistic view of digital-relational harm. Although African relational ontology, Western phenomenology and care ethics, Eastern relational philosophies, and relational ethics all foreground relationality, they are brought together in this paper. Their convergence on relationality is not redundancy but conceptual triangulation.
Philosophical/theoretical foundations of digital-relational harm.
African relational ontology: Personhood as communal becoming
While this paper acknowledges the diversity within African philosophical thoughts, a common thread emerging from the works of African scholars like John Mbiti, 38 Ifeanyi Menkiti, 39 Kwame Gyekye, 40 and Kwasi Wiredu 41 regarding relational ontology highlight personhood as a process of becoming with the community playing a critical role. 21 This offers the deepest philosophical grounding for digital-relational harm because it begins from a radically different premise than most Western individualist frameworks: personhood is not something one possesses, but something one becomes through other persons.20,21,42 This assertion is captured in the famous maxim by Mbiti that ‘I am because we are; and since we are, therefore I am’ (p. 106). 43 Within this worldview and anchored in traditions such as Ubuntu, Ukama, and Consciencism, the self is constituted through ongoing participation in communal life, reciprocal recognition, and moral accountability. Personhood is therefore a relational, temporal, and ethical achievement, continually enacted through practices of care, solidarity, and mutual regard.20,21,42
In this ontological frame, relationships with other persons are not merely social interactions; they are the very medium through which human beings come into existence as moral subjects and become persons. 21 To be recognised, to be held within a web of communal obligations, to be accountable to others; these are the conditions that make personhood possible. 21 Nursing, as a relational and moral practice, is deeply aligned with this worldview: the nurse becomes a nurse through relational presence, shared vulnerability, and moral responsiveness to the patient and community.42,44 The care provided in the context of nurse-patient relationship does not only contribute to healing, but also facilitates the person becoming process of the patient. 44 When platformized digital systems intervene in the nurse–patient relationship, they can sever the relational continuity that grounds nursing’s relational ontology, resulting in ontological harm that affects both the nurse’s professional becoming and the patient’s experience of being cared for. Together, African relational ontology uniquely illuminates the ontological dimension of digital-relational harm by showing how digital infrastructures disrupt the communal processes of person-becoming and moral accountability.
Western philosophical traditions: Intersubjectivity, embodiment, and moral presence
Western philosophical traditions, particularly phenomenology, Levinasian ethics, and care ethics, provide a rich account of how personhood, moral responsibility, and relational life emerge through embodied presence and intersubjective encounter.45–47 These traditions converge on a central insight: the ethical and relational fabric of human life is constituted through lived experience, embodied attunement, and the immediacy of face-to-face encounter. 47 Phenomenology, as developed by Husserl and Merleau-Ponty, foregrounds the body as the primary site of perception, meaning-making, and relational engagement. For Merleau-Ponty, the body is not an object but a lived body, a medium through which we encounter others and the world. 48 Nursing practice is deeply phenomenological in this sense: it relies on embodied attunement, sensory presence, and the subtle, pre-reflective cues that arise in shared space. 49
Levinasian ethics deepens this analysis by arguing that moral responsibility arises in the face-to-face encounter, where the presence of the Other calls the self into ethical relation. 47 The face is not merely a physical feature; it is a moral event, a summons to responsibility, vulnerability, and care. 47 Care ethics, articulated by scholars such as Gilligan 50 and Tronto, 51 positions relational attentiveness, responsiveness, and contextual understanding as the core of moral life. From these perspectives, care is not a set of tasks, but a relational practice grounded in empathy, mutuality, and responsiveness to the needs of others. Taken together, phenomenology, Levinasian ethics, and care ethics reveal that digital-relational harm is not simply a matter of reduced communication or interpersonal strain. It is a disruption of the embodied, intersubjective, and moral foundations of nursing practice. Western philosophical traditions therefore suggest that digital-relational harm is a form of moral and relational displacement, where the ethical immediacy, embodied presence, and relational attentiveness that define nursing are disrupted by technological systems via mediation, constraint, and replacement.
In practical nursing settings, these three forms of disruption operate differently. Mediation occurs when digital systems filter or structure the encounter, for instance, when an electronic triage tool determines which symptoms are visible to the nurse, shaping how the patient’s condition is first perceived. Constraint arises when digital workflows limit the nurse’s ability to act on relational cues, such as when rigid documentation templates prevent the recording or in-depth exploration of contextual or narrative information. Replacement is evident when digital systems take over relational functions entirely, as in automated patient-facing chatbots that substitute for human contact which may occur when robots are assigned to assess vital signs or provide companionship. Each of these mechanisms demonstrate how digital systems alter the embodied and ethical immediacy central to phenomenological and care-ethical accounts of nursing. Put together, Western phenomenology and care ethics uniquely clarify the embodied and intersubjective dimension of harm, demonstrating how digital mediation displaces moral presence, embodied attunement, and the immediacy of the face-to-face encounter.
Eastern philosophical traditions: Interdependence, harmony, and moral relationality
Eastern philosophical traditions, particularly Confucianism, Buddhism, and Daoism, offer a profoundly relational and interdependent understanding of personhood, moral life, and social order.52–54 While distinct in emphasis, these traditions converge on a shared insight: the self is not an isolated entity but a node within a dynamic web of relationships, obligations, and interdependent processes. 55 This worldview provides a powerful foundation for understanding how digital infrastructures disrupt the relational and moral conditions that sustain nursing practice.
Confucian philosophy grounds personhood in the cultivation of ren (humaneness or benevolence) and li (relational propriety, ritual, and appropriate conduct). 56 These concepts emphasise that moral life is enacted through harmonious relationships, where individuals fulfil their roles with attentiveness, respect, and mutual responsibility.56,57 Personhood is not a private possession but a relational achievement, cultivated through ethical participation in family, community, and society. In nursing, this resonates deeply: the nurse–patient relationship is a moral role requiring attentiveness, compassion, and relational propriety.
Buddhist philosophy promotes the notion that all phenomena, including the self, arise through interdependent causes and conditions. 58 The self is therefore not a fixed entity but a relational process, continually shaped by interactions, perceptions, and shared experiences. 59 Compassion and mindfulness emerge from recognizing this interdependence. In nursing practice, this aligns with the understanding that care is a co-created relational process, shaped by the mutual presence and shared vulnerability of nurse and patient. Buddhist philosophy offers further depth through the principle of Pratītyasamutpāda (dependent origination), which teaches that all phenomena, including the nurse–patient relationship, arise co-dependently through shared conditions. This view highlights that relational presence is not a one-directional act but a mutually constituted process of interbeing. Digital infrastructures disrupt this co-arising by reducing relational encounters to discrete data points, thereby severing the dynamic interdependence that sustains compassionate care. The Buddhist concept of Karuṇā (compassion) further illuminates how digital mediation can erode the moral impulse to alleviate suffering when attentiveness is displaced by screen-based tasks. When digital systems narrow the relational field, they compromise the conditions under which compassion naturally emerges, deepening the disturbance of relational harmony.
Daoist philosophy emphasises attunement to the Dao (the natural, dynamic flow of life) 60 and the cultivation of wu wei, a form of effortless, responsive action grounded in harmony with relational and environmental rhythms. 61 Daoism values balance, subtle responsiveness, and the capacity to move fluidly within relational contexts. Nursing practice often mirrors this Daoist sensibility: effective care requires attunement to the patient’s needs, responsiveness to changing conditions, and the ability to act with fluidity rather than rigid adherence to protocol.
Together, these Eastern traditions illuminate three distinct mechanisms of digital-relational harm. Confucianism reveals how digital acceleration and standardised workflows generate relational disharmony by disrupting ren and li; the relational propriety and role-responsiveness that sustain moral order. Buddhism shows how digital mediation disrupts interdependence by severing the co-arising relational processes through which compassion, presence, and mutual vulnerability emerge. Daoism highlights how rigid interfaces, algorithmic prompts, and taskification produce a loss of attunement, undermining the fluid, responsive, and context-sensitive action essential to therapeutic nursing encounters. In all, Eastern relational philosophies uniquely reveal the harm to relational harmony and interdependence, showing how digital acceleration and standardization disturb the relational rhythms through which compassion, balance, and moral understanding arise.
Labour process theory: Algorithmic control and work restructuring
Labour Process Theory (LPT), originating from Braverman’s Labor and Monopoly Capital, provides a critical framework for understanding how work is organized, controlled, and experienced under capitalism. 62 Braverman argued that management continually seeks to increase control over labour through deskilling, standardization, and surveillance, restructuring work in ways that reduce worker discretion and consolidate managerial authority. 62 Contemporary scholars have extended LPT into the digital era, showing how algorithmic management, data-driven oversight, and behavioural nudging introduce new forms of labour discipline within platform-mediated work.63,64
In digital nursing environments, the dynamics of maximizing control, efficiency, and extraction are intensified through algorithmic management, where platforms allocate shifts, rank workers, and shape behaviour through opaque data-driven systems. 3 Nursing labour becomes taskified, broken into discrete, time-bound units that prioritise throughput over relational depth. 33 Surveillance, once managerial and episodic, becomes continuous and infrastructural, embedded in digital workflows, geolocation tools, and performance dashboards. These conditions generate precarity, weaken professional autonomy, and erode the stable relational environments required for ethical and therapeutic practice. LPT emphasizes how labour fragmentation weakens collective organisation and worker solidarity. Platformized nursing isolates nurses from organizational communities, reduces opportunities for collective bargaining, and fosters competition through ratings and metrics. 65 These dynamics erode the collective foundations of nursing professionalism and limit nurses’ ability to advocate for safe working conditions or ethical practice. LPT therefore reveals that digital-relational harm is not incidental but structurally produced by the logics of platform capitalism, which reorganize nursing work in ways that fragment relationships.
LPT is a directly applicable theoretical basis because digital platforms introduce concrete mechanisms of control that reorganise how nursing labour is allocated, monitored, and valued. Algorithmic scheduling systems determine which nurses are visible and eligible for shifts, often prioritising metrics such as acceptance rates or punctuality over contextual knowledge or relational continuity. Ratings systems, such as those generated by patients, facilities, or automated behavioural analytics shape future access to work, creating a feedback loop in which algorithmic visibility replaces relational recognition. Productivity dashboards quantify labour into discrete metrics such as task completion times, documentation speed, or mobility patterns, narrowing the space for relational judgement. Taskification further fragments nursing work into isolated, measurable units, eroding the holistic and relational nature of practice. Together, these mechanisms illustrate how platform governance restructures the labour process in ways that directly produce digital-relational harm by displacing professional autonomy, fragmenting continuity, and subordinating relational care to algorithmic priorities.
A further concern is the emergence of a responsibility gap in algorithmically mediated environments.13,15 When the system appears to decide, the locus of ethical intention becomes obscured, creating conditions for moral disengagement. This dynamic reinforces the structural nature of digital-relational harm by showing how algorithmic authority can reconfigure not only labour processes but also the distribution of moral accountability. Together, LPT uniquely accounts for the structural and organizational mechanisms of digital-relational harm, showing how algorithmic control, taskification, and precarity fragment relational continuity and constrain moral agency.
Relational ethics
Relational ethics emphasizes that ethical practice emerges through relationships characterised by trust, mutuality, attentiveness, and contextual understanding. 28 It begins from the premise that ethical practice is not an abstract principle or a set of rules, but a lived, situated, and relational engagement between persons. 28 Rooted in feminist ethics, narrative ethics, and contextual moral philosophy, relational ethics emphasises that moral life unfolds through trust, mutuality, attentiveness, and responsiveness; qualities that arise only within sustained, meaningful relationships.63,66 In this framework, ethical action is inseparable from the relational context in which it occurs. 63 Trust is not a static attribute but a co-created moral achievement; mutuality is not symmetry but a recognition of shared vulnerability; attentiveness is a moral stance that requires presence, curiosity, and openness; and contextual understanding is essential for discerning what care means in a particular moment for a particular person. Nursing practice is deeply aligned with this ethical worldview. The nurse–patient relationship is not merely instrumental but morally generative, producing the conditions for ethical discernment, shared decision-making, and compassionate care. 67 Ethical practice emerges not from detached reasoning but from relational attunement, that is, the ability to perceive, interpret, and respond to the needs of the Other within a specific context. 67 Relational ethics uniquely explains the ethical-responsiveness dimension of harm by highlighting how digital systems erode trust, mutuality, attentiveness, and contextual understanding. That is, digital systems increasingly redirect moral attention away from the patient and toward compliance with algorithmic prompts, documentation requirements, and performance dashboards, thereby displacing the relational attentiveness and mutual responsiveness that relational ethics identifies as the core of ethical nursing practice. An outcome of this is potentially more time on screen or managing machines and less face time with patients.68,69
Digital professionalism: Identity, visibility, and algorithmic mediation
Digital professionalism examines how digital infrastructures reshape professional identity and visibility. 70 In platformized nursing, identity is no longer grounded solely in clinical expertise or organizational membership but is increasingly mediated through components such as algorithms, ratings, data profiles, and digital traces.3,65,71 These systems determine how nurses are evaluated, often privileging metrics over relational competence or contextual judgement. As a result, professional identity becomes fluid, fragmented, and algorithmically curated, exposing nurses to misrecognition when their relational labour is rendered invisible or reduced to data points.3,65,71 Digital professionalism therefore illuminates how digital-relational harm manifests as identity destabilization, diminished professional autonomy, and the erosion of relational legitimacy within digital care environments.
Digital professionalism also reshapes professional accountability by shifting evaluative authority from relational judgement to algorithmic scoring systems. Reputational metrics such as punctuality scores, shift acceptance rates, behavioural analytics, and generated star ratings become proxies for professional competence, even though they capture only narrow fragments of nursing practice. These systems accumulate digital traces that follow nurses across platforms and organisations, creating durable reputational profiles that influence access to work, visibility, and perceived reliability. Crucially, relational competence in the areas of attunement, presence, contextual sensitivity, and ethical responsiveness remains largely invisible within these metrics, leading to a form of evaluative distortion where what is measurable becomes what is valued. As a result, digital professionalism exposes nurses to new forms of algorithmic accountability that privilege compliance with system-generated expectations over relational excellence. Together, digital professionalism uniquely exposes the identity and visibility dimension of harm by demonstrating how algorithmic visibility, ratings, and datafication destabilize professional identity and render relational labour invisible.
Integrating the theoretical and philosophical basis of digital-relational harm
As shown in Figure 1 and Table 1, digital-relational harm arises from the convergence of six philosophical and theoretical traditions that together reveal how digital infrastructures fundamentally reshape the relational, ethical, and ontological foundations of nursing practice. At its core, the mechanism of harm commences when digital systems reorganize the conditions under which personhood, moral responsibility, relational presence, and professional identity are formed and sustained. African relational ontology provides the deepest ontological grounding by showing that personhood is a communal-relational becoming, enacted through mutual recognition, shared vulnerability, and moral accountability. When digital infrastructures fragment continuity, weaken communal grounding, or reduce nurses and patients to data points, they disrupt the very processes through which persons come into being. This produces ontological disruption and diminishment, where the relational fabric that sustains human becoming is thinned or distorted. Theorizing digital-relational harm in nursing.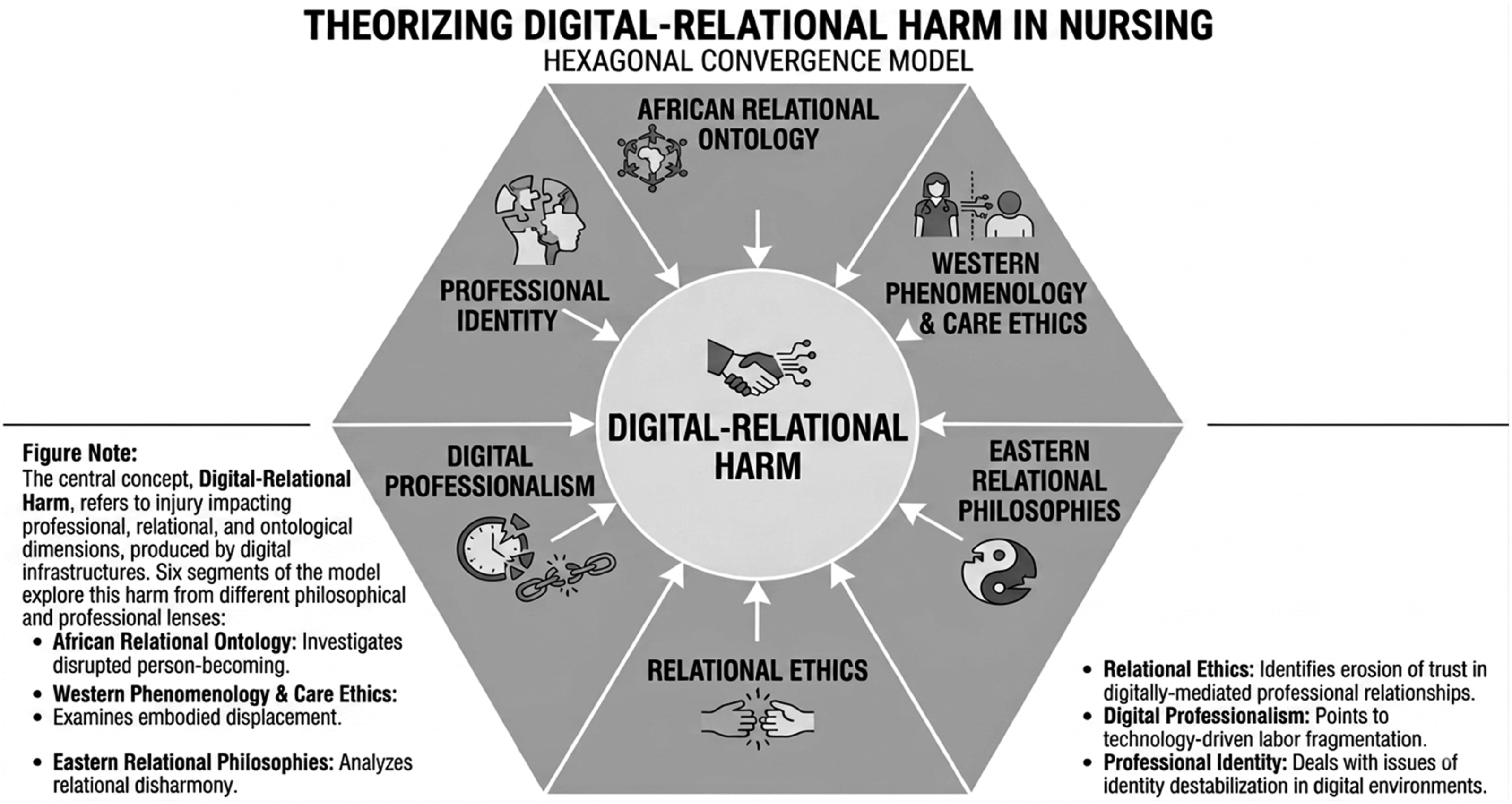
Western phenomenology, Levinasian ethics, and care ethics deepen this analysis by emphasizing that ethical and relational life emerges through embodied presence, intersubjective encounter, and relational attentiveness. Nursing practice depends on the immediacy of the face-to-face encounter, the lived body, and the subtle cues that arise in shared space. Digital mediation displaces these foundations by filtering perception, obscuring the face of the Other, and replacing relational cues with algorithmic prompts. The result is a form of moral and relational displacement, where the ethical immediacy and embodied attunement that define nursing are constrained or replaced by technological systems contributing to the developing of thin persons.
Eastern philosophical traditions (Confucianism, Buddhism, and Daoism) further illuminate how digital infrastructures disrupt interdependence, harmony, and relational attunement. Confucian ethics grounds moral life in relational propriety and harmonious roles; Buddhism frames the self as an interdependent process shaped through shared experience; Daoism emphasises attunement to relational flow and responsive action. Digital acceleration, standardization, and rigid workflows may disrupt these relational rhythms, producing relational disharmony and weakening the interdependent processes through which compassion, meaning, and moral understanding arise in nursing encounters. Labour Process Theory reveals how digital infrastructures restructure the process of labour itself through algorithmic control, surveillance, taskification, and precarity. Platformized nursing decomposes care into discrete, time-bound tasks, embeds continuous surveillance into workflows, and externalises risk onto workers. These dynamics fragment relational continuity, weaken professional autonomy, and erode the collective foundations of nursing.
Relational ethics brings these ontological and moral insights into the domain of ethical practice. It shows that ethical action is not abstract or rule-based but emerges through trust, mutuality, attentiveness, and contextual understanding. Digital systems fragment continuity, displace attentiveness toward documentation, and flatten contextual nuance through standardization. These disruptions generate ethical erosion, where the relational conditions necessary for moral discernment and compassionate care are undermined. Finally, digital professionalism shows how digital infrastructures reshape professional identity, visibility, and legitimacy. When relational labour becomes invisible or is reduced to quantifiable indicators, nurses experience identity destabilization and professional mis-recognition, further weakening the relational and ethical foundations of practice. While concerns about the invisibility and devaluation of relational labour have a long history in critiques of New Public Management, audit cultures, and managerialism, 72 digital infrastructures introduce qualitatively new mechanisms through which relational work is obscured or displaced.
Across these six traditions, a coherent mechanism becomes visible: digital-relational harm emerges when digital infrastructures reorganize the conditions that underpin nursing practice. At the ontological level, digital systems disrupt the processes of person becoming described by fragmenting continuity, weakening communal grounding, and reducing persons to data profiles. At the intersubjective level, they displace embodied presence and moral immediacy by filtering perception and mediating the face-to-face encounter. At the relational level, they disturb harmony, interdependence, and attunement through acceleration, standardization, and rigid digital workflows. At the ethical level, they erode trust, mutuality, and contextual responsiveness by redirecting attentiveness toward documentation and algorithmic demands. At the structural level, they fragment labour, continuity, and autonomy, as through algorithmic management, surveillance, taskification, and precarity. Finally, at the professional level, they destabilize identity, visibility, and recognition by privileging metrics over relational competence and rendering relational labour invisible. Together, these disruptions form a multi-layered socio-technical mechanism through which digital infrastructures produce relational, ethical, and ontological injury constituting digital-relational harm.
Digital-relational harm can be conceptualized as emerging when socio-technical systems fragment continuity, mediate recognition, distort visibility, or weaken the foundations through which nurses and patients become persons in relation to one another. Digital-relational harm is, thus, produced not through physical or psychological injury, but through structural and relational disruptions that undermine relational continuity (the ability to form sustained, trusting, therapeutic relationships), mutual recognition (being seen, valued, and acknowledged as a person), communal accountability (shared responsibility within teams and communities), ontological becoming (the relational processes through which personhood is cultivated), and professional identity integrity (the coherence of the nurse’s moral, relational, and professional self).
Digital-relational harm therefore names a category of injury that is ontological, structural, and relational. Digital-relational harm is ontological because it affects the modes of being of both nurses and patients. When digital infrastructures displace embodied presence, truncate narrative understanding, or reduce persons to data objects, they reshape how nurses and patients can exist in relation. The efficiency of digital systems notwithstanding, they may contribute to nurses experience a narrowing of their professional agency and moral identity as their relational judgement is subordinated to algorithmic logics. Patients experience a diminished sense of recognition and personhood when their stories, contexts, and relational histories are rendered invisible within digital systems. 73 Describing this harm as structural implies that it arises from the design and governance of digital systems, not from isolated errors or interpersonal misunderstandings. For example, when an algorithm consistently allocates nurses to unfamiliar wards, the resulting loss of relational continuity is not an accident, but a predictable outcome of a system optimised for efficiency rather than relationship-building. Similarly, when documentation templates omit space for narrative or contextual information, the erosion of relational understanding is built into the system’s architecture. Describing digital-harm being as relational indicates that the injury it produces is enacted within, and through, the relationships that constitute nursing practice. When digital systems mediate encounters, they disrupt the very relational processes through which nurses come to know patients and patients come to feel known. The harm is therefore relational because it alters the quality, depth, and integrity of the nurse–patient relationship itself, diminishing the relational fabric that sustains therapeutic trust, shared meaning, and moral accountability.
Distinguishing digital-relational harm from existing harm concepts
Distinguishing digital-relational harm from existing harm concepts.
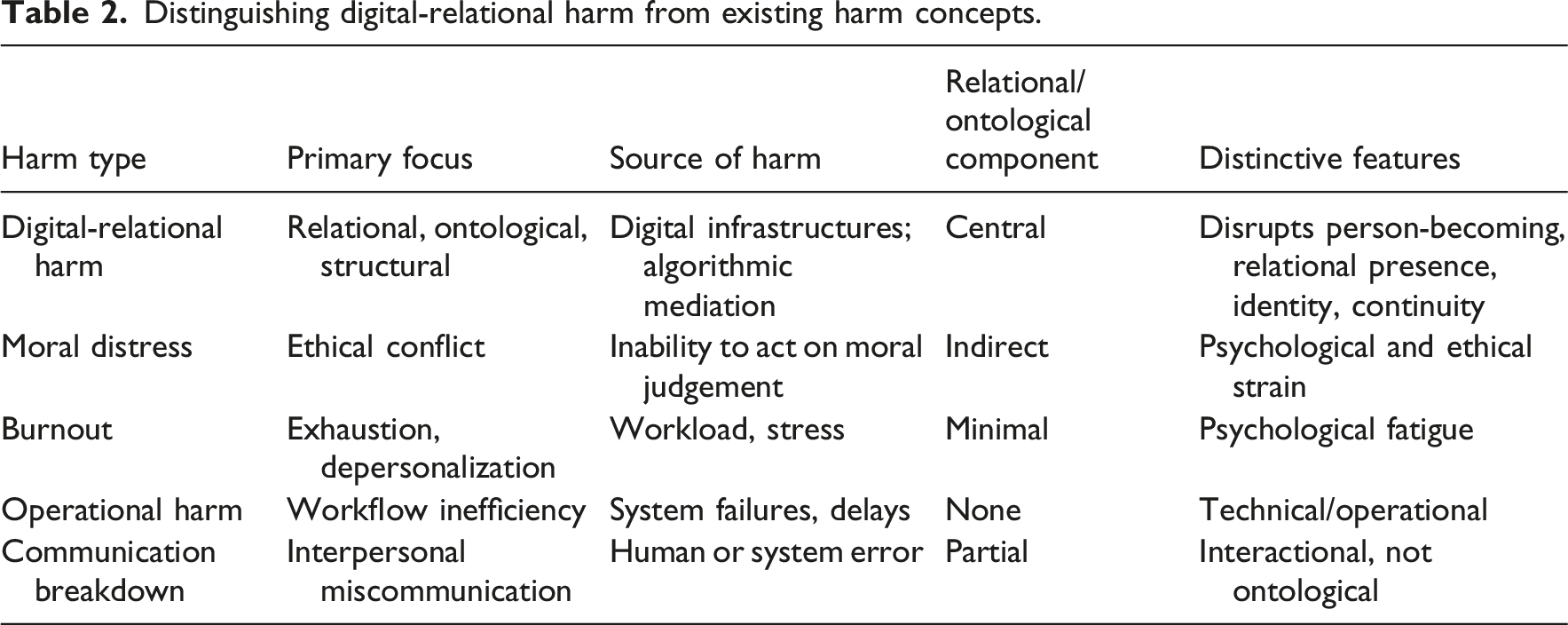
Second, digital-relational harm is structural before it is psychological, setting it apart from burnout or emotional exhaustion. Burnout describes an individual’s response to chronic stressors, 75 whereas digital-relational harm originates in the socio-technical organization of work: algorithmic governance, taskification, datafication, and platform precarity. These structural forces reshape how nurses encounter patients, colleagues, and institutions, producing relational injuries that cannot be reduced to individual coping or resilience.
Third, digital-relational harm is ontological before it is operational, distinguishing it from workflow inefficiencies or system usability problems. Operational harms arise when digital tools impede task performance. 76 Digital-relational harm, by contrast, occurs when digital systems disrupt the processes of person-becoming, relational presence, and moral agency. It is not the malfunction of a system that causes harm, but the way the system reorganizes the conditions under which nurses and patients come to know, recognise, and respond to one another as persons.
Finally, digital-relational harm is socio-technical before it is interpersonal, differentiating it from communication breakdowns or interpersonal conflict. It arises not from poor communication between individuals but from the ways digital infrastructures mediate visibility, recognition, and relational access. When algorithms determine who is seen, how they are evaluated, and what forms of relational labour are acknowledged or erased, harm is produced through socio-technical mediation rather than interpersonal failure.
Discussion
The concept of digital-relational harm reframes how nursing understands the consequences of digital transformation. Rather than viewing digital technologies as neutral tools that merely enhance efficiency or streamline workflow, this paper argues that digital infrastructures actively reshape the relational foundations of nursing practice which can potentially lead to a unique form of harm. 77 The synthesis presented here suggest that harm in digital environments is not limited to technical failures, privacy breaches, or moral distress; instead, harm emerges through the subtle, cumulative, and often invisible disruptions to the relational conditions that make nursing a moral and person-affirming practice. For example, when algorithmic staffing tools prioritize efficiency over continuity, nurses may rotate rapidly across wards, preventing the formation of therapeutic relationships. Over time, this fragmentation weakens not only relational depth but also the moral agency that emerges through sustained engagement with patients and colleagues. Similarly, when digital documentation systems prioritize standardized inputs, nurses may lose opportunities to record narrative or contextual information, diminishing the relational understanding required for ethical decision-making.
The mechanisms identified such as taskification, relational discontinuity, algorithmic governance, datafication, platform precarity, and AI-mediated recognition demonstrate that digital-relational harm is produced through socio-technical systems rather than interpersonal failures. These mechanisms reveal how digital infrastructures reorganize nursing work in ways that weaken relational depth, fragment team cohesion, and destabilise professional identity. Importantly, these harms accumulate over time, creating a cascade from structural to relational to ontological injury. 78 This layered understanding underscores the need for nursing scholarship to move beyond incident-based models of harm and toward systemic analyses of how digital environments shape the conditions of care.
The implications of this conceptualization extend across ethics, practice, education, leadership, workforce policy, and research. Ethically, digital-relational harm calls for a shift from traditional autonomy-based frameworks towards digital-relational ethics; one that recognizes that moral life in nursing is fundamentally constituted through relationships rather than individual choice alone. 79 This shift also reframes what it means for nurses to be digitally competent. It is no longer sufficient for nurses to know how to use technological artefacts or navigate digital systems. Competence must also include an awareness of the relational consequences that emerge from digital mediation 80 ; how algorithmic triage tools shape recognition, how documentation interfaces redirect attention, how platformized staffing fragments continuity, and how datafication reduces persons to thin digital profiles. Nurses must be able to identify when digital systems support relational practice and when they undermine it, and they must develop the ethical sensitivity to recognise subtle forms of relational erosion that may not be visible within traditional safety or quality metrics. 80 In this sense, digital-relational ethics expands the moral responsibilities of nurses: they become not only users of technology but stewards of relational integrity within increasingly digital care environments. Clinically, the notion of digital-relational harm highlights the need for relational safeguards in digital workflows and platformized staffing models. Educationally, it underscores the importance of preparing nurses to navigate AI-mediated interactions and algorithmic systems with relational awareness. What is more, nursing leadership plays a pivotal role in mitigating digital-relational harm by shaping organizational cultures, priorities, and governance structures through which digital systems are adopted. Nurse leaders must move beyond viewing digital transformation as a technical upgrade and instead recognise it as a relational and ethical redesign of care environments. At the policy level, it exposes gaps in workforce governance, particularly regarding algorithmic transparency and platform precarity. Digital-relational harm highlights the need for digital health policies that explicitly recognize relational integrity as a core dimension of quality and safety. Current policy frameworks often prioritise interoperability, efficiency, cybersecurity, and data governance. 81 These are all essential, but insufficient. For research, digital-relational harm opens a new agenda focused on measuring relational harms, examining cross-national variations, and evaluating interventions that protect relational integrity.
This paper also contributes to broader debates about digital transformation in health systems. While digital technologies are often framed as solutions to workforce shortages, inefficiencies, or rising demand, the concept of digital-relational harm reveals that these technologies can simultaneously undermine the relational foundations that sustain high-quality care.3,32 This tension suggests that digital innovation must be evaluated not only for its operational benefits but also for its relational and ontological consequences. 82 Without such evaluation, health systems risk adopting technologies that inadvertently erode the very conditions that make nursing effective, ethical, and humanising.
While digital-relational harm highlights structural injuries, it is equally important to recognise nurses’ capacity for relational agency within digital constraints. Drawing on the Buddhist Middle Way (Majjhimāpaṭipadā), 83 nurses can navigate between uncritical technological optimism and total rejection of digital systems. Through Viriya (energetic effort) 84 and Paññā (practical wisdom), 85 nurses often enact subtle forms of resistance such as pausing to make eye contact despite documentation demands, re-ordering tasks to preserve relational presence, or creatively working around rigid interfaces to honour patient narratives. These micro-practices demonstrate that even within algorithmic environments, nurses can actively reclaim ethical space and sustain relational integrity.
Finally, digital-relational harm positions nursing as a critical voice in shaping digital futures. Because nursing is grounded in relational practice, the discipline is uniquely equipped to identify and articulate the relational consequences of digital transformation. By naming and theorizing digital-relational harm, this paper provides a conceptual foundation for nurses, policymakers, and technologists to design digital systems that honour relational integrity rather than undermine it. In doing so, it contributes to a broader movement toward socio-technical design that centres human relationships, communal belonging, and personhood.
Strengths and limitations
A key strength of this paper lies in its theoretical originality. By synthesizing African relational ontology, Western phenomenology and care ethics, Eastern relational philosophies, relational ethics, Labour Process Theory, and digital professionalism, the manuscript offers a conceptual framework that reframes digital transformation as a relational and ontological concern rather than a technical or operational issue. This breadth allows the concept of digital-relational harm to illuminate forms of injury that remain invisible within existing models of harm, ethics, and workforce analysis. Another strength is the paper’s timeliness and relevance. As digital infrastructures increasingly mediate nursing work, the manuscript offers a vocabulary and analytic lens capable of naming emerging harms that practitioners and scholars are already encountering but lack conceptual tools to articulate. However, the paper also has limitations. The breadth of philosophical traditions, while a strength, introduces conceptual density that may challenge readers unfamiliar with ontological or relational theory. A second limitation is that the analysis is primarily conceptual, with limited empirical grounding. While this is appropriate for a theoretical paper, it means the framework has not yet been tested across diverse digital environments or cultural contexts. The scope of the concept is necessarily limited by its theoretical and philosophical orientation. While digital-relational harm is grounded in six robust traditions, it remains a conceptual framework that has not yet been empirically tested. The applicability, salience, and manifestations of digital-relational harm require empirical validation across diverse clinical settings, countries, platform models, and digital health systems. Different labour structures, regulatory environments, and cultural understandings of relationality may shape how digital-relational harm emerges in practice. As such, the concept should be understood as a generative theoretical foundation that invites empirical examination rather than a fully operationalised model.
Future theoretical directions
Calls for relationally oriented ethics are well-established in nursing ethics,66,86 feminist care ethics, 87 and relational autonomy scholarship. This paper builds on that foundation by showing how digital infrastructures introduce new relational and ontological vulnerabilities that existing frameworks have not yet theorised. The concept of digital-relational harm opens a wide horizon for future theoretical development in nursing and allied fields. Because digital infrastructures continue to evolve rapidly, the discipline requires new conceptual tools capable of analysing how relational, ethical, and ontological conditions are reshaped within digital care environments. As a starting point, there is a need to build further on existing digital-relational ethics framework that moves beyond autonomy-centred frameworks and foregrounds relational integrity, mutual recognition, and communal accountability in digital systems. 88 Such a framework would examine how digital infrastructures can be designed to support, rather than erode, the relational foundations of nursing practice.
Future scholarship in the discipline of nursing should also theorize algorithmic visibility and misrecognition as central mechanisms of harm. As digital systems increasingly determine who is seen, how they are evaluated, and what forms of labour are acknowledged, nursing requires conceptual tools to understand how recognition is mediated, distorted, or withdrawn through algorithmic processes. Together, these directions position digital-relational harm not only as a conceptual tool for analysing current challenges but as a foundation for a broader theoretical agenda that reimagines how nursing engages with digital transformation. By advancing these lines of inquiry, the discipline can shape digital futures that honour relational life rather than diminish it.
Future research/empirical direction
Future research should explore how digital-relational harm can be empirically identified, measured, and evaluated across diverse clinical and cultural contexts. Methodological priorities include developing relational-ontological indicators of harm; conducting ethnographic studies of algorithmic mediation in clinical environments; examining cross-cultural variations in relational disruption; and designing evaluative frameworks that assess how digital systems support or undermine relational integrity. Because digital-relational harm manifests through disruptions to recognition, continuity, presence, and relational integrity, empirical work must move beyond traditional metrics of efficiency or satisfaction. Qualitative methodologies such as ethnography, digital ethnography, and phenomenology are well-suited to examining how digital infrastructures reshape everyday encounters, embodied attunement, and moral agency across settings. Mixed and multi-method designs could integrate these relational insights with quantitative indicators such as continuity metrics, relational workload measures, or indicators of algorithmic visibility. Such work will be essential for informing policy, governance, and design strategies that safeguard the relational foundations of nursing.
Future educational direction
Future work can explore how nursing education can cultivate the ethical, relational, and critical capacities required to recognise and respond to digital-relational harm. Digital competence can no longer be limited to technical proficiency or functional literacy. Instead, curricula at undergraduate and postgraduate levels must integrate digital-relational ethics, preparing nurses to identify how digital infrastructures shape recognition, continuity, presence, and moral agency. This includes developing pedagogical approaches that foreground relational awareness in digitally mediated encounters; critical reflection on datafication, algorithmic visibility, and platform logics; ethical sensitivity to subtle forms of relational erosion; and the capacity to advocate for relational integrity in digital environments.
Design direction
Future work must focus on the design of digital infrastructures that actively support, rather than erode the relational fabric in nursing practice. This requires moving beyond user-centred design toward relational-centred design, where the primary design question becomes: How does this system shape the relationships that make care possible? This calls for collaboration between designers, engineers, and clinicians to ensure that digital systems are not evaluated only for usability or efficiency, but for their capacity to sustain the relational, ethical, and ontological foundations of nursing practice.
Policy direction
Digital-relational harm highlights the need for digital health policy frameworks that explicitly recognise relational integrity as a core dimension of quality and safety. Policies must also address the governance of platformized nursing work, including protections against algorithmic precarity, relational fragmentation, and the reduction of nurses and patients to thin digital profiles. A relationally attuned policy framework would position relational integrity as a non-negotiable ethical standard in digital health governance.
Conclusion
Digital-relational harm reframes digital transformation in nursing as a relational and ontological challenge rather than a purely technical or operational one. By drawing together six philosophical and theoretical traditions, this paper demonstrates that digital infrastructures reshape the conditions under which personhood, ethical responsiveness, relational presence, and professional identity are formed and sustained. Recognising these dynamics enables a more precise and ethically grounded understanding of how digital systems affect nursing practice.
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.