
Abstract
Background
Financial toxicity imposes a heavy burden on older cancer patients and their families. In Confucian societies, cultural norms fundamentally shape how financial burden is experienced, communicated, and managed—caregivers feel duty-bound to bear treatment costs, while older patients often conceal financial concerns to avoid burdening their families. This renders financial toxicity a dyadic, relational phenomenon rather than a purely individual economic stressor. Yet how patients and caregivers together experience and cope with this culturally embedded stress remains poorly understood.
Aims
To investigate the experiences and coping mechanisms of older cancer patients and their caregivers regarding financial toxicity from a dyadic perspective.
Design
A descriptive qualitative study was conducted from May to August 2025 with 12 purposively sampled older cancer patient-caregiver dyads from two tertiary cancer hospitals, using semi-structured, in-depth face-to-face interviews. Data were analyzed following Braun and Clarke’s thematic data analysis guide.
Ethical Considerations
The study protocol was approved by the ethics committee and adhered to ethical principles.
Findings
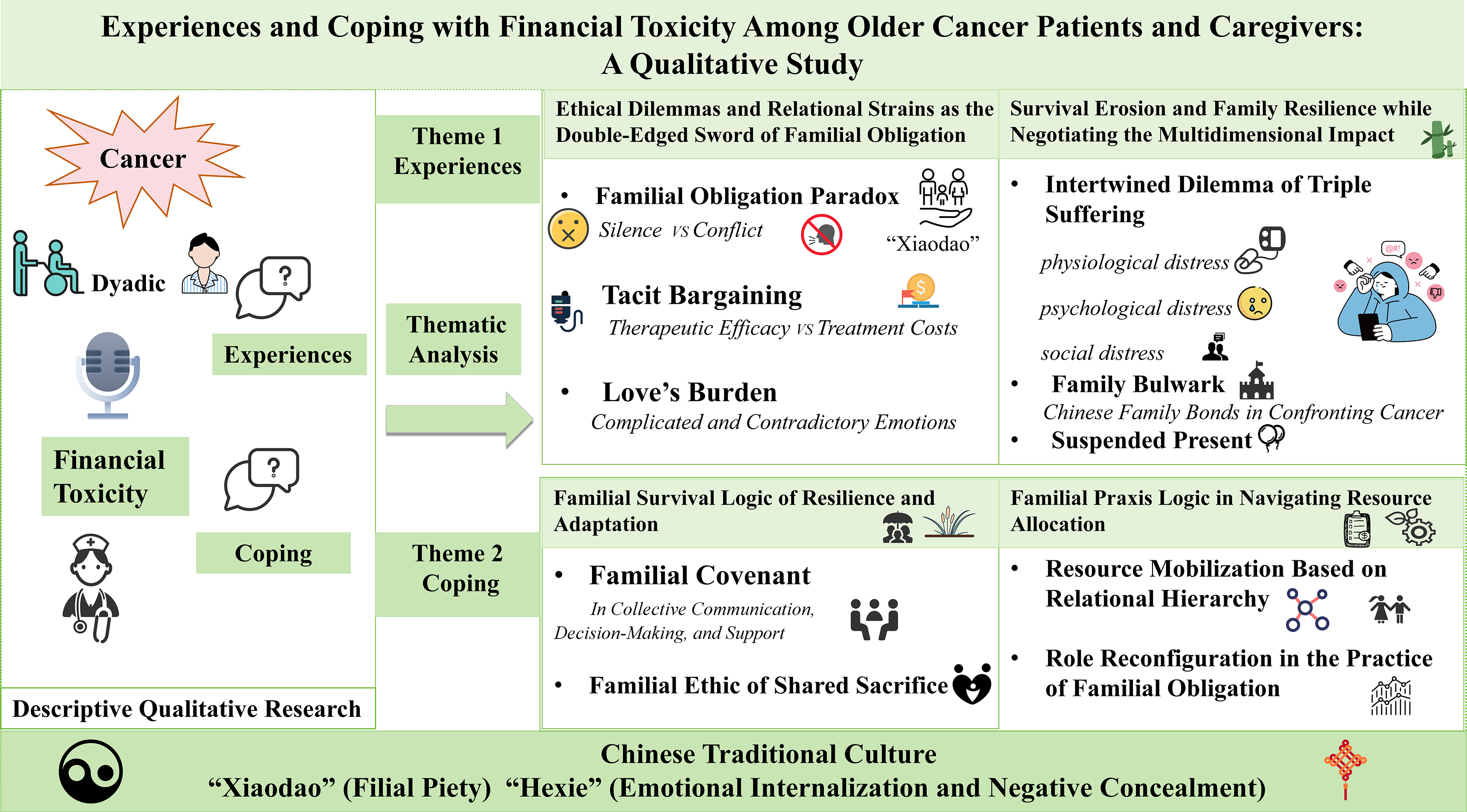
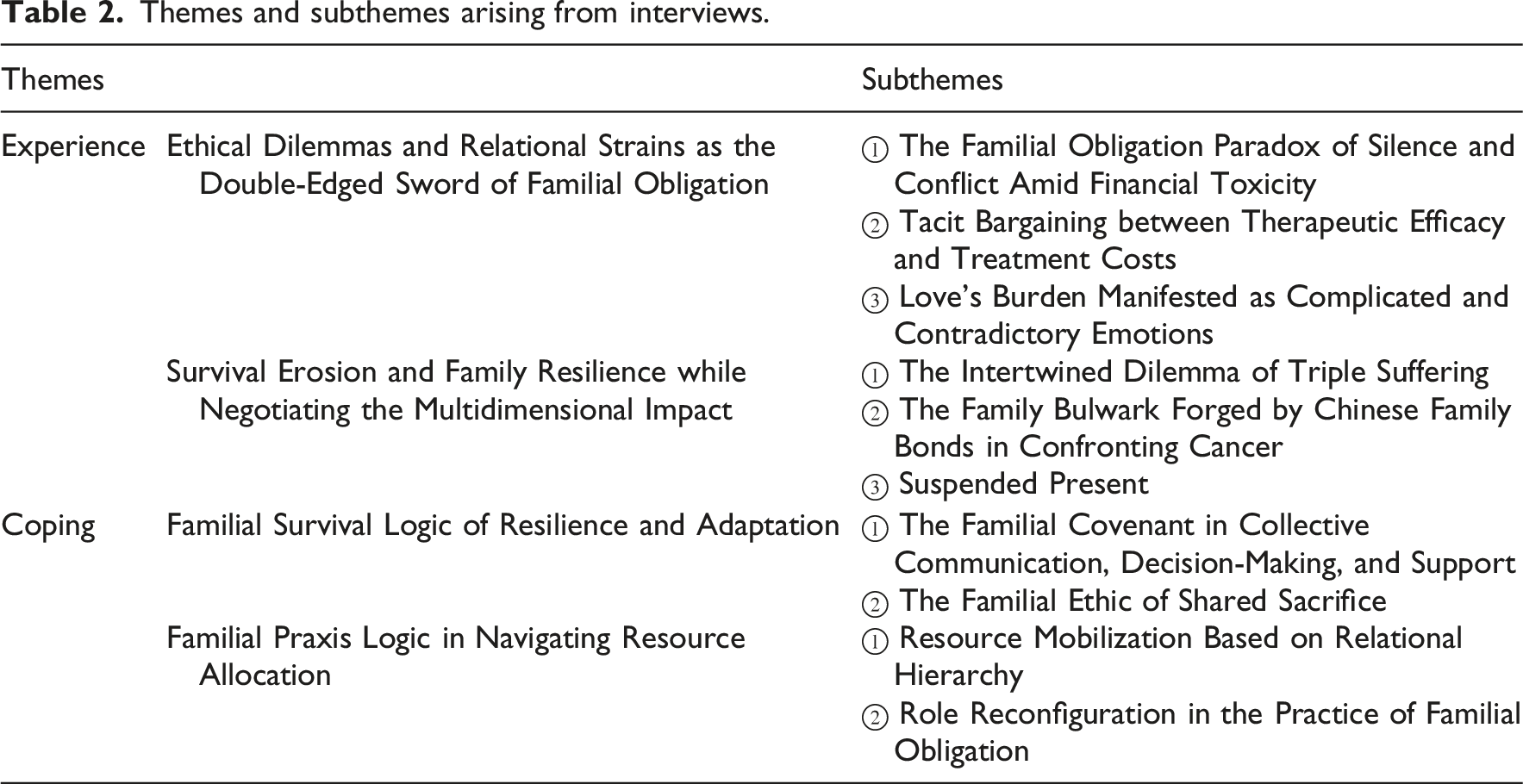
Four themes comprising ten sub-themes were extracted and organized into two overarching domains. Regarding the experience of financial toxicity, two themes emerged: (1) ethical dilemmas and relational strains as the double-edged sword of familial obligation; (2) survival erosion and family resilience while negotiating the multidimensional impact. Regarding coping mechanisms, two themes emerged: (3) familial survival logic of resilience and adaptation; (4) familial praxis logic in navigating resource allocation.
Conclusion
Rooted in traditional Chinese family culture, where Confucian ethics predominate, financial toxicity imposes a shared burden on patients and caregivers, creating a family-level crisis. Healthcare providers should recognize its profound impact on both caregivers and families. Given the confluence of rapid population aging, family-centered care expectations, and insurance gaps in China, targeted interventions should be developed through a multi-tiered approach, helping cancer-affected families mitigate financial toxicity and improve quality of life.
Introduction
Cancer persists as a preeminent global health challenge, contributing substantially to morbidity and mortality worldwide. 1 By 2040, patients aged 65 years and older will comprise 69% of all new cancer diagnoses.2,3 Older cancer patients, due to physiological decline, a higher prevalence of comorbidities, and cognitive impairments, often require more complex and protracted treatments,4,5 thereby exposing this population to substantial financial burden. The financial burden of cancer, termed “financial toxicity,” has emerged as a critical issue in oncology research, 6 which encompasses both the objective economic strain and the subjective psychological distress resulting from cancer-related expenses. This phenomenon not only undermines patients’ quality of life but also imposes significant strains on healthcare systems.7,8 In China, a national multi-site study reported that approximately 40% of cancer patients experience severe financial toxicity, 9 with out-of-pocket costs frequently exceeding 40% of household income, a threshold considered catastrophic by WHO standards. 10
Notably, a cancer diagnosis reverberates throughout the entire family system, altering roles, straining communication, and disrupting established patterns of functioning. In China, traditional family values emphasize intergenerational support, 11 meaning the financial and emotional repercussions on older cancer patients and their family caregivers are especially pronounced. However, existing research has largely examined either patient costs or caregiver burnout in isolation, overlooking their interactive nature. To address this significant knowledge gap, this study explores the lived experiences of older cancer patients and their family caregivers, along with the coping strategies they employ to manage financial toxicity, from a dyadic perspective. By focusing on the patient-caregiver dyad as the core relational unit, this study aims to clarify how cultural norms (e.g., filial piety and spousal duty), structural factors (e.g., healthcare costs and insurance limitations), and relational dynamics (e.g., role negotiation and communication patterns) jointly shape experiences and coping responses, thereby informing culturally tailored interventions to support the dyad’ s collective quality of life.
Background
Among older cancer patients, financial vulnerability is exacerbated by age-related comorbidities, diminished functional capacity, increased susceptibility to treatment-related complications, and a lack of sustainable income sources. 12 In the United States, older cancer survivors face substantial economic burdens—for example, annual out-of-pocket costs averaging $18,860 (USD) for colorectal cancer, $14,351 (USD) for breast cancer, and $16,851 (USD) for prostate cancer. 13 In China, although direct comparative data are limited, multicenter data from a national survey across twelve hospitals in three Chinese provinces with distinct economic gradients reported a strikingly high financial toxicity prevalence of 82.6%, with 40.9% of the 1,208 patients presenting with severe financial toxicity. 9 Furthermore, in China, despite near-universal basic medical insurance coverage, reimbursement limitations for innovative therapies, substantial non-medical costs (transportation, accommodation, caregiver income loss), and cultural expectations of family-funded care create distinct patterns of financial vulnerability. 14 Consequently, financial toxicity is particularly severe among Chinese cancer patients, especially older adults, posing a profound burden on both patients and their caregivers.
Caregivers, whether spouses or adult children, frequently experience declines in their own physical and mental health, social isolation, and significant economic vulnerability. 9 Studies grounded in family systems frameworks demonstrate that financial stress compounds cancer-related distress, potentially leading to maladaptive coping patterns, reduced family cohesion, and diminished communication quality. 15 Family members may forego their own medical care, sacrifice basic necessities, and deplete savings intended for education or retirement, patterns that are observed across healthcare contexts but intensified in cultures where family-funded care is the normative expectation. 15
Rooted in family systems theory, the dyadic perspective provides a comprehensive framework for understanding how illness affects both patient and caregiver, 16 with each individual’s behaviors, emotions, and resources shaping the other’s adaptation.17,18 Within this framework, traditional Chinese culture, grounded in Confucian ethics, introduces distinct relational expectations that shape how financial toxicity is experienced. Filial piety (“Xiao Dao”) and familial collectivism create a moral imperative for family-funded care, leading families to confront cancer as a unified entity.19,20 While filial piety most directly binds adult children, spousal caregivers are similarly governed by expectations of lifelong mutual duty, a related cultural logic that equally shapes dyadic responses to financial strain. Therefore, patients’ illness directly affects the caregiver’s financial stability and well-being. 21 This interdependence confirms that financial toxicity is a dyadic phenomenon, in which stressors and coping strategies of patients and caregivers are closely intertwined. However, few studies have adopted this perspective to examine how patients and caregivers jointly navigate these challenges, particularly within Confucian contexts that prioritize family cohesion over individual needs. To bridge this gap, the present study aims to elucidate how cultural norms, structural factors, and relational dynamics jointly shape experiences and coping by analyzing dyadic interactions, with the goal of advancing understanding of financial toxicity and informing culturally tailored interventions that support the dyad’s collective quality of life.
Methods
Study design
To gain a comprehensive understanding of dyadic coping experiences, this study utilized a descriptive qualitative method, which is particularly suited to capturing detailed, first-hand accounts of under-explored phenomena. 22 The study was reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist.
Participants and sampling procedure
Dyads of older cancer patients (≥ 60 years, pathologically diagnosis) and their unpaid caregivers (≥18 years, familiar with the patient’s condition) were recruited via purposive sampling from two tertiary hospitals between May and August 2025. All patients were receiving usual oncological care within the public hospital system, consisting of standardized, guideline-concordant therapies including surgery, chemotherapy, radiotherapy, immunotherapy, and targeted therapy as clinically indicated. No participants were receiving experimental, off-label, or non-standard “heroic” measures. Participant selection ensured variation in demographics and clinical characteristics. Individuals with cognitive or mental disorders were excluded.
Data collection
Face-to-face, in-depth interviews (30–45 min) were conducted in Mandarin by the first author in a quiet reading room. Interviewer (RN and MNS) had qualitative research training. Interviews were audio recorded.
The interview outline was developed on the previous qualitative studies examining financial toxicity and family caregiving in cancer populations. Specifically: Question 1 (cancer/treatment experience) was adapted from Lu et al.'s work on family caregiver experiences in China 23 ; Questions 2–3 (financial situation and impact) drew from Yabroff et al.'s framework for assessing financial hardship domains 24 ; and Questions 4–5 (coping strategies and support needs) were informed by Yuan et al.'s study of financial toxicity interventions. 25 Standardized probes were prepared to deepen responses, including “Can you tell me more about that?”, “How did that make you feel?”, “What did you do in response?”, and “Can you give me a specific example?” To ensure conceptual understanding, the term “financial toxicity” was introduced and explained before each interview, with “financial burden” or “economic strain” used as alternative phrasing when necessary.
Data collection continued until thematic saturation was achieved, that is, the point at which no new codes or themes emerged from subsequent interviews and further data collection would be unlikely to yield additional insights. 26 An iterative process of concurrent data collection and analysis enabled continuous assessment of saturation, with the research team meeting weekly to review emerging findings and determine when informational redundancy had been reached. Saturation was confirmed after 12 dyads, consistent with established guidance that saturation in qualitative studies with relatively homogeneous samples typically occurs within 6–12 interviews. 26
Data analysis
All interview records were transcribed verbatim to Chinese and translated to English by the first researcher who is bilingual. Braun and Clarke’s thematic data analysis guide (2006) 27 guided the process. Two researchers (the first researcher and the last researcher) independently read and reread all the transcripts for immersion in the data. Key quotes were highlighted, and initial codes were developed based on participants’ verbatim statements. Codes were grouped according to similarity into subthemes and then themes based on common threads throughout the data. Any disagreement or contested theme/subtheme was discussed within the team with all researchers until consensus was reached. Interview transcripts were returned to participants for comments and further clarifications.
Rigor
The rigor of this study was enhanced by applying Guba and Lincoln’ s (1994) criteria, 28 including credibility, transferability, dependability, and confirmability. To ensure the credibility of the study, peer debriefing was employed, and a comprehensive audit of the transcripts, sub-themes, themes, and findings was conducted under the supervision of the corresponding author. Transferability was reinforced through the provision of a thick, contextualized description of the research setting, participant characteristics, and methodological procedures, thereby enabling readers to evaluate the potential applicability of the results to other similar contexts. Dependability was strengthened via member checking, whereby a summary of the identified themes and sub-themes relevant to participants’ experiences, accompanied by illustrative interview excerpts, was shared with participants for verification. Furthermore, two independent researchers with expertise in oncology nursing—who were not substantially involved in the primary data analysis—reviewed the thematic structure to verify its faithful representation of the data. Finally, confirmability was established through reflexive practice by all authors. Throughout data collection, the interviewer maintained a neutral, nonjudgmental presence, bracketing personal assumptions about filial piety and financial sacrifice to minimize interviewer bias. During analysis, all team members maintained reflexive journals documenting how their own cultural backgrounds and clinical experiences might shape data interpretation. The research team held regular debriefing sessions to critically examine emerging interpretations and challenge potential biases. This reflexive practice ensured that the findings remained grounded in participant accounts rather than researcher preconceptions.
Ethical considerations
Ethical approval for this study was approved by the Ethics Committee (NCC2025C-042) of National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College. Written informed consent was obtained from all participants, who were assured of confidentiality and the right to withdraw without penalty at any time.
Results
Demographic characteristics
Characteristics of older cancer patients and their caregivers (N = 12).
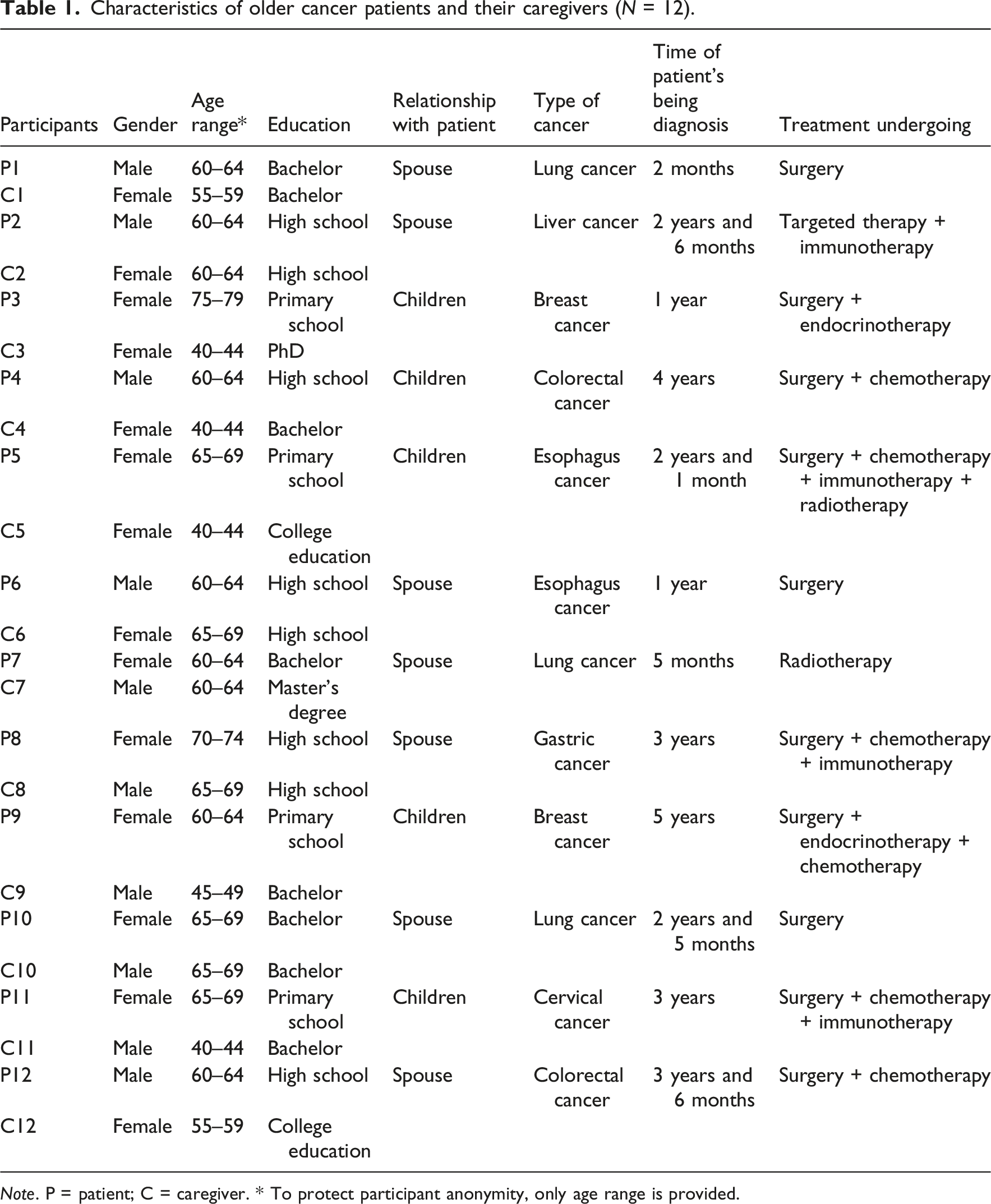
Note. P = patient; C = caregiver. * To protect participant anonymity, only age range is provided.
Themes
Themes and subthemes arising from interviews.
Theme 1: Ethical Dilemmas and Relational Strains as the Double-Edged Sword of Familial Obligation
This theme elucidates how financial toxicity creates ethical dilemmas and strains within traditional Chinese families, older patients may silently endure hardships and delay treatment, while caregivers make deep personal sacrifices out of a strong sense of filial duty. This dynamic leads to a pattern of “tacit bargaining” over resources, where avoided communication widens emotional gaps.
The Familial Obligation Paradox of Silence and Conflict Amid Financial Toxicity
This pattern acts as a critical mechanism through which financial toxicity manifests within patient-caregiver dyads. Cultural norms, particularly the Chinese ethos of familial devotion and the mutual desire for protection, are deeply rooted in society but paradoxically create relational strain. A key manifestation is mutual avoidance, where patients often conceal financial concerns and illness severity, while caregivers hide the true cost of treatment, each attempting to shield the other from distress. As one caregiver daughter explained: “We never tell mom the real price of the targeted therapy. We say it’s mostly covered by insurance. She would refuse treatment immediately if she knew we are using our savings” [C8].
Conversely, older patients suppress their preferences, remaining silent about desires for conservative treatment to avoid appearing ungrateful or burdening their children. One patient confessed, “I don’t want this expensive medicine, but how can I say that? My children have gone through so much trouble. I just stay silent” [P5].
This avoidance inevitably brews underlying tension, which surfaces as open conflict when critical decisions arise. The clash emerges between the patient’s desire to conserve family resources and the caregiver’s imperative to fulfill filial duties at any cost. “We had a huge argument when I proposed selling their apartment. He [the father] flatly refused. It was the first time I saw him so angry”[C7].
Tacit Bargaining between Therapeutic Efficacy and Treatment Costs
Guided by filial piety and tempered by low efficacy expectations due to comorbidities, older patients frequently favor family financial security over optimal care to avoid burdening their children. A central theme thus emerged: the continual, strained negotiation between therapeutic efficacy and treatment costs. Such a dilemma fosters a silent divergence within the dyad. This fundamental tension between safeguarding the family’s socioeconomic future and pursuing all clinical avenues constitutes the core of dyadic distress within financial toxicity. “Dad refused the costly targeted therapy. ‘My old body isn’t worth it’, he said, choosing chemo to spare us debt” [C4]. “The doctor said this new treatment could give me a few more months, but it costs as much as my grandson's entire university tuition. How can I take that from him?” [P4]. A caregiver son revealed this tension: “We cannot put a price on my father's life. I know he worries about the money, but what is money for if not for this? I would rather be in debt and know we tried everything” [C5].
Love’s Burden Manifested as Complicated and Contradictory Emotions
The experience of financial toxicity is deeply permeated by complex and contradictory emotions, profoundly shaped by the dual pressures of filial piety and intergenerational responsibility. Older patients and their caregivers become entangled in a heavy burden of guilt, shame, and ambivalence, where every decision is fraught with moral and emotional conflict. Patients grapple with the tension between self-preservation and altruism. “My son says money is not a problem…I was supposed to help with my grandson’s education, not drain their savings. Sometimes I think stopping treatment would free them. But then I feel guilty for giving up; it's like spitting on their love. I am trapped between being a good father who protects his family and a sick man who wants to live” [P12].
This poignant statement captures the core conflict between a deeply ingrained desire to protect the family’s legacy and a fundamental will to survive. Simultaneously, caregivers are burdened by a parallel, yet contrasting, set of contradictions. They perform filial devotion while privately confronting financial terror. A daughter expressed this inner turmoil: “As the only daughter, you must do everything. So, we chose aggressive treatment. But between the bills and my own family’s needs, I'm being crushed. I feel ashamed for calculating the cost, but the thought of leaving my own family with nothing is terrifying. I am performing the role of a devoted daughter, while inside, I’m terrified of the financial abyss.” [C11]
Caught between filial duty and parental responsibility, caregivers are burdened by financial shame. The patient-caregiver dyad is locked in a silent symbiosis. Love is expressed through financial sacrifice, which in turn breeds unspoken resentment and distress.
Theme 2: Survival Erosion and Family Resilience while Negotiating the Multidimensional Impact
This theme captured the dual pressures of systematic depletion and fragile adaptive under financial toxicity. “Survival erosion” manifests through three interconnected dimensions: the relentless depletion of economic assets, the physical exhaustion from prolonged caregiving coupled with treatment side effects, and the psychological toll of shattered future planning. Families existed in a “suspended present,” deferring aspirations to handle immediate crises.
The Intertwined Dilemma of Triple Suffering
Financial toxicity constitutes a systemic dyadic crisis, where tightly interlocked physiological, psychological, and social distress concurrently and mutually reinforce one another within patient-caregiver dyads, creating a cohesive yet destructive feedback loop.
Physiologically, patients’ cost-driven care compromises, such as forgoing medications, directly harm their health. “I had serious sleeping disorder even before cancer. Now, worrying about costs makes my anxiety and stressed, and I can’t sleep well” [P2]. “Truth is, I haven’t been in the best health myself. I’ve had hypertension for years and take medication regularly. Before, my retirement income could basically cover it. But after he got sick—with the chemotherapy, radiation, and then the surgery—the medical bills piled up all at once. There are times I get so worried that I can’t rest properly, and when I don't rest well, my blood pressure shoots up” [C5].
Psychologically, the sustained financial strain internalizes distress within the dyad, leading to shared feelings of guilt, depression, frustration, and anxiety. This emotional burden is compounded by the mutual influence of psychological distress between patients and caregivers throughout the illness trajectory. “I feel so guilty. I was supposed to enjoy my retirement and help my kids, but now I’m a burden on them” [P3]. “The pension and savings of my parents aren't really enough, so of course we children have to shoulder the financial responsibility. But I still have two kids in secondary school—that's another big financial demand. The financial strain is really heavy, and it’s making me very anxious… (sighs)” [C7].
Financial strain induces social contraction for both patients and caregivers, as the unaffordability of social activities deepens their isolation. A sentiment captured by one patient’s expression of “sitting at home, feeling like a burden.” This social isolation exacerbates psychological distress, which in turn intensifies physical suffering. “My work performance has dropped. I keep thinking about my mom’s treatment costs and her condition. I can’t focus” [C5]. “I’ve had to stay at the hospital to care for my father because my mother is also elderly. Because of this, I had no choice but to request an extended leave from my workplace”[C8]. “I was supposed to retire next year but then came the cancer diagnosis. I had no choice but to take early retirement. Compared to retiring at the normal age, my pension is significantly less. What's more, I likely won't be able to earn anymore in the future” [P4].
The Family Bulwark Forged by Chinese Family Bonds in Confronting Cancer
“Familial Fortress” captures how Chinese families collectively mobilize to protect older cancer adults amid vulnerabilities like multimorbidity and caregiver risks. It functions as a coordinated resource-pooling system to alleviate financial toxicity from prolonged treatment, with caregiving strategically shared to prevent caregiver collapse. This collective endeavor buffers against the compounded “survival erosion” in later life, transforming a clinical crisis into a managed familial process that sustains the dignity while navigating intergenerational dynamics. “Coordinating my father’s chemo schedule with my own work and my mother’s frailty is a complex logistics. We function as a relay team, ensuring constant coverage despite the immense personal cost” [C2]. “The financial planning is daunting. We siblings collectively contribute to cover the targeted therapy costs, understanding that our retired parents' savings alone could not withstand this strain” [C9]. “The greatest fear was becoming a burden. But my daughter’s daily visits and my grandson's simple help with my smartphone reinforced that I remain a valued part of our family, not just a patient” [P6].
Suspended Present
Beyond direct costs, financial toxicity casts a long shadow of uncertainty that paralyzes dyadic mental well-being. This pervasive insecurity encompasses the illness trajectory, escalating treatment expenses, and caregiver’ s diminishing capacity to provide long-term support. Patients express a deep-seated fear of depleting finite family resources; a sentiment highlights how financial uncertainty forcibly contracts their temporal horizon and extinguishes future planning. As one patient shared, “We talk about ‘saving for a rainy day’, but this feels like a permanent storm. How many more ‘rainy days’ can our savings cover? I dare not think about next year. We have stopped planning altogether” [P4].
For caregivers, this uncertainty transforms into a constant, draining anxiety about sustaining the care effort. “My greatest fear is not today’s bill, but the unknowable total at the end. I am living in a state of permanent alert, with no finish line in sight” [C6].
This continuous calculation against an unknown future imposes a significant psychological burden, leaving the dyad navigating a precarious present with no clear path forward, thereby compounding the distress of the illness itself.
Theme 3: Familial Survival Logic of Resilience and Adaptation
Influenced by traditional values, Chinese families respond to the financial toxicity of cancer through a “family survival logic”—a collective, strategic system of prioritization and resource allocation that emerges under pressure. This is not merely reactive but profoundly shapes illness narratives, redefines roles and responsibilities, and ultimately determines the family’s long-term trajectory through cancer.
The Familial Covenant in Collective Communication, Decision-Making, and Support
The “familial covenant” is a culturally embedded pact that coordinates collective action against adversity, such as cancer-related financial strain. It operates through communication together, shared decision-making, and mobilized support, rooted in filial piety and intergenerational duty. This moral framework transforms the family into a resilient, cohesive unit, distinguishing Chinese illness coping from more individualistic models. “My children and I talk about every expense. They want the best for me, and I don't want to waste their hard - earned money. We find a balance” [P6]. “We are a family. We discussed and decided to use a more cost - effective treatment plan that still has good results” [C2]. “I told my son to be honest about the costs. We will figure it out together. After all, family is more important” [P5].
Chinese patient-caregiver dyads often engage in active to co-regulate economic stress. Guided by a family-centered ethos, they collaboratively mitigate financial worries through mutual reassurance and joint decisions, thereby buffering the psychological burden of financial toxicity. “My husband was feeling so guilty about the cost, so I told him, ‘Your well-being is the most important. The rest we can figure out side-by-side’. Now, we face every financial decision as a team, not as his burden alone” [C4].
The Familial Ethic of Shared Sacrifice
Faced with the long-term financial burden of cancer care, families demonstrate remarkable adaptability, proactively reducing non-essential treatment and daily living expenses. Patients frequently scrutinize the necessity of supportive treatments in order to prioritize core treatments, especially when managing multiple chronic conditions. “The oxygen therapy seems not very necessary for me now. I can save that money for more important medications. I have diabetes and heart problems too, so every penny counts” [P10]. “Daytime pain is bearable. I don't want to use the painkiller often. I have to save money for my treatment in the long run” [P5].
Concurrently, caregivers implement significant adjustments to household expenditures, transforming daily living patterns to redirect funds toward medical care. A caregiver illustrated this shared sacrifice: “We used to eat out once a week. Now, we cook at home. Every little bit of savings helps with my husband’s treatment” [C6].
This collective belt-tightening across both medical and domestic spheres represents a pragmatic, dyadic coping strategy aimed at preserving the family’s financial resilience for the challenging treatment journey ahead.
Theme 4: The Logic of Familial Praxis in Navigating Resource Allocation
Resource Mobilization Based on Relational Hierarchy
To sustain cancer treatment, families systematically mobilize a hierarchy of limited resources. This typically follows a sequence: first depleting personal savings and pensions, then seeking support from the immediate family, and ultimately turning to loans from relatives and to social capital for practical aid. This layered process highlights the profound financial strain of cancer and the indispensable role of familial and social networks, with adult children’s financial reservoir often serving as the primary buffer. “My pension is not enough to cover my treatment. My daughter helps me out. I feel bad, but I have no choice” [P9]. “I borrowed money from my brother. Without his help, I don't know how I would continue” [P5].
Beyond finances, the resource pool includes non-monetary support from the broader social network, which is indispensable for managing daily logistics. A caregiver highlighted this practical aid: “My cousin lives nearby. She comes to help take care of my dad when I have to work. I'm so grateful for her support” [C1]. “My boss is very understanding. He allowed me to work part-time so that I can take care of my mom” [C7].
Role Reconfiguration in the Practice of Familial Obligation
A cancer diagnosis significantly restructures traditional family roles, necessitating a profound intergenerational recalibration. Older generation, once authoritative and caregivers, now assume dependent roles, while younger members assume unprecedented caregiving and decision-making responsibilities. Though emotionally challenging, this role reveal is a pivotal adaptive mechanism for preserving family homeostasis during crisis. An older patient expressed this poignantly: “I used to be the one taking care of everyone. Now, my kids are taking care of me. I try to be as independent as possible to not trouble them too much” [P10].
This sentiment reflects a common struggle to reconcile their former role with new vulnerabilities. Concurrently, adult children and spouses make significant personal sacrifices to fill the care gap. A caregiver detailed this expanded burden: “Before, my parents helped with the housework and my kids. Now, I have to do everything myself while also looking after my sick father” [C6].
These adjustments are not merely pragmatic but are framed by a powerful narrative of familial unity and filial duty, which helps legitimize the sacrifices. As a young caregiver affirmed, “I encourage my father every day. I tell him that our family will always be there for him. We will all get through this” [C7]
This collective ethos enables difficult choices, such as career compromises described by another caregiver. “I gave up a promotion at work. I need to be with my mom during her treatment. Family comes first” [C11].
Through this reciprocal adaptation and reaffirmation of shared commitment, the family system seeks a new, functional equilibrium to navigate the disruption caused by illness.
Discussion
This dyadic qualitative study provides a detailed portrayal of how older Chinese cancer patients and their caregivers experience and cope with financial toxicity. Our findings reveal that financial toxicity is not merely as an economic strain, but as a profound psychosocial phenomenon embedded in the culture of filial piety and family interdependence. The themes our analysis yielded form a complex narrative in which cultural strengths and systemic vulnerabilities are inextricably linked.
Our first theme highlights filial piety’s dual role in financial toxicity. While it provides a care framework, it paradoxically exacerbates distress through a “filial piety paradox”: mutual avoidance and tacit bargaining over resources. Patients hide financial worries to avoid burdening families, while caregivers conceal costs out of duty, causing communication breakdowns. This aligns with Chinese studies linking self-perceived burden, caregiver strain, and poor mental health. 29 The resulting silence breeds tension and conflict, echoing global concerns over financial communication gaps. One study conducted in the USA revealed that financial distress is prevalent in cancer families, and spouse’s ease of engaging with illness communication could be a potential target for future intervention studies. 18 Although improving patient-provider financial dialogue is needed, 30 our study stresses that interventions must address critical communication deficits within the family system itself.
Furthermore, the “tacit bargaining” between therapeutic efficacy and cost, together the manifestation of “love’s burden” as complicated emotions, highlights the intense moral and emotional calculus faced by dyads. The conflict between a patient’ s desire to conserve family resources and a caregiver’ s imperative to “do everything possible” creates a profound ethical dilemma. 31 The resulting guilt, shame, and ambivalence, as poignantly expressed by our patients and their caregivers in our study, represent a significant psychological toll that is intricately tied to cultural expectations. This finding contrasts with some Western settings where individual autonomy in treatment decision-making might be more pronounced 32 and underscores that in China, financial toxicity is experienced as a relational and moral crisis within the family.
Our second theme confirmed and deepened that financial toxicity manifests as a multidimensional crisis, triggering an interlocking cycle of physiological, psychological, and social distress within patient-caregiver dyads—a “triple suffering” dilemma. Substantial evidence has established the connection between individual financial strain and physical 33 and mental health, 34 while relational dynamics amplify the burden: a caregiver’s cost-related anxiety worsens their own health, and a patient’s sense of being a burden deepens the caregiver’s psychological strain, creating a mutually destructive feedback loop. Furthermore, financial toxicity significantly impacts the careers of adult-child caregivers. Against China’s one-child policy backdrop, this “sandwich generation” experiences declining job performance, reduced promotion prospects, and increased turnover risk, undermining long-term professional development. 35 A comprehensive, multi-tiered intervention strategy is therefore urgently needed to address this systemic crisis.
In confronting with the heavy financial erosion, Chinese families often construct a “Familial Fortress.” This protective mechanism, mobilized through coordinated caregiving and resource-pooling among kin, is a powerful manifestation of resilience. Further evidence from global studies mirrors these findings—family members may forego or delay medical care of their own, sacrifice on basic necessities like food, and experience challenges in affording housing and transportation.36,37 However, the Chinese fortress is distinct in its scale, coordination, and its foundation in filial piety. A recent paper published in Lancet also suggests that these negative impacts of financial toxicity may be exacerbated among cultures with family-centered care approaches, where family members disproportionately bear the burden of home caregiving instead of relying on facility care. 38 Yet, this fortress comes at a cost, often intensifying internal burdens and leading to a “suspended present,” where long-term planning is abandoned due to profound uncertainty about future costs. This temporal dislocation, a global concern, is accentuated by the lack of a comprehensive long-term governmental and organizational initiatives, 39 forcing families to bear the full weight of the unknown.
The coping themes elucidate the strategic, family-centric approaches adopted by Chinese dyads. The “Familial Survival Logic of Resilience and Adaptation” is governed by a “familial covenant,” an implicit pact that orchestrates collective communication, shared decision-making, and mobilized support. This covenant transforms the family into a cohesive unit for co-regulating economic stress. This family-centered communication model offers a valuable alternative to the often provider-centric approaches discussed in Western literature and could inform global efforts to improve financial navigation in cancer care. 40
Furthermore, the “Logic of Familial Praxis in Navigating Resource Allocation” demonstrates a sequential and hierarchical approach to resource mobilization. Chinese families first deplete personal savings, then seek support from adult children, and finally extend to the broader kinship network. This reliance on strong “social fabric” differs from the pattern observed in some Western countries, where patients primarily use savings or rely on state welfare and professional financial services. 41 The “role reconfiguration” within this praxis is profound. The shift of older patients from caregivers to dependents and the significant sacrifices made by younger members are framed by a powerful narrative of filial duty and familial unity, which helps legitimize the sacrifices and maintain family homeostasis during crisis. Therefore, future research should develop culturally tailored interventions such as financial navigation and psychosocial support to address the distinct financial toxicity experienced by older cancer patient and their families. 42
The experience of financial toxicity differed meaningfully between spousal and adult-child caregivers. Spousal caregivers, mostly retired, experienced financial toxicity as the depletion of shared retirement savings and grief over a jointly planned future now unraveled. Adult-child caregivers, however, were caught in the “sandwich generation” dynamic—simultaneously supporting aging parents, their own children, and their careers. Their burden manifested as competing resource demands across three generations, compounded by career sacrifices including reduced work performance and forgone promotions, with long-term wealth accumulation consequences. Communication patterns also diverged: parent-child dyads displayed more mutual concealment around costs driven by filial piety, whereas spousal dyads showed greater financial transparency born of a lifetime of shared resource management. These distinctions underscore the need for tailored interventions—retirement-preservation strategies for spouses, and support addressing tri-generational financial strain for adult children.
Our focus on patient-caregiver dyads rather than broader family networks reflects the demographic realities of contemporary urban China. Decades of the one-child policy, combined with urbanization, have produced the “4-2-1” family structure, wherein a single adult child bears primary responsibility for two aging parents while often raising a child of their own. In this compressed structure, extended relatives typically offer only occasional practical assistance, leaving the dyad as the functional unit of cancer care. This reality underscores the urgency of policy intervention: without expanded long-term care insurance, caregiver subsidies, and community-based supportive care infrastructure, the “4-2-1” structure places unsustainable burdens on adult children—a vulnerability that will only intensify as China’s population continues to age.
This study has several limitations. First, as a qualitative study within a specific cultural context, the findings may not be statistically generalizable. Second, participant recruitment was limited to tertiary hospitals in urban settings, potentially excluding perspectives from rural or primary care populations. Furthermore, this study focused on short-term experiences and coping strategies regarding financial toxicity, and future research should explore its long-term impact on patients and caregivers.
The study yields multi-level implications for clinical practice, healthcare administration, and policy development. At the clinical level, financial toxicity should be recognized as a dyad-level issue, with providers facilitating open family communication about treatment costs and offering culturally sensitive financial navigation. At the institutional level, cancer centers should integrate financial counseling into standard care pathways and develop peer support programs connecting affected families. At the policy level, insurance coverage should be expanded for non-medical costs, reimbursement for supportive care services strengthened, and systemic supports developed to address the unique vulnerabilities created by China’s aging population and one-child policy legacy.
Conclusion
This qualitative dyadic study elucidates financial toxicity as a profoundly relational process shaped by Confucian cultural imperatives of filial piety and familial interdependence. While filial piety serves as a protective resource that fosters family cohesion and motivates caregiving, it also functions as an ethical constraint that generates internal contradictions, mutual concealment, and emotional ambivalence within patient-caregiver dyads. The findings reveal a distinctively Chinese “familial survival logic” through which families navigate multidimensional erosion, underscoring that financial toxicity constitutes not merely an individual economic hardship but a systemic family crisis. The experience, negotiation, and management of financial burden through the moral lens of intergenerational duty mark a key distinction from more individualistic Western contexts. Thus, interventions should adopt a family-centered framework, integrating practical financial guidance with culturally attuned psychosocial support to enhance collective well-being among older cancer patients and their families.
Footnotes
Acknowledgments
The authors of this study would like to express their sincere gratitude to all interviewees for sharing their experiences and insights.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grants from CAMS Innovation Fund for Medical Sciences (CIFMS) (2025-I2M-C&T-B-045), Beijing, China.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The interview transcript data generated and analyzed during the current study are not publicly available due to confidentiality and privacy considerations.