
Abstract
Abortion rates in England and Wales have reached record levels, highlighting the increasing need for skilled and ethically grounded nurses in abortion care. Despite its clinical importance, nurses involved in abortion services frequently encounter ethical tensions when their personal beliefs conflict with professional responsibilities. This literature review explores how nurses navigate conscientious objection (CO) and related ethical challenges within emotionally complex clinical environments. A structured search was conducted across CINAHL Ultimate, SCOPUS, Embase, and PsychINFO (via EBSCO), using the SPIDER tool to identify qualitative studies addressing nurses’ experiences in abortion care. After applying rigorous inclusion and exclusion criteria, five studies were selected for critical appraisal. Thematic analysis following Braun and Clarke’s six-step framework reveals three overarching themes: personal versus professional conflicts, institutional and organisational barriers to conscientious objection, and conscience formation and ethical growth. Findings indicate that nurses frequently suppress personal emotions to meet professional expectations, often without adequate institutional support. The absence of clear policies on CO, coupled with high workloads, staff shortages, and inadequate resources, further complicates their ability to exercise moral agency. Participants reported feeling ethically unsupported, emotionally isolated, and constrained by workplace cultures that discourage open discussion of values. At the same time, conscience was found to be fluid and shaped over time by experience, reflection, and contextual influences. This review concludes that systemic barriers and a lack of policy clarity undermine nurses’ ethical resilience in abortion care. To address this, healthcare organisations must implement clear and accessible CO protocols, offer structured ethics training and support emotionally reflective practice. Fostering a culture of inclusivity and ethical dialogue is essential to empower nurses and ensure equitable, compassionate care for women accessing abortion services.
Keywords
Introduction
Abortion, defined as the termination of pregnancy (TOP) through medical or surgical intervention, is a recognised component of reproductive healthcare globally; considered a safe and essential component. Its provision, however, is regulated differently across legal and cultural contexts. In Great Britain, abortion may be lawfully provided under specified conditions. 1 Even so, nearly half of all abortions worldwide are performed under unsafe conditions, making them a major contributor to preventable maternal death and long-term health complications. 2 Consequently, the provision of safe and accessible abortions is necessary. 2 In 2022, the highest number of abortions was recorded since the Abortion Act was introduced in 1967, with 251,377 abortions. 3 The British Pregnancy Advisory Service (BPAS) states that abortion is an essential part of women’s healthcare, which 1 in 3 women will need. 4 Therefore, ensuring the provision of safe, legal, and accessible abortions should not only be prioritised in healthcare but also considered a public health imperative.
Several challenges persist for nurses working in abortion services, including institutional, interpersonal, and intrapersonal conflicts, such as balancing professional expectations with personal beliefs. 5 In line with the current National Institute of Health and Care Excellence (NICE) guidance, abortion providers are encouraged to maximise the role of nurses and midwives in service delivery, reinforcing the importance of tailored training and support. 1 Evidence supports this, stating that high-quality care in these settings requires targeted training to strengthen practical and ethical competencies. 6 Additionally, evidence suggests a profound psychological impact on nurses and midwives with many reporting emotional strain and moral distress related to the stigmatisation of being an abortion provider, as well as a need for emotional support. 7
The Royal College of Nursing affirms that nurses involved in abortion care must be familiar with the policies applicable to their location. 8 In Great Britain, abortion care is governed by the Abortion Act (1967), which amends and clarifies the law relating to termination of pregnancy (TOP) by registered medical practitioners. 9 Section 4 (1) of the Act permits healthcare professionals, including registered nurses, to conscientiously object (CO) to participation in abortion treatment where this conflicts with their personal moral or religious beliefs. 10 However, this right is expressly limited. Section 4 (2) provides a statutory derogation, stipulating that CO does not apply where abortion treatment is necessary to save the life of the pregnant woman or to prevent grave permanent injury to her physical or mental health. This provision makes clear that CO is not absolute and may be overridden by clinical necessity.
Further constraints arise through regulatory interpretation. Under the Abortion Regulations (1991), CO only applies to direct involvement in the abortion procedure. 11 Nurses may therefore still be professionally expected to undertake indirect responsibilities, including patient preparation, post-abortion care, and completing necessary documentation, though this is an institutional expectation rather than an explicit requirement of the Regulations. 11 In addition, all abortions must be formally recorded and reported to the Chief Medical Officer within 14 days, regardless of personal beliefs. For some nurses, mandatory reporting is experienced not as a neutral administrative task but as indirect participation in abortion care, thereby challenging the moral separation they seek through CO. These obligations can blur the boundary between permitted objection and professional obligation, especially in fast-paced clinical settings. 12 As a result, many nurses experience uncertainty about what constitutes legitimate refusal, feeling caught between legal duties and personal convictions, contributing to broader ethical ambiguity in practice. 13
Alongside statutory duties, nurses’ decision-making is framed by professional regulation, most notably the Nursing and Midwifery Council Code, which requires nurses to prioritise patient safety, practise effectively, and uphold professional standards, even where moral beliefs are engaged. 14 Together, the Abortion Act and the NMC Code form a dual legal-professional framework within which nurses must navigate CO, clinical responsibility and ethical integrity. This framework may generate uncertainty regarding the legitimacy of refusal and contribute to ethical ambiguity in practice.
Despite this, a noticeable gap exists in the literature regarding how nurses experience and respond to conscientious objection in practice. 15 There are limited published articles exploring nurses’ perspectives on abortion care and CO directly, 5 leaving a significant area of ethical and professional concern under-researched. Although CO is legally recognised, the absence of formal guidance or institutional policy in many healthcare settings means that nurses often navigate these decisions independently. 16 Although nurses have a professional responsibility to act with integrity and avoid discrimination or compromised care, serious threats to moral integrity may still cause ethical distress and require institutional support 16 ; legal provision for CO further complicate this responsibility by creating tension between professional duty and personal conscience.
The care of women who are considering or undergoing an abortion is a sensitive area of practice, requiring knowledge and compassion. 8 Therefore, the role of the nurse becomes more complex as they must encompass these attributes but also act as advocates for informed decision-making, emotional support, and as carers throughout each woman’s perioperative process, as well as maintain their moral integrity.
Methods
The SPIDER framework (Sample, Phenomenon of Interest, Design, Evaluation, Research type) created by Cooke, Smith and Booth (2012) guided the inclusion criteria, offering a structured way to identify relevant studies. 17 The sample included registered nurses involved in abortion care with awareness or experience of CO. The phenomenon of interest centred on their lived experiences and ethical challenges surrounding participation or refusal. Eligible designs included qualitative methods such as interviews or focus groups. Evaluation focused on how nurses described ethical tension, decision-making, and professional impact. All included studies used or incorporated qualitative components.
An in-depth systematic search was conducted using relevant academic databases: CINAHL Ultimate, PsycINFO (via EBSCO), SCOPUS, Embase, and the University of Derby’s advanced library search engine. These databases were selected for their relevance to nursing, allied healthcare professionals, and behavioural sciences. 18 Boolean operators (AND/OR), truncation (*), and varied combinations of keywords and synonyms were used to build phrases that ensured a broad yet focused search. 19 For example, ‘nurs* perspectives’ was combined with terms like ‘ethical challenges’ and ‘abortion care’ or ‘conscientious objection’.
The initial search generated 199 results. Filters applied: English language, 2014-2025 publication, peer-reviewed, and topic relevance, reducing results to 46 articles. This ensured evidence reflected recent practices and standards. Peer-reviewed sources were prioritised to enhance the credibility, academic rigour, and validity of the review’s findings. 20 The abstracts from the 46 articles were read to assess the appropriateness and applicability of each. Abstracts were screened for relevance, and 5 studies were selected for critical appraisal, addressing the central research question. Studies were excluded if they were purely quantitative, did not report nurses’ perspectives separately, lacked an explicit ethical focus on conscientious objection, or were non-empirical publications such as editorials or opinion pieces.
Each included study was critically appraised using the CASP (Critical Appraisal Skills Programme) qualitative checklist. 21 This tool ensured consistency in evaluating credibility, rigour, and relevance. 22 For paper 5, which included quantitative components, the CASP cohort checklist was also applied.
Methodology
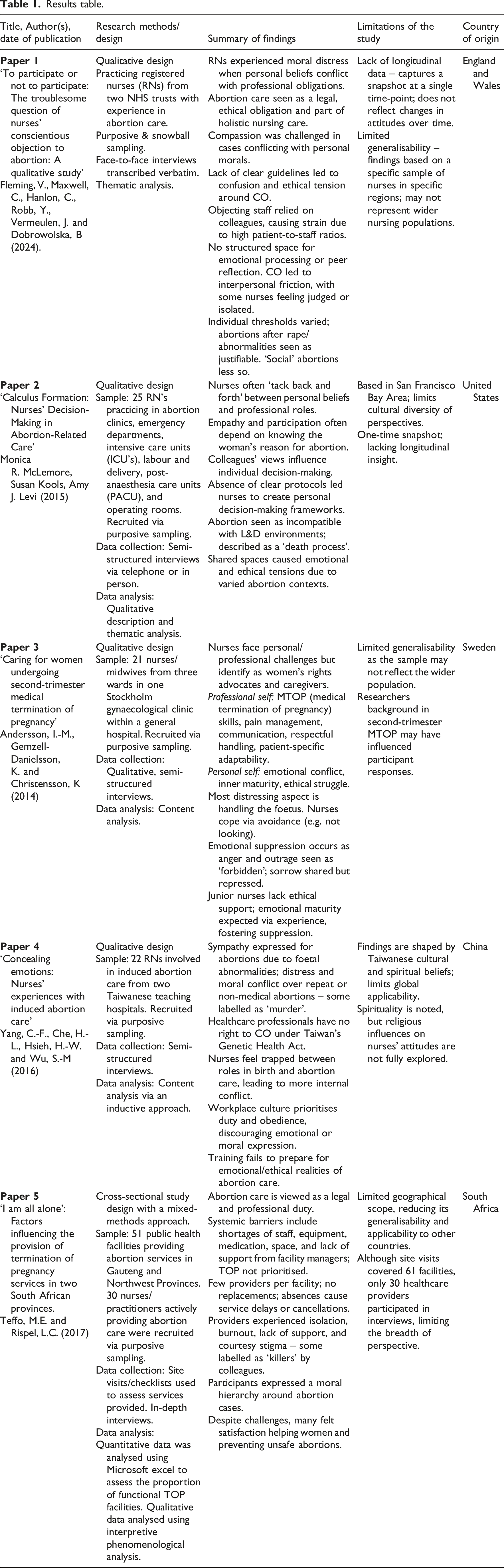
A critical appraisal revealed similarities and contrasts across design, sampling, data collection and analysis, and ethical considerations.
All studies utilised purposive sampling, suitable for the sensitivity of the topic.26–28 Paper 1 added snowballing, gaining rich accounts from 20 nurses from England and Wales’, but its small, homogenous sample limits generalisability. 29 Paper 2’s inclusion of varied clinical specialities strengthened transferability. Paper 3 (21 Swedish nurses/midwives) allowed depth but was confined to one hospital, reducing the scope. Paper 4 (22 Taiwanese nurses, two hospitals) offered cultural insight but weak transparency in inclusion criteria. Paper 5, with 30 providers across two South African provinces, combined multisite breadth and clear reporting, making it the most robust.
Papers 1-4 employed semi-structured, face-to-face interviews, well-suited to eliciting sensitive emotional experiences. 30 Reflexivity varied: Paper 1 emphasised openness, while Paper 4 overlooked researcher-participant dynamics. 31 Paper 2 added written reflections, deepening introspection, but risking self-censorship. 32 Paper 5 combined interviews with facility checklists and observations, capturing both personal and systemic factors, 33 and offering the most comprehensive design. 34 All studies used verbatim transcription, strengthening credibility and minimising misinterpretation.35,36
Analytical strategies differed in rigour and reflexivity, shaping credibility. Papers 1 and 2 used Braun and Clarke’s thematic analysis with a reflective, inductive stance. 37 Paper 1 followed the six steps and clearly explained theme development, strengthening credibility. 23 Paper 2 added memos and multiple coders, strengthening confirmability and reflexivity. 38 Papers 3 and 4 employed content analysis, suitable for categorising emotional themes, but less interpretively rich. 39 Paper 3 applied dual coding but ignored researcher influence, limiting depth, while Paper 4 detailed steps and memos but overlooked positionality. Both produced credible themes but weaker reflexivity than Papers 1, 2, and 5. Paper 5 employed Interpretive Phenomenological Analysis (IPA), enabling nuanced exploration of meaning,40,41 and offering the most robust analysis, though requiring interpretive skill may reduce coder consistency. 42 Overall, all methods were appropriate but varied in transparency and reflexive depth.
All studies reported ethics approval, consent, and anonymisation, 43 though details varied. Overall, paper 1 showed proactive safeguarding, while others took a more procedural approach with limited discussion of emotional risk. 44
The studies’ methodological diversity introduced variation in analytic transparency, sampling rigour, and reflexivity. Qualitative designs, while suited for ethical exploration, may limit generalisability. 26 Additionally, the limited representation of UK-based studies may restrict the applicability of findings to the NHS context. Even so, international research offers insight into global abortion care models, which may inform NHS practice. 45 These factors should be considered when interpreting the overall strength and transferability of the evidence base.
This literature review uses research carried out in varied political, legal, regulatory, cultural, and economic frameworks, such as the United Kingdom, United States of America, Sweden, China, and South Africa. Inasmuch as this reflects the globalised issue of abortion care and the ethics of nursing, it also poses several challenges regarding methodology. The legal definition of conscientious objection, professional regulations, institutional culture, as well as collective beliefs regarding the issue of abortion, vary widely among these countries. This means the included research cannot be considered equivalent in either legal safeguards, professional freedom, or institutional support for nurses.
Instead of attempting structural equivalence between different healthcare systems and thus comparing similar structures and organisation of care in different countries, research studies were synthesised through the lens of themes that are experiential and ethical in nature and include themes such as moral distress, professional duty and commitment, emotional labour, and conscience formation. It becomes possible through this method of synthesising research studies to point out what ethical tensions are common and how such tensions are experienced in different conditions. Therefore, when results are interpreted within the context of the UK healthcare system, there must be an important degree of caution.
The geographical scope and variations in jurisdiction represented across the studies should thus be appreciated as providing a depth of context and not generalisability. The results aim to provide insight into the generic ethical challenges faced by nursing practitioners in abortion care and not that the practices and legal protections exist as a norm. These considerations are implicit in the conduct of a qualitative meta-synthesis across ethically complex and globally diverse contexts.
Discussion
The three themes discussed across the five papers include (1) personal versus professional conflicts, (2) institutional and organisational barriers to conscientious objection, and (3) conscience formation and ethical growth in practice, all relating to abortion care and provision. These themes collectively explore the intrapersonal dilemmas faced by nurses, their strategies for navigating interpersonal and institutional challenges, and the development of their conscience and ethical decision-making within clinical practice.
Theme one
Personal vs. professional conflicts
A central theme emerging across all five papers is the internal conflict nurses experience when their personal moral beliefs clash with professional obligations in abortion care. All studies demonstrate that abortion care challenges clinical competencies while deeply engaging personal identity and ethics, resulting in what has been described as the division between the ‘personal self’ and the ‘professional self’ (paper 3).
Participants consistently reported that engaging in abortion care often required emotional suppression, particularly when their moral stance did not align with the procedure. In paper 2, this was described as ‘tacking back and forth’, capturing the emotional dissonance of switching between inner views and professional expectations. Nurses in paper 3 also described navigating between two distinct identities in practice: one’s ‘personal self’ marked by moral discomfort, and one’s ‘professional self’, committed to delivering calm, compassionate, and patient-centred care. Participants spoke about masking feelings of sadness, grief, or even anger, as these emotions were considered unprofessional in abortion care settings. Similarly, paper 1 found that participants viewed their role in abortion care as part of their ethical responsibility, even if they disagreed with it. Several reported emotionally ‘switching off’ as a coping strategy. Such coping mechanisms often became habitual, as participants internalised the belief that emotional neutrality was a mark of professionalism. One nurse in paper 2 challenged a colleague’s selective objection, stating: ‘You can take care of the murderer, the rapist, the bank executive, but you can’t take care of the 21-year-old…’. This powerful assertion exposes the moral inconsistency that can arise when personal beliefs are applied unevenly across patients. 46 This reinforces the need for institutional guidance and ethical training, as emphasised by NICE (2019), 47 to ensure that CO is exercised in a principled, equitable manner rather than influenced by personal bias.
The ethical complexity is further heightened by the legal framework nurses must navigate. Under the Abortion Regulations (1991), 11 all abortions must be formally recorded and reported to the Chief Medical Officer within 14 days; this constitutes a statutory requirement applicable regardless of personal belief. By contrast, indirect responsibilities such as documentation, patient coordination and aftercare represent institutional expectations rather than explicit requirements of the regulations, yet they may still evoke moral distress when perceived as complicit in an objectionable practice. Although the Abortion Act (1967) provides statutory protection for nurses who conscientiously object to abortion, such protection does not necessarily preclude indirect involvement in abortion-related care. A parallel right to CO also exists under s38 of the Human Fertilisation and Embryology Act 1990, which applies to licensed fertility treatment involving embryos; however, as this review focuses specifically on abortion care, a full discussion of that provision falls outside its scope. 48 The limitations of conscientious objection were clarified in Greater Glasgow Health Board v Doogan (2014), in which the Supreme Court restricted its scope to direct participation in abortion procedures. 49 This narrow interpretation has significant implications for nursing practice, as it exposes a legal-ethical gap wherein professional accountability may supersede personal moral conviction. The resulting dissonance has been identified in the literature as a contributor to moral distress, highlighting how legal compliance does not necessarily equate to ethical resolution for nurses in clinical settings. As a result, a disconnect emerges between legal requirements and ethical convictions, where professional accountability can override personal belief. This tension, frequently reflected in papers 1, 3, and 5, suggests that while such regulations aim to ensure compliance, they may inadvertently exacerbate emotional strain and contribute to long-term ethical distress.
Abortion care demands not only clinical skill but also emotional resilience. The divide between personal and professional roles noted across studies reflects the psychological strain of balancing moral integrity with professional duties, 50 often leading to burnout and compassion fatigue when institutional support is lacking. 51 Nurses in paper 5 viewed abortion care as part of their role yet reported discomfort when personal values conflicted, while in paper 1 some felt compelled to provide care despite deep unease. These conflicts are often internalised, affecting long-term mental health, with the Royal College of Gynaecologists (RCOG) describing this ‘internalised state’ as pride and purpose coexisting with guilt and shame. 52
The Abortion Regulations (1991) 11 represent a professional expectation for nurses to provide care despite moral uncertainty. Papers 2 and 5 highlight how this may pressure them to suppress their beliefs to appear ‘professional’, which can lead to feelings of isolation or regret. However, Merrifield 53 found that while these regulations can be perceived negatively, their actual influence on professional identity is insignificant. Instead, factors like organisational culture, interpersonal relationships, and individual moral development are more central.
While most participants felt unprepared to handle these conflicts, NICE (2019) 47 has since emphasised the importance of equipping healthcare staff with abortion-specific training, recommending that specialities involving abortion ensure all trainees receive practical experience and education unless they formally opt out due to CO. This reflects a shift toward proactive policy alignment that acknowledges the emotional complexity of abortion care, while still maintaining clinical competence and patient access.
Addressing this emotional conflict requires proactive strategies in both education and practice. Nursing training programmes must prepare practitioners for ethical ambiguity, equipping them with emotional intelligence and tools for moral reflection. 13 Regular debriefing sessions and ethics consultations could provide spaces for nurses to explore moral distress without fear of judgement. Embedding content related to conscientious objection and value-based decision-making into pre-registration curricula would better prepare nurses for navigating such challenges. 52 Nursing leadership should also model open discussions and foster environments where expressing ethical discomfort is not seen as weakness but as a professional responsibility.
Across the studies, the moral framing of abortion significantly influenced the emotional response of nurses. Participants in papers 1, 3, and 4 expressed greater empathy toward women seeking abortion in cases of rape, incest, or foetal abnormalities, which they perceived as more morally legitimate. In contrast, elective or repeat abortions, especially those perceived as ‘lifestyle choices’, provoked frustration and emotional detachment. In paper 4, one participant went so far as to describe such procedures as ‘murder’, underscoring the extent to which perceived legitimacy shapes emotional engagement. In paper 2, nurses working in labour and delivery units described abortion as a ‘death process’, contrasting sharply with the congratulatory nature of childbirth they were accustomed to. These findings suggest that nurses apply a moral filter to different types of abortion, potentially influencing empathy and care unconsciously.
The variability in moral judgement across studies reveals an underlying ethical hierarchy, where some patients are seen as more deserving of compassion than others. The NMC Code (2018) 14 asserts that nurses must not allow personal views to affect the quality or delivery of care. However, the literature suggests that in practice, nurses struggle to maintain this standard, particularly without adequate institutional support. One participant from paper 1 stated that ‘Sometimes it’s hard to engender compassion (…) but if she gives me her hand, I’ll hold it’. This sentiment exemplifies the emotional complexity of care provision in abortion contexts. Despite this, many nurses still prioritised human connection, suggesting that compassion is not absent but often conditional or situational. Unacknowledged, this variability risks undermining consistent, ethical care. 54
To mitigate this, organisations must foster a culture of reflection and self-awareness. Training in bias recognition, empathy building, and values clarification could help nurses become more conscious of how their own moral frameworks influence practice. 55 Reflective practice groups and case discussions could provide safe spaces for exploring difficult emotions and enhancing ethical consistency. 56 Additionally, routine access to supervision or clinical ethics support could help nurses process complex moral experiences, reducing the risk of compassion fatigue and professional burnout.
The psychological toll of reconciling personal values with professional responsibilities was clear in papers 3 and 5. Participants reported sleep disturbances, emotional exhaustion, and, in some cases, regret about participating in abortion care. One nurse in paper 5 described an inability to express their feelings openly, stating that even discussing distress with colleagues felt ‘unprofessional’. Paper 3 further explored this emotional repression: participants reported internalising distress and appearing calm while feeling ‘broken’ inside. Participants frequently noted the absence of debriefing or structured emotional support, framing abortion work as an isolating experience.
The combined effect of unspoken and suppressed emotional burden is substantial. Nurses experiencing prolonged moral dissonance without institutional support are at risk of developing high levels of stress, compassion fatigue, and even attrition from the field. 57 While emotional regulation is a key component of nursing professionalism, the expectation to continuously suppress genuine feelings without release or validation is unsuitable. These findings suggest that the nursing profession must move beyond a purely passive model of care and recognise the human cost of ethically complex work.
Healthcare providers must incorporate mental health safeguarding into abortion care roles. This could include providing psychological support services, facilitating team-based reflections, and acknowledging emotional labour as part of the job description. Managerial staff should receive training to recognise signs of emotional fatigue and proactively support staff well-being. Furthermore, professional bodies such as the Royal College of Nursing and the NMC should update guidance to explicitly address emotional well-being in ethically charged practice areas. By doing so, organisations not only support staff retention and satisfaction but also improve patient care outcomes through more engaged and emotionally healthy practitioners.
In summary, this theme reveals that nurses do not simply perform clinical duties in abortion care; they manage complex moral challenges that test their personal values and professional ethics. The ‘tacking back and forth’ reported in paper 2 is not just a descriptive metaphor but a lived reality that significantly impacts emotional health, quality of care, and professional identity. Participants’ views reflect a clear need for more structured emotional and ethical support systems that acknowledge and address the internal conflicts inherent in abortion provision. To move forward, education, policy and institutional culture must all play a role in supporting nurses to deliver compassionate, equitable care while protecting their emotional integrity.
Theme two
Institutional and organisational barriers to conscientious objection
Nurses’ ability to exercise conscientious objection (CO) in abortion care is shaped not only by legislation, but also by the healthcare system’s institutional and organisational frameworks. While CO may be legally permitted in some regions, its implementation is often hindered by unclear policies, lack of support mechanisms, workplace stigma, and logistical pressures. The five papers reviewed highlight how these institutional conditions can either empower or suppress nurses’ moral agency. This is particularly evident across healthcare systems where policy clarity, support, and training vary significantly. For instance, some hospitals may facilitate objections with formal protocols, while others rely on impromptu responses leading to confusion, stress, and a lack of systemic ethical support. To address this disparity, practical interventions such as mandatory ethics training, peer support programmes, and communicated CO policies could empower nurses to act in alignment with their moral beliefs while ensuring continuity of care.
The most common pattern across the studies was the absence of formal guidelines and protocols for CO. In papers 1 and 2, participants described unclear or non-existent institutional policies, leaving nurses to interpret their responsibilities and rights. In paper 2 the lack of open discussion about CO created a sense of confusion and isolation, as nurses were unsure how to object without facing professional repercussions. Paper 2 found that nurses developed ‘calculus formations’ to decide on participation, relying on context, relationships with colleagues, or perceived severity of the case rather than institutional guidance. This inconsistency increased psychological pressure and reduced care consistency and the inability to distinguish diverse cases contributed to discomfort and a sense of professional inadequacy. A participant from paper 2 described the ethical tensions of a unit that grouped all cases: ‘we’re not set up to be an all-encompassing kind of women’s health place (…) someone’s there for their 20th abortion, and someone there is needing an abortion that they don’t want’. The inability to distinguish these experiences both practically and ethically, contributed to a sense of moral discomfort and professional inadequacy.
Operational and staffing constraints further exacerbated these challenges. In paper 5, nurses reported that in some facilities, only one or two staff members were trained in abortion care. In such contexts, objecting meant service disruptions, increased pressure on colleagues, or patient care delays. Paper 1 revealed similar concerns, where high patient-to-staff ratios made it impractical for nurses to object to participation without impacting team function. Consequently, many continued providing care despite moral opposition to avoid burdening colleagues. As previously mentioned in theme 1, this sense of duty often pushed nurses to suppress personal objections, leading to what might be considered coerced participation. In this context, the tension between institutional obligation and personal ethics becomes an operational barrier to enacting CO meaningfully.
Stigma also played a significant role in shaping institutional cultures. Nurses in papers 2 and 5 described being labelled as abortion-friendly or facing degrading insults from colleagues simply for providing care. In extreme cases, participants reported being called ‘killers’ or ‘murderers’ by other healthcare workers. This courtesy stigma, where individuals are tainted by association, created a culture of silence and avoidance. 58 As a result, some nurses chose not to speak up about their discomfort or to conceal their objections for fear of professional or social ostracism. Paper 1 supported these findings, noting that institutional cultures rarely encouraged open discussion of ethical concerns, further increasing feelings of isolation.
Paper 3 focused on a critical gap in the preparation of nurses for ethically complex scenarios due to a lack of formal ethics education and mentoring. To address this, findings suggest a need for educational reform that incorporates structured ethics modules, simulation-based learning, and ongoing mentorship programmes. 59 These improvements would help nurses build confidence, articulate COs appropriately, and navigate ethical dilemmas with greater clarity. Participants reported that while clinically trained, they received little guidance in managing complex ethical dilemmas, with structured opportunities for debriefing being minimal. Instead, ethical resilience was expected to develop through personal trial and error. Paper 4 echoed these limitations in Taiwan, where the Nurses’ Act mandated participation in abortion procedures. Although this legal framework removed the confusion of CO policies, it also removed moral autonomy, as nurses were expected to comply without objection. Participants reported being discouraged from expressing discomfort, with professionalism defined by emotional suppression and obedience rather than ethical reflection.
The physical environment of care settings also acted as a barrier to ethical practice. In paper 5, nurses described settings with broken equipment, limited access to medication, and resource shortages. These constraints not only added practical strain but also ethical distress. 51 One nurse noted, ‘When we get there, everybody already knows what they have come for. There is no privacy at all’, revealing how inadequate spatial arrangements jeopardised patient confidentiality and dignity. This contravenes NICE guidance 1 which emphasises respecting privacy and confidentiality. Such failures reflect how physical space and organisational oversight overlap to undermine ethical care standards. Nurses felt unsupported, and their concerns, whether about practical issues or moral objections, were often overlooked.
Conscientious objection is not solely an individual moral decision; it is deeply influenced by institutional culture and structure. To accommodate moral diversity, healthcare organisations could implement formalised conscience clauses, regular ethics meetings, and staff surveys to monitor the efficacy of objection protocols. These mechanisms would provide nurses with clear, supported pathways to navigate ethical dilemmas, ensuring that moral autonomy is preserved without compromising patient care. Nurses may technically have the right to object, but without clear protocols, sufficient staffing, emotional safety, and ethical education, that right becomes inaccessible. The Royal College of Nursing affirms that nurses involved in abortion care must be familiar with the legal requirements of the legislation and policies applicable to their location. 8 The papers reviewed consistently demonstrated that ethical engagement requires more than legality; it requires a workplace that actively supports reflective practice, respects diverse viewpoints, and fosters open conversations.
For CO to be a meaningful, ethically grounded option in abortion care, healthcare institutions must prioritise clarity, transparency, and emotional support. This includes developing accessible CO policies, creating structured opportunities for ethics discussions, and ensuring that refusing to participate does not result in professional consequences. Staffing systems must be robust enough to accommodate objections without compromising patient care, and organisations must take active steps to validate nurses’ ethical experiences. Without these reforms, CO becomes ineffective, forcing nurses to face complex ethical challenges alone.
Within the UK, the General Medical Council 60 and the Royal College of Nursing (2024) both stress that conscientious objection must not compromise timely access to care. NHS Trusts are advised to implement local protocols to manage objections fairly while maintaining service continuity. However, as the reviewed literature shows, many nurses report either no awareness or no enforcement of these guidelines. This highlights a gap between national policy and local practice that institutions must address through training, audits, and implementation.
Theme three
Conscience formation and ethical growth in practice
The development of conscience in nursing is a dynamic, ongoing process shaped by education, lived experiences, reflective practice, and professional socialisation. Unlike fixed belief systems, conscience is continually formed and reformed in response to clinical encounters and moral reasoning. 61 Several studies emphasised that nurses’ perspectives on abortion and conscientious objection (CO) evolved through their careers via reflection, education, and professional exposure.61,62
In paper 3, participants reflected on a shift in their moral outlook after repeated exposure to ethically complex abortion cases. This is echoed in midwives’ accounts in England and Wales, where many described the challenge of ‘finding a balance’ between legal duties and conscience, evolving their stance over time. 62 Some nurses reported becoming more tolerant of differing perspectives, often through mentorship and structured discussions, and pre-registration ethics education, as seen in paper 5. NICE (2024) 1 supports this, recommending that practical experience of abortion care should be embedded into professional training programmes unless formally declined through CO. Such experiential learning opportunities allow nurses to confront moral complexity in real time, strengthening rather than diminishing ethical clarity. Papers 1 and 2 show that even among objectors, repeated clinical exposure prompted nurses to reflect on whether their objections were absolute or context-dependent. This highlights a process of ethical malleability, where experience strengthens rather than weakens moral reasoning. Thematic cross-paper analysis revealed that conscience development is most robust when supported by formal reflective spaces, as seen in paper 3, and weakest when ethical reflection is informal or absent.
Papers 1 and 4 revealed that emotional intelligence and empathy played a pivotal role in shaping nurses’ consciences. One participant noted that hearing patients’ personal stories surrounding abortion deepened their appreciation for the complexity of such decisions, prompting contemplation about previously held assumptions. This aligns closely with Beauchamp and Childress’s (2013) four pillars of biomedical ethics, which underpin ethical decision-making in healthcare. 63 Developing conscience requires the ability to balance respect for autonomy, supporting women’s right to choose, with non-maleficence and beneficence, which involve protecting patients while acting in their best interests. 64 In ethically complex areas like abortion care, the principle of justice also becomes relevant, requiring equitable care regardless of personal belief. To facilitate this, NICE (2024) 1recommends that nurses and midwives be positioned at the forefront of abortion care delivery, supported through appropriate education and policy frameworks. This strategy not only builds capacity but also affirms the legitimacy of their role in care delivery.
However, the reviewed literature also reveals a geographical divergence in how conscience is institutionally nurtured. While paper 3 reflects a Swedish model in which reflective practice is integrated into daily operations, papers 4 and 5 show that ethical growth is either stifled or overshadowed by obedience and institutional rigidity. Yet even in the UK, nurses expressed uncertainty about CO policy scope, suggesting that without clear parameters, conscience may be inconsistently or unfairly applied. 12 This supports the earlier discussion of legal and ethical dissonance, where ambiguity in policy undermines ethical confidence and practice consistency. Without consistent support for ethical development, nurses risk forming rigid, unexamined views that may hinder compassionate and balanced care.
Therefore, it is essential that nurse education and continuing professional development (CPD) explicitly include content that nurtures ethical reflection and critical thinking. 59 Programmes that incorporate structured ethical discussions, scenario-based learning, and values clarification exercises may support nurses in navigating this moral ambiguity. Frameworks like Gibbs’ Reflective Cycle 65 provide accessible structures, enabling nurses to learn from their lived experiences with guided ethical reflection. Embedding Gibbs’ Reflective Cycle in training and practice could improve ethical preparedness and help reconcile belief with duty. A systematic review of midwives’ and nurses’ reasons for objection supports this gap in ethical preparedness, calling for proactive integration of ethics training in the UK nursing curriculum. 15 In turn, this enhances nurses’ ability to reconcile belief and duty in emotionally charged scenarios like abortion care.
These findings highlight the need for education and practice environments that promote reflection and ethical competence. Developing conscience is not simply about reinforcing pre-existing beliefs. When institutions create environments that support reflection, critical dialogue, and ethical inquiry, nurses are better able to engage with complex moral issues like abortion. 66 Conversely, without support, conscience may become rigid or conflict with professional responsibilities and the NMC Code (2018), 14 which calls on nurses to ‘practice in line with best available evidence’, ‘prioritise people’, and ‘preserve safety’. These standards require a flexible conscience capable of navigating uncertainty.
Intersectionality plays a key role in how conscience forms and is expressed in nursing. Nurses do not make ethical decisions in isolation from social identity. Factors like religion, age, ethnicity, gender, and cultural influence how nurses approach abortion care. Nurses from conservative backgrounds may experience more internal conflict, while others may feel pressure from institutions. Paper 4 hinted at this, linking obedience and morality to traditional values. However, none of the studies directly addressed how identity shapes ethical development. Future research should examine how nurses’ identities intersect with role expectations, shaping how they deliver abortion care. Patient perspectives in the UK support this view, noting that ethical decision-making is often shaped by providers’ values and backgrounds. 67
Conscience is not static; it develops through clinical experience, emotional reflection, and professional relationships. In abortion care, this evolution is crucial, as decisions often involve personal belief, legal limits, and compassionate care. Nurses’ moral frameworks are shaped by patients, peers, and policies over time. Still, conscience alone may not protect them. Without institutional safeguards, like emotional support and clear objection policies, even ethically mature nurses risk feeling unsupported or silenced. To be meaningful, conscience must be paired with structural support.
Recent nurse-led ethical frameworks for evaluating CO emphasise proportionality, professional responsibility and moral integrity as relational rather than absolute concepts. The findings of this review align with these approaches, particularly in highlighting the need for case-sensitive ethical support rather than binary classifications of ‘objector’ or ‘provider’. Rather than framing CO as a fixed moral position, nurses in the reviewed studies described fluid, context-dependent ethical reasoning shaped by experience, institutional culture, and available support.68,69
Conclusion
This literature review explored nurses’ perspectives on abortion care, conscientious objection (CO), and the ethical, legal, and emotional challenges encountered in practice. Through thematic analysis of five qualitative studies, three key themes emerged: personal versus professional conflicts, institutional barriers to CO, and conscience formation within ethical nursing practice.
The first theme revealed how moral dissonance arises when personal beliefs clash with professional duties. While compassion and patient-centred care helped nurses manage this tension, many described their stance as fluid, shaped by experience. Instead of identifying solely as ‘objectors’ or ‘providers’, they articulated morally ambiguous positions. This suggests nurses construct internal thresholds for participation, navigating a ‘grey zone’ of ethical reasoning often unsupported by legislative expression of policy.
The second theme examined organisational and legal barriers to moral autonomy. Participants across all studies described vague CO protocols, limited ethical support, and fear of stigma. In paper 4, CO was absent from policy, forcing nurses to participate. Even where CO was recognised as a right, it was weakened by unclear procedures and a lack of institutional support. These findings reveal a disconnect between national policies like the Abortion Act 1967 9 and how they are implemented locally, leaving nurses without meaningful ethical guidance.
The third theme explored how nurses’ conscience develops through experience, reflection, and institutional culture. Rather than fixed, conscience emerged as an evolving ethical identity shaped by clinical exposure. Participants expressed that abortion care deepened their understanding of advocacy, empathy, and resilience. NICE (2024) 1 supports embedding abortion training in education, echoing calls for structured reflection and mentorship. Still, without systemic support, conscience development alone may not be enough.
These findings demonstrate that ethical resilience cannot rely on reflection alone. Moral complexity requires clear policy, consistent training, and emotional safeguards. Education and CPD must prepare nurses for ethically challenging care. Establishing clear, enforceable CO policies protects both nurse autonomy and patient access. Institutions should foster ethical discussions, peer learning, and debriefing to move beyond basic compliance. 6
With educational and systemic reforms, nursing can advance a more compassionate, ethically resilient model of abortion care; one that protects nurses’ integrity and patients’ rights.70,71
Limitations
This review is limited by the inclusion of a small number of studies and by significant variation in legal, cultural, and organisational contexts across countries. While thematic synthesis enabled exploration of shared ethical experiences, findings should be interpreted cautiously and not assumed to be directly transferable across jurisdictions. Further detail regarding methodological limitations and cross-context comparability is discussed within the Methods section.
Footnotes
Acknowledgements
This literature review was conducted as part of the requirements for the Bachelor of Science program in Adult Nursing at the University of Derby. The author wishes to express sincere gratitude to Mrs. Danielle Dunne for her encouragement and support. Their support has contributed to the development and refinement of this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.