
Abstract
Background
Repeated exposure to ethically challenging situations may lead to moral injury (MI). Though MI among healthcare professionals has attracted increasing attention, studies on the process of MI are limited.
Aim
To elucidate the entire process that psychiatric nurses in Japan undergo from before experiencing MI to their subsequent recovery. Core values in psychiatric nursing, what mitigate MI, and what is important to prevent MI are discussed.
Research design
A descriptive, qualitative design was adopted.
Participants and research context
Twelve nurses were interviewed between May 2024 and February 2025. Participants were nurses who had worked in psychiatric settings and had resigned because of witnessing or conducting unethical practices. Purposive snowball sampling, semi-structured interviews, and thematic data analysis were conducted.
Ethical consideration
Ethical approval was obtained from institutional IRBs.
Results
Before starting work, the nurses had professional values in psychiatric nursing, and they expected to practice nursing based on these values. On entering the wards, they encountered various events that conflicted with their values. At first, participants doubted whether the practices they observed were appropriate, which gradually intensified and developed into persistent internal conflict. Repeated failure to improve the quality of care led to MI. Participants felt a strong responsibility, which mitigated MI and kept them working. As morally injurious events accumulated, participants developed increasingly negative feelings, ultimately leading to resignation. Their recovery after resignation involved positive and negative emotions. Eventually, they recovered sufficiently to move forward.
Conclusion
Core values in psychiatric nursing include commitment to patients and respect for their rights. One effective way to mitigate MI is to establish psychologically safe spaces in which shared experiences and values are acknowledged and validated. Moral resilience and courage are important in preventing MI. Both concepts should not be considered personal traits but rather a shared capacity in a group.
Introduction
In healthcare settings, professionals are increasingly exposed to ethically distressing situations that may profoundly challenge their moral integrity and professional identity. Among the moral suffering nurses undergo, moral injury (MI) has recently gained attention. Psychiatric nurses may be particularly vulnerable to morally injurious experiences because they frequently navigate tensions between patient autonomy, safety, institutional demands, and limited resources. Repeated exposure to ethically challenging situations within resource-constrained systems may increase their risk of MI. In this context, psychiatric care involves many ethical challenges, particularly in Japan, as the United Nations Convention on the Rights of Persons with Disabilities 1 has been repeatedly criticised.
What causes MI is violations of one’s sense of right or wrong, which are called potentially morally injurious events (PMIEs). 2 The studies on the process of MI focused mainly on examining the link between PMIEs and MI.3,4 What values did nurses embrace before they experienced MI, and what happened after they experienced MI? It is important to investigate the entire process of MI, and psychiatric nurses are suitable subject for the purpose.
Background
MI was first described as psychological suffering among war veterans. 5 Many soldiers experience injuring or killing others, failing to prevent the suffering of colleagues or civilians, and feeling betrayed by a leader or other trusted authority.6–9 Although soldiers may have to use and witness violence in dangerous circumstances, they remain members of a society in which violence is considered taboo. 9 Such moral conflict causes psychological harm: MI. Although MI was initially conceptualised in military contexts, increasing evidence suggests that healthcare professionals may experience similar moral wounds when repeatedly exposed to ethically challenging situations within constrained systems of care.
MI is severe distress and functional impairment with a wide range of biological, psychological/behavioural, social, and religious/spiritual sequelae, caused by exposure to PMIEs. 6 The outcomes of MI are reported to resemble post-traumatic stress disorder (PTSD) and other symptoms, such as depression.8,10 The degree of psychological, social, and spiritual harm and impairment is extreme compared to moral distress, although there is no cut-off point between these two concepts. 11 Wilson et al. 12 conducted a scoping review and found that MI and moral distress share overlapping, while also having distinct features. Both concepts are connected to a person’s values and encompass a moral obligation or sense of duty. Moral distress is related to organisational factors, whereas MI is related to more personal factors. Regarding symptoms or manifestations, MI does not typically involve an immediate psychological response, and presents a more progressive onset, whereas moral distress presents as an early indicator. 12
PMIEs are defined as ‘perpetrating, failing to prevent, or bearing witness to acts that transgress deeply held moral beliefs and expectations’. 2 The COVID-19 pandemic forced medical professionals into morally difficult situations, in which they had to care for large numbers of patients with insufficient medical resources. In addition to working overtime, having inadequate rest, and experiencing anxiety about becoming infected and transmitting the infection to their loved ones, they witnessed patients in life-threatening situations and were unable to help them.13–15 They were sometimes required to make difficult, or even impossible decisions, such as determining who would have the chance to survive. 13 PMIEs in clinical settings include deciding which patients would be given no chance of survival, confining infected patients and prohibiting contact with family members, and leaving patients without proper care because of nurses’ fear of infection.
PMIEs among psychiatric nurses are being identified, and include restrictions such as physical restraint4,16 and physical or verbal abuse by nurses. 4 The root causes of these problems include nurses’ lack of knowledge and professional experience, 17 nurses’ shortage, and psychiatric healthcare policies.4,18 These systemic and relational tensions repeatedly expose psychiatric nurses to experiences that challenge their moral integrity and contribute to the development of MI.
Several psychotherapeutic approaches have been proposed to address MI, including cognitive approaches, 19 Adaptive Disclosure, 2 and Acceptance and Commitment Therapy. 20 However, no standardised treatment for MI exists, and evidence regarding its effectiveness remains limited. 21 While some interventions have been developed for war veterans experiencing PTSD, 6 these interventions were primarily developed in military contexts, and may not fully address the relational, ethical, and organisational dimensions of MI experienced by nurses.
A deeper understanding of nurses’ lived experiences is needed to support those who experience MI and to promote recovery. Although associations between PMIEs and MI have been reported, little is known about how nurses experience, interpret, and recover from MI. This study aimed to explore the full process of MI among psychiatric nurses, including the values they held before suffering from MI, their experiences of MI, their coping strategies, and recovery from MI. Understanding these experiences may contribute to the development of more ethically responsive and contextually appropriate support strategies for psychiatric nurses.
Aims
This study aimed to elucidate the entire process that psychiatric nurses in Japan undergo, prior to experiencing MI and their subsequent recovery. Specifically, we focused on core values in psychiatric nursing and factors that mitigate MI. Additionally, the importance of MI prevention is discussed.
Methods
Study design
This study was part of a broader research project examining MI among psychiatric nurses. In a previous qualitative descriptive study 4 , we reported findings on the experiences and perceived causes of MI among psychiatric nurses in Japan who had resigned from their positions due to moral or ethical distress. Although the same participant dataset was used, the present analysis differs substantially from the previous publication in focus, analytical scope, and contribution. The previous study focused specifically on two core categories: (1) the causes of MI and (2) the experiences of MI among psychiatric nurses, with the aim of exploring how psychiatric nurses experience MI and identifying the factors contributing to those experiences in psychiatric settings. In contrast, the present study examines the broader trajectory and recovery process associated with MI. Specifically, this analysis aims to understand the entire process from the period before experiencing MI to recovery and adaptation. It focuses on core values in psychiatric nursing and on the factors that mitigate MI and support recovery.
Participants and recruitment
Purposive and snowball sampling methods were used for recruitment. The inclusion criteria were as follows: nurses, regardless of age, gender, current employment status, or place of work, who had worked in psychiatric hospital settings, suffered from moral or ethical issues, and had resigned. To recruit participants, flyers were distributed at mental health nursing conferences and lecture meetings.
The study included 12 nurses (A–L) residing in six prefectures. The group comprised seven women and five men, spanning a wide range of ages, from their twenties to their sixties: three participants were in their twenties, one in their thirties, four in their forties, two in their fifties, and two in their sixties. Their clinical nursing experience varied considerably, ranging from 1.2 to 32.2 years (mean = 15.5 years). The time elapsed between resignation and participation in the interview also differed substantially, from 0.8 to 24.3 years (mean = 6.0 years).
At the time of the interviews, four participants were working in community settings (as visiting nurses), two were university faculty members, one was a school nurse, one was a public health nurse, and one was unemployed. Only three were working in other psychiatric hospitals.
Data collection
Data were collected between May 2024 and February 2025. Participants were interviewed face-to-face in a private setting of their choosing, such as university facilities or other neutral locations, to ensure confidentiality. The mean interview duration was 58.9 min (range: 45-81 min). Semi-structured interviews were conducted using the following questions: (1) Work experience: ‘Why did you want to work in a psychiatric hospital?’ ‘What was important to you when practicing nursing?’ ‘What events or situations were morally injurious to you or what made you distressed?’ and ‘How did you feel and react to them?’ (2) Resignation history: ‘What made you decide to quit?’ ‘Why was it so critical for your decision?’ ‘Were you able to keep practicing what you thought was important in nursing?’ and ‘What made you give up working at the hospital?’ (3) Support: ‘What supported you during and after working?’
Ethical considerations
Ethical approval was obtained from the research ethics committees of the universities to which the researchers belonged before the research was conducted. Participants were interviewed in rooms where privacy could be maintained, as the topic was sensitive. All participants provided written informed consent. They were informed that they could withdraw from the interview at any time, and were not required to discuss topics they felt uncomfortable discussing.
Data analysis
An inductive thematic analysis approach was adopted to analyse the data. Interviews were recorded and transcribed verbatim. The research team repeatedly reviewed the data and divided them into codes. Each code represented a single distinct meaning and constituted a self-contained piece of information. When two codes had similar meanings, they were grouped together; when they differed, they were placed in separate groups. When a third code had a similar meaning to an existing group, it was added to that group. The fourth code was then analysed. The inductively generated groups were categorised into subcategories. Each subcategory was named to reflect the meaning shared by the codes that comprised it. Similarly, the subcategories were integrated into categories, which were then classified into core categories. Each was named considering the research aims at a higher level of abstraction. 22
All narratives were divided into codes and analysed without selection to ensure credibility. The research team comprising mental health nurses with expertise in mental health and nursing ethics discussed the categorisation until consensus was reached to enhance the validity of the study.
Among the six core categories obtained in this study, details of two core categories relating to causes of MI and experiences of MI have been previously published 4 . Without these two core categories, the entire process could not have been fully captured. Only unpublished narratives were used in this study.
Results
The process from before experiencing moral injury to subsequent recovery.
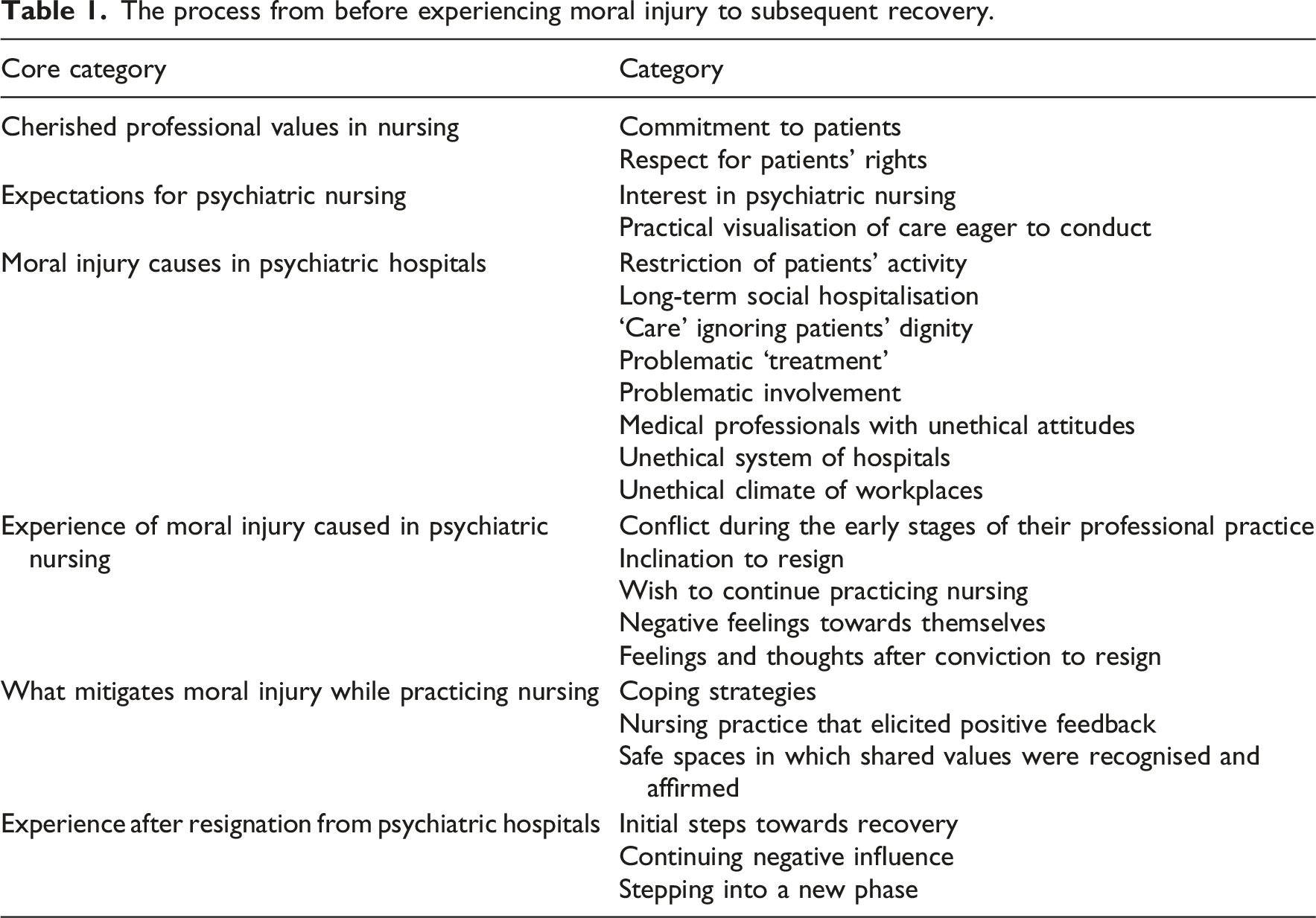
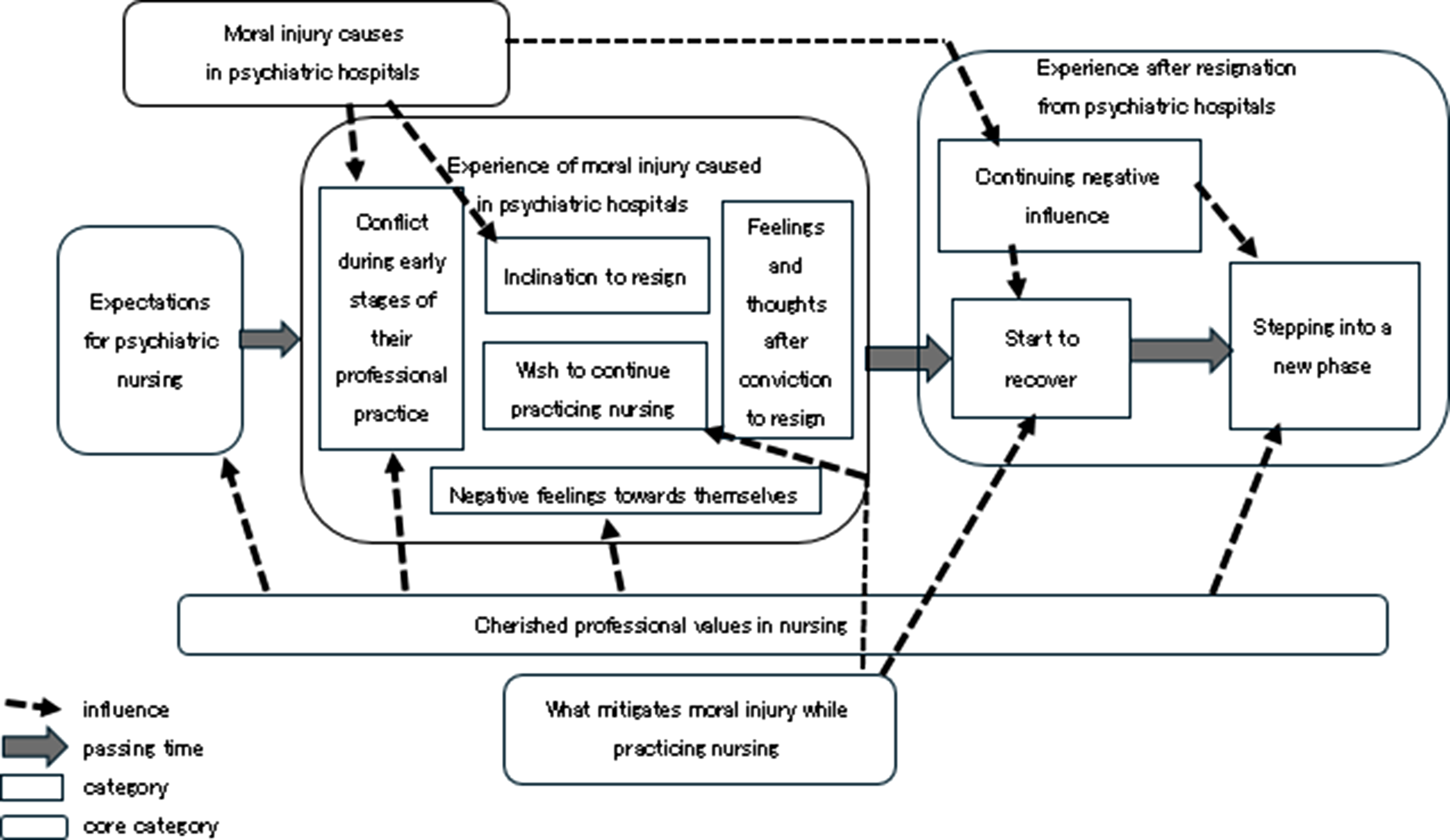
The process of moral injury among psychiatric nurses.
Before working
Before starting to work in psychiatric hospitals, participating nurses possessed professional values in psychiatric nursing that they cherished (cherished professional values in nursing). One value was commitment to patients, which comprised thoughtful and careful support for daily living activities, respect for patients as persons, standing by patients, and activities with patients. ‘It is not special, but I’d like to do for patients what I would want done for my family members when they are in hospitals’. (E) ‘I hate prejudice, and would like patients to live as they are without feeling prejudice against them’. (L) ‘I think the most important thing in nursing is to spend time with patients, not to write nursing reports nor prepare a drip infusion away from patients’. (J)
The other value was respect for patients’ rights, encompassing advocacy for patients’ rights, respect for patients’ autonomy and self-management, and support for transitions to more appropriate care settings, such as community-based environments. ‘I want patients to keep their money with them and spend it as they want’. (B) ‘Patients should not be forced to stay in hospital as a source of income for hospitals. They need to be moved into their communities’. (A)
Grounded in these personal and professional values, participants held clear expectations of psychiatric nursing before entering practice. Their interest in psychiatric nursing was reflected in their choice of psychiatric care settings aligned with these values and was further shaped by the influence of professional role models. They also articulated concrete visions of the care they aspired to provide (practical visualisation of care eager to conduct), including a strong commitment to patients, the use of therapeutic approaches, and efforts to enhance the protection of patients’ rights. ‘As I would like to take time to commit to patients, I thought of becoming a psychiatric nurse’. (F) ‘The psychiatric nurse who trained us (students) was so nice that I aspired to become such a nurse’. (I) ‘I wanted to stay with patients, and listen to them rather than perform advanced medical procedures’. (C)
While working: Experiencing MI in psychiatric nursing
Expecting to practice nursing based on these values, nurses began working in psychiatric hospitals. Upon entering the wards, they encountered various events that conflicted with their values, causing MI (moral injury causes in psychiatric hospitals). These events included restriction of patients’ activity, such as physical restraints, long-term social hospitalisation, medical professionals with unethical attitudes, and problematic ‘treatment’. A nurse (E) was surprised by a psychiatrist who ordered the restraint of all patients upon admission. Some patients had remained in hospital for 20 or 30 years, and neither they nor the nurses understood the purpose of their treatment (G). The behaviours of other nurses and healthcare professionals were also inappropriate. A nurse (J) witnessed a psychiatrist slap away a patient’s hand, and walk off when the patient requested discharge.
At first, participants began to question whether the ‘treatment’ and ‘care’ they observed were appropriate. Gradually, these doubts intensified, leading to persistent internal conflict during the early stages of their professional practice. Despite repeated efforts to improve the quality of care, their attempts were largely unsuccessful, leading to significant distress and MI. Participants described strong negative emotions, such as disgust, anger, and disdain, which caused an inclination to resign. A nurse (C) was disgusted by seeing other professionals displaying their superiority, while showing no intention of standing by patients. Another nurse (E) was angry when a patient was denied discharge because of family opposition, even though he was not a criminal. They also felt isolated, as one nurse (G) lamented that no one else in the ward shared his perspective.
At the same time, the participants expressed a strong wish to continue practicing nursing motivated by empathy for patients, a sense of professional responsibility, the value they placed on their roles, and a reluctance to abandon patients in need. One nurse (F) felt a profound sense of responsibility when he realised that he was entrusted with patients’ lives. Another nurse (J) wondered what would happen to the patients if she quit. She could not quit because she believed that the patients might be beaten by nurses and left without care.
Despite experiencing MI, the participants’ strong sense of responsibility kept them working. Some participants described being supported by factors that helped mitigate its impact (what mitigates moral injury). These mitigating influences comprised three interrelated categories: (1) coping strategies, including stress relief, setting distressing issues aside, and making compromises; (2) aspects of nursing practice that elicited positive feedback, such as receiving affection and trust from patients and engaging in efforts to improve care; and (3) access to psychologically safe spaces in which shared values were recognised and affirmed, such as teachers from whom they had been taught psychiatric nursing and directors of nursing in other hospitals. ‘I put to one side what I was unable to change, such as the hospital’s structures’. (F) ‘I convinced myself that these events might be ordinary and not wrong, to ease myself’. (H) ‘I untied patients who were restrained and lowered their beds so that they would not be hurt if they fell out of their beds’. (E) ‘Some patients asked me when I would come next. They looked forward to seeing me’. (J) ‘I sometimes visited a teacher who had taught me mental health nursing, and told her that I thought what was happening in my hospital was inappropriate’. (I)
As morally injurious events accumulated, participants developed increasingly negative feelings towards themselves and ultimately decided to resign from their positions. Following this decision, they described a shift in their emotions and thinking (feelings and thoughts after conviction to resign), characterised by a renewed commitment to practicing nursing in accordance with their professional values and a reduced concern about colleagues’ reactions. One nurse (C) said that she had explained medication to patients after her decision to quit, although the hospital’s policy had prevented patients from being informed.
This turning point led participants to develop a growing interest in studying ethical and humane approaches to mental health nursing as well as in pursuing community-based mental health nursing practices. One nurse (J) stated that she wanted to learn empathy or attentive listening, which she considered essential for psychiatric nursing, as nursing in her hospital had been nothing like that.
Aftermath and process towards recovery
Participants’ initial steps towards recovery after resigning from psychiatric hospitals involved both positive and negative emotions. Although they felt relieved at first, they gradually came to realise that they had participated in nursing practices that they later viewed as inappropriate. They found themselves to be perpetrators as well as victims. Having gained a broader perspective, they became aware that they had not sensed wrongdoing and had become numb. ‘I was really relieved when I quit’. (H) ‘The psychiatric hospital I worked at was a strange place. We, nurses, like the patients, were also disconnected. Once we entered the ward, we did not go outside, and were unaware of the outer world or other principles. We did not feel that anything was odd’. (G) ‘I think we, nurses, were subject to pressure, or harassment, from above, which influenced our authoritative attitudes towards patients’. (D) ‘The patients in the psychiatric hospital where I am working now are different. I was surprised to find out that they are allowed to carry their money with them, to go out, to drink juice freely, and to be discharged! I hadn’t experienced any of these in the previous hospital’. (J)
Even though they had resigned, they struggled with a continuing negative influence. They felt responsible for and guilty about the patients they had abandoned. They were exhausted, and experienced apathy, regret, and feelings of self-condemnation. Some suffered flashbacks. They were disenchanted with the Japanese psychiatric system. ‘I still remember patients waving, and seeing me off when I quit. I left them in such bad conditions’. (J) ‘Even now, I can still feel the sensation in my hands when I pushed patients into the seclusion room and shut the door in front of them. It was painful’. (G) ‘Nurses care for patients with, for example, cardiovascular disease based on established knowledge of the circulatory system. In contrast, psychiatric nursing does not rely on the same type of organ-based knowledge. In Japan, psychiatric nurses often practice based primarily on their own experience’. (K)
Eventually, they recovered sufficiently and moved forward (stepping into a new phase). Some decided to address the organisational climate in other hospitals to eliminate patient abuse, some began working in community mental health settings, and some became university faculty members to educate nurses to practice ethical nursing. In this new phase, they experienced a sense of release and reward in their current jobs while also developing a heightened awareness of the importance of the government’s responsibility. ‘I hated that patients in restraints were neglected. Now I often intervene to release patients from restraints’. (C) ‘Now [in community mental health nursing] I don’t have to obtain agreement from the nursing team, nor report to the head nurse. It is great that I can do whatever I think is good for clients’. (B) ‘I think the government is an accomplice [in patients’ rights violations]. As the government is working to force people with mental diseases to be admitted, it has a duty to make efforts to discharge them [back into their communities]’. (G)
Discussion
Participating nurses began working in psychiatric hospitals with the intention of practicing nursing based on their professional values. Once they had entered psychiatric wards, they encountered various unethical, or morally questionable events, and sometimes had to carry out actions they considered inappropriate such as restraints, which caused MI. Although they had a desire to quit their jobs, their sense of responsibility and positive feedback from patients kept them working. Coping strategies and psychologically safe spaces mitigated their psychological distress. The accumulation of PMIEs led them to resign, but the process towards recovery was not easy. They experienced continuing negative influences before moving forward to new phases.
The values deeply embedded in psychiatric nurses’ minds can be inferred not only from their explicitly expressed professional values and expectations but also from what was compromised or undermined. The nurses in this study imagined nursing as thoughtful and careful support for patients’ daily activities and engagement, and wanted to ‘stand by patients’ or ‘listen to patients’. Some participants were sensitive to patients’ rights and eager to protect them. As Heitzmann et al. 17 emphasised, values such as respect, honesty, justice, and empathy towards both patients and staff are integral to professional commitment. Nurses are eager to commit to patients in accordance with these values. In their wards, however, patients were miserable: abused, disrespected, and neglected, which undermined their core values and integrity, and caused MI.
The factors that mitigate MI were identified in this study. Among them, nursing practice that elicited positive feedback is a characteristic of nursing. In psychiatric nursing, seeing a patient as unique and as a whole person is the basis for moral commitment. 23 Positive feedback from patients is evidence that nurses can build trusting relationships with patients, that nurses’ commitment is appropriate, and that it encourages nurses to continue practicing in this way.
Personal coping strategies, such as dissipating stress, did not solve the problems they faced, although they can reduce stress. Additionally, in safe spaces in which shared values were recognised and affirmed, nurses can make sense of their feelings and gain insights into how to address their problems. Such spaces should be fostered not only within hospitals where nurses practice but also beyond institutional boundaries. Creating opportunities for nurses from different hospitals to share moral challenges openly and be heard with empathy may help reduce their moral burden.
Moral resilience is the capacity to sustain or restore moral integrity in the face of moral distress, ethical conflicts, and structural constraints inherent in contemporary clinical practice.24,25 Moral resilience is not reduced to passive endurance; rather, it encompasses reflective, relational, and deliberative processes that enable professionals to remain faithful to their core moral values, even under conditions of pressure. The participants’ narratives suggested that one of the main difficulties in resisting and confronting unethical practices was their profound sense of isolation and loneliness. Psychologically safe spaces can provide nurses with companionship and a feeling of support, which strengthens their moral resilience.
In the absence of ethical work environments, supportive leadership, and opportunities for ethics education, nurses may be morally aware, yet unable to act. As Lachman 26 noted, although acting with moral courage often entails personal sacrifice, it is frequently accompanied by a sense of inner peace derived from upholding non-negotiable principles. The lack of moral action observed in clinical contexts in this study should not be interpreted as indifference or moral deficiency but rather as a result of the simultaneous erosion of moral resilience.
Furthermore, this study reflects on the psychiatric nurses’ experience of practice as a temporary career path, showing that many were initially motivated by their ethical values when they started working, and that these values were undermined over time by witnessing and sometimes participating in unethical practices. Thus, strengthening moral resilience, particularly in its collective dimension, is a prerequisite for enabling moral courage and sustaining ethical actions in psychiatric nursing practice.
Before the nurses recovered, they needed to reflect on their own nursing practice, including what they did for patients, what they failed to do for patients, and instances of misconduct that they did not recognise at the time. Becoming aware of their own behaviours may have led to regret, feelings of guilt, or depression. By experiencing and working through these negative emotions, they developed a renewed commitment to practice nursing in accordance with their values.
Hope for the future is essential for recovery from MI. Most nurses found hope in community mental health nursing or psychiatric nursing education, although a few were so disappointed with psychiatric nursing that they found jobs outside psychiatry, maintained their interest in mental health and psychiatric nursing and were able to move forward. In any case, it is important for nurses who have experienced MI to extend their perspectives on psychiatric nursing.
Limitations
This study had several limitations. The most serious limitation was that all participants were nurses who had recovered and were willing to talk. It is unclear whether nurses who have not recovered continue to suffer, sometimes from depression or other mental health problems, and are unable to talk about their experiences. Further research is needed to explore the experiences of these nurses. Second, as participants were recruited using snowball sampling and data saturation was not reached, there may be other unreported categories, which also requires future research. Nevertheless, a wide variety of participants may be helpful in revealing diverse experiences. Additionally, participants’ narratives were based on memory, which may be biased. The time that elapsed between resignation and interviews varied. In the case of a nurse who had resigned 24.3 years before the interview, his memory is likely to be biased.
As more experienced nurses can easily cope with ethical issues, and recover sooner, the process towards recovery from MI differs depending on the nurse. However, the heterogeneity of participants may have enriched the transferability of this research. This study sheds light on the process of recovery from MI, and supports strategies for its mitigation, as little is known about this process.
Conclusions
This study examined the entire MI process among psychiatric nurses. Psychiatric nurses possess professional values and anticipate nursing practices based on them before they work. When nurses start work, they witness or are sometimes forced to engage in unethical conduct that conflicts with their values and causes MI. They experience negative emotions and thoughts towards other professionals and themselves, as well as a sense of isolation and begin to question whether to resign. However, positive feedback from patients, psychologically safe spaces where they feel empathised, and their sense of professional responsibility reduced the likelihood of resignation. With the accumulation of morally injurious events, nurses eventually decide to quit and pursue practical care based on their values. Even after resignation, they struggle with the continued negative influence of their experiences. Eventually, they are able to move forward into new phases such as community mental health practice or university education.
The core values of psychiatric nursing are commitment to patients and respect for their rights. These values include thoughtful and careful support for patient activities, standing by patients, respect for autonomy, and support for transitions to more appropriate care settings, and as well as avoiding unnecessarily prolonged hospitalisation.
The nurses in this study were sensitive to ethical issues, and tried to practice ethical care, but were unable to do so. They were isolated from an unethical workplace climate and hierarchical power dynamics, and their moral resilience was weakened.
The results of this study suggest effective ways to mitigate MI, one of which is to establish psychologically safe spaces in which shared experiences and values are acknowledged and validated. These spaces should exist not only in hospitals to which the nurses belong but also outside hospital settings. Further research will include holding meetings in which psychiatric nurses with MI discuss their experiences and coping strategies, and exploring the effects of these meetings.
Footnotes
Acknowledgements
The authors would like to thank all the participants for their contribution to this study.
Author contributions
K.O. and S.T. designed the study and performed data collection. K.O., S.T., M.A., and K.K. analysed the data. J.D. supervised the interpretation of the data and revised the whole manuscript. All the authors contributed to writing the manuscript.
Funding
This research was supported by a Grant-in-Aid for Scientific Research JSPS KAKENHI (Grant Number JP24K13628).
Declaration of conflicting interests
Data Availability Statement
Subject to ethical and legal considerations, the data supporting the findings of this study are available upon reasonable request.