
Abstract
Background
Nurses in neonatal intensive care units (NICUs) play a pivotal role in managing ethically complex care for infants at the threshold of viability. However, institutional hierarchies, policies, and relational dynamics may constrain nurses’ ability to voice concerns and influence decisions, contributing to moral distress and moral residue.
Aim
To explore how NICU nurses experience and enact moral agency under constraint during threshold-of-viability decision-making, and how these experiences shape moral distress and moral residue.
Research design
Hermeneutic phenomenological study, reported in accordance with COREQ guidelines.
Setting/Participants
A purposive maximum-variation sample of 28 registered nurses (≥12 months of NICU experience) was recruited from four Level III NICUs in one administrative region of the country.
Methods
Semi-structured interviews were conducted remotely via videoconferencing in Arabic or English, audio-recorded, and transcribed verbatim. Arabic transcripts were translated and verified through back-translation to ensure semantic and conceptual equivalence. Data were analysed using hermeneutic phenomenological thematic analysis, supported by NVivo.
Ethical considerations
Ethical approval was obtained from the relevant university institutional review board and participating clinical sites. Written informed consent was obtained, and confidentiality was ensured through pseudonymization and secure data management.
Findings
Four themes captured nurses’ ethical experience: (1) Navigating the Grey Zone: The Weight of Ambiguity; (2) Voiceless at the Bedside: Structural Constraints on Moral Agency; (3) The Insider–Outsider Paradox: Peripheral Participation in Ethical Deliberation; and (4) The Lingering Echo: Moral Residue and Its Professional Toll.
Conclusions
Nurses’ moral distress at the threshold of viability was closely linked to constrained moral agency in hierarchical, policy-bound decision-making environments. Strengthening nursing inclusion in ethical deliberation and embedding structured post-case debriefing are plausible organisational strategies to reduce cumulative moral residue.
Keywords
Introduction
Threshold-of-viability care places neonatal intensive care unit (NICU) nurses in ethically demanding situations where clinical uncertainty, parental vulnerability, and high-stakes treatment decisions converge.1–3 Although nurses are closely involved in the everyday delivery of care, their capacity to influence ethically consequential decisions may be limited, creating tension between professional responsibility and formal decision-making authority.4,5 This hermeneutic phenomenological study explores how NICU nurses experience and enact moral agency under constraint in threshold-of-viability care. Drawing on in-depth interviews with 28 registered nurses across four Level III NICUs, it examines how organisational, relational, and clinical conditions shape nurses’ ethical voice, advocacy, moral distress, and moral residue. By centring nurses’ interpretive accounts, this work contributes a nuanced understanding of constrained moral agency in neonatal care at the threshold of viability.
Background
Neonatal intensive care at the threshold of viability, operationally defined in this study as 22 weeks and 0 days to 24 weeks and 6 days of gestation (22 + 0 to 24 + 6 weeks), constitutes a high-stakes ethical environment in which decisions to initiate, escalate, limit, or withdraw life-sustaining treatment occur under profound prognostic uncertainty, time pressure, and heightened parental vulnerability.6,7 In this context, clinical choices have immediate implications for infant survival and suffering and may carry longer-term psychosocial consequences for families. 8 NICU nurses are continuously present at the bedside and sustain prolonged contact with parents; consequently, they observe infants’ clinical trajectories in granular detail, track shifts in parental understanding over time, and encounter ethically consequential moments that may be less visible within intermittent physician encounters.9–11 This proximity positions nurses as key ethical actors, expected to uphold professional commitments while operating within decision-making structures in which they may have limited authority. 12
Moral distress refers to the psychological and emotional suffering that occurs when clinicians judge a course of action to be ethically appropriate yet are unable to enact it because of institutional, relational, or clinical constraints.13,14 When such exposure is repeated and unresolved, moral distress may accumulate as moral residue, experienced as persistent compromised integrity, guilt, and self-reproach that extends beyond the immediate event.15,16 In neonatal intensive care units, commonly reported sources of constraint include hierarchical decision-making, limited access to formal ethical deliberation, and communication norms that restrict the articulation or uptake of nurses’ ethical concerns.17–19 These constraints may be intensified in viability-related care because uncertainty is structurally embedded: infants can rapidly improve or deteriorate, decisions must be revisited iteratively, and ethically salient trade-offs are rarely fully determined by protocols alone. 20
The concept of moral agency offers a necessary analytic lens for understanding how moral distress is produced and sustained in this setting.21,22 Moral agency in nursing encompasses the capacity to recognise ethically salient features of care, engage in deliberation and moral judgment, communicate concerns, and act in accordance with professional commitments to beneficence, nonmaleficence, and justice. 23 Importantly, moral agency is enacted within organisational and relational structures; they can be enabled or constrained by leadership practices, interprofessional norms, unit culture, and policy architecture.24,25 When nurses’ moral agency is constrained, distress may arise not only from the ethical complexity of care itself but also from repeated experiences of limited influence, silenced concerns, or moral accountability without commensurate decision authority.26,27
Although moral distress among NICU nurses has been documented, three limitations restrict the field’s capacity to generate actionable ethical and organisational responses.28,29 First, much of the literature emphasises prevalence and correlates rather than explicating the mechanisms through which moral agency becomes constrained during real-time ethical decision-making. 30 Second, viability-related care is often subsumed within broader neonatal ethics discussions, leaving the distinctive decision ecology of this period with extreme uncertainty, time-critical turning points, and emotionally charged deliberation insufficiently examined from nurses’ perspectives. 31 Third, existing work frequently reports moral distress without detailing how hierarchy, policy, and communication practices shape nurses’ participation and advocacy, or how these conditions contribute to moral residue and professional consequences. 32 Addressing these gaps is essential to inform ethically coherent neonatal intensive care practice and to guide leadership, policy, and educational strategies that protect nurses’ ethical integrity and support workforce sustainability.33,34
Research question/aim/objectives
Aim
To explore how NICU nurses experience and enact moral agency under constraint during ethical decision-making at the threshold of viability, and how these experiences shape moral distress and moral residue.
Research question
How do NICU nurses describe organisational, relational, and clinical conditions that constrain or enable moral agency during threshold-of-viability decision-making, and how do these conditions shape experiences of moral distress and moral residue?
Objectives
(1) To describe nurses’ experiences of moral distress in threshold-of-viability care. (2) To identify perceived organisational, relational, and clinical constraints on nurses’ moral agency (e.g., hierarchical communication, policy architecture, time pressure, prognostic uncertainty). (3) To examine how nurses describe their role in ethical deliberation, including participation, influence, indirect advocacy, or exclusion from decision processes. (4) To explore perceived consequences of constrained moral agency, including moral residue and impacts on professional practice, wellbeing, and intentions to remain in bedside care. (5) To elicit nurse-derived implications for ethically supportive leadership, policy, and education in neonatal intensive care at the threshold of viability.
Research design
Design/approach
This study used an interpretive (hermeneutic) phenomenological approach,35,36 to explore how NICU nurses experience and interpret moral agency under constraint during threshold-of-viability care. Hermeneutic phenomenology is appropriate when the objective is to develop an interpretive understanding of how individuals make meaning of ethically complex experiences embedded within specific relational and organisational contexts. Given the ambiguity, emotional intensity, and interprofessional power dynamics characteristic of viability-related care, this approach enabled in-depth examination of the meanings nurses attributed to ethical action, constrained voice, and enduring moral impact. 37 The manuscript is reported in accordance with the COREQ guidelines. 38
Theoretical framework
The study was informed by an integrated conceptual lens linking moral distress (as a constraint-based ethical phenomenon) with moral agency (nurses’ capacity to perceive ethically salient situations, deliberate, voice concerns, and act in accordance with professional values).39,40 Figure 1 represents a dynamic pathway in which threshold-of-viability clinical conditions (e.g., prognostic ambiguity, rapid deterioration/improvement, time-critical turning points, heightened parental vulnerability) interact with multi-level constraints (organisational policies, interprofessional hierarchy, workflow compression, and communication norms). These conditions shape moral agency processes (moral perception, deliberation, perceived legitimacy to speak, advocacy, and participation), which, in turn, influence moral outcomes, including moral distress, moral residue, and ethical engagement.
23
Conceptual framework linking clinical conditions, multi-level constraints, moral agency processes, and moral outcomes in threshold-of-viability NICU decision-making.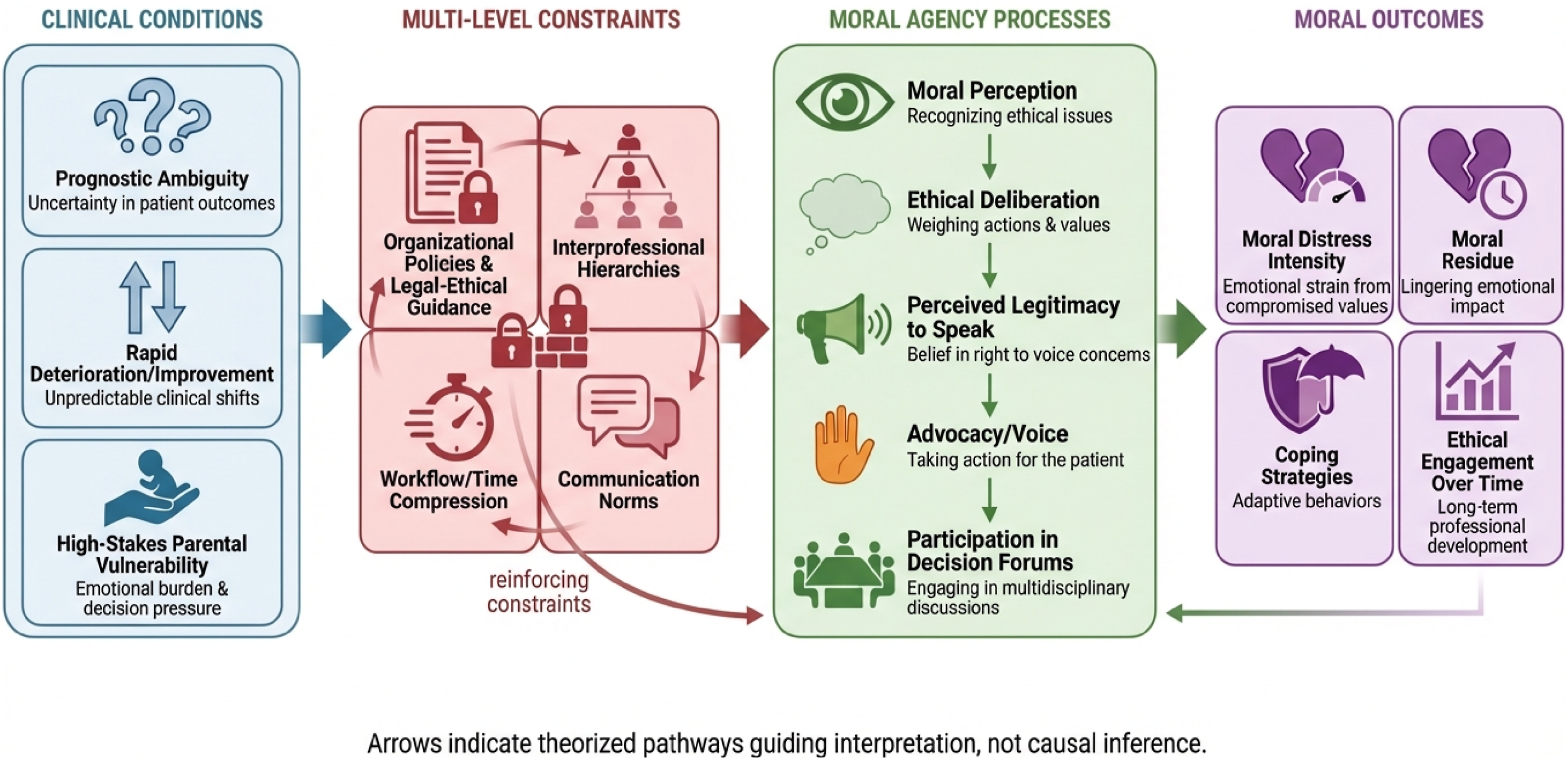
Consistent with interpretive phenomenology, the framework functioned as a sensitising concept rather than a deductive coding template. 41 It informed the research question and interview guide to ensure comprehensive coverage of key constructs while preserving openness to participants’ meanings. Analytically, the study adopted a primarily inductive stance: initial coding remained grounded in participants’ language; the framework was subsequently used during interpretation to examine how emergent themes mapped onto, refined, or challenged the proposed pathways. 42
Data collection
Data analysis
Data were analysed using hermeneutic phenomenological thematic analysis,49,50 managed in NVivo 12. 51 Analysis proceeded iteratively alongside data collection to refine developing interpretations and to guide sampling toward conceptual depth. Consistent with hermeneutic phenomenology, analysis moved recursively between detailed textual segments and the developing whole (the hermeneutic circle) to interpret meanings situated within clinical, organisational, and sociocultural contexts. Themes were treated as patterns of meaning rather than frequency-based categories; theme development was used as an analytic strategy to articulate shared meaning structures across accounts while retaining attention to contextual nuance and individual variability. 52
Transcripts were read and re-read alongside field notes (and audio where needed) to support interpretive immersion. 53 Two researchers independently coded the first five transcripts to enhance analytic sensitivity and surface divergent interpretations; differences were discussed to refine code meanings while preserving openness to multiple readings. Coding remained grounded in participants’ language and concrete accounts. Codes were clustered into provisional themes capturing patterned meanings related to constraints, moral agency processes, and moral outcomes. 54 The research team reviewed the developing thematic structure against coded extracts and the full dataset, refining boundaries, merging or splitting themes, and actively searching for disconfirming cases. 55 Themes were then defined with analytic clarity and aligned with the study aim. The sensitising framework informed interpretation and theme refinement but was not used as a deductive coding template, ensuring themes remained grounded in the data. 56 Analytic memos and an audit trail documented decisions throughout the coding and theme development process. Translated English transcripts were used for analysis; translation verification procedures are described in Section 4.3.
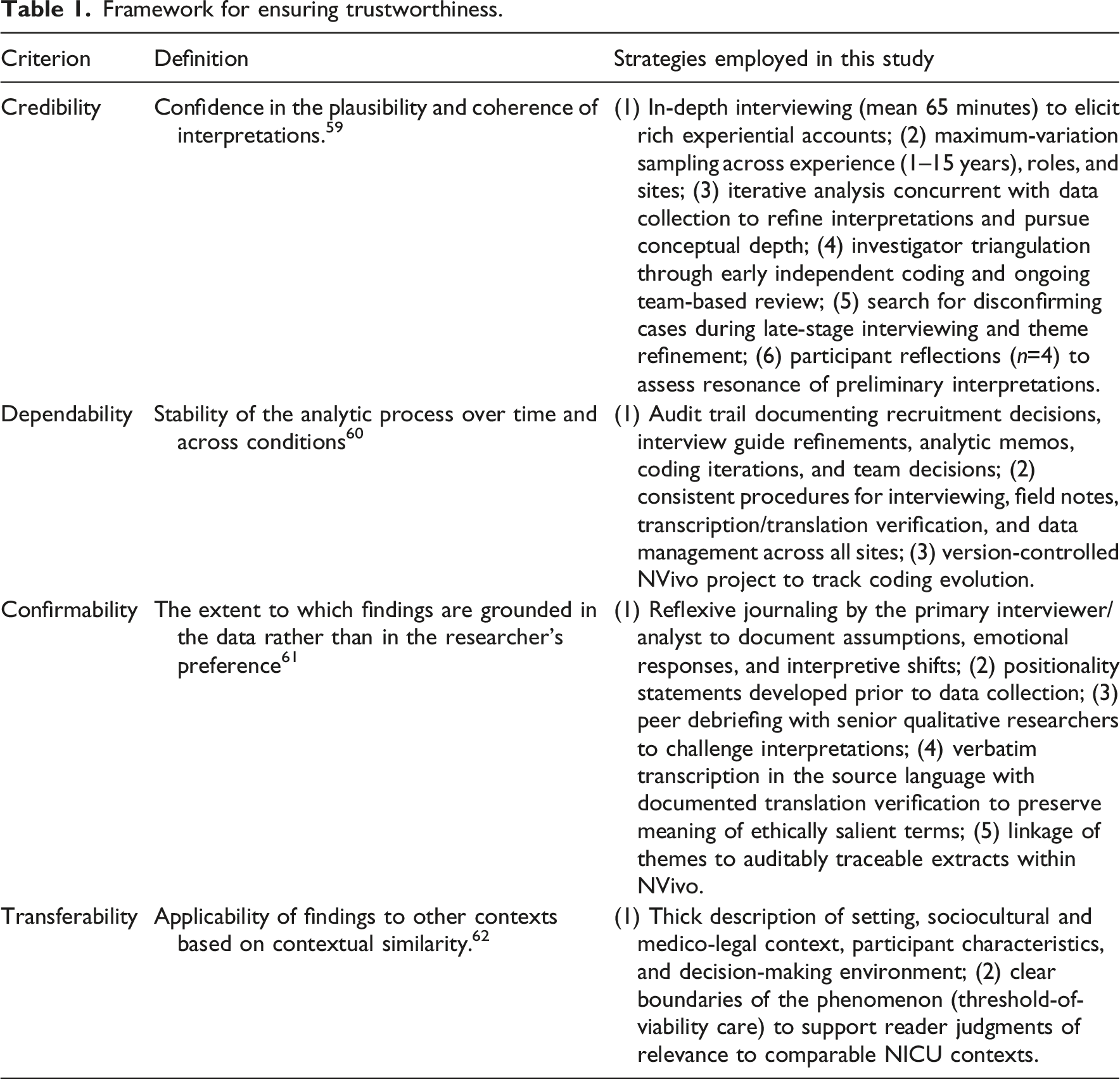
Rigour/trustworthiness
Framework for ensuring trustworthiness.
Reflexivity
Reflexivity was embedded throughout the study. 63 Strategies included 1 documented positionality statements prior to data collection; 2 ; reflexive journaling by the primary interviewer to track methodological decisions, emotional responses, and evolving interpretations; and 3 regular team debriefing to interrogate assumptions, consider alternative readings, and ensure interpretations remained grounded in the dataset.64,65
Participant reflections and interpretive integrity
Consistent with interpretive phenomenology, the study did not employ transcript-return or traditional member checking as a test of ‘accuracy’. Instead, rigour was strengthened through participant reflections focused on interpretive resonance. A summary of preliminary interpretations was shared with a purposively selected subset of participants (n = 4), chosen to reflect variation in years of NICU experience, clinical role, and hospital site; participants who had provided particularly detailed interview accounts were also preferentially included to support rich feedback on interpretive resonance. All four responded, indicating that the interpretations resonated with their experiences and that they did not identify any substantive misrepresentations. This process supported interpretive fidelity while maintaining the research team’s analytic responsibility.
Ethical considerations
Ethical approval was obtained from the relevant university institutional review board and the ethics committees of the participating clinical sites. Written informed consent was obtained from all participants before data collection. Participants were informed of their right to withdraw at any time without penalty. Confidentiality was protected through pseudonymization and removal of identifying details from transcripts and reports. Audio recordings, transcripts, and analytic materials were stored on encrypted, password-protected systems accessible only to the research team. Given the sensitive nature of discussions on ethically challenging care and moral distress, participants were reminded that they could pause or stop the interview at any point. A referral pathway for confidential counselling support was available if required, although no participant requested its use. Data management, retention, and disposal were conducted in accordance with ethics requirements and institutional policies.
Findings
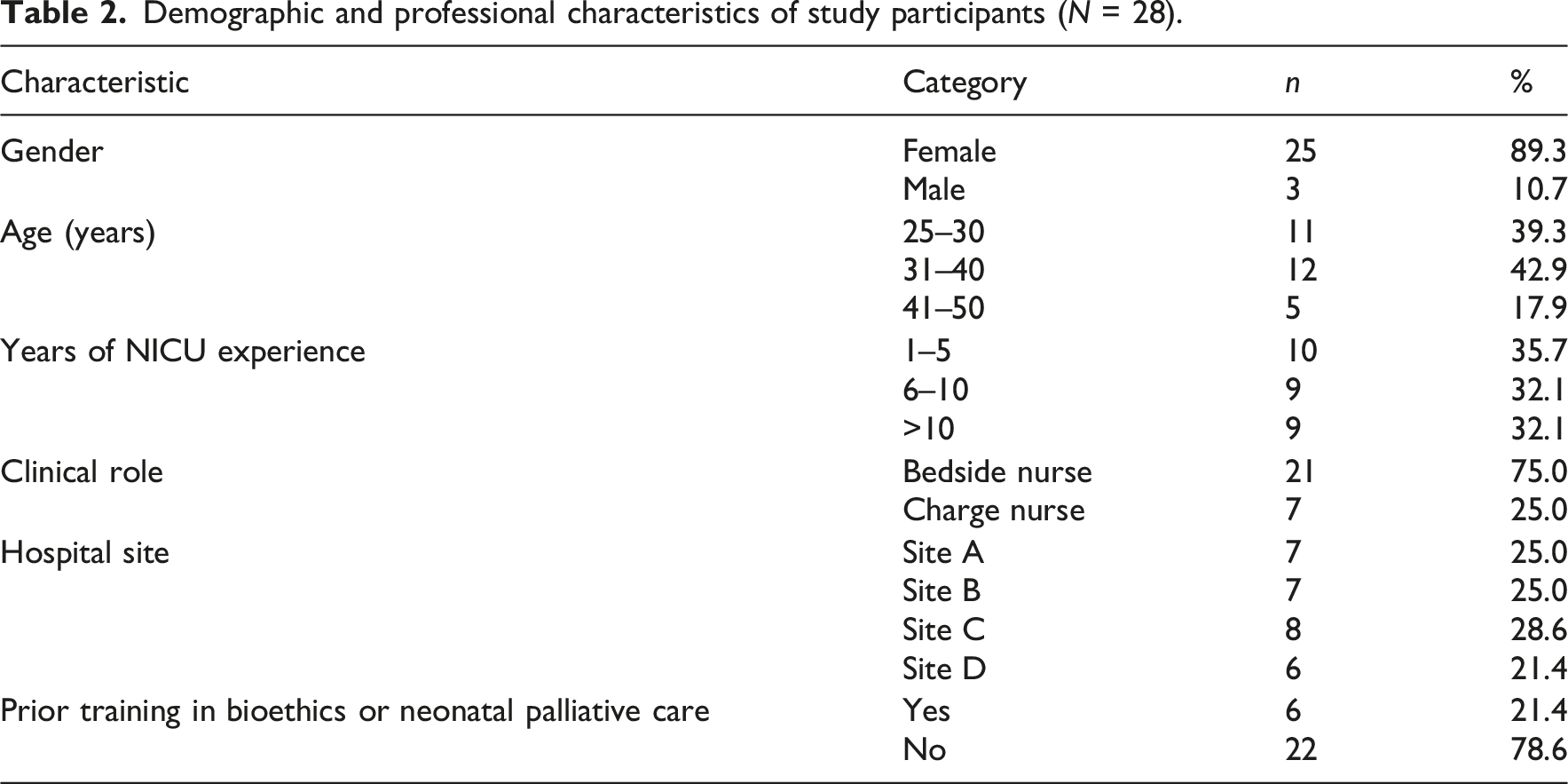
Demographic and professional characteristics of study participants (N = 28).
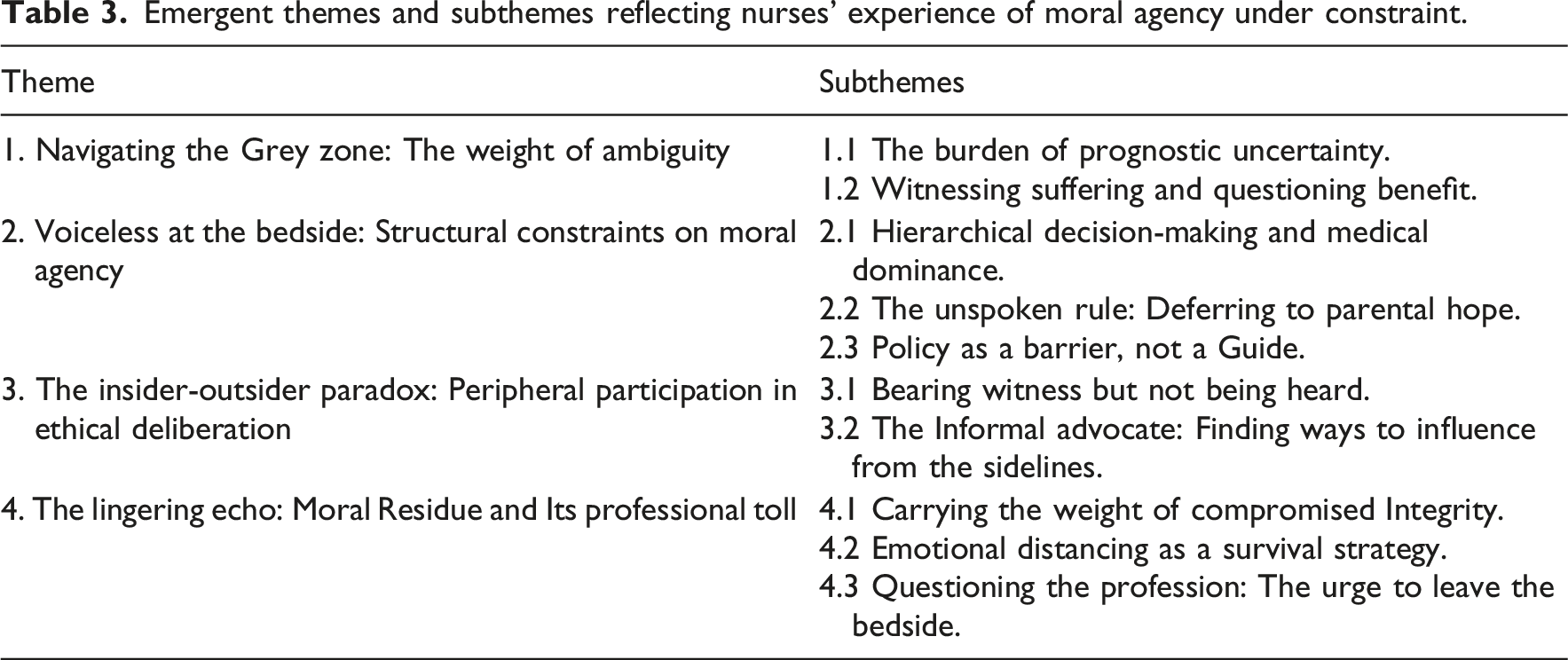
Emergent themes and subthemes reflecting nurses’ experience of moral agency under constraint.
Overview of the participants
Twenty-eight registered nurses from four Level III NICUs in the study setting participated. The sample was predominantly female (n = 25, 89%), included nurses across bedside and charge roles, and represented a broad range of ages and NICU experience (Table 2). Participants were distributed across all sites, supporting the interpretation of recurring patterns across different unit contexts. A senior nurse described the enduring emotional weight associated with viability-related decisions: ‘Whether you have been here two years or twenty, the weight of these decisions never really leaves you. It just changes how you carry it’ (Participant 19, 14 years’ experience).
Key themes identified
Four themes and ten subthemes were developed to address how nurses experienced moral agency under constraint during threshold-of-viability decision-making, how constraints shaped participation and advocacy, and how these experiences contributed to moral distress and moral residue. Themes and subthemes are summarised in Table 3.
Theme 1: Navigating the Grey Zone: The Weight of Ambiguity
This theme captures the moral and emotional burden nurses described when providing intensive care under conditions of extreme prognostic uncertainty. Moral distress was often rooted in the experience of acting amidst ambiguity, delivering invasive interventions while simultaneously questioning the likelihood of benefit and the meaning of ‘doing good’ in rapidly shifting clinical trajectories.
The burden of prognostic uncertainty
Participants described viability-related care as psychologically taxing because infants’ trajectories could change abruptly, creating a persistent tension between hope and anticipated loss. This uncertainty was experienced as ethically consequential because it complicated nurses’ ability to reconcile aggressive treatment with their bedside observations of fragility and decline: You are doing everything, every procedure, every line, on a baby that weighs 500 grams. And in the back of your mind, you are constantly asking, ‘For what?’ … it’s a heavy, heavy burden to carry when you don’t know if you are helping or just prolonging the inevitable. (Participant 04, 5 years’ experience) The hardest part is the rollercoaster… That constant swing between hope and despair is exhausting… Am I doing the right thing? No one can tell you for sure. (Participant 21, 11 years’ experience)
Witnessing suffering and questioning benefit
Nurses frequently described moral distress as intensified by their role as frontline witnesses to infant discomfort and procedural pain. They reported experiencing a conflict between executing treatment plans and perceiving themselves as active agents in infant suffering: We are the ones inflicting the pain… There are days when you feel like a torturer, and you go home with that feeling. It eats away at you. (Participant 15, 8 years’ experience)
One nurse described how emotional responses after an infant’s death could become ethically distressing in themselves, contributing to lingering residue: …a part of me felt… relief. Relief for him. And then comes the guilt… That’s the residue. It stays with you. (Participant 28, 15 years’ experience)
Interpretive synthesis: Across accounts, ambiguity functioned as a moral pressure amplifier. Nurses described distress not only from difficult outcomes, but from sustaining ethically consequential actions in a space where certainty and closure were rarely possible.
Theme 2: Voiceless at the bedside: Structural Constraints on Moral Agency
This theme identifies organisational and relational constraints that participants experienced as limiting their moral agency. Nurses described moral distress as closely tied to situations in which they perceived ethically salient concerns but lacked the legitimacy to raise, pursue, or influence them within formal decision-making pathways.
Hierarchical decision-making and medical dominance
Participants commonly described decision-making as physician-led, with nursing input valued primarily for implementation and monitoring rather than ethical judgment. Attempts to raise ethically oriented concerns were described as crossing an implicit boundary: The plan is made on rounds… The attending decides… You become a pair of hands. (Participant 09, 4 years’ experience) I once tried to raise a concern in a family meeting… ‘We will handle the medical plan.’ … my observations were welcome, but my ethical judgment was not. (Participant 17, 12 years’ experience).
The unspoken rule: Deferring to parental hope
Nurses described pressure to align with parental hope and cultural expectations to ‘do everything’, even when their own assessments raised concerns about futility or suffering. This was experienced as a constraint that restricted honest ethical communication and intensified feelings of complicity: The parents are clinging to a miracle… You feel like you are participating in a fantasy. (Participant 02, 3 years’ experience) …the family’s hope is sacred… The path of least resistance is to just keep going. (Participant 25, 9 years’ experience)
Policy as a barrier, not a guide
Participants described policies as rigid or insufficiently responsive to clinical nuance, framing them as mechanisms that could compel ethically troubling actions rather than support deliberation: We have a policy that says we must resuscitate any baby over 23 weeks… the policy ties your hands. (Participant 11, 7 years’ experience) The guidelines are black and white, but these babies are grey… It’s a checklist… even if your gut… is screaming no. (Participant 20, 10 years experience)
Interpretive synthesis: Nurses described constrained moral agency as structurally produced: hierarchy, norms surrounding hope, and policy rigidity collectively narrowed what could be said, by whom, and with what consequences.
Theme 3: The insider-outsider paradox: Peripheral Participation in Ethical Deliberation
This theme describes a paradox in which nurses perceived themselves as insiders to the infant’s lived clinical reality, yet outsiders to formal ethical deliberation. Participants described being morally and emotionally proximate to infants and families while simultaneously positioned at the margins of decision authority.
Bearing witness but not being heard
Participants described holding ‘human data’ about infant suffering, subtle clinical changes, and family dynamics that they perceived as ethically relevant but difficult to integrate into physician-dominated deliberations: I am with the baby for 12 hours… I have all this data, this human data, but there is no place to put it… The story of the baby gets lost. (Participant 07, 6 years’ experience) You feel like a silent observer… It’s like you are behind a glass wall. (Participant 14, 9 years’ experience)
The informal advocate: Finding ways to influence from the sidelines
In response to limited formal influence, nurses described indirect strategies to advocate for infants and families, including discreet conversations, ‘planting seeds’, and supporting parents’ question-asking capacity: You can talk to the fellow later… You plant seeds… You learn to influence without confronting. (Participant 23, 13 years’ experience) I spend a lot of time ‘translating’ for the parents… I can’t give my opinion, but I can empower them…. (Participant 05, 4 years’ experience)
Interpretive synthesis: Moral agency was frequently enacted indirectly; participants described advocating through quiet, relational, and strategic routes when formal deliberative spaces felt inaccessible.
Theme 4: The Lingering Echo: Moral Residue and Its Professional Toll
This theme captures the enduring consequences of nurses’ constrained moral agency. Participants described moral residue as cumulative, shaping emotional well-being, professional identity, and intentions to remain in bedside NICU practice.
Carrying the weight of compromised integrity
Nurses described persistent self-reproach and perceived complicity when they could not act in accordance with their ethical judgments: You go home, and you replay it… ‘I should have said something…’ That feeling… builds up over time, case after case. (Participant 18, 10 years’ experience) It’s like a stain on your conscience… You become complicit in a system that you know is causing harm. (Participant 27, 14 years’ experience)
Emotional distancing as a survival strategy
Many described emotional distancing as protective but morally costly, creating tension between survival and professional ideals: You have to build a wall… You become a bit numb… It’s a double-edged sword. (Participant 01, 2 years’ experience) I keep my distance… it doesn’t hurt as much… But… I think it makes me a colder person. (Participant 13, 8 years’ experience)
Questioning the profession: The urge to leave the bedside
Some participants described the cumulative moral toll as contributing to burnout, cynicism, and intentions to leave bedside practice: I am actively looking for a way out… The moral toll is too high. (Participant 26, 12 years’ experience) …you watch them become jaded… I love babies, but I am starting to hate the job. (Participant 10, 7 years’ experience)
Interpretive synthesis: Moral residue appeared as an accumulative ‘afterlife’ of constrained moral agency, persisting beyond individual cases and reshaping nurses’ emotional labour, professional self-concept, and retention intentions.
Overview of thematic relationships
The four themes were interrelated and were interpreted as a cyclical process (Figure 2). Ambiguity and moral conflict in viability-related care (Theme 1) were experienced within organisational and relational constraints that limited voice and influence (Theme 2), contributing to peripheral participation and indirect forms of advocacy (Theme 3). When ethical tensions remained unresolved, participants described enduring moral residue and a professional toll (Theme 4), which, in turn, shaped how subsequent viability-related cases were approached. Cyclical process of constrained moral agency and distress among study participants in threshold-of-viability NICU care.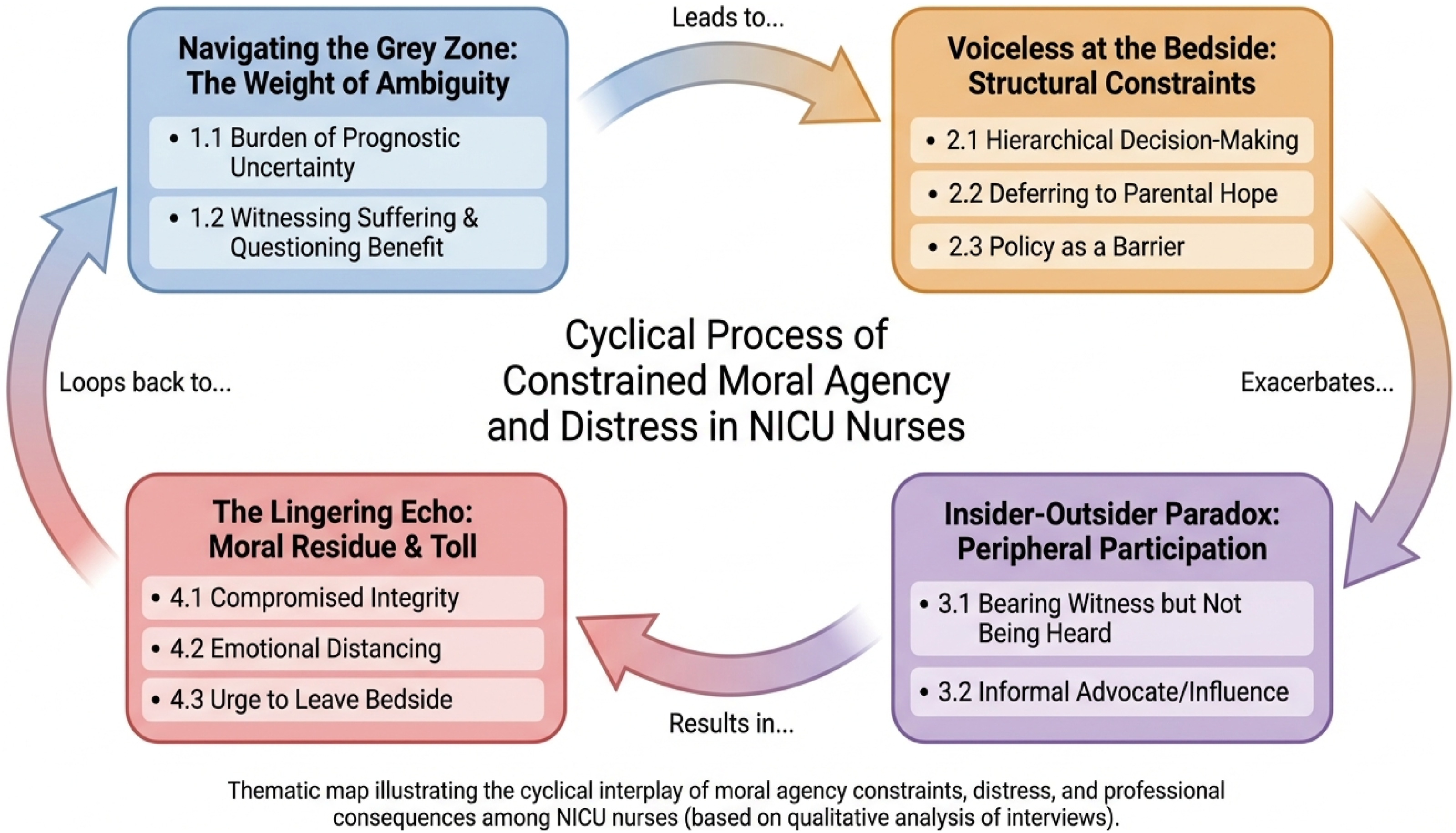
Discussion
This study explored how NICU nurses experience and enact moral agency under constraint when caring for infants at the threshold of viability. The findings suggest an interconnected process in which profound clinical ambiguity, together with structural and relational constraints, shapes nurses’ participation in ethical deliberation and is experienced as contributing to moral distress and the accumulation of moral residue. In what follows, we interpret these findings, situate them within relevant scholarship, and consider implications for nursing practice, leadership, education, and future research.
Across themes, moral distress was described as arising not only from ethically complex clinical situations, but also from constrained capacity to influence ethically consequential decisions. ‘Navigating the Grey Zone’ highlighted the felt weight of prognostic uncertainty and the moral burden of witnessing infant suffering while providing invasive interventions. ‘Voiceless at the Bedside’ foregrounded constraints that nurses faced in hierarchical decision-making, normative expectations to align with parental hope, and policy structures that were experienced as rigid or insufficiently responsive to clinical nuance. ‘The Insider–Outsider Paradox’ captured the tension of being proximal to infants and families while remaining peripheral to formal deliberation, prompting the use of indirect influence strategies. Finally, ‘The Lingering Echo’ illustrated how unresolved ethical tensions were experienced as persisting beyond individual cases, shaping emotional labour, professional self-concept, and, in some accounts, intentions to leave bedside NICU work.
These findings align with prior work that describes moral distress as intertwined with interprofessional power gradients and limited avenues for ethical voice, particularly in high-acuity settings.66–68 They also extend existing knowledge by illuminating how constraint and ambiguity operate together within threshold-of-viability care, where time-critical turning points and rapidly shifting trajectories intensify ethical pressure. The account of ‘informal advocacy’ adds nuance to the literature on nursing advocacy by illustrating how moral agency may be enacted through indirect, relational, and strategically timed practices when formal channels are perceived as inaccessible.69,70
Considering Navigating the Grey Zone specifically, the present findings align with those of Boutillier et al., who similarly identified prognostic uncertainty as a primary driver of morally distressing experiences in NICU contexts, particularly when nurses are required to enact interventions whose clinical benefit remains unclear. 22 The distinctive contribution of the present findings lies in showing how ambiguity functions not merely as clinical uncertainty but as a moral pressure amplifier intensifying distress because ethical closure is structurally unavailable within the rapidly shifting trajectories characteristic of care at the threshold of viability. 71
Regarding Voiceless at the Bedside, Alodhialah et al. similarly found that individual-level responses alone are insufficient when moral distress is institutionally produced. 72 However, while their study recommends building individual resilience within existing structures, our findings suggest that those structures themselves require reform, reducing hierarchical constraints and formalising nurses’ ethical voice, rather than adapting to them.
With respect to the Insider–Outside Paradox, the present findings align with Devireddy et al., who demonstrated that regular palliative care-neonatology collaborative conferences significantly reduced moral distress among NICU clinicians and concluded that such interdisciplinary models should be implemented more widely. 73 The informal advocacy strategies participants described in the present study, including planting seeds, translating for families, and strategically timing concerns, may be understood as compensatory responses to the absence of such formalised deliberative spaces. Importantly, our findings add nuance by suggesting that the effectiveness of any such model will depend on whether it actively solicits and meaningfully incorporates nursing perspectives, rather than, within a conference format, replicating the same hierarchical authority that currently marginalises the nursing voice at the bedside.
Finally, regarding The Lingering Echo, the present findings are consistent with Epstein and Hamric’s foundational conceptualisation of moral residue as a persistent compromise of integrity accumulating across repeated ethically distressing encounters. 39 Our findings extend this literature by illustrating how moral residue in viability-related NICU care specifically reshapes professional identity, emotional coping strategies, and intentions to leave bedside practice, adding qualitative depth to quantitative studies that have identified moral distress as a significant predictor of nurse turnover intention in intensive care settings.10,11
The Saudi Arabian setting brings important contextual specificity to the analysis. Participants’ descriptions of deferring to parental hope and of culturally inflected expectations to ‘do everything possible’ reflect how familial authority and collective orientations toward hope, shaped in part by the Islamic imperative to preserve life, configure both parental expectations and nurses’ perceived room for honest ethical communication.74,75 Additionally, policies governing resuscitation and treatment limitation operate within a specific medico-legal and institutional framework in Saudi Arabia that may shape how rigidly nurses experience protocol-based constraints. The predominantly expatriate composition of the nursing workforce in Saudi NICUs introduces further relational and identity dimensions, including cultural distance from patients and families and potentially different professional socialisation trajectories, which may modulate how hierarchy and ethical voice are experienced. Rather than treating these observations as culturally deterministic, the findings underscore the importance of attending to how family roles in decision-making, institutional norms, and workforce composition interact to configure what forms of ethical participation are possible for nurses in a given setting. 69 While key processes identified in this study, constrained agency, moral residue, and informal advocacy likely recur across high-income NICU settings, their specific contours are locally patterned, and readers in other national or regional contexts should consider these dynamics when interpreting the findings. Comparative work across contexts would further clarify which constraints reflect shared features of NICU work and which are context-specific. 76
Theoretical and Practical Implications
Theoretically, this study offers an empirically grounded account of moral agency under constraint in threshold-of-viability care. The thematic relationships illustrated in Figure 2 suggest that moral distress may be understood as part of a reinforcing process: prognostic ambiguity and ethically fraught care amplify moral tension, structural constraints narrow nurses’ perceived legitimacy to speak and influence decisions, and unresolved tensions accumulate as moral residue that shapes subsequent engagement, coping, and professional identity.
In practice, the findings indicate that exclusively individual-focused responses, such as resilience training alone, are unlikely to be sufficient when moral distress is experienced as structurally produced. Participants’ accounts point to the need for organisational strategies that formalise nursing inclusion in ethical deliberation and create protected spaces for processing ethically challenging cases. For example, the recommendation for interprofessional ethics rounds is grounded in participants’ descriptions of peripheral participation in formal deliberations, whereas the recommendation for structured post-case debriefing responds to their accounts of unresolved moral tensions that accumulate as moral residue. Potential strategies include interprofessional ethics rounds that actively solicit nursing perspectives, structured debriefing after viability-related turning points, and leadership development focused on psychologically safe communication and ethically attuned team practices. Such strategies require evaluation and local adaptation rather than assumptions of direct transferability across settings.
For health professions education, the findings suggest the need to prepare nurses, physicians, and allied health professionals not only in ethical principles but also in the practical enactment of moral agency within hierarchical clinical environments. This includes raising concerns, communicating across power gradients, participating in shared deliberation, and responding to ethical uncertainty in family-centred NICU care. Although this study was not designed to compare participants with and without prior training, most participants reported receiving no formal training in bioethics or neonatal palliative care. Those who had received such training described it as largely theoretical and insufficiently applicable to viability-specific clinical pressures. Educational interventions should therefore move beyond ethics theory alone toward interprofessional simulation and case-based learning that reflects prognostic uncertainty, family dynamics, hierarchical communication, and the relational complexity of NICU decision-making. Embedding this learning across health professions programmes, rather than only in nursing curricula, reflects the systemic and interprofessional nature of the constraints identified in this study.
Strengths and Limitations
A key strength of this study is the interpretive (hermeneutic) phenomenological design, which enabled in-depth examination of how nurses made meaning of constrained moral agency and its moral consequences. The multisite sampling across four hospitals and the use of trustworthiness strategies (audit trail, peer debriefing, reflexivity, and participant reflections) strengthen the credibility and transparency of the analysis.
Limitations should be considered. First, as a qualitative study conducted in a single region of Saudi Arabia, the findings are context-specific and not intended to be statistically generalisable. The cultural, medico-legal, and workforce-related specificities of the Saudi Arabian context, including familial decision-making norms, Islamic orientations toward life preservation, and the predominantly expatriate nursing workforce, should be considered when interpreting and transferring the findings to other settings. Second, self-selection may have favoured participation by nurses with salient experiences of moral distress, potentially shaping the range of accounts captured. Third, although confidentiality protections were emphasised, social desirability bias cannot be fully excluded. Finally, the study reports nurses’ perspectives; triangulation with physicians’ or parents’ accounts and with local policy documents could further enrich understanding of the decision ecology.
Recommendations and Future Research
Based on these findings, NICU leadership may consider piloting structured interprofessional debriefing models and formalised ethics deliberation processes that explicitly invite and operationalise nursing participation. Future research could test and refine the proposed interpretive model using mixed-methods or quantitative approaches, examine the prevalence of identified constraints in larger samples, and evaluate interventions designed to strengthen moral agency and reduce moral residue. Comparative qualitative studies across cultural and organisational contexts would further clarify which constraints reflect shared features of NICU work and which are context-specific.
Conclusion
This study illuminates how NICU nurses at the threshold of viability experienced moral distress and moral residue, which are closely linked to constrained moral agency within hierarchical, policy-bound decision-making environments. Despite sustained bedside proximity and ethically salient knowledge of infants and families, nurses described limited formal influence in ethical deliberation and reliance on indirect forms of advocacy. Over time, unresolved ethical tensions accumulated into moral residue, shaping emotional coping, professional identity, and, in some accounts, intentions to leave bedside practice. The central contribution of this work is an empirically grounded account of moral agency under constraint as an interconnected process rather than an isolated event. The findings suggest that mitigating moral distress in viability-related care requires attention to organisational conditions that enable ethical voice, structured participation in deliberation, and systematic opportunities for reflection and debriefing. Strengthening these conditions is likely to be important not only for supporting nurses’ moral integrity and workforce sustainability but also for sustaining ethically coherent care for infants and families facing the most difficult decisions.
Supplemental material
Supplemental Material - Constrained moral agency, distress, and residue in Neonatal Intensive Care Nurses
Supplemental material for Constrained moral agency, distress, and residue in Neonatal Intensive Care Nurses by Osama Mohamed Elsayed Ramadan, Alaa Hafiz, Areej Abunar, Minerva Raguini, Nadia Bassuoni Elsharkawy, Manar Fayez Alruwaili, Maha Suwailem S. Alshammari, Hassan M. Elamin, Reda Samy in Nursing Ethics
Footnotes
Acknowledgements
The authors thank all nurses who participated in this study and the hospital and academic coordinators who facilitated data collection and administrative support.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to participant privacy and confidentiality considerations. De-identified data may be available from the corresponding author on reasonable request and subject to institutional and ethical approval requirements.
Supplemental material
Supplemental material for this article is available online.