
Abstract
Background
Neonatal nursing care requires ethical competence alongside technical expertise. Despite progress in Spain, disparities persist in ethical training and professional autonomy in neonatal units.
Objective
To examine the ethical dimension of neonatal nursing in Spain, including training, institutional resources, ethical climate, and experiences of ethical conflict and moral distress.
Research design
A descriptive, observational, and cross-sectional study was conducted, combining quantitative and qualitative analyses to examine the ethical-professional reality of neonatal nurses nationwide. The study was based on an ad hoc questionnaire specifically designed for this research and validated through expert review and content validation procedures.
Participants and research context
A total of 307 neonatal nurses in Spain completed an online questionnaire developed by the researcher with 24 structured and semi-structured items. The sample size was determined based on voluntary nationwide participation during the 6-month data collection period, aiming to maximize territorial representation and professional heterogeneity among neonatal nursing staff. The instrument explored sociodemographic, educational, professional, and institutional variables, together with experiences of moral distress and ethical conflict.
Ethical consideration
The study followed the Declaration of Helsinki and Spanish and European data protection regulations. The questionnaire was fully anonymous, and no personal data or IP addresses were collected. Informed consent was obtained from all participants. As the study involved anonymous voluntary participation without clinical intervention or sensitive data processing, Ethics Committee approval was not required under regulations.
Findings
Most participants had non-formal bioethics training, whereas formal postgraduate education was rare. Moral distress was reported by 85% of respondents, mainly related to treatment limitation, therapeutic obstinacy, and end-of-life care. Bioethics training and professional experience predicted moral distress, while Clinical Ethics Committees showed no predictive value. These findings highlight the need to strengthen ethics education and promote participatory institutional environments to support ethical decision-making and reduce moral distress in neonatal nursing practice.
Conclusion
The ethical dimension of neonatal nursing in Spain is shaped by education, experience, and institutional climate. Training was associated with moral distress, but its impact depends on organizational support, underscoring the need for participatory environments to reduce suffering and strengthen ethical care.
Keywords
Introduction
Neonatal care represents one of the most ethically demanding areas of contemporary healthcare. Neonatal intensive care units (NICUs) involve highly complex clinical decisions, uncertainty regarding prognosis, end-of-life situations, and emotionally charged interactions with families, requiring nurses not only to possess advanced technical competencies but also strong ethical competence to support decision-making and person-centered care.1–3
International research has highlighted the relevance of moral sensitivity, ethical conflict, and moral distress in neonatal and intensive care settings.4–7 Despite the growing international literature on ethics in intensive and neonatal care, empirical evidence focusing specifically on neonatal nurses in Spain remains scarce, particularly regarding ethics education, institutional support, and nurses’ participation in ethical decision-making.
This study constitutes the first initiative of the Ethics Working Group of the Spanish Society of Neonatal Nursing (SEEN), framed within the strategic line of the Ethical Observatory on Neonatal Nursing. Its purpose is to provide an updated overview of the ethical and professional situation of neonatal nurses in Spain. Specifically, it seeks to explore nurses’ perceptions of the main ethical conflicts present in neonatal care, the organizational conditions of units, the ethical training they have received, the tools available to them, and the potential existence of institutional initiatives aimed at strengthening the ethical dimension of neonatal care.8–10
Background
To understand the current state of ethics in neonatal nursing in Spain, it is essential to review its historical and academic trajectory. From a socio-educational perspective, Spanish nursing has undergone a profound transformation over recent decades, evolving from a technical and subordinate role—that of the Health Technical Assistants or Ayudantes Técnicos Sanitarios (ATS)—into an autonomous profession with university recognition. This transition began in 1977, when ATS schools were restructured into University Schools of Nursing, progressively replacing Catholic moral instruction with courses on professional ethics, in parallel with Spain’s transition towards a democratic and secular state. This reform culminated in 2010 with the full integration of nursing into the European Higher Education Area, granting it university degree status with access to master’s and doctoral programs. 11
In parallel, ethical reflection was institutionalized within the profession through the publication of professional codes of ethics and the progressive development of Clinical Ethics Committees (CECs).12–15 Despite these advances, significant disparities in ethical training and competence remain within neonatal nursing. Although the Pediatric Nursing specialty was formally recognized in 2010, 16 and more recently in 2023 the Specific Accreditation Diploma in Palliative Care was created, 17 current legislation does not require any specialized certification to work with newborns. This regulatory gap results in the coexistence of highly diverse professional profiles—diploma holders, bachelor’s graduates, specialists, and PhD nurses—often with heterogeneous levels of ethical education, producing variability in how clinical dilemmas are addressed and decisions are made.
International research has highlighted the relevance of concepts such as moral sensitivity, ethical conflict, and moral distress in emotionally demanding care settings such as NICUs and intensive care units.4–7 However, much of this literature has focused primarily on physicians, relegating nurses to a secondary position or portraying them mainly as mediators between medical teams and families.8,9,18 Within the Spanish context, studies addressing ethics in neonatal nursing remain scarce and generally fail to explore the ethical autonomy, deliberative participation, or institutional support perceived by nurses. 19 Considering this reality, generating empirical evidence is a priority to better understand how Spanish neonatal nurses experience, confront, and conceptualize ethics in their daily practice.
This study aimed to describe the ethical-professional landscape of neonatal nursing in Spain by examining ethics education, institutional ethics resources, perceived ethical climate, and experiences of ethical conflict and moral distress.
Methodology
Research context and study design
It is a descriptive, observational, and cross-sectional study aimed at examining the current state of clinical ethics from the perspective of nursing professionals working in neonatal units within the Spanish healthcare system. This design was considered appropriate for exploring the ethical-professional landscape of neonatal nursing at a national level and for identifying associations between educational, professional, and institutional variables related to ethical practice.
The methodological design was based on the development of an ad hoc questionnaire as the main data collection tool, allowing for the analysis of sociodemographic, educational, professional, and institutional variables related to ethical practice. Data collection was conducted between June and December 2024, ensuring accessibility, territorial representation, and heterogeneity of professional profiles. Although the nationwide scope of the sample represents a major strength of the study, the recruitment strategy relied partly on professional networks and snowball sampling, which may limit the representativeness and generalizability of the findings.
Participants and data collection procedure
Data were obtained through a self-administered online questionnaire consisting of 24 structured and semi-structured items, specifically developed for this study and subjected to expert-based content review to improve conceptual relevance and clarity, with an estimated completion time of 10 min. The form remained available online for 6 months.
The link to the questionnaire was disseminated through several channels: (a) direct distribution to heads of neonatal units in public and private hospitals; (b) publication in the official communication channels of SEEN and the Spanish National Nursing Council; and (c) a snowball sampling strategy to enhance territorial representation, which, although useful for reaching a wider and more heterogeneous sample, may introduce selection bias and limit the representativeness of the findings.
Participation was voluntary, anonymous, and non-incentivized. Informed consent was considered granted through submission of the completed questionnaire, after reading the ethical conditions stated at the beginning of the form, where participants had to indicate their agreement before proceeding.
The target population comprised practicing nurses working in neonatal units or other services in contact with neonatal care. Inclusion criteria were as follows: • Holding an official nursing degree (Diploma or Bachelor’s). • Being professionally active in neonatal care at the time of participation. • Voluntary acceptance of the study conditions.
Incomplete responses or those not meeting the inclusion criteria were excluded.
Study instrument
The questionnaire was developed within the framework of the Ethical Observatory on Neonatal Nursing (OEEN), promoted by the Spanish Society of Neonatal Nursing (SEEN) and designed by its Ethics Working Group. The development process followed several sequential phases to improve methodological rigor, conceptual clarity, and content relevance. Initially, a comprehensive review of the literature on bioethics, moral distress, ethical climate, clinical decision-making, and neonatal nursing practice was conducted to identify the principal domains and variables explored in previous studies. This review informed the conceptual structure of the instrument and the selection of the thematic dimensions included.
The preliminary version of the questionnaire was constructed by the research team based on both the literature review and the clinical and academic expertise of professionals with experience in neonatal nursing, bioethics, and healthcare research. The instrument combined closed multiple-choice questions with a limited number of short open-ended items in order to capture both standardized information and contextual qualitative insights related to ethical experiences in neonatal care.
Subsequently, the questionnaire underwent a content validation process through expert review. A panel composed of professionals with expertise in neonatal nursing, bioethics, nursing education, and clinical research evaluated the instrument in terms of conceptual relevance, clarity, comprehensibility, coherence between items and dimensions, and adequacy of response options. Based on their feedback, several items were reformulated to improve semantic clarity and reduce ambiguity, thereby strengthening the face and content validity of the instrument.
The final version of the questionnaire was organized into six thematic blocks: (1) Sociodemographic data. (2) Bioethics training. (3) Professional experience. (4) Institutional practices related to ethics. (5) Perceptions of ethical climate, CECs, and clinical decision-making. (6) Experiences of ethical conflicts and moral distress.
Prior to dissemination, the questionnaire was pilot-tested with a small group of neonatal nursing professionals to assess item comprehension, usability of the online format, estimated completion time, and overall acceptability. Minor linguistic and structural adjustments were subsequently incorporated. The final instrument consisted of 24 structured and semi-structured items and required approximately 10 min to complete.
The questionnaire was anonymous and did not require personal identification data, thereby ensuring the confidentiality and security of responses.
Because no previous validated instrument specifically addressed the combination of ethical training, institutional ethics resources, ethical climate, participation in decision-making, and moral distress in Spanish neonatal nursing contexts, an ad hoc instrument was considered methodologically appropriate for this exploratory nationwide study. However, the questionnaire should not be considered a fully validated psychometric scale. Complex constructs such as ethical climate, participation in decision-making, and interaction with CECs were assessed using simplified indicators rather than validated multi-item subscales. Consequently, the interpretability, construct precision, and comparability of some findings may be limited.
Regarding sample size, no formal a priori power calculation was performed because the study was designed as an exploratory, descriptive, nationwide survey based on voluntary participation. Recruitment remained open for 6 months with the objective of maximizing territorial representation and professional heterogeneity among neonatal nurses across Spain. Although the final sample size (n = 307) allowed the performance of descriptive, inferential, and multivariable analyses with adequate variability across categories, the absence of a formal power analysis should be considered when interpreting the statistical findings, particularly for subgroup comparisons and predictive models.
Data analysis
Data processing was performed using IBM SPSS Statistics (Version 29) 20 and, complementarily, the Python programming language,21,22 with the support of the scikit-learn, matplotlib, NumPy, and pandas libraries.23–25
First, univariate descriptive analyses (frequencies, percentages, means, and standard deviations) were conducted to characterize the sample and the main variables included in the questionnaire. Special attention was given to the distribution of work shifts and religious beliefs, in addition to sociodemographic and professional data.
Given the ordinal and categorical nature of most variables, the assumption of normality was verified using the Shapiro–Wilk test, which confirmed non-normal distributions (all p < 0.001). Consequently, non-parametric statistical tests were employed. Chi-square tests of independence (χ2) were applied to examine associations between categorical variables, such as the relationship between bioethics training and moral distress, or between religion and the presence of ethical conflicts. For ordinal variables such as perception of the ethical climate or availability of reflection spaces, Kruskal–Wallis tests were used to compare distributions across categories of work shift and religion.
Binary logistic regression models were carried out to identify predictors of two key outcomes: the experience of moral distress and the presence of ethical conflicts. Independent variables included in these models were bioethics training, years of professional experience, professional role, existence of CECs, participation in decision-making, work shift, and religion. This approach allowed simultaneous evaluation of the contribution of professional and contextual factors.
To further explore heterogeneity within the sample, a cluster analysis (k-means, k = 3) was performed, grouping participants into distinct ethical-professional profiles based on bioethics training, participation in committees, professional experience, perception of the ethical climate, moral distress, and type of institution. For graphical representation of these profiles, a Principal Component Analysis (PCA) was applied to the standardized variables, producing a two-dimensional scatterplot that illustrated the distribution of clusters and their interrelationships (Figure 1). Principal component analysis (PCA) scatterplot of ethical-professional profiles (k-means, K = 3).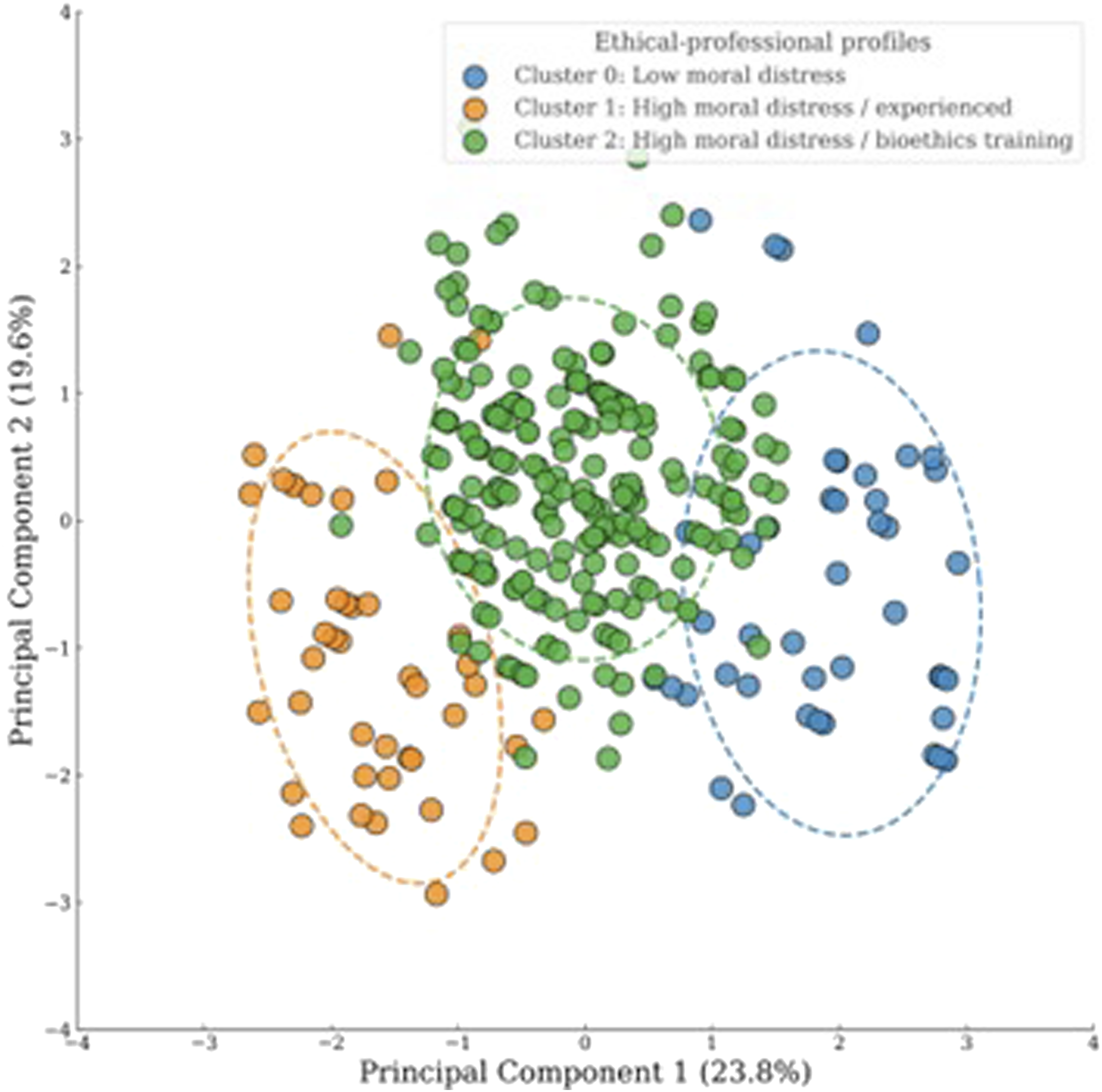
This methodological approach combined classical descriptive and inferential techniques with multivariate analyses and advanced visualization tools, enabling not only the exploration of associations between work shift, religion, and ethical awareness, but also the identification of complex patterns and emerging professional profiles within the sample.
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki and European and Spanish legislation on research and data protection (EU Regulation 2016/679 and Organic Law 3/2018).
The online questionnaire was designed so as not to collect personal information or direct or indirect identifiers (names, postal or email addresses, IP addresses, or other traceable data), and responses were stored in a secure database hosted on private servers owned by SEEN, with exclusive access for the research team, thereby ensuring confidentiality and scientific use of the data only. Consequently, in accordance with the GDPR and the Spanish LOPDGDD, the research did not involve the processing of personal data nor direct intervention with participants and was therefore considered minimal risk.
Participation was voluntary, anonymous, and non-incentivized, following explicit informed consent, with the right to withdraw at any time without consequence being guaranteed. Under these conditions, and since neither privacy nor the fundamental rights of participants were compromised, approval by a research ethics committee was not legally required.
The questionnaire was specifically developed within the framework of OEEN, promoted by SEEN as a strategic line of its Ethics Working Group. Also, the initiative was recognized as being of Professional Interest by the Spanish Institute of Nursing Research, under the Spanish General Council of Nursing, according to the technical report INF23_2024 certified on 27 May 2024.
In this study, variables related to CECs referred exclusively to participants’ reported awareness of the existence of such committees and their familiarity with consultation procedures. The study did not assess the accessibility, responsiveness, quality of deliberation, or degree of nursing inclusion within CECs processes; therefore, findings concerning CECs should be interpreted cautiously and limited to their formal institutional presence rather than their practical effectiveness in ethical support.
Results
Sample characterization
Sociodemographic, professional, and personal characteristics of the sample.
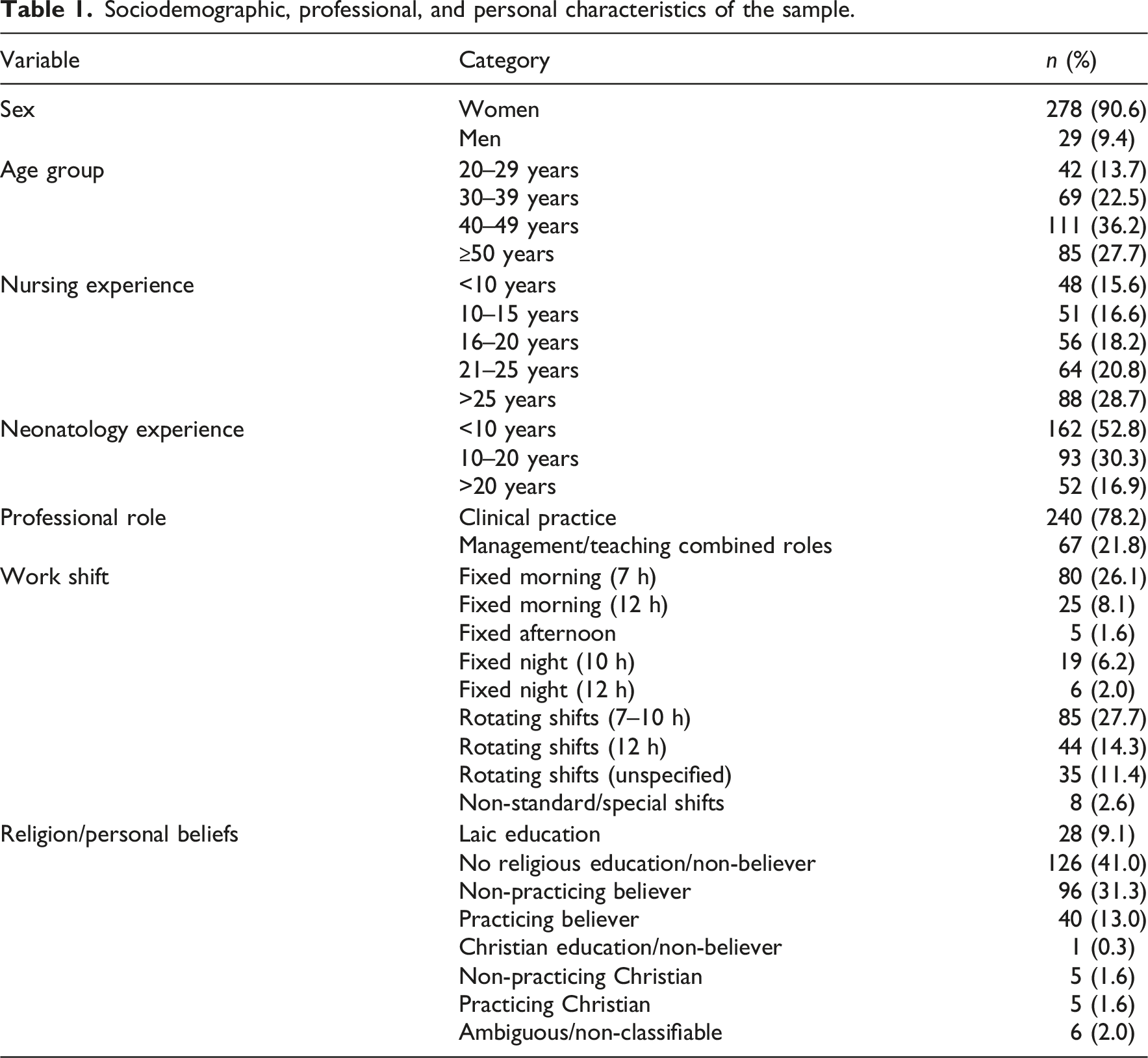
The most represented age groups were 40–49 years (36.2%) and 30–39 years (22.5%). Regarding professional trajectory, the largest proportion of participants had between 21 and 25 years of nursing experience, whereas experience in neonatology was predominantly concentrated in the lower ranges (<10 years). The predominant professional role was clinical practice (78.2%), although some respondents reported combined responsibilities in management and teaching.
Concerning work organization, rotating schedules were the most common, particularly 7–10-h rotating shifts, followed by fixed morning shifts. Smaller proportions reported fixed night shifts, afternoon schedules, or non-standard working arrangements.
With respect to religion or personal beliefs, the largest proportion of participants reported no specific religious education and identified as non-believers, followed by non-practicing believers and practicing believers. Smaller groups corresponded to other religious categories.
Ethical training, institutional climate, and moral distress
Ethical training, institutional climate, and moral distress among neonatal nurses in Spain.
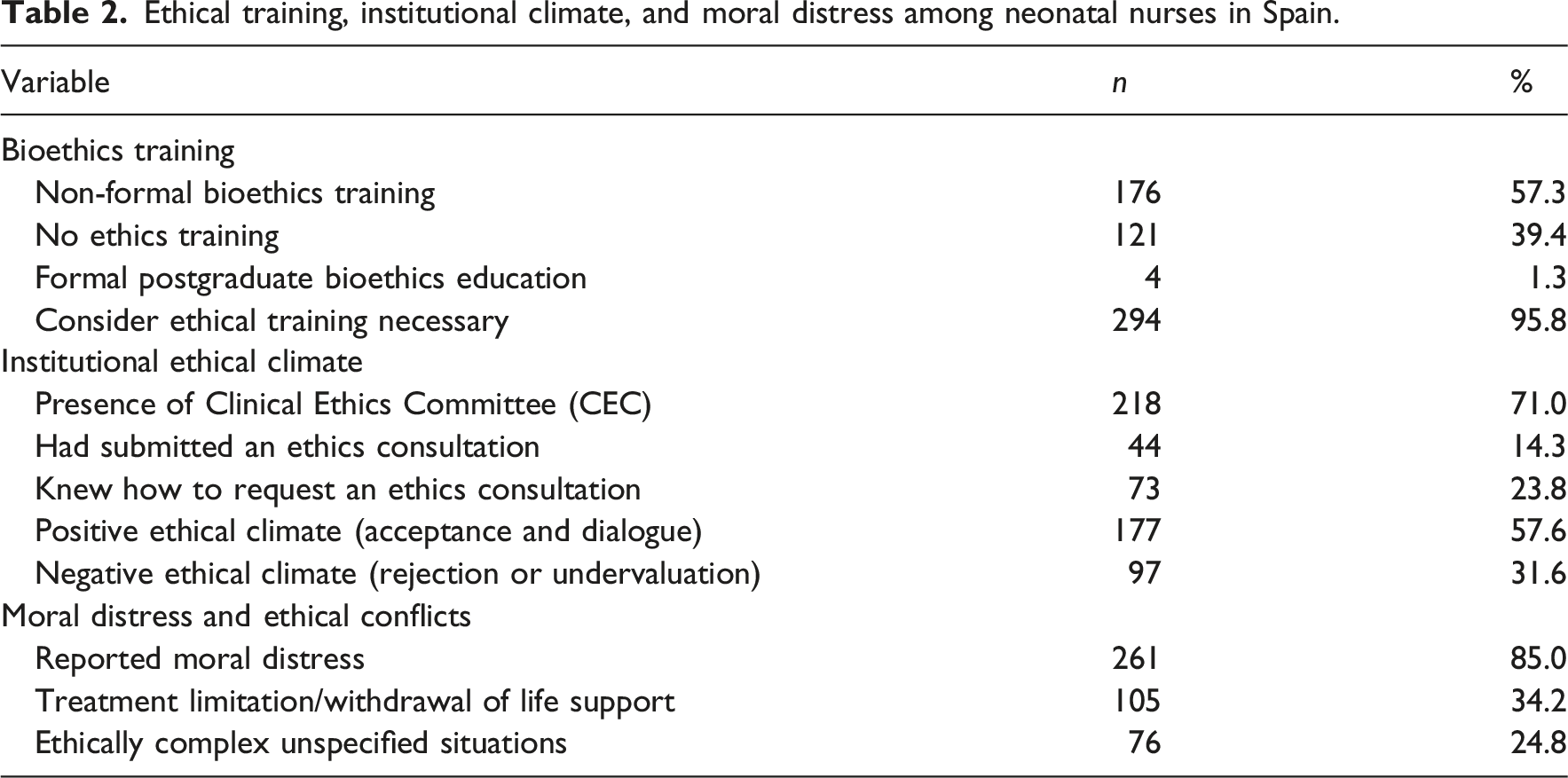
Regarding institutional ethical resources, 71.0% of respondents indicated that their institution had CECs, although only 14.3% had ever requested an ethics consultation and 23.8% knew the procedure for doing so. Concerning ethical climate, 57.6% perceived an atmosphere of acceptance and dialogue, while 31.6% reported dynamics of rejection or undervaluation.
Moral distress was reported by 85.0% of participants. The most frequent ethically challenging situations involved treatment limitation or withdrawal of life-sustaining interventions (n = 105), followed by unspecified ethically complex situations (n = 76). Additional sources of conflict included end-of-life care, therapeutic obstinacy, social problems, and deficiencies in interprofessional communication. Qualitative responses also highlighted perceptions of disproportionate medical interventions, institutional barriers such as the absence of protocols or palliative care teams, and limited nursing participation in ethically relevant decision-making.
Association analyses
Chi-square tests revealed a significant association between the level of bioethics training and the experience of moral distress (χ2 = 15.63; df = 4; p = 0.004; Cramér’s V = 0.23). In addition, a significant relationship was observed between moral distress and the experience of ethical conflicts (χ2 = 7.58; df = 1; p = 0.006; Phi = 0.16).
When exploring the role of work shifts, no significant associations were found with ethical climate (H = 7.64; p = 0.470), participation in deliberation (χ2 = 4.29; p = 0.830), availability of reflection spaces (H = 2.28; p = 0.971), or moral distress (χ2 = 11.76; p = 0.162). The presence of ethical conflicts also showed no significant differences across shifts (χ2 = 13.77; df = 8; p = 0.088; Cramér’s V = 0.21).
In relation to religion or personal beliefs, no significant associations emerged with ethical climate (H = 9.69; p = 0.207), participation in deliberation (χ2 = 5.79; p = 0.565), reflection spaces (H = 8.31; p = 0.306), or moral distress (χ2 = 6.89; p = 0.441). However, a significant association was found between religion and the presence of ethical conflicts (χ2 = 18.12; df = 7; p = 0.011), with a small effect size (Cramér’s V = 0.19). Higher frequencies of reported ethical conflict were observed among several religious orientation groups, although categories with small sample sizes should be interpreted cautiously.
The joint analysis confirmed that work shift and religion were independent (χ2 = 50.57; df = 56; p = 0.680). A multivariable logistic regression model including both predictors indicated that their associations with ethical conflicts became marginal (religion: p = 0.079; shift: p = 0.064), suggesting that neither factor exerts a strong or consistent influence once adjusted simultaneously.
Chi-square tests of association between key study variables.
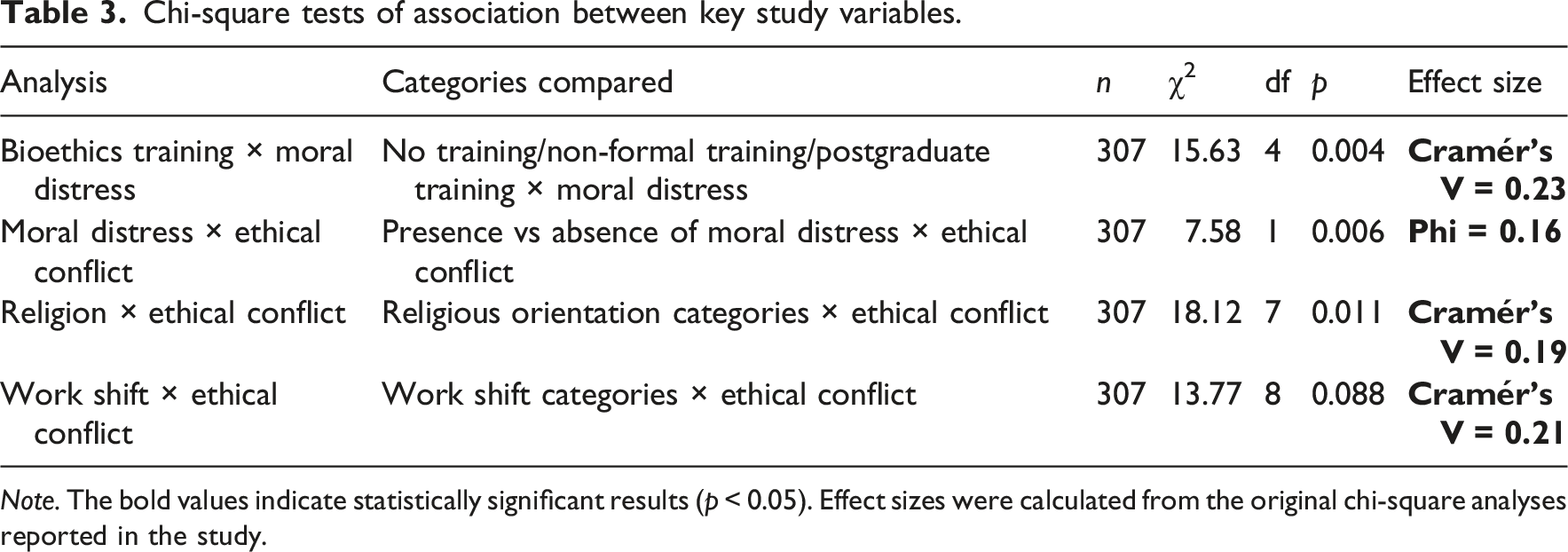
Note. The bold values indicate statistically significant results (p < 0.05). Effect sizes were calculated from the original chi-square analyses reported in the study.
Predictive models
A logistic regression model confirmed that bioethics training (OR = 3.44; 95% CI = 1.48–7.99; p < 0.001) and years of professional experience (OR = 1.35; 95% CI = 1.07–1.71; p = 0.011) were significant predictors of moral distress. In contrast, neither the existence of CECs (OR = 0.75; 95% CI = 0.15–3.65; p = 0.808) nor participation in shared decision-making (OR = 0.87; 95% CI = 0.32–2.36; p = 0.774) had predictive value. When shift type and religion were included as predictors of ethical conflict, both variables yielded only marginal significance (religion: p = 0.079; shift: p = 0.064).
Logistic regression model predicting moral distress.
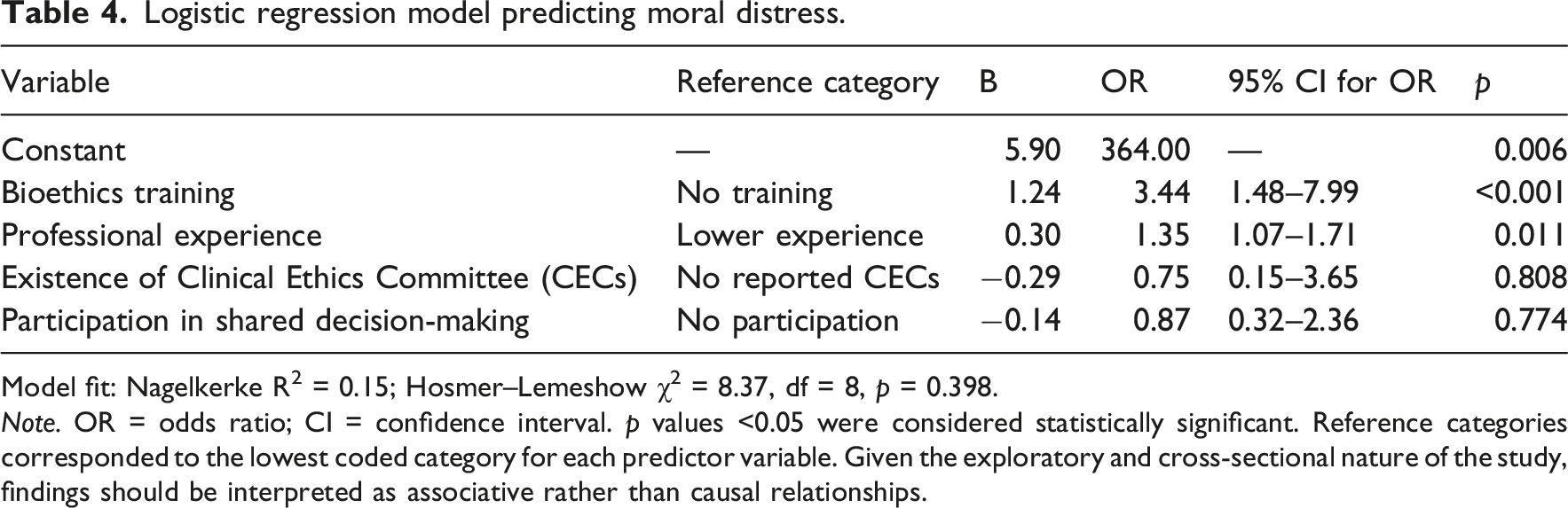
Model fit: Nagelkerke R2 = 0.15; Hosmer–Lemeshow χ2 = 8.37, df = 8, p = 0.398.
Note. OR = odds ratio; CI = confidence interval. p values <0.05 were considered statistically significant. Reference categories corresponded to the lowest coded category for each predictor variable. Given the exploratory and cross-sectional nature of the study, findings should be interpreted as associative rather than causal relationships.
Ethical-professional profiles
Ethical-professional profiles identified through cluster analysis.
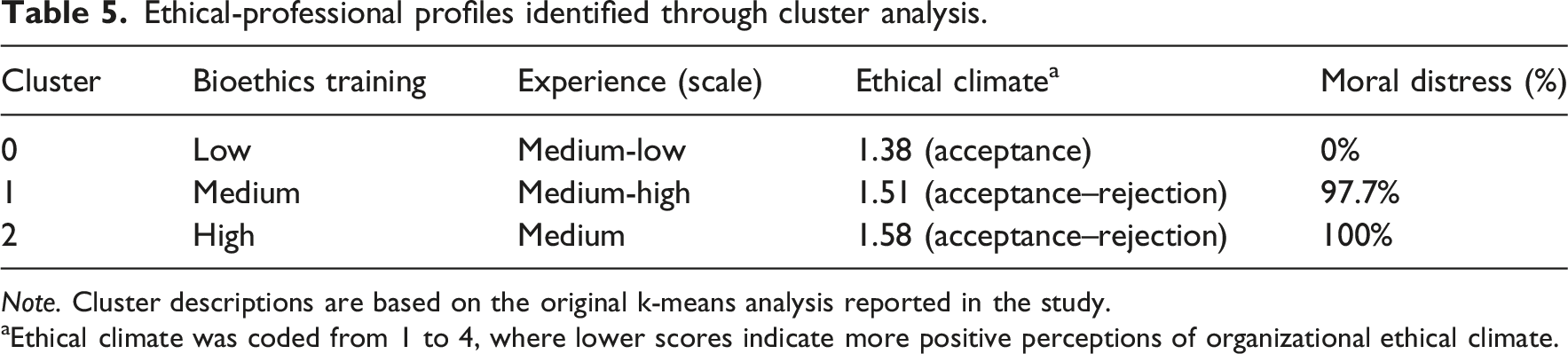
Note. Cluster descriptions are based on the original k-means analysis reported in the study.
aEthical climate was coded from 1 to 4, where lower scores indicate more positive perceptions of organizational ethical climate.
The ethical climate variable was coded from 1 to 4, where lower scores reflected more positive perceptions of ethical climate and organizational dialogue. These profiles should be interpreted as exploratory analytical groupings rather than fixed professional categories.
The PCA scatterplot illustrates the spatial distribution of the three ethical-professional profiles identified through k-means clustering. Cluster 0 (“low moral distress”) appeared more clearly differentiated along the positive axis of Principal Component 1, whereas Clusters 1 and 2 showed partial overlap, suggesting shared characteristics related to moral distress despite differences in professional experience and bioethics training. Cluster 1 (“high moral distress/experienced”) was concentrated mainly in the negative region of Principal Component 1, while Cluster 2 (“high moral distress/bioethics training”) occupied a more central distribution. These findings support the presence of heterogeneous but partially interconnected ethical-professional profiles within the sample.
Discussion
This study provides an unprecedented nationwide overview of the ethical dimension of neonatal nursing in Spain, emphasizing the interaction between training, professional experience, institutional climate, and the lived experience of ethical conflicts. The broad participation and heterogeneity of professional profiles represented lend robustness to the findings and allow for the extraction of implications relevant to education, clinical practice, and health policy.12,13 However, the findings should be interpreted within the exploratory scope of the study and in light of the methodological limitations inherent to the design and measurement approach employed.
Ethics education: Insufficiency and paradox
A particularly significant finding is the limited provision of formal training in bioethics. Although more than half of the participants had attended some type of non-regulated course, almost 40% reported never having received any training, and only 1.3% held postgraduate studies in this area. Nevertheless, nearly the entire sample (95.8%) considered ethics education to be necessary. This paradox reflects the persistence of a gap between the supply of and demand for ethics training, consistent with findings from both European and Latin American contexts.5,7
The significant association between bioethics training and moral distress supports the hypothesis that education increases sensitivity and the ability to identify ethical dilemmas. 25 While this effect might initially appear counterproductive, it may also reflect greater awareness and recognition of ethically complex situations among professionals with more training. Accordingly, the findings should not be interpreted as suggesting that ethics education causes moral distress, but rather that ethically trained professionals may be more capable of identifying and articulating situations perceived as morally problematic. Previous research has shown that ethics education accompanied by spaces for reflection and deliberation may contribute to resilience and professional development. 26 At the same time, the simplified measurement of moral distress and ethical training in this study limits the extent to which these relationships can be interpreted in depth.
Professional experience and cumulative exposure
Although years of professional experience were significantly associated with moral distress in the logistic regression model, these findings should nevertheless be interpreted cautiously given the exploratory and cross-sectional nature of the study. This finding is consistent with studies conducted in neonatal and adult intensive care settings, where repeated exposure to end-of-life decisions, resuscitations, or perceived futile interventions increases the likelihood of ethical discomfort.3,27,28 Greater seniority not only entails increased exposure to clinical dilemmas, but it may also be associated with greater awareness of therapeutic proportionality and institutional tensions. Nevertheless, due to the cross-sectional design and the use of self-reported measures, these associations should not be interpreted causally.
Clinical ethics committees: Between formality and practice
Another relevant finding is the gap between the wide availability of CECs, present in 71% of institutions, and their limited use: only 14.3% of nurses had ever submitted a case, and fewer than one in four knew the procedure to do so. This reproduces patterns described in other European contexts, where CECs often remain formal institutional structures with limited nursing participation or visibility.14,15 Importantly, the present study only assessed the reported existence of CECs and participants’ familiarity with consultation procedures. It did not evaluate accessibility, responsiveness, quality of deliberation, effectiveness, or the degree of nursing inclusion within committee processes. Therefore, the absence of predictive value observed for the reported existence of CECs in the regression model cannot be interpreted as evidence that CECs are ineffective or irrelevant in neonatal care settings. Rather, the findings suggest that the formal presence of CECs may not necessarily reflect their practical integration into nurses’ ethical support experiences. Literature suggests that improving visibility, accessibility, and interdisciplinary participation may facilitate greater use of these institutional resources.9,14
Ethical climate and organizational culture
The perceived ethical climate in units was notably heterogeneous: while 57.6% described an environment of acceptance and dialogue, 31.6% reported rejection or devaluation dynamics. These findings are consistent with evidence identifying organizational culture as a relevant factor in professional satisfaction and moral distress.29,30 Collaborative environments with open communication have been associated with lower levels of moral suffering, whereas hierarchical dynamics may constrain nurses’ perceived ethical autonomy. However, the present study was not designed to directly evaluate organizational structures or institutional functioning, and therefore these interpretations should be understood as contextual reflections supported by previous literature rather than definitive conclusions derived from the data alone.
Ethical conflicts and moral distress
The prevalence of moral distress observed (85%) exceeds values frequently reported in international literature, which generally range between 60% and 80%.27,28 The most common conflicts—limitation or withdrawal of life support, therapeutic obstinacy, end-of-life decisions, social issues, and communication failures—coincide with those reported internationally. However, the qualitative responses additionally highlighted perceptions of disproportionate interventions and institutional barriers affecting participation in ethically relevant situations. These findings suggest tensions between professional responsibility and organizational contexts, although the exploratory methodology used does not permit detailed evaluation of institutional practices or causal mechanisms. This observation aligns with the literature describing nurses as moral witnesses in highly demanding healthcare environments. 31
Work shifts and religion: Marginal associations and practical relevance
Although statistical analyses did not find significant associations between work shifts and ethical conflicts, ethical climate, or participation in deliberation, previous literature has documented the impact of scheduling on professionals’ well-being and ethical perception.29,32 Factors such as fatigue, shift rotation, and extended work hours may influence how professionals experience ethical dilemmas. The absence of significance in the present study should therefore be interpreted cautiously and warrants further longitudinal investigation.
Regarding religion or personal beliefs, an association was observed with the presence of ethical conflicts, although this relationship showed only marginal significance in the multivariable model and should therefore be interpreted cautiously. Previous studies have suggested that religious convictions may influence interpretations of end-of-life dilemmas or therapeutic proportionality.3,28 Thus, although religion did not emerge as a strong predictor, the findings suggest that personal beliefs may still form part of the contextual background shaping ethical experiences.
Ethical-professional profiles: Heterogeneity and typologies
Cluster analysis identified three profiles with contrasting ethical experiences. The “no moral distress” profile (Cluster 0), associated with lower ethics training and moderate experience, suggests that lower ethical sensitivity may coexist with positive perceptions of ethical climate. The “high experience and high distress” profile (Cluster 1) illustrates the cumulative ethical tensions associated with prolonged professional exposure. Finally, the “high training and high distress” profile (Cluster 2) suggests that advanced ethics education, in the absence of perceived institutional support, may coexist with greater moral suffering. These findings are consistent with latent profile analyses showing the coexistence of groups with varying levels of ethical sensitivity and resilience within the same clinical environment.6,25,30
At the same time, these results should be interpreted cautiously given that both moral distress and perceptions of institutional ethical climate were assessed through self-reported measures and simplified indicators rather than validated multidimensional psychometric instruments. Self-reported experiences may be influenced by individual interpretative frameworks, emotional state, recall bias, or differences in ethical awareness and expressiveness among participants. Likewise, perceived institutional support may not necessarily correspond to the actual availability, accessibility, or effectiveness of organizational ethical resources. Consequently, the identified clusters may reflect subjective experiential patterns as much as stable institutional or professional realities.
Nevertheless, these profiles should be interpreted as exploratory analytical categories rather than fixed professional typologies.
Practical and policy implications
The findings of this study support four main recommendations for neonatal nursing practice and policy. First, ethics education may benefit from being strengthened through postgraduate and continuing professional development initiatives that incorporate reflective and participatory methodologies such as simulation, case deliberation, and mentorship. 26 Second, improving nurses’ awareness of institutional ethics resources and consultation procedures may encourage more active engagement with ethical support structures.14,32 Third, fostering participatory organizational climates with greater inclusion of nurses in ethical decision-making processes may help mitigate the experience of moral distress and ethical conflict.29,30 Fourth, future institutional and research initiatives should prioritize the development of structured spaces for ethical reflection and interdisciplinary dialogue within neonatal care settings. 33
However, because the present study relied on exploratory self-reported data and simplified indicators, these implications should not be interpreted as direct evaluations of institutional quality or effectiveness, but rather as potential areas for future investigation and professional reflection.
Limitations and future research
The cross-sectional nature of this study precludes causal inference, and the use of a self-administered questionnaire may have introduced recall bias, subjective interpretation, or social desirability bias. Furthermore, the non-probabilistic recruitment strategy, based partly on professional networks and snowball sampling, limits the representativeness and generalizability of the findings.
An additional limitation concerns the use of an ad hoc questionnaire specifically designed for this study. Although the instrument underwent expert-based content review, it was not a previously validated psychometric scale. Consequently, complex constructs such as ethical climate, participation in decision-making, interaction with CECs, and moral distress were assessed using simplified indicators rather than validated multi-item instruments. This methodological choice limits the depth, precision, and comparability of the findings with other studies in the field.
Similarly, the study relied exclusively on self-reported perceptions and experiences, which may not fully reflect actual institutional practices, organizational dynamics, or ethical support mechanisms. Variables related to CECs, for example, referred only to their reported existence and familiarity with consultation pathways, without assessing their functioning, accessibility, or effectiveness in practice.
Future research should therefore consider longitudinal and mixed-methods designs, including validated measurement scales and in-depth qualitative approaches such as interviews or focus groups, to better understand how neonatal nurses experience ethical conflict and moral distress over time and across institutional contexts.7,9
Conclusion
The ethical dimension of neonatal nursing in Spain is shaped by a complex interplay of educational, professional, and institutional factors. This study provides a national exploratory overview of how neonatal nurses perceive ethics education, moral distress, institutional ethical resources, and organizational climate within their professional practice. Bioethics training and experience were associated with moral distress, but their relationship should be interpreted cautiously given the cross-sectional and exploratory nature of the study.
Rather than providing definitive evidence regarding the effectiveness of ethics education, CECs, or institutional ethical climates, the findings identify relevant patterns and potential areas for future research and professional reflection. The results suggest that organizational climate and access to deliberative resources may influence how nurses experience ethical challenges in neonatal care settings.
These findings support the importance of continuing to explore strategies that may strengthen ethical competence, participatory environments, and reflective clinical practice in neonatal nursing. Scientific societies may also contribute by promoting shared standards, fostering ethical reflection, and encouraging the development of common frameworks to support neonatal care practice.
Supplemental material
Supplemental material - First national study on the ethical dimension of neonatal nursing
Supplemental material for First national study on the ethical dimension of neonatal nursing by Javier Jiménez Flores, Aroa Casado Rodríguez, María del Carmen Fernández Tuñas, Marta Eva Láiz Rodríguez, Ángel Salcedo Madridejos, Patricia Sánchez Suárez, Leticia Lambea Rueda, Lorena Torres López, Cristina Molina Ruiz, María F. Jiménez Herrera, and Leticia Bazo-Hernández in Nursing Ethics
Supplemental material
Supplemental material - First national study on the ethical dimension of neonatal nursing
Supplemental material for First national study on the ethical dimension of neonatal nursing by Javier Jiménez Flores, Aroa Casado Rodríguez, María del Carmen Fernández Tuñas, Marta Eva Láiz Rodríguez, Ángel Salcedo Madridejos, Patricia Sánchez Suárez, Leticia Lambea Rueda, Lorena Torres López, Cristina Molina Ruiz, María F. Jiménez Herrera, and Leticia Bazo-Hernández in Nursing Ethics
Footnotes
ORCID iDs
Funding
The Spanish Society of Neonatal Nursing (Sociedad Española de Enfermería Neonatal) supported the open access publication of this article.
Declaration of conflicting interests
The authors declare that there are no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data generated and analyzed during the current study were collected through an anonymous questionnaire. Although no directly identifiable personal data were collected, the dataset includes sensitive variables related to participants’ professional context. For this reason, the data are not publicly available in order to protect participant confidentiality and comply with applicable data protection regulations, including the General Data Protection Regulation (EU) 2016/679 and Spanish Organic Law 3/2018. An anonymized and coded version of the dataset may be made available from the corresponding author on reasonable request, subject to appropriate ethical and data protection safeguards.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.