
Abstract
Background
Frontline nurses and nurse leaders faced profound psychological, ethical, and professional challenges during the COVID-19 pandemic. Less attention has been given to how meaning in life supports moral resilience and ethical nursing practice during prolonged public health crises.
Research question/aim
This study aimed to explore how frontline nurses and nurse leaders experienced pandemic-related stress, constructed meaning in life, and developed moral resilience within pandemic clinical settings.
Research design
A descriptive phenomenological design was used, and data were analysed using Giorgi’s descriptive phenomenological method.
Participants and research context
Semi-structured in-depth interviews were conducted with 18 participants, including 14 frontline nurses and four nurse leaders, from four hospitals in southern Taiwan.
Ethical considerations
The study was approved by an institutional review board, and all participants provided informed consent.
Findings
Three major categories were identified: crisis conditions and ethical pressures, meaning-making as a source of moral resilience, and transformative meaning, professional identity, and moral agency. Meaning-making enabled frontline nurses to connect suffering with patient care, teamwork, and professional commitment, while nurse leaders constructed meaning through staff support, ethical decision-making, and reflective leadership.
Discussion
Meaning in life functioned not only as a psychological coping resource but also as an ethical resource supporting moral resilience, moral agency, and professional identity.
Conclusions
Meaning-centred reflection, moral resilience training, peer support, and reflective leadership development should be incorporated into organisational crisis preparedness to strengthen ethical nursing practice during future public health emergencies.
Introduction
Large-scale public health crises jeopardise not only healthcare workers’ physical and psychological well-being but also destabilise their sense of professional purpose and moral identity. During the COVID-19 pandemic, frontline nurses and nurse leaders were exposed to sustained clinical demands, rapidly evolving protocols, social stigma, and ethically complex situations. Research has documented high levels of fatigue, insomnia, psychological distress, and moral tension among healthcare professionals during the pandemic.1,2
While existing studies have extensively described stress, burnout, and psychological symptoms, less attention has been given to how nurses sustain ethical practice, professional commitment, and moral agency during prolonged crisis conditions. In particular, limited qualitative research has examined how meaning in life supports moral resilience within real-world pandemic care, especially across hierarchical nursing roles. This gap is important because frontline nurses and nurse leaders encounter ethically demanding situations from different positions: frontline nurses are directly involved in patient care and nurse–patient relationships, whereas nurse leaders are responsible for decision-making, staff support, and the coordination of care under uncertainty.
Understanding how frontline nurses and nurse leaders construct meaning amid crisis is essential for supporting professional commitment, safeguarding psychological well-being, and strengthening ethical nursing practice during future large-scale public health emergencies. By linking meaning in life with moral resilience, this study moves beyond a primarily psychological account of coping and examines how nurses sustain ethical commitment, professional identity, and moral agency in morally demanding care contexts. The inclusion of both frontline nurses and nurse leaders further enables comparison of how meaning-making operates across direct caregiving roles and leadership responsibilities. Therefore, this study aimed to explore how frontline nurses and nurse leaders experienced pandemic-related stress, constructed meaning in life, and developed moral resilience within pandemic clinical settings.
Background
Meaning in life encompasses an individual’s perception that life is coherent, purposeful, and significant. Three key dimensions of meaning – coherence, purpose, and significance – help individuals organise life experiences and guide future actions. 3 Coherence reflects the ability to integrate experiences into an understandable narrative; purpose refers to having direction and goals; and significance involves perceiving one’s life as valuable and connected to something larger.
These perspectives align with theoretical arguments suggesting that understanding and purpose form core psychological foundations for human resilience, 4 and with Frankl’s assertion that individuals who understand ‘why’ they live can endure almost any ‘how’. 5 Within high-pressure healthcare environments, these dimensions may shape how nurses interpret ethical dilemmas, sustain motivation, and enact leadership responsibilities.
Moral resilience further extends this discussion into the domain of nursing ethics. Moral resilience has been conceptualised as the capacity to restore or sustain integrity in response to moral adversity. 6 In clinical nursing contexts, this concept is particularly relevant because nurses often encounter situations in which professional values, patient needs, institutional demands, and personal safety may come into tension. From this perspective, moral resilience is not simply the ability to endure stress, but an ethically grounded capacity to maintain alignment between one’s values, commitments, and actions when facing morally challenging circumstances.
During the COVID-19 crisis, frontline nurses and nurse leaders experienced intense physical strain, emotional distress, ethical dilemmas, role conflict, family separation, and social stigma. Meaning in life has been identified as a crucial psychological resource that strengthens resilience, mitigates stress, and facilitates psychological growth during adversity.7,8 However, limited qualitative research has examined how meaning in life contributes to moral resilience within ethically demanding nursing contexts. In particular, few studies have explored how meaning-making supports frontline nurses’ caregiving roles and nurse–patient relationships, while also sustaining nurse leaders’ ethical decision-making and responsibility for staff support. Addressing this gap may clarify how meaning in life functions not only as a psychological resource, but also as an ethical resource for sustaining professional identity, moral agency, and ethical nursing practice during public health crises.
This study integrates data from two descriptive phenomenological inquiries conducted at different stages of a large-scale public health crisis to explore frontline nurses’ and nurse leaders’ lived experiences of stress, coping, and meaning-making. By focussing on both frontline nurses and nurse leaders, this study provides deeper insight into how meaning in life functioned as a psychological foundation for moral resilience and ethical leadership in pandemic clinical settings.
Theoretical framework
This study was informed by existential psychology, contemporary multidimensional models of meaning in life, and nursing ethics. Existential psychology emphasises that individuals can endure suffering when they are able to identify purpose and meaning within adversity. 5 In addition, multidimensional conceptualisations describe meaning in life as comprising coherence, purpose, and significance.3,4 These theoretical perspectives provided an interpretive lens for understanding how participants integrated crisis experiences into meaningful professional narratives and enacted moral resilience across hierarchical nursing roles.
This framework was further informed by nursing ethics, particularly the concept of nurses as moral agents. Nurses are accountable for their own nursing practice and are responsible for making decisions and taking actions consistent with the obligation to promote health and provide optimal care. 9 From this perspective, moral agency refers not only to ethical awareness, but also to nurses’ capacity to make ethically grounded judgements, assume professional responsibility, and act in ways that uphold patient well-being and dignified care. In this study, moral agency provided an ethical lens for interpreting how participants reaffirmed professional identity and ethical commitment during pandemic-related uncertainty.
Care ethics also informed the interpretation of participants’ meaning-making. In nursing, care ethics emphasises relational responsibility, responsiveness to patients’ needs, and the moral significance of sustaining caring relationships. Care ethics is closely connected to nursing workload, as workload may affect nurses’ capacity to enact caring practices, maintain relational care, and respond to patients’ needs. 10 This perspective was particularly relevant to the present study because participants described providing care under conditions of high workload, infection risk, isolation policies, and disrupted nurse–patient relationships. Care ethics therefore provided a lens for understanding how meaning-making was linked to nurses’ continuing efforts to sustain caring responsibilities within constrained and ethically demanding pandemic care environments.
Virtue ethics provided an additional ethical lens for interpreting nurses’ meaning-making as the enactment of professional character in crisis. Rooted in Aristotelian thought, virtue ethics emphasises the cultivation of moral character and virtues such as practical wisdom, courage, temperance, and justice. 11 In nursing and health care teams, this perspective may help explain how professionals seek to act well under uncertainty, pressure, and relational responsibility. Virtue ethics offers a valuable framework for health care teams and nursing leaders, particularly in the post-COVID-19 context of burnout, incivility, turnover, and the need to rebuild healthy practice environments. 12 In the present study, virtue ethics helped interpret participants’ meaning-making as more than psychological adjustment; it also reflected the practice of professional virtues, including courage, compassion, responsibility, and practical wisdom, within morally demanding care and leadership situations.
The study
Aim(s)
The aim of this study was to explore how frontline nurses and nurse leaders experienced pandemic-related stress, constructed meaning in life, and developed moral resilience within pandemic clinical settings.
Research question
How did frontline nurses and nurse leaders construct meaning in life and sustain moral resilience and ethical leadership during a large-scale public health crisis?
Technical terminology used to describe the Aim(s)
This study employed a descriptive phenomenological approach to examine lived experiences related to meaning in life, moral resilience, moral agency, and ethical leadership. The terminology of ‘meaning in life’ was informed by multidimensional conceptualisations encompassing coherence, purpose, and significance.3,4 It was also grounded in existential psychological perspectives. 5 ‘Moral resilience’ was conceptualised as the capacity to sustain or restore integrity in response to moral adversity within clinical contexts. 6 In this study, ‘moral agency’ referred to nurses’ capacity to make ethically grounded judgements, assume professional responsibility, and take action to uphold patient well-being and dignified care. Care ethics was used as an interpretive ethical lens for analysing caregiving responsibilities and nurse–patient relationships. 10 Virtue ethics was used as an additional interpretive ethical lens for understanding how nurses and nurse leaders sought to act well under uncertainty, pressure, and relational responsibility.11,12 In this study, this lens helped interpret participants’ meaning-making as involving professional virtues such as courage, compassion, responsibility, and practical wisdom in morally demanding care and leadership situations.
Methods
Design
A descriptive phenomenological design was adopted to explore the lived experiences of frontline nurses and nurse leaders during the COVID-19 pandemic. Phenomenology provides a structured approach to understanding how individuals give meaning to their experiences within specific contexts.13,14 Giorgi’s descriptive phenomenological method was selected because it provides a rigorous and psychologically grounded framework suited for nursing research.15,16 Consistent with phenomenological principles, researchers engaged in bracketing to set aside preconceptions and focus on participants’ authentic descriptions. 17
Study setting and recruitment
Participants were recruited from four hospitals in southern Taiwan. Purposive sampling was used to recruit individuals with direct experience providing care for patients with confirmed COVID-19 or supervising frontline nursing teams during the pandemic. Recruitment continued until data saturation was achieved.
Inclusion and/or exclusion criteria
Inclusion criteria were:
Direct involvement in COVID-19 clinical care or supervisory responsibilities.
Willingness to participate in an in-depth interview.
There were no specific exclusion criteria beyond lack of direct pandemic clinical involvement.
Data collection
Semi-structured, in-depth interviews were conducted between March 14 and July 29, 2022. An interview guide was developed based on the study aim and relevant literature on meaning in life, moral resilience, and pandemic-related stress.
The interview guide explored the following domains: • Experiences of working during the pandemic • Sources of stress and ethical challenges • Coping strategies and support systems • Perceived changes in professional identity • Meaning-making processes and personal reflections on life
Example guiding questions included: • ‘How would you describe the working atmosphere during the pandemic?’ • ‘What sustained your motivation to continue working during this period?’ • ‘How did the pandemic influence your view of life?’
Follow-up prompts and clarifying questions were used to deepen exploration of participants’ lived experiences.
All interviews were conducted in private conference rooms to ensure confidentiality and comfort. Interviews were audio-recorded with participant consent and transcribed verbatim within 24 h.
A reflective journal was maintained throughout the data collection process to enhance transparency and reflexivity. 18
Data analysis
Data were analysed using Giorgi’s descriptive phenomenological method, which involves:15,16 1. Reading transcripts for holistic understanding; 2. Identifying meaning units; 3. Transforming meaning units into psychologically sensitive expressions; 4. Synthesising these into an essential structure of the phenomenon.
Each transcript was independently coded by at least two researchers. Differences in interpretation were resolved through discussion until consensus was reached. Bracketing was maintained throughout the analytic process to minimise researcher bias. 17
Ethical considerations
Ethical approval for this study was granted by the Antai Medical Care Corporation Antai-Tian-Sheng Memorial Hospital Institutional Review Board (TSMH IRB No. 21-126-B; approved December 15, 2021). All participants provided informed consent. Confidentiality was assured through coded identifiers, and the study adhered to the principles of the Declaration of Helsinki.
Rigour and reflexivity
Trustworthiness was established using the criteria of credibility, dependability, confirmability, and transferability. 19 Credibility was enhanced through member checking.20,21 Purposive sampling ensured information-rich cases aligned with the research aim. 22
Reflexive journals were maintained throughout the research process to document analytic decisions and researcher positioning. 18 The research team reflected on their clinical and academic roles to minimise potential interpretive bias and to maintain awareness of how prior experiences may have influenced analysis. This study is reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist (see Supplemental File 1).
Findings
Characteristics of participants
Participant characteristics.
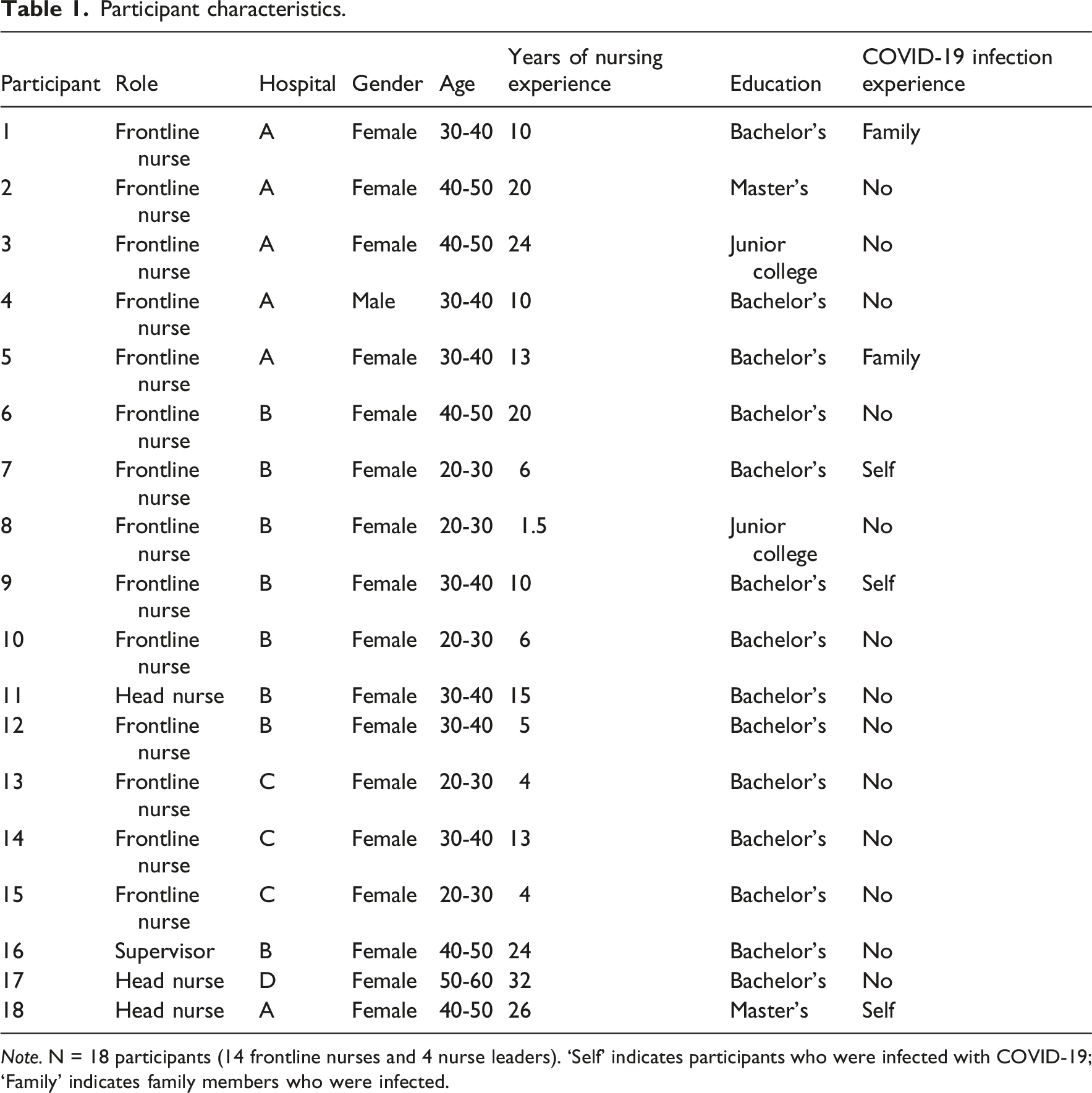
Note. N = 18 participants (14 frontline nurses and 4 nurse leaders). ‘Self’ indicates participants who were infected with COVID-19; ‘Family’ indicates family members who were infected.
Analysis yielded three analytically distinct categories that reflected a developmental trajectory of participants’ lived experiences during the pandemic. The first category describes the crisis conditions and ethical pressures that disrupted participants’ professional and personal lives. The second category explains how participants reconstructed meaning through caregiving, teamwork, responsibility, and leadership commitment. The third category captures the longer-term transformation of life values, professional identity, and moral agency. An integrative synthesis was subsequently conducted to articulate the essence of the lived experience across participants.
Crisis conditions and ethical pressures
Overwhelming workload and physical exhaustion
Both nurses and leaders described persistent physical fatigue resulting from prolonged work hours and the demands of wearing multilayer protective gear. Heat, dehydration, and rashes were common. After twelve hours inside the ward, my uniform was soaked through. Taking off the gown felt like peeling off another layer of my skin. (NA4)
Nurse leaders reported similar exhaustion but concealed it to maintain team morale: Even if I was tired, I couldn’t let my staff see it. I had to stay strong for them. (LA1)
Fear of infection and anxiety for family
Fear of contagion was universal. Many nurses isolated themselves from loved ones to protect them: I stopped hugging my kids for months. I was terrified I might bring the virus home. (NB3)
Leaders carried additional anxiety regarding staff safety: Every day I worried that one of my nurses would test positive. That would mean I failed to protect them. (LB2)
Emotional isolation and social stigma
Participants described social avoidance from neighbours and acquaintances: People thanked nurses on TV, but in real life they avoided us. (NC6) Even taxi drivers didn’t want to take us when they heard we worked in the hospital. (LC3)
Moral dilemmas in the face of suffering
Witnessing patient deaths in isolation created moral distress: I understood the rules, but it felt cruel to see a patient die without anyone beside them. (ND7)
Leaders struggled when required to enforce policies that conflicted with their personal values: Sometimes I had to insist on policies I didn’t fully agree with. It broke my heart. (LD2)
Initial coping through team support, humour, and faith
Participants described team support, humour, and faith as immediate ways of coping with the intense emotional pressure of pandemic care. These strategies did not remove the ethical burden of the crisis, but they helped participants continue working in situations marked by uncertainty, fear, and exhaustion: We joked during short breaks just to release pressure. (NE1) The overall atmosphere was highly tense; however, staff members consistently supported one another and aligned with my leadership in carrying out the assigned tasks. (LE4)
These shared experiences reflected collective vulnerability and the ethical pressure of sustaining care under prolonged crisis conditions, while also foreshadowing the solidarity and meaning-making processes described in the next category.
Meaning-making as a source of moral resilience
While the first category described the crisis conditions and ethical pressures participants encountered, this second category explains how they interpreted these experiences and reconstructed meaning through patient care, teamwork, professional responsibility, and leadership commitment. Meaning-making did not eliminate fear, exhaustion, or moral tension; rather, it enabled participants to connect their suffering with professional purpose and to sustain their commitment to ethical nursing practice.
Frontline nurses: Finding meaning through patient care
For frontline nurses, meaning-making emerged through direct patient care despite physical exhaustion and emotional strain. Rather than describing burden alone, participants connected difficult care experiences with professional pride, patient recovery, and recognition from patients and families. Although protective equipment complicated routine procedures and limited sensory clarity, nurses continued to interpret their work as meaningful when they perceived that their care was helpful to patients: Drawing blood became very difficult because we wore two to three layers of gloves. (NF2) I was dripping wet in the protective suit… the mask always became foggy, so everything I saw was blurry. (NF11) I feel a sense of achievement when my patients tell their family members that I did a good job… moments like this always make me happy. (NF12)
Nurse leaders: Constructing meaning through responsibility and ethical leadership
For nurse leaders, meaning-making was closely connected to responsibility for staff support, care coordination, and decision-making under uncertainty. Although leaders experienced administrative scrutiny, emotional labour, and moral tension, they interpreted these demands as part of their ethical responsibility to protect both patients and staff. Their accounts showed that leadership during the pandemic was not experienced merely as managerial pressure, but as a form of moral commitment enacted through difficult decisions and sustained guidance of others: Every phone call from the director made my heart race. I had to justify every decision. (LG1) I couldn’t show weakness. If I broke down, the team would collapse. (LG4) I wanted to protect my nurses, but management demanded more shifts. (LG3) Being a leader meant guiding others through fear. It wasn’t easy, but it made me stronger. (LH2)
Transformative meaning, professional identity, and moral agency
The third category captures how participants’ meaning-making extended beyond immediate coping and contributed to longer-term transformation in life values, professional identity, and moral agency. Participants did not describe the pandemic only as a period of suffering; rather, they reflected on how crisis experiences reshaped their understanding of life, nursing, and ethical responsibility.
Rediscovering the value of life and health
Participants described renewed appreciation for life, health, and family. The pandemic led them to reconsider what they regarded as most important and to shift attention from external achievement to the preservation of life and relationships: I used to chase promotions. Now I just want my family safe and healthy. (NI5) This crisis reminded me that life itself is precious. (LI1)
These reflections suggested that meaning-making involved a reorientation of personal values. For some participants, the crisis intensified awareness of human vulnerability and strengthened appreciation for ordinary forms of safety, health, and family connection.
Reaffirming professional identity and moral agency
Participants also described a renewed sense of professional identity. Their accounts showed that being a nurse during the pandemic was not understood merely as fulfilling a job requirement, but as responding to a moment of profound social and ethical need. Remaining in their roles despite fear and uncertainty became a way of reaffirming who they were as nursing professionals: When people needed us most, we didn’t back down. That’s the meaning of being a nurse. (NJ10)
For nurse leaders, professional identity was closely linked to responsibility, compassion, and ethical leadership. Leadership was not framed as authority alone, but as the ability to guide others while carrying responsibility for both staff and patients: Leadership is not power – it’s compassion with responsibility. (LJ4)
These narratives suggest that meaning-making strengthened participants’ moral agency by helping them interpret their professional roles as ethically significant. Through continuing to care, make decisions, and support others under crisis conditions, participants reaffirmed their capacity to act in accordance with professional values and ethical commitments.
Spiritual reflection and ethical growth
Some participants engaged in spiritual reflection as part of their meaning-making process. These reflections did not remove the hardship of pandemic care, but helped participants interpret the crisis as an opportunity for humility, gratitude, courage, and empathy: Every crisis has a lesson. For me, it was humility and gratitude. (NK6) I believe God placed me there to learn courage and empathy. (LK3)
Spiritual reflection therefore contributed to ethical growth by helping participants connect suffering with personal transformation and professional values. For these participants, the pandemic became a context in which they reconsidered not only the fragility of life, but also the kind of nurse or leader they aspired to become.
Essence of the experience
Integrating perspectives across both groups, the essence of the lived experience revealed a developmental trajectory from crisis conditions and ethical pressure toward meaning reconstruction, professional reaffirmation, and moral resilience. For frontline nurses, meaning emerged through direct patient care, nurse–patient relationships, teamwork, and the recognition that their care remained valuable despite fear and exhaustion. For nurse leaders, meaning was grounded in responsibility for staff support, care coordination, ethical decision-making, and reflective leadership under uncertainty. Across both groups, meaning-making enabled participants to connect suffering with professional purpose, sustain moral agency, and reaffirm the ethical significance of nursing during a large-scale public health crisis.
Discussion
This study advances understanding by conceptualising meaning in life not merely as a psychological coping resource, but as an ethical and existential resource that supports moral resilience, moral agency, and ethical leadership across hierarchical nursing roles. By including both frontline nurses and nurse leaders, the findings show how meaning-making operated differently yet complementarily across direct caregiving and leadership responsibilities. For frontline nurses, meaning was grounded in patient care, nurse–patient relationships, teamwork, and continued commitment to compassionate care. For nurse leaders, meaning was linked to responsibility for staff support, ethical decision-making, care coordination, and reflective leadership under uncertainty. These findings contribute to nursing ethics by showing how meaning in life may help nurses sustain professional identity and ethical practice in morally demanding crisis contexts.
Emotional and physical burden as catalysts for meaning-making
Frontline nurses reported substantial physical exhaustion, emotional distress, and fear of contagion – experiences consistent with research describing insomnia, fatigue, and psychosocial strain among healthcare workers during COVID-19.1,2 In this study, however, these burdens were not experienced solely as psychological stressors. They also disrupted nurses’ capacity to sustain ordinary forms of relational care, particularly when infection-control measures, isolation policies, and heavy workload constrained nurse–patient interaction.
From the perspective of care ethics, these findings suggest that meaning-making emerged through nurses’ continued efforts to respond to patients’ needs and preserve caring relationships under constrained conditions. This interpretation is consistent with the view that nursing workload is closely connected to care ethics because workload may affect nurses’ capacity to enact caring practices, maintain relational care, and respond to patients’ needs. 10
These findings remain consistent with meaning in life theories that emphasise coherence, purpose, and significance as central dimensions of meaning,3,4 and with Frankl’s view that meaning enables individuals to endure hardship with purpose. 5 However, the present findings extend this psychological account by showing that, in pandemic nursing care, meaning-making also functioned as an ethical process through which nurses reaffirmed the moral importance of caring for isolated and vulnerable patients.
Moral responsibility and ethical leadership among nurse leaders
In highly uncertain and rapidly evolving public health crises, nurse leaders assume simultaneous responsibility for clinical quality, workforce safety, staff support, and care coordination. 23 Prior research has shown that nurse managers faced heavy workloads, negative emotional reactions, fear of infection, crisis-management challenges, and moral burden during the COVID-19 pandemic, particularly when making decisions that required balancing care needs with staff safety. 24
Similarly, care unit managers were required to support nurses under heavy stress, respond to staff anxiety, and coordinate work resources to meet rapidly changing clinical demands. 25
Consistent with these studies, nurse leaders in the present study described sustained decision fatigue, administrative scrutiny, emotional labour, and moral tension. However, the findings extend previous research by showing how leadership responsibility itself became a source of meaning. Participants did not interpret their role merely as managerial duty; rather, they reframed leadership as ethical stewardship, expressed through protecting staff, maintaining team morale, coordinating care, and making difficult decisions under uncertainty.
From a nursing ethics perspective, this reframing is important because it shows how meaning-making supported nurse leaders’ moral resilience and ethical leadership. By connecting administrative and clinical pressures with professional responsibility, nurse leaders were able to sustain their commitment to both patient care and staff well-being. Thus, meaning in life functioned not only as a personal coping resource, but also as an ethical resource that helped nurse leaders maintain moral responsibility and reflective leadership during a prolonged public health crisis.
Resilience through purpose, connection, and professional identity
Across both frontline nurses and nurse leaders, meaning in life emerged as a critical source of moral resilience. Participants described resilience not merely as endurance, but as an ongoing reconstruction of purpose, connection, and professional significance in the midst of suffering. This interpretation is consistent with the conceptualisation of moral resilience as the capacity to restore or sustain integrity in response to moral adversity. 6 From this perspective, the participants’ resilience was not simply psychological adaptation; rather, it involved maintaining alignment between professional values, ethical commitments, and actions under morally challenging conditions.
The findings also extend existing meaning in life literature. While previous studies have shown that meaning contributes to adaptive coping and buffers psychological distress during adversity,3,7 the present study shows that meaning-making in pandemic nursing care was closely connected to ethical practice. Participants derived meaning from teamwork, shared mission, patient improvement, and leadership responsibility. These sources of meaning helped them sustain professional identity and continue acting in accordance with nursing values despite fear, exhaustion, and moral tension.
This ethical dimension is important because moral suffering in nursing arises when ethical conflict, uncertainty, or competing commitments threaten nurses’ integrity and well-being. Unresolved ethical challenges may undermine nurses’ well-being, teamwork, integrity, and safe, high-quality care. 26 In the present study, meaning-making appeared to help participants respond to such challenges by reconnecting suffering with professional purpose and by reaffirming their commitment to patients, colleagues, and ethical nursing practice.
Ethical tensions and the search for significance
Both frontline nurses and nurse leaders encountered ethically complex situations, including enforcing isolation policies, balancing personal safety with professional duty, responding to patient suffering, and managing limited resources. These situations were not only stressful but also morally distressing, because participants often knew what compassionate or appropriate care required, yet were constrained by infection-control policies, organisational demands, or resource limitations. Similar ethical tensions have been reported among nurses caring for patients with COVID-19, including moral distress related to uncertainty, infection risk, personal protective equipment, and restrictions on usual caregiving roles. 27
The present findings further show that meaning-making helped participants respond to these ethical tensions by reaffirming the significance of their professional role. Rather than interpreting moral distress only as a source of psychological burden, participants used reflection, teamwork, patient care, and leadership responsibility to reconnect their suffering with ethical commitment. This interpretation is consistent with evidence that frontline nurses during COVID-19 faced ethical challenges when safety requirements conflicted with patient care, yet some nurses demonstrated moral courage by acting in ways they believed supported compassionate care and patients’ best interests. 28
Thus, the search for significance in this study was closely linked to ethical practice. Meaning-making enabled participants to transform ethically distressing experiences into opportunities for reaffirming their identity as compassionate professionals and sustaining moral agency in challenging clinical contexts. This process reflects the view that meaning enables individuals to endure suffering with purpose, 5 while extending this existential insight into nursing ethics by showing how meaning may support moral resilience and ethical action during public health crises.
Meaning-making as ethical practice: Moral agency, care ethics, and virtue ethics
Taken together, the findings suggest that nurses’ meaning-making during the COVID-19 pandemic was not merely an internal psychological process, but also an ethical practice through which participants reaffirmed moral agency, caring responsibility, and professional virtues. In line with the ANA Code of Ethics, nurses may be understood as moral agents who are accountable for their nursing practice and responsible for making decisions and taking actions consistent with the obligation to promote health and provide optimal care. 9 In the present study, participants’ moral agency was expressed through their efforts to continue caring for patients, support colleagues, make difficult decisions, and preserve professional integrity under crisis conditions.
Care ethics further clarifies the relational dimension of this process. Participants’ meaning-making was closely linked to their efforts to sustain caring relationships despite isolation policies, infection-control restrictions, workload pressures, and disrupted nurse–patient interaction. From this perspective, meaning in life supported not only individual endurance, but also the ethical commitment to remain responsive to patients’ needs and to preserve dignified care in constrained environments.
Virtue ethics provides an additional interpretation of these findings. From this perspective, participants’ meaning-making may be understood as the enactment of professional virtues in morally demanding care and leadership situations. Frontline nurses demonstrated courage and compassion by continuing to care for isolated and vulnerable patients, whereas nurse leaders demonstrated responsibility and practical wisdom by supporting staff, coordinating care, and making difficult decisions under uncertainty. Thus, meaning in life functioned as an ethical resource that helped participants sustain moral resilience, professional identity, and ethical nursing practice during a prolonged public health crisis.
Strengths and limitations of the work
A strength of this study is the inclusion of both frontline nurses and nurse leaders across four hospitals, allowing comparison of meaning-making processes across hierarchical roles. The descriptive phenomenological design enabled in-depth exploration of lived experiences and the identification of an essential structure of meaning in crisis contexts. However, the study was conducted in a single geographic region, which may limit transferability to other healthcare systems or cultural contexts.
Recommendations for further research
Future research should explore longitudinal trajectories of meaning-making beyond acute crisis periods and examine intervention-based approaches designed to strengthen moral resilience. Cross-cultural comparisons may further clarify how organisational and sociocultural contexts influence the development of meaning in life among nurses and nurse leaders.
Implications for policy and practice
The findings suggest that meaning-making should be incorporated into nursing-specific interventions designed to support moral resilience during public health crises. Rather than addressing nurses’ distress solely through stress management, healthcare organisations should provide structured opportunities for nurses to reflect on ethically challenging experiences, reconnect with the meaning of patient care, and reaffirm professional identity. Meaning-centred reflective debriefing sessions may be integrated into routine post-shift discussions, particularly after situations involving patient isolation, end-of-life care, moral distress, or conflict between infection-control requirements and compassionate care.
For frontline nurses, interventions should focus on sustaining relational care under constrained conditions. Unit-based reflective discussions, peer-support groups, and ethics rounds may help nurses process emotional strain, discuss morally difficult cases, and identify ways to preserve dignified nurse–patient relationships even when usual forms of contact are limited. These strategies may strengthen nurses’ moral resilience by helping them connect daily caregiving tasks with professional values, patient dignity, and the ethical significance of compassionate care.
For nurse leaders, training should include moral resilience, ethical decision-making, reflective leadership, and staff-support skills. Nurse managers need support not only in operational crisis management, but also in managing the moral burden of decisions involving staffing, resource allocation, infection risk, and workforce safety. Formal mentorship programmes pairing senior leaders with emerging nurse managers may provide a space for reflective dialogue, emotional support, and ethical consultation during prolonged crises.
At the organisational level, institutions should establish peer-support networks, ethics consultation mechanisms, and crisis response teams that explicitly address the ethical dimensions of nursing work. Embedding meaning-centred reflection and moral resilience training into disaster preparedness plans may help sustain professional identity, reduce moral distress, and promote workforce stability. Because public health crises occur across diverse cultural and healthcare contexts, these interventions should be adapted to local organisational structures, cultural expectations regarding caregiving, and available ethical support resources.
Conclusion
This study provides an in-depth exploration of how frontline nurses and nurse leaders constructed meaning, navigated ethical challenges, and sustained moral resilience during a large-scale public health crisis. Across hierarchical nursing roles, participants demonstrated a developmental process in which crisis-induced stress and ethical pressure prompted reflective meaning reconstruction. Through integrating emotionally and morally challenging experiences into coherent professional narratives, participants strengthened their sense of purpose, reaffirmed the significance of nursing, and sustained their commitment to ethical practice.
Meaning in life – encompassing coherence, purpose, and significance3,4 – functioned not only as a foundational psychological structure, but also as an ethical resource that supported moral resilience, moral agency, and professional identity. Consistent with the conceptualisation of moral resilience as the capacity to sustain or restore integrity in response to moral adversity, 6 the findings suggest that meaning-making helped participants maintain alignment between professional values, ethical commitments, and actions under morally demanding conditions. For frontline nurses, meaning emerged primarily through patient care, nurse–patient relationships, teamwork, and continued commitment to compassionate care. For nurse leaders, meaning was closely linked to moral responsibility, staff support, decision-making under pressure, and ethical stewardship.
These findings contribute to nursing ethics by showing how meaning-making may help nurses maintain professional integrity and ethical commitment when ordinary caregiving relationships and leadership responsibilities are disrupted by crisis conditions. Embedding meaning-centred reflection, moral resilience training, peer support, and reflective leadership development within organisational crisis preparedness may strengthen ethical nursing practice and workforce sustainability in future public health emergencies.
Supplemental material
Suppplemental material - Meaning, moral resilience and pandemic nursing: A phenomenological study
Suppplemental material for Meaning, moral resilience and pandemic nursing: A phenomenological study by Mei-Hsiu Lee, Yu-Jyuan Lin, Li-Chen Yu, Szu-Mei Hsiao, Chin-Chin Hsu in Nursing Ethics
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Taiwan Nurses Association (No. TWNA-1111003).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.