
Abstract
Background
Nurses, as the most frequent providers of healthcare services, play a key role in nursing research. Their knowledge of ethics ensures scientific quality and respect for human rights.
Objectives
To identify nurses’ knowledge of Research Ethics Committees (REC) and to explore barriers and facilitators to access.
Research design
Descriptive cross-sectional study of nurses from two Spanish hospitals, conducted in March-April 2025, using ad hoc questionnaire.
Ethical considerations
Participants’ confidentiality and anonymity were guaranteed. All participants provided informed consent.
Results
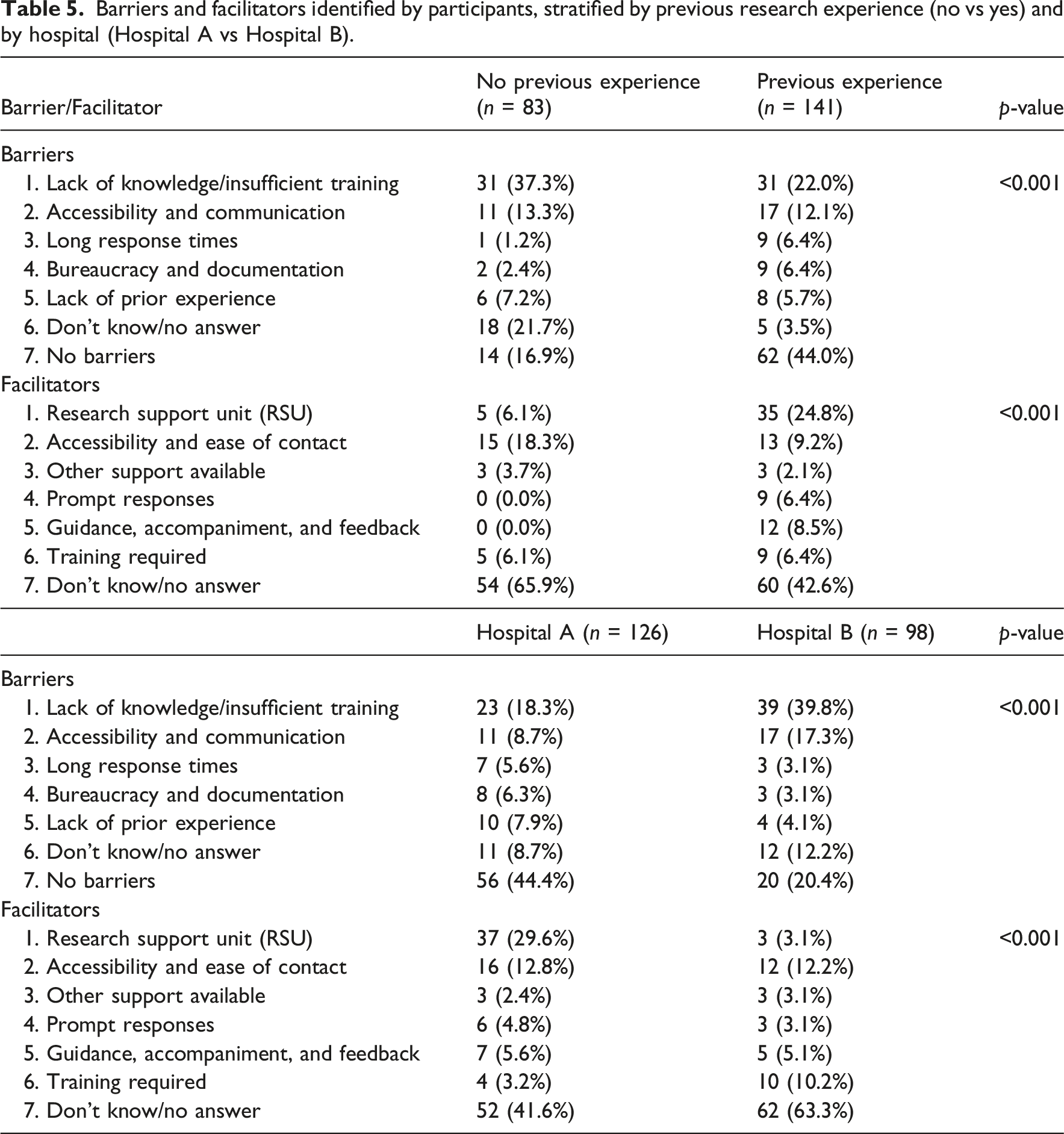
A total of 224 nurses responded. The mean age was 43.15 years (SD 9.45), and the mean length of professional experience was 18.97 years (SD 9.53). More than 67% were aware of the definition and functions of the REC. Only 45.5% knew that a lay member is required as part of its composition. A total of 55.8% knew how to properly obtain informed consent, and between 41.5% and 65.2% were aware of its use in studies involving minors or image-based research. Previous research experience was associated with higher overall knowledge, although not with knowledge related to informed consent. Lack of knowledge and/or training was the main barrier in both hospitals, significantly higher in Hospital B (p < 0.001) and among nurses without prior research experience (p < 0.001). The Research Support Unit (RSU) was identified as the main facilitator in Hospital A compared with Hospital B.
Conclusions
Participants demonstrated adequate knowledge of the definition and functions of REC, but limited understanding of their composition and accessibility. Gaps were also identified in the use of informed consent, particularly in studies involving minors. Lack of training was the main barrier, while the RSU was the main facilitator. REC should improve their accessibility and promote dissemination strategies, training in research ethics, and mentoring in order to reduce barriers and facilitate nurses’ engagement in research.
Introduction
Nursing research has grown globally in response to the challenges posed by current demographic changes and the increasing care demands placed on healthcare systems worldwide. Nurses are directly involved in frontline care and constitute the largest workforce within health systems; therefore, their contribution to nursing research can be pivotal. 1 Ethics in nursing practice places patients’ wellbeing as the primary focus of all actions. In research ethics, the parallel guiding principle, as articulated in the Belmont Report, is ‘respect for persons’. In nursing research, additional challenges may arise, as the nurse–patient relationship becomes a nurse–research participant relationship, which may lead to tensions between adherence to research protocols and the advocacy and care of the patient/research participant. 2 Ethical principles aimed at preserving the autonomy of research participants, avoiding harm, ensuring privacy and data protection, maintaining anonymity, guaranteeing the right to informed consent to participate, and allowing withdrawal at any time must be present in researchers’ minds at every stage of the research process. 3
Background
All research involving human participants requires approval from a Research Ethics Committee (REC) prior to initiation. Consequently, RECs are the main guarantors of compliance with the ethical principles set out in the Declaration of Helsinki and with the legal regulations applicable in each region or country. 4 The legislative regulation of REC, is framed within a multilevel regulatory structure. In the international context, and particularly within the European framework, a key reference is the Oviedo Convention (1997), which establishes ethical and legal principles for biomedicine and the protection of human rights, and has been ratified by 29 member states of the Council of Europe. Within the European Union, REC are also primarily governed by Regulation (EU) No 536/2014, which harmonises the ethical and scientific assessment of clinical trials across Member States, ensuring coordinated procedures and increased transparency. 5 In Spain, the specific regulatory framework is Royal Decree 1090/2015, which regulates clinical trials with medicinal products and formally defines the REC as independent bodies responsible for safeguarding the protection of participants and issuing opinions on clinical studies. 6
However, obtaining approval from a REC does not in itself guarantee that research will be conducted ethically, highlighting the importance of maintaining Research Integrity (RI). This concept encompasses the principles of honesty, transparency and respect for ethical norms and standards at all stages of the research process, including study design, data collection, analysis, reporting and publication. Preserving RI is essential to maintaining trust in science and is the responsibility of researchers, journals, readers and, particularly, institutions, which must foster an environment that supports the ideals of integrity while providing researchers with appropriate guidance, training and support.7–9
Within the European Union, these concerns were reflected in the publication of Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data.10,11 In Spain, this regulation was implemented through Organic Law 3/2018 on Personal Data Protection and the guarantee of digital rights.
In addition, in Spain, the Ministerial Order of 3 April 1992 (BOE, 14/04/92) established the creation of Research Units within the National Health System, with the aim of maintaining and enhancing the quality of existing research and facilitating the integration of research into the routine clinical activity of all healthcare professionals. However, their development has been uneven across different healthcare areas and institutions, and their internal organisation varies according to available resources. 12
Over recent decades, nursing in Spain has undergone substantial academic and professional development, accompanied by increased participation of nurses in research studies.13,14 Currently, healthcare institutions are developing strategies to enhance nurses’ research competencies so that nursing care achieves high-quality standards and generates sufficient scientific evidence to directly impact population health and quality of life. Nevertheless, the implementation of these strategies has been uneven across healthcare organisations, largely depending on how managerial teams allocate support and resources to nurses and the value they place on nursing research. Indeed, some of the barriers identified by nursing professionals in Spain include nursing staff shortages, lack of time to develop new research ideas, insufficient institutional support to implement them, and limited funding opportunities.15,16
Nursing professionals have increasingly assumed leadership roles in research, prompting some authors to examine the implications of the latest 2024 revision of the Declaration of Helsinki for nursing research. These authors have analysed key updates and proposed practical strategies for nurse researchers, such as the use of artificial intelligence management tools, dynamic consent models and context-sensitive sustainability practices. This update also considers the constraints faced by nurse researchers working in underfunded and culturally diverse settings. 17 However, research ethics cannot be separated from the ethical climate and culture of everyday clinical practice. This entails consensus on standards of conduct and accepted ethical norms within an organisation, as well as staff perceptions of the ethical standards applied in their workplace and their most pressing ethical concerns. 18
Considering the above, the REC of our Health Area aims to explore nurses’ perceptions of this entity, identify potential gaps in theoretical knowledge or areas for improvement, and thereby contribute to strengthening nurses’ research capabilities. This, in turn, may support nurses in designing research studies that uphold participants’ rights, wellbeing and safety.
Objectives
General objective
To identify nurses’ knowledge regarding REC ethical and legal principles, and the accessibility of these committees for the conduct of research studies.
Specific objectives
• To compare knowledge of the REC and its accessibility between nurses who have previously conducted research studies and those who have not. • To compare the facilitators and barriers identified in the two study centres and their relationship with nurses’ knowledge of the REC and its accessibility.
Methods
Study design
A descriptive cross-sectional survey study. This study is reported in accordance with the STROBE guidelines for cross-sectional studies. 19
Participants and setting
The study population comprised 1,647 nurses employed at two tertiary-level hospitals within the Castilla y León Health Network in Spain, who were actively working during the study period (Hospital A: 918 nurses; Hospital B: 629 nurses).
The study was conducted between March and April 2025.
Sample size
Based on data from the annual research reports of both hospitals, it was assumed that 10% of nurses had previously conducted research studies and had knowledge of the REC. On this basis, with a precision of 5% and a confidence level of 95%, a minimum sample of 121 nurses from Hospital A and 117 nurses from Hospital B was required to obtain representative estimates.
Variables and data collection
Data were collected using a questionnaire developed by the research team based on current legislation governing RECs, including Law 14/2007 of 3 July on Biomedical Research, Royal Decree 1090/2015 of 4 December regulating clinical trials with medicinal products, Research Ethics Committees with Medicines and the Spanish Clinical Studies Registry, 6 and the recently published International Council for Harmonisation (ICH) Good Clinical Practice guidelines, specifically ICH E6(R3). 20
A pilot test was conducted to identify unclear items, and final consensus on the questionnaire was reached among REC members. The final questionnaire consisted of: • Four sociodemographic items: age, sex, years of professional experience as a nurse, and workplace. • • • • Two open-ended questions on facilitators and barriers to submitting a research project to the REC • An overall assessment of the REC using a Likert scale from 1 to 10, where one indicates a very negative assessment and 10 a very positive assessment.
The questionnaire was distributed via corporate email and through QR codes placed at nursing stations and work areas by unit managers. To ensure voluntary participation, a passive recruitment strategy was used. Hierarchical structures served only as channels for disseminating the link and QR code, without any role in the responses. Participation was entirely voluntary and depended solely on individual initiative, as staff could simply choose not to access the link. Responses were collected anonymously through a corporate digital platform, independent of the work environment, thereby minimising hierarchical influence. The first page of the questionnaire included the study aim, estimated completion time, and data use. Informed consent was obtained through a mandatory agreement item (‘I agree to participate freely and voluntarily’), which had to be completed to proceed.
Statistical analysis
Data were analysed using IBM SPSS Statistics for Windows, version 26.0. Quantitative variables are presented as mean and standard deviation, with minimum and maximum values (or as median and interquartile range where appropriate). Qualitative variables are presented as frequencies and percentages.
Associations between qualitative variables were analysed using Pearson’s chi-squared test. Comparisons of quantitative variables were performed using Student’s t-test for two groups and analysis of variance (ANOVA) when more than two groups were compared. A p-value < 0.05 was considered statistically significant.
In addition, a post-hoc power analysis was conducted to assess the ability of the performed contrasts to detect significant differences between groups, using the pwr statistical package in R software. The calculation was based on the comparison of two independent proportions using Cohen’s h as a measure of effect size, with a significance level of alpha = 0.05 and the specific sample sizes for each group.
For the formation and comparison of study groups, classification was based on dichotomous responses (‘Yes’ or ‘No’) to the corresponding questionnaire item. This categorisation enabled sample segmentation according to the presence or absence of the characteristic under study, facilitating statistical comparisons between groups.
Free-text responses were thematically coded, and participants’ arguments were summarised using absolute frequencies.
Ethical considerations
The researchers declare compliance with Organic Law 3/2018 of 5 December on Personal Data Protection and the guarantee of digital rights, which adapts Spanish legislation to Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016 (GDPR). Participants’ confidentiality and anonymity were preserved at all times. The study was approved by the REC of the Health Area under approval code PI-25-197-C.
The protocol was evaluated and approved exclusively by committee members not part of the research team or involved in study design or execution. To minimise bias, it was submitted anonymously, with evaluators acting as an independent subcommittee unaware that the committee itself was the subject of analysis. Members involved as researchers were excluded from deliberation and final decision-making, in accordance with the Committee’s standard operating procedures.
The questionnaire was hosted within the Microsoft 365 environment of the Regional Health Authority information systems. A specific paragraph informed participants of, and requested consent for, the dissemination of study results in scientific forums.
Results
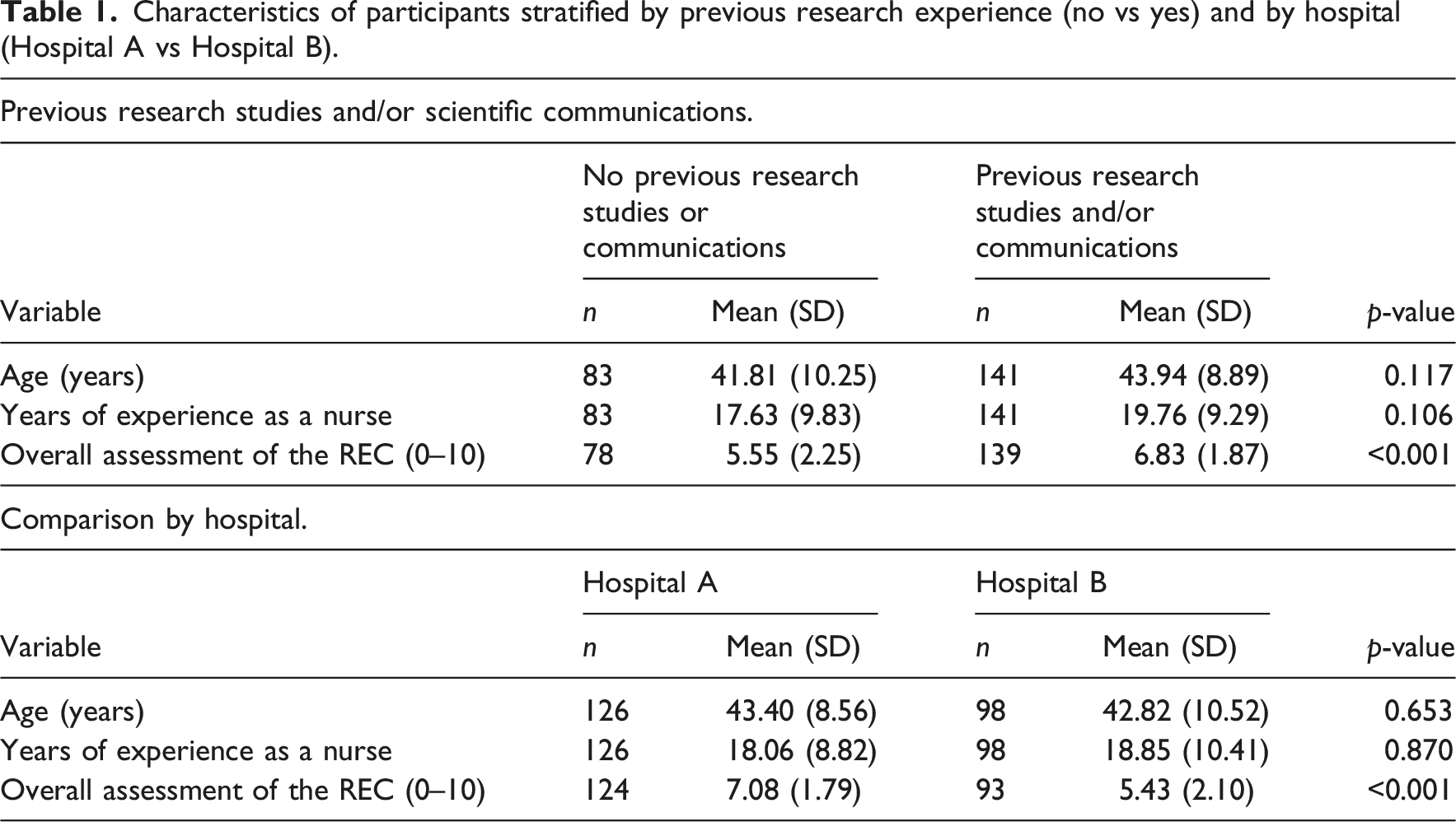
Out of a total population of 1,647 nurses, 224 valid responses were obtained (response rate: 13.6%), with 126 (13.7%) from Hospital A and 98 (15.6%) from Hospital B. The mean age was 43.15 years (SD 9.45), and the mean length of professional experience as a nurse was 18.97 years (SD 9.53). Of the participants, 17.4% (n = 39) were men and 82.6% (n = 185) were women. Regarding workplace, 56.3% (n = 126) were employed at Hospital A and 43.8% (n = 98) at Hospital B.
Overall, 42.4% (n = 95) of participants reported having conducted at least one research study, of whom 92.6% (n = 88) had applied for REC approval, compared with 7.4% (n = 7) who had not. Additionally, 58.0% (n = 130) reported having participated in scientific meetings or conferences with scientific communications, excluding literature reviews; among these, 70.8% (n = 92) had applied for REC approval, whereas 29.2% (n = 38) had not. In total, 141 participants reported having conducted previous research studies and/or presented scientific communications, of whom 66.0% (n = 93) were from Hospital A and 34.0% (n = 48) from Hospital B.
Characteristics of participants stratified by previous research experience (no vs yes) and by hospital (Hospital A vs Hospital B).
Items from sections 1, 2 and 3 and frequency of correct responses in the total sample.
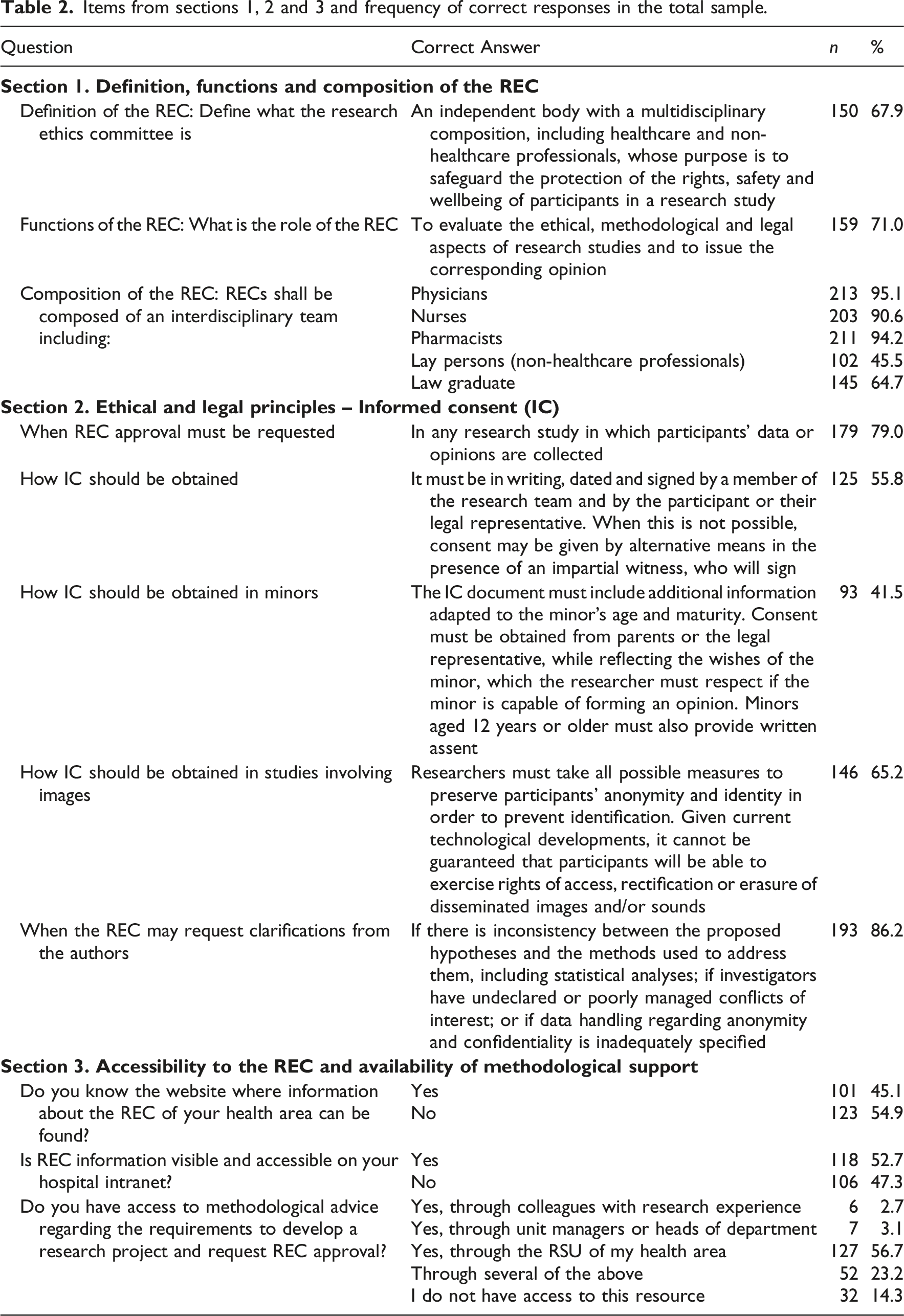
With regard to accessibility, approximately half of respondents reported knowing where to find information about the REC, and more than half indicated that they had access to methodological support through the Research Support Unit (RSU) to develop a research project and submit it to the REC.
Comparison of knowledge and accessibility between participants with and without previous research experience.
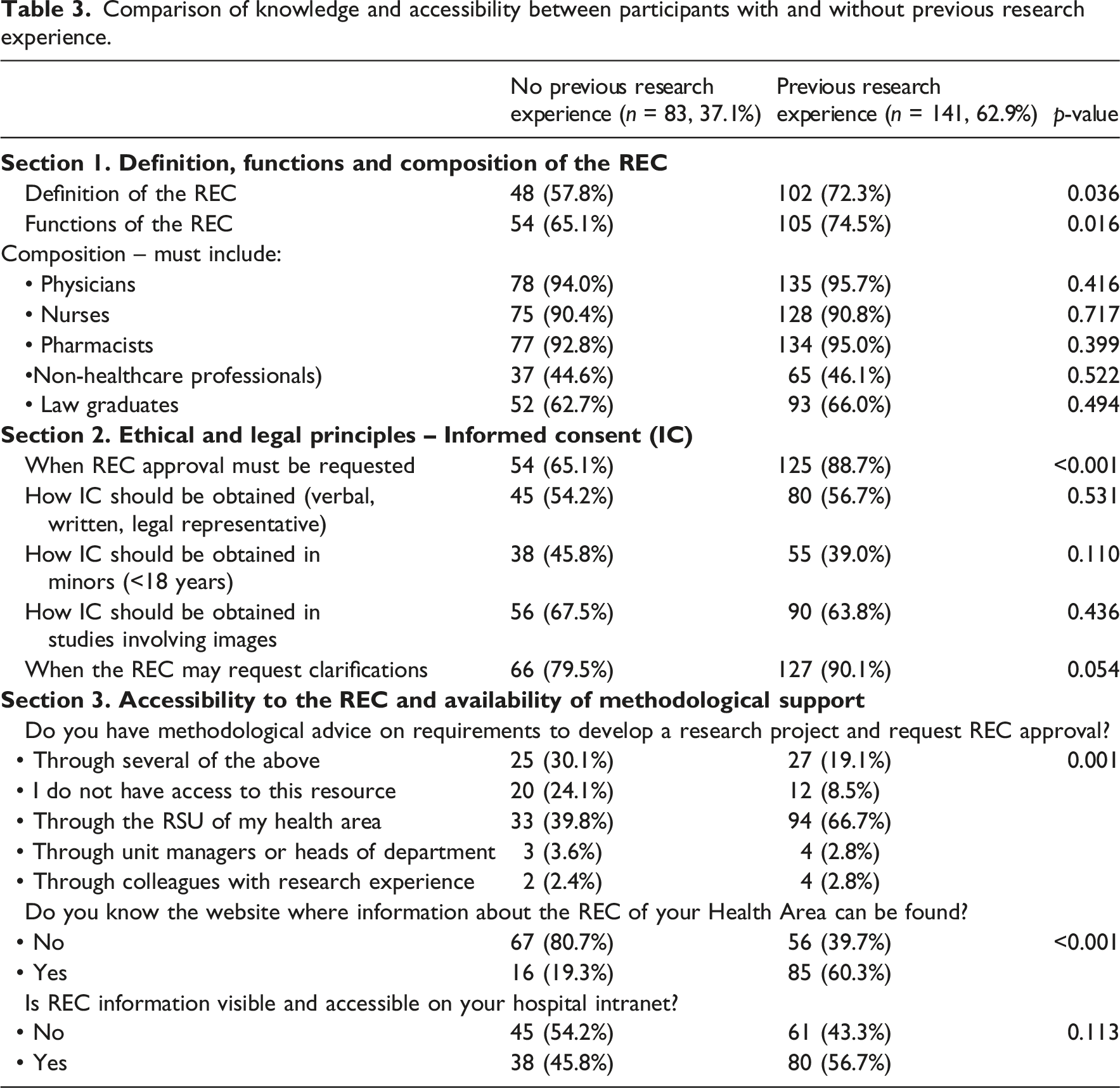
Regarding accessibility, participants with previous research experience most frequently reported having received support through the RSU, compared with other sources of support, and were more likely to report knowing the REC website. In both groups, the visibility of REC information on the hospital intranet was reported by 46% and 56% of participants, respectively.
Comparison of the frequency of correct responses between nurses from Hospital A and Hospital B.
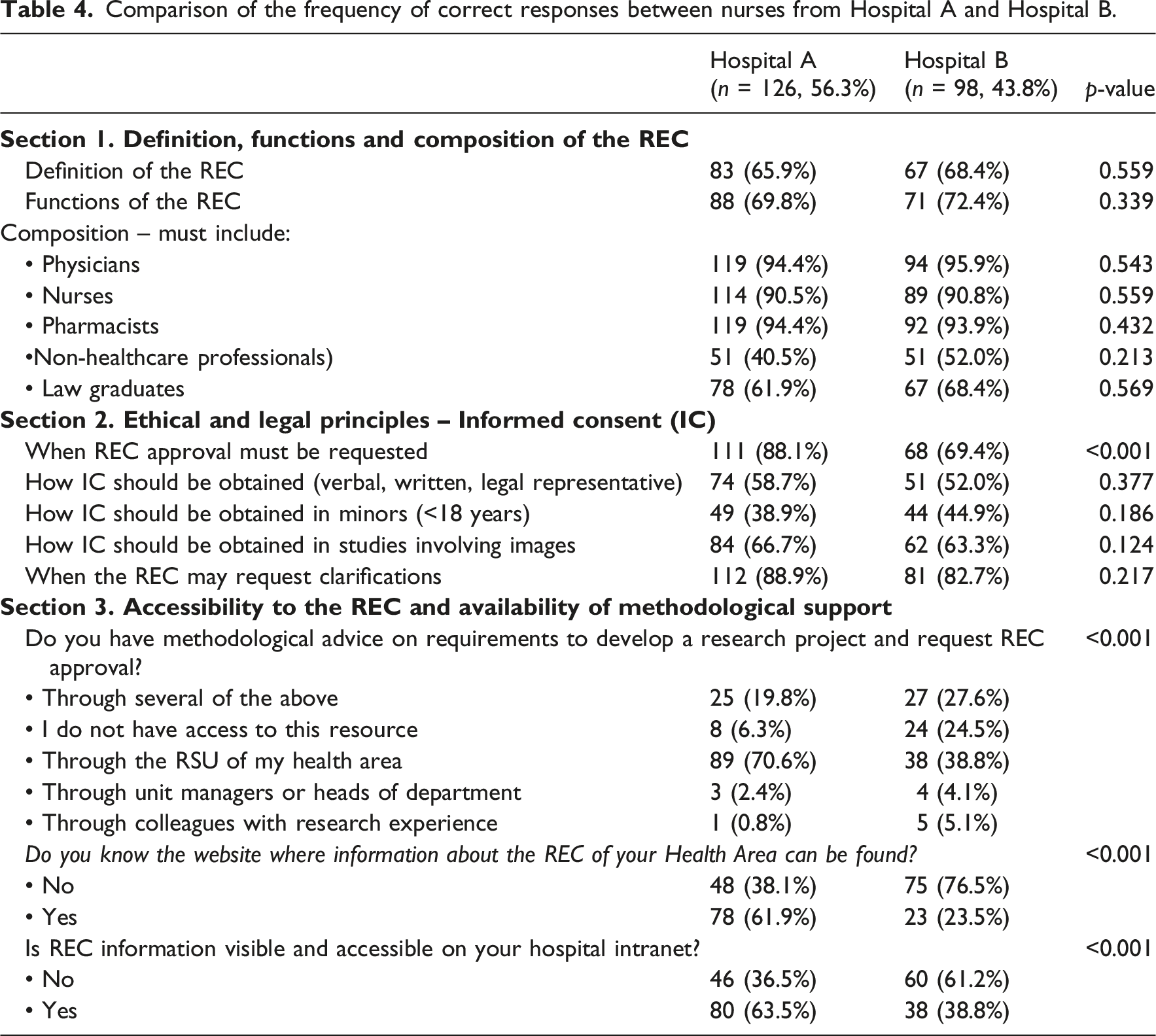
The post-hoc power analysis conducted using group specific sample sizes (n = 83 vs n = 141 for previous research experience; n = 126 vs n = 98 for hospitals) shows high power (estimated >0.80) for variables with marked nominal differences, which suggests the robustness of the significant findings, whereas low power in non-significant contrasts indicates that these variables would require larger sample sizes to detect small differences.
Barriers and facilitators identified by participants, stratified by previous research experience (no vs yes) and by hospital (Hospital A vs Hospital B).
Discussion
The study population showed high rates of correct responses regarding the definition and functions of the REC, with some errors concerning its composition. This indicates adequate knowledge of the general functioning of the REC, including when and how to access it and how to respond to requests for clarifications. However, only around half of the participants considered it accessible, correctly identified how IC should be obtained, and an even smaller proportion correctly addressed IC in studies involving minors. This study also provides an opportunity to explore the main barriers and facilitators reported by participants, according to their prior research experience and whether they worked in Hospital A or B.
Comparison of nurses with prior research experience versus those without
Nurses who had previously conducted research studies demonstrated higher frequencies of correct responses than those who had not. This is logical and aligns with other studies, which show that a lack of prior research experience limits understanding of the importance of REC and increases barriers to implementing the necessary ethical procedures in scientific studies. 21 However, no differences were observed between the two groups regarding the composition of the REC, particularly in relation to non-healthcare professionals such as a layperson or a legal expert. A layperson contributes a citizen’s perspective, while a law graduate provides a legal-normative viewpoint. This suggests limited knowledge of the regulatory framework and the functioning of the REC, as well as a possible undervaluation of the interdisciplinary and citizen role in ethical decision-making, since these two figures serve as representatives of patients and ensure pluralism and protection of their rights. Other studies have similarly identified areas for improvement in healthcare professionals’ knowledge of current REC regulations. 22
No differences were found between the groups in relation to obtaining IC from research participants, particularly in paediatric populations. This is a critical point and represents a challenge for nurses in research due to the inherent complexity of the process and the need to communicate clear, relevant information to the patient. IC is not only a legal requirement but also an ethical cornerstone that ensures informed, voluntary participation, reinforces research credibility, and dignifies professional nursing research practice. 23 Lack of knowledge in this area may lead to REC requests for clarifications, causing delays in the research process, postponement of publications, and potential loss of professional credibility.24,25 This gap in knowledge regarding proper IC management may be explained by the relatively recent and difficult integration of nurses into research in Spain, which has historically been dominated by descriptive and low-complexity studies. Nevertheless, in recent years there has been an increase in doctoral-level studies and those with greater methodological rigour and social impact, which require solid ethical and legal standards. 13 IC is a complex process that requires specific training, advanced communication skills, and a strong commitment to participant protection. 26 Special attention should be given to studies involving children, where IC ensures respect for their dignity, protects their rights, and guarantees voluntary and ethical participation, preventing exploitation or harm. Comprehensive knowledge in this area is essential as a safeguard of participants’ rights and research integrity 27 . Similarly, the use of images must be limited to the purposes authorised in the consent, with proper storage and access, in compliance with current data protection regulations. 28 Therefore, the absence of statistically significant differences, coupled with consistently low effect sizes, suggests a uniformly limited level of knowledge among nursing staff. This indicates that prior research experience was not a differentiating factor in this context, as a significant disparity in knowledge would likely have been reflected in larger effect sizes.
Accessibility and available support for accessing the REC
The results highlight a significant gap in accessibility. Nurses with prior research experience reported receiving methodological support for accessing the REC, particularly via the RSU, and were aware of the REC website. However, no significant differences were found in terms of visibility and accessibility through the hospital intranet. This underscores the need to improve institutional dissemination of REC information and to strengthen accessible communication channels for all staff, regardless of research experience. It is essential that the REC be integrated into institutional life, with adequate resources, trained members, and transparent procedures for consultation requests from all professionals. 29
Comparison of results between hospital A and B
This analysis addresses the potential relevance of research management in different hospitals across two health areas, reflecting different levels of organisational research culture. In fact, participants with prior research experience were twice as numerous in Hospital A compared to Hospital B. This prior experience may explain differences in knowledge between hospitals: Hospital A demonstrated significantly better results regarding when REC approval should be sought, availability of methodological support via the RSU, and greater accessibility to the REC website and intranet resources. These differences may relate to the management of the RSU in both hospitals, including mentorship programmes, research management, and support activities. Notably, in Hospital A, the nurse responsible for the RSU is also a REC member. This may have been perceived as a facilitator by RSU users, promoting the integration of ethical considerations from the study’s conceptual phase, including its justification and potential benefits. RSU users receive guidance not only on methodological aspects of their projects but also in the implementation of good research practices, with the RSU nurse acting as consultant and educator. This aligns with studies highlighting the importance of organisations employing nurse bioethicists to integrate methodology and ethics in nursing research, facilitating access to institutional resources and supporting colleagues in resolving ethical issues.30,31
Another factor potentially contributing to Hospital A’s better results in ethical knowledge and REC accessibility is its participation in the national Nursing Research Challenge® programme, promoted by the Spanish National Association of Nursing Managers. This programme aims to foster nursing research within healthcare organisations in Spain, with managers facilitating research by clinical nurses. 32
Barriers and facilitators
Lack of knowledge or insufficient training was identified as the main barrier across all groups, particularly among nurses without prior research experience and those in Hospital B. This is crucial for addressing ethical challenges in increasingly complex clinical and scientific settings. Incorporating nurses with expertise in ethics into research teams and continuing education programmes should be a key institutional strategy to ensure integrity and excellence in health research33,34. Integration into undergraduate curricula is also essential to equip students with the necessary knowledge and skills in research ethics before entering professional practice, as well as in postgraduate training. 35
Accessibility and communication were identified as both barriers and facilitators. Although long response times, bureaucracy, and documentation were not considered barriers by most respondents, these findings are important for the REC to consider when designing strategies to improve communication and professional accessibility.
The RSU was highlighted as the main facilitator, especially in Hospital A and among professionals with prior research experience. This indicates that the RSU promotes the development of ethical competencies and methodological guidance, fostering good research practices.
Our findings highlight the structural challenges that exist in Spain regarding training in research ethics. The limited integration of REC into university education may contribute to delays in acquiring competencies in this area. Furthermore despite the current regulatory framework (Royal Decree 1090/2015), the practical application of these principles is not always perceived as fully integrated into clinical practice. In this context, REC are sometimes viewed more as an administrative requirement than as an ethical and legal safeguard. This perception, combined with time constraints in clinical practice, could diminish professional commitment and underscores the need for formal training and nurse-led support throughout the research process, in accordance with other authors.36,37 These factors, taken together, may have influenced the levels of knowledge observed in our study.
Limitations
The main limitation of this study is that it was restricted to two specific health areas, which limits the generalisability of the findings, although it addresses the objectives set out. Additionally, the lack of randomisation in the study population and the participation rates obtained may indicate self-selection bias, with a possible overrepresentation of more motivated professionals or those with greater interest. Since no information was available on non-respondents, it was not possible to compare the two groups, which limits the assessment of non-response bias and restricts the generalisability of the findings.
The low power observed in non-significant comparisons should be interpreted in light of the available sample size, particularly in comparisons between hospitals, as this reflects a limited ability to detect small differences. Consequently, these results should be interpreted with caution, and future studies with larger sample sizes would be needed to confirm these findings.
Conclusions
Participants demonstrated a high proportion of correct responses regarding the definition and functions of the REC and correctly identified the members from healthcare professions. However, knowledge was limited regarding the inclusion of a layperson and a legal expert. Areas for improvement were also identified in knowledge related to obtaining informed consent in studies involving minors or the use of images, and only around half of participants considered the REC accessible.
The main barrier identified was lack of knowledge or insufficient training, while the RSU was regarded as the principal facilitator.
Implications for practice
Considering these findings, education in research ethics should be strengthened within nursing curricula at both undergraduate and postgraduate levels, as well as within continuing professional development programmes in healthcare institutions. This need is consistent with international evidence which points to a persistent gap between ethical standards and their application, reflecting a structural problem in knowledge of and access to REC.18,21 In this regard, it is essential to promote institutional support mechanisms, such as mentoring and nurse-led, to facilitate the integration of ethics into research practice from the outset. Adapting these strategies to different organisational contexts will be key to advancing toward an ethically sound research culture.
This study should also encourage REC members to develop new strategies and accessible institutional resources, such as guidelines, repositories, and rapid consultation channels, to facilitate access and communication for professionals interested in conducting research.
New lines of research could evaluate educational and management interventions aimed at improving nurses’ ethical, procedural, and regulatory knowledge regarding the REC, thereby ensuring the ethical and regulatory quality of research led or coordinated by nurses.
Footnotes
Acknowledgements
The authors wish to thank all the nurses who kindly responded to this survey. The members of the RCE of the Valladolid Areas are gratefully acknowledged for their unconditional support.
Author contributions
Conceptualisation: M. Fernández-Castro, B. Martín-Gil and J.M. Alonso-Fernández
Data curation: B. Martín-Gil, M. Fernández-Castro, and J.M. Alonso-Fernández
Formal analysis: M. Fernández-Castro, N. Rivas-González and I. Alcoceba-Herrero
Methodology: J. Álvarez-González and M. Fernández-Castro
Supervision: B. Martín-Gil, J. Álvarez-González, M. Fernández-Castro and N. Rivas-González
Writing – original draft: M. Fernández-Castro, B. Martín-Gil and J.M. Alonso-Fernández
Writing – review and editing: B. Martín-Gil, M. Fernández-Castro and J. Álvarez-González.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Valladolid Ethics Committee for Research with medicinal products (ECRmp), under the reference code PI-25-197-C. At all times, the anonymity of those surveyed was maintained, in accordance with Basic Law 3/2018 of 5 December 2018 on the Protection of Personal Data and Guaranteeing of Digital Rights. Participants provide consent scientific purposes
Data Availability Statement
Data will be available upon request to the authors.