
Abstract
Background
Integrity is a foundational value in nursing, essential for ethical practice, professional accountability, and maintaining patient trust. Growing evidence of dishonest behaviors in academic and clinical settings highlights the complexity of practice, where boundaries between honesty and dishonesty are not always clear-cut. Despite this, limited research has explored how senior nursing leaders conceptualize integrity and dishonesty across the academic-clinical continuum.
Aim
This study aimed to explore senior nursing leaders’ perceptions of integrity and dishonesty, the underlying factors contributing to unethical behaviors, and potential strategies for addressing these challenges in educational and clinical contexts.
Design
A qualitative study was conducted. Data was collected through semi-structured, in-depth interviews and analyzed using thematic analysis to identify patterns and themes.
Participants
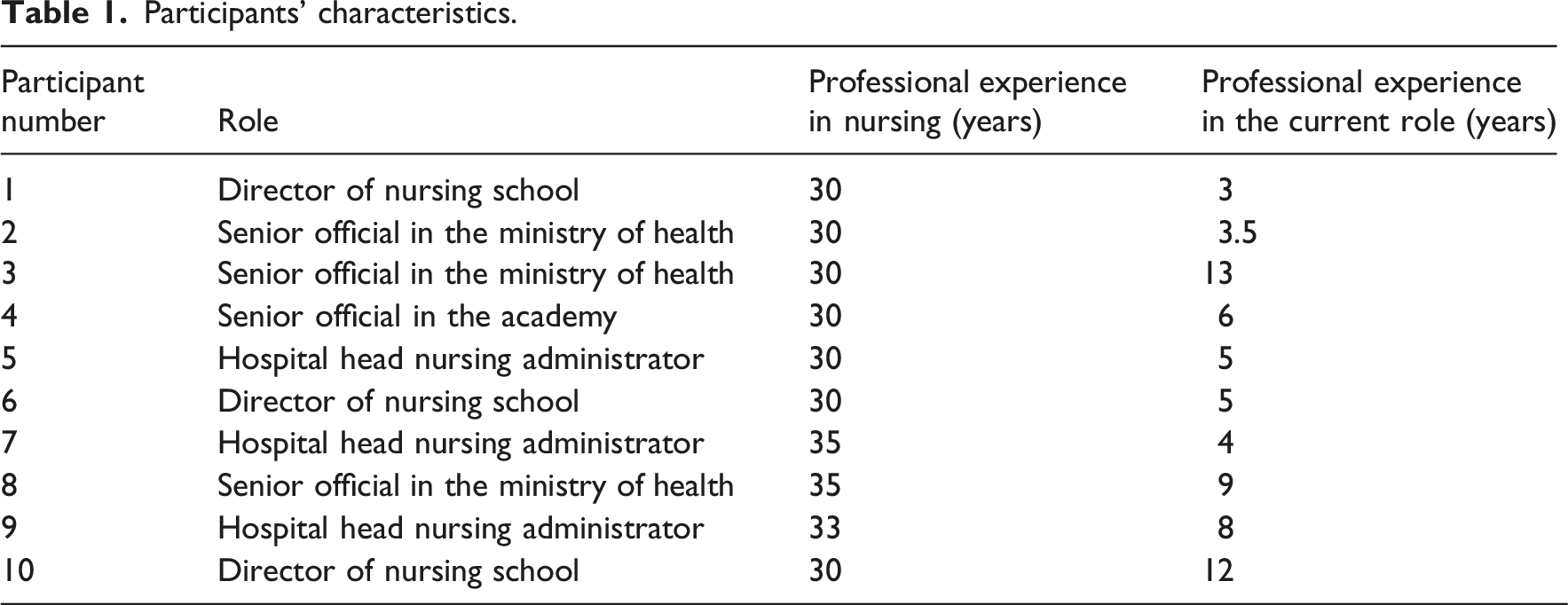
The study included ten senior nursing leaders from academia, hospitals, and the Ministry of Health. All participants held managerial roles and had experience in nursing education or training, allowing for perspectives across the educational-clinical continuum.
Ethical considerations
Ethical approval was obtained from the institutional review board. Informed consent was secured from all participants, and principles of confidentiality, anonymity, and voluntary participation were strictly maintained.
Findings
Three themes emerged: (1) integrity and dishonesty were perceived as existing along a continuum rather than as dichotomous constructs, with patient safety serving as a key moral boundary; (2) dishonest behaviors were shaped by a combination of individual, cultural, and systemic factors, including organizational pressures and inconsistent enforcement; and (3) leadership practices, particularly education, role modeling, and case-by-case management, were viewed as central to promoting integrity.
Conclusions
Integrity in nursing is not solely an individual attribute but is co-constructed within organizational and educational systems. Promoting ethical practice therefore requires integrated approaches that combine education, supportive organizational cultures, and clear policies, while acknowledging the complexity and ambiguity inherent in real-world clinical practice.
Introduction
Integrity is widely recognized as a foundational value in nursing, 1 underpinning professional responsibility, ethical decision-making, and the trust placed in nurses by patients and society. 2 Professional integrity encompasses honesty, accountability, transparency, and adherence to ethical standards in both academic 3 and clinical practice. 4 These principles are central to safe and ethical patient care and are reinforced through professional codes of conduct, nursing education, and regulatory frameworks.
Professional integrity is distinct from personal integrity, which reflects an individual’s broader moral values and consistency in everyday life beyond professional roles. 5 While personal and professional integrity are related and may influence one another, they are not identical: professional integrity is shaped by contextual demands, organizational structures, and professional codes of practice, whereas personal integrity is more stable and general across life domains.5,6 Therefore, recognizing the distinction and overlap between personal and professional integrity is essential for understanding ethical behavior within nursing practice.
Background
Despite the centrality of integrity to nursing practice, dishonest behaviors in both academic and clinical settings have been increasingly documented. Academic dishonesty among nursing students has been widely reported in the literature. 7 Such behaviors raise significant concerns because patterns of dishonesty established during education may persist in professional practice. 8 Indeed, previous research suggests that unethical academic conduct may be associated with dishonest or unsafe behaviors in clinical settings later in nurses’ careers. 9
In clinical practice, dishonesty may manifest in various forms and is often addressed within regulatory or disciplinary frameworks. 10 However, such behaviors also arise within complex organizational and interpersonal contexts of nursing practice. 11 Nurses frequently operate in environments characterized by heavy workloads, hierarchical structures, and competing professional demands, 12 which may influence ethical decision-making and the ways in which honesty and transparency are enacted in practice. 11
Importantly, ethical conduct in healthcare is not determined solely by individual moral character but is also shaped by organizational culture, leadership practices, and professional socialization processes. 13 Senior nursing leaders play a particularly significant role in shaping these ethical environments. Through their leadership, policies, and role modeling, they influence how integrity is interpreted, taught, and enacted across both educational and clinical systems.14–16 At the same time, leaders must often navigate tensions between ethical ideals and the practical realities of complex healthcare systems.
While previous studies have examined academic dishonesty among nursing students 7 and ethical challenges faced by practicing nurses, 17 far less attention has been given to how senior nursing leaders conceptualize integrity and dishonesty across the educational-clinical continuum. Understanding these perspectives is important because senior nursing leaders are responsible not only for enforcing ethical standards but also for shaping professional culture in which those standards are interpreted and applied. 18
Dishonesty is particularly concerned in nursing education because professional identity formation begins during training, and patterns of ethical reasoning established in academic settings may later shape clinical decision-making. Therefore, the aim of this study was to explore perceptions of integrity and dishonesty in nursing education and professional practice from the perspectives of senior nursing leaders working in academia, hospitals, and the Ministry of Health. By examining how these leaders interpret dishonest behavior, its underlying causes, and possible strategies for addressing it, this study seeks to contribute to a deeper understanding of ethical challenges in nursing and the role of leadership in fostering professional integrity.
Methods
Study design
This qualitative interview study explored perceptions of integrity and dishonesty in nursing education and professional practice from the perspectives of senior nursing leaders. The study was guided by an interpretive phenomenological approach aimed at understanding the essence of participants’ lived experiences and the meanings they assign to ethical behavior in nursing. This approach sought to capture participants’ experiences and interpretations, while promoting open reflection and deeper emotional insight. 19 Semi-structured, in-depth interviews enabled participants to reflect openly on complex ethical situations and professional dilemmas, facilitating exploration of the meanings they attribute to integrity and dishonest behavior. The objective was to reveal the underlying meanings and common essences emerging from participants’ subjective interpretations of their experiences. 20 The interviews were conducted by trained qualitative researchers, both women (one with a PhD working in the nursing education system and the other with a PhDc working in the Ministry of Health), who have experience in nursing education and leadership. Within this interpretive phenomenological orientation, thematic analysis was employed as a method for identifying patterns of meaning that reflect the essence of participants’ lived experiences rather than merely descriptive categories.
Study setting and recruitment
Participants were recruited using purposive sampling complemented by snowball sampling, to identify individuals with extensive experience in senior nursing leadership roles. Recruitment continued until thematic saturation was reached. Participants were recruited from three domains: senior academic leadership in nursing education (e.g., deans, heads of nursing campuses); senior clinical management (e.g., hospital nursing directors); and national-level policy and regulatory positions within the Ministry of Health. Participants were eligible if they had at least two years of experience in their current role and have previous experience in nursing education.
Interviews began with broad open-ended questions such as “How do you define integrity in nursing?” and “What types of dishonest behaviors have you encountered in academic or clinical contexts?” Follow-up questions were used to clarify and deepen participants’ responses to meanings of honesty and dishonesty; personal and observed experiences of academic and clinical dishonesty; perceived motivations and contextual factors; implications for patient care and professional identity; and recommendations for education and practice.
Data collection and analysis
All interviews were audio-recorded with participants’ consent and transcribed verbatim. Each interview lasted approximately 1 hour, and no written notes were taken during the interviews. Data was analyzed using thematic analysis following the approach described by Vaismoradi et al. (2013). 21 Thematic analysis in this study was conducted within a phenomenological interpretive framework, where codes and themes were developed to capture the essence and meaning of participants’ lived experiences rather than to merely categorize content. The analysis involved repeated reading of the transcripts, coding of meaningful units, grouping codes into categories, and identifying overarching themes. These themes were interpreted as representations of shared experiential meanings across participants, reflecting the essence of how integrity and dishonesty are understood in nursing practice.
Rigor
To enhance trustworthiness, two researchers [xx and yy] independently coded the transcripts and collaboratively developed themes. Differences in interpretation were discussed until consensus was reached. Reflexivity was maintained throughout the research process through continuous reflection on potential assumptions and biases. This reflexive process supported the phenomenological aim of remaining grounded in participants’ lived experiences while acknowledging researcher interpretation.
Ethical considerations
The study received ethical approval from the Helsinki Committee of the Shamir Medical Center (approval number: ASF-0281-22). Informed consent was obtained from all participants prior to the interviews.
The study adhered to ethical principles of autonomy, confidentiality, and non-maleficence. Participation was voluntary, and participants could withdraw at any time without consequence. To minimize potential fear of repercussions, interviews were conducted in private settings, names were not recorded, and no identifying information was included in transcripts. Data was accessible only to researchers and was used solely for research purposes.
Results
Participants’ characteristics.
Perceptions of integrity and dishonesty
The first theme presented leaders’ views of integrity and dishonesty, seen not as dichotomous but as a continuum shaped by context, severity, and consequences. Participants also described a hierarchical understanding of dishonest behavior, distinguishing between minor deviations and more severe actions. Notably, patient safety emerged as the primary moral threshold distinguishing tolerable deviations from unacceptable dishonest behaviors.
Most interviewees emphasized that integrity and dishonesty are not absolute constructs. Rather than conceptualizing these notions as dichotomous, they described them as existing along a continuum between integrity and dishonesty. In this view, both nursing students and professionals may be positioned at different points along the continuum. Accordingly, interviewee 6 (a director of a school of nursing with five years of experience in the role) stated: “Is it dichotomous [integrity and dishonesty]? No. There may be a place on a continuum. I think there are people who are more honest.” Similarly, interviewee 3, who has held a senior position in the Ministry of Health for 13 years, noted that “all of us,” from students to senior leaders within the system, occupy a place along this continuum: “You can sometimes look critically and see that actions are being carried out that are not entirely acceptable, and those performing them are the most senior people in the system.”
While interviewees agreed that integrity is a core professional value, they recognized that relational complexities can sometimes challenge absolute transparency. Interviewee 1 (the director of a school of nursing) explained: “I think that all of us… face situations where I cannot say that 100% of the time we only: ‘let’s say, you know, absolute things’. And what is truth? You know, it’s, like, relative, it’s not absolute. It is relative.”
Moreover, the interviewees noted that when considering the concept of dishonesty, they perceive it along a hierarchy based on context and the severity of dishonest behavior. In other words, they considered academic or administrative dishonesty to be “lighter” cases compared to clinical dishonesty, especially when patient harm might result. Interviewee 8 described where, in her view, the line is drawn between minor and serious cases: “This is the line I distinguish: as long as the behavior does not cause psychological or physical harm to the patient or the caregiver, on the contrary, it is an opportunity for improvement and investment, something to work on. But if the behavior endangers patients or even the caregiver, then we cannot overlook it.” Interviewee 6 added: “One can speak about [dishonest] behaviors that are more severe and those that are less severe.”
To emphasize the hierarchy of dishonesty, interviewees described minor cases with softened language (”cutting corners” and “deviating from rules”) rather than labeling them as outright fraud. Interviewee 5, a head nursing manager at one of the country’s largest hospitals for five years, described her view of minor dishonesty as “We had rules that we occasionally deviated from. I know that every rule has exceptions. But this is not at the level of dishonesty… I would say it is bending the rules.”
Reasons for dishonest behavior
In the discussion of factors leading to dishonesty, the interviewees identified several reasons, including cultural and social influences; individual and behavioral factors; academic and environmental pressures; and systemic and institutional constraints.
Cultural and social influences
Accordingly, the interviewees attributed cultural gaps to differing values and varying interpretations of what is permissible versus prohibited. As noted by Interviewee 2, who has 30 years of professional experience, including 3.5 years in a senior position at the Ministry of Health: “The range [of cultural gaps] is much broader, and the boundaries are extremely unclear. And sometimes students do not understand when they have crossed the line, when it is unacceptable… because it is not clear.” Interviewee 5 added: “I think we are a society in which… integrity is not what guides our society.”
Following the discussion of cultural gaps, most interviewees agreed that values instilled at home and family during childhood influence individuals’ conduct later as students and as professionals. Interviewee 3 explained this by stating: “I identify it [values of integrity] from the place the student comes from… there are people who do not see cheating or lying or committing [such acts] as a very serious wrongdoing. On the contrary… and there are those who are educated that under no circumstances is it allowed to cheat. It is a life rule. And there are those who do not see it as a major wrongdoing and can even live with it very well, and even look at it differently, not as cheating, but as special skills that I have, through which I succeeded or achieved some good points… I say that the main problem is… values from home.”
Individual and behavioral factors
Previous successful experiences with dishonest behaviors were emphasized as one of the central reasons for engaging in dishonest behavior later. The interviewees noted that students are exposed to academic dishonesty already during their school years, and when such behavior is successful, or when schools refrain from imposing serious sanctions or any sanctions at all, this experience provides students with confidence to engage in dishonesty both in their academic studies and later in their professional lives. Interviewee 10 (director of school of nursing) shared a story about a student who engaged in dishonest behavior several times without being sanctioned, explaining that “many times in conversations with him he said, ‘Listen, this was acceptable in my school, and there was no problem with it. Now that you told me it is forbidden, I will not do it again.’” She further described the effect of an unaddressed case of dishonesty, stating, “he [the student] already tried the ‘criminality’ [academic dishonesty]. He saw that you do not die from it. His ease in doing things that are against the law and against society - it becomes easier. The finger on the trigger is lighter. And therefore, it is easy for him to be dishonest in any situation and in any context….”
Academic and environmental pressures
Another reason raised by the interviewees was students’ perception of dishonesty as an immediate solution to challenging academic tasks or as a means of success in a competitive environment. Interviewee 7 (head of the school of nursing for 4 years) described this perception, stating that “from my experience, what motivates it [dishonest behavior]? It is easier, it requires less investment… it can be cultural or competitive, and then he [the student] chooses the easier path.” Dishonesty aimed at achieving success was also described as emerging when junior professionals are exposed to senior professionals who behaved dishonestly and nevertheless advanced within the system, with such examples serving as justification for dishonest behavior in their own professional careers. As interviewee 7 explained, “because he [the professional] says, ‘if he [the senior position holder] is like that [dishonest] and reached the senior position, why should I change my behavior?’” Interviewee 8 added on the same issue: “it is simply very bad [the dishonest behavior], in my opinion, and it can serve as a completely wrong example. Sometimes things are known, even to students, and then they identify people who are seniors in the system and were not very honest and still succeeded. And then unfortunately, they [students] sometimes start taking this as an example.”
Systemic and institutional constraints
One of the most actively discussed reasons among all interviewees concerned the way the system responds when dishonesty is identified. The interviewees noted that both the academic and clinical systems tend to be lenient and often do not allow for the implementation of punitive measures. As a result, even when there is a strong suspicion of dishonesty but no solid evidence, management may choose to ignore the issue altogether. Interviewee 5, a nursing administrator in a hospital, described this shift by stating that “I think that in the past people would be removed from frameworks and would not continue their studies if they were caught this way [for dishonesty]. Today there is leniency. Today there is very great leniency toward these processes…it is very difficult in the end to terminate their [professionals’] employment on such a basis… and there is always tendency to give another chance and leniency.” Similarly, interviewee 10, who works as a director of nursing school, added: “Let’s be honest… wherever a student can cut corners and the system allows him to cut corners - it [dishonest behavior] happens. If the regulations do not explicitly specify punishments, the student will do things where he can bend the rules a little and later say: ‘It is not written in the regulations.’” Interviewee 2, who has been working in a senior position at the Ministry of Health for 3.5 years, also referred to the leniency of the system, explaining: “Now I am speaking from my position in a senior role. It depends on what enforcement tools I have, how much power I have to enforce. Many times, I think five times whether I enter a case, because if I enter the case and I have nothing to do with it and no way to prove it with certainty, I do not enter it. Because the outcome will be a bad outcome - the other side [the student] will understand that I know, will understand that I identified it [dishonest behavior], and will also understand that I cannot do anything about it. And therefore, it will reinforce this behavior.”
Recommendations for addressing the phenomenon
A substantial part of the interviews focused on strategies for eliminating or preventing dishonesty in both academic and clinical settings. The participants agreed that education for the values of professional integrity does not begin and end solely during formal academic training. On the contrary, they emphasized that integrity education is a lifelong process that must be continuously maintained among both students and practicing professionals. The recommendations centered on four main areas: examining each case of dishonesty individually; emphasizing the importance of education for integrity values, particularly following an incident of dishonesty; incorporating real-life examples from clinical practice into the educational process; and serving as a role model for students and professionals.
Leaders preferred restorative approaches rather than punitive responses. From the interviews, it emerged that the participants recommended thoroughly investigating each case of dishonesty and making decisions on a case-by-case basis. The interviewees agreed that enforcement measures are essential in all settings, both academic and clinical. However, the recommendation was not to rely exclusively on enforcement mechanisms, but rather to “look at the person” (Interviewee 2) and to consider the underlying reasons and circumstances of each incident. Interviewee 7 explained: “It depends on the circumstances of the case. You do not always have a punishment that fits every case and its specific circumstances.” Interviewee 3 further elaborated on how, in his professional opinion, cases of dishonesty should be addressed: “I think there is no uniform framework…each case must be considered individually, and therefore a disciplinary committee provides the opportunity for the individual to defend themselves, to express their perspective, and to convey their deep regret over what happened, or to offer an apology. Such a committee can certainly be composed of very experienced individuals within the system. It can assess each case on its own merits and can indeed reach the appropriate decision.”
The interviewees also agreed that following an incident of dishonesty, students or professionals should be given a second chance, rather than adopting a punitive “zero-tolerance” or “head-cutting” approach. Interviewee 7 explained: “…the system can adopt a head-cutting approach, but I do not think that head-cutting is the right way.” Interviewee 10 emphasized that “we cannot change a person’s DNA, but you can teach them or lead them to make this educational change. Ultimately, people do understand that this is a matter of human lives. When you explain and provide examples, you give them an opportunity.”
An additional theme that emerged as a means of addressing the phenomenon was education for integrity using real-life examples. The interviewees noted that this approach is effective for both students and practicing professionals. Interviewee 7 indicated that, among students, real cases of dishonesty should be brought “into classroom discussion,” while interviewee 1 added that “these examples should be linked to the consequences for the patient.” Regarding professionals, the interviewees suggested conducting more simulations based on real cases that occurred in practice and “flooding the process with examples that will be etched in memory” (Interviewee 5).
The final issue identified as effective in fostering integrity was the use of role modeling. The interviewees noted that, in their view, they serve as role models for students and junior professionals. Interviewee 6 stated: “We all need to understand that our conduct has an impact on the student… I cannot expect a student not to plagiarize a presentation if I present slides that are not my own, or if I have copied. Therefore, this requires ethical behavior, and it comes with holding a senior position.”
Moreover, some interviewees viewed role modeling as also involving acknowledgment and transparency in cases where individuals in senior positions themselves did not act with integrity. Interviewee 9 (head nursing manager in hospital) explained: “…it is also about setting an example in the sense that we are human. That is, I also make mistakes. This is not always simple in senior managerial roles and at the level of upper management.”
An open discussion about personal behavior and role modeling, led the most interviewees reported cases in which they had acted without full integrity during their professional careers. Interviewee 6 shared: “If we are talking about integrity, then in terms of integrity I cannot say that I never [acted dishonestly]. I never [acted dishonestly]. I try not to, but I cannot say that I never [acted dishonestly].” Nevertheless, all participants described themselves as honest individuals with strong professional values. Interviewee 4, that fill a senior position in academia, reflected on her own behavior: “I’m not saying you must be, like, an idiot and always just honest, honest, honest. There are also many things that happen…not everything needs to be told with absolute truth. And there are things that are not simple. But overall, this is what I stand by, and I think I am an honest person.”
Discussion
This study examined senior nursing leaders’ perceptions of integrity and dishonesty in academic and clinical contexts, highlighting three interrelated dimensions. First, integrity and dishonesty were described as existing along a continuum, with behaviors ranging from minor rule-bending to serious violations that threaten patient safety. Second, systemic factors, including organizational structures, cultural norms, and enforcement practices, were seen as shaping and influencing moral choices. Third, leadership practices, including education, role modeling, and individualized case management, were emphasized as essential for fostering integrity within complex and imperfect contexts.
Integrity in a continuum
Participants consistently described integrity and dishonesty as existing along a continuum rather than as mutually exclusive categories. This perception challenges traditional regulatory and educational frameworks,22,23 which tend to conceptualize dishonest behavior as a clear and unequivocal violation. Instead, the leaders differentiated between “minor” deviations, often framed as bending or stretching rules, and more severe acts that cross a moral threshold, particularly when patient safety is compromised.
The prominence of patient safety as the defining boundary is highly significant. It suggests that within nursing leadership discourse, the ethical weight of dishonest behavior is evaluated less in terms of formal rule-breaking and more in relation to the potential for harm. This harm-based orientation aligns with the profession’s foundational commitment to human dignity and the prioritization of patient welfare. 24 At the same time, constructing a hierarchy of dishonesty may inadvertently legitimize lower-level transgressions in academic 25 or administrative contexts. When such behaviors are perceived as relatively harmless, they may become normalized, gradually weakening the ethical climate. Over time, this normalization may influence professional socialization processes, particularly when students encounter ambiguous messages about acceptable conduct during formative stages of identity development.25,26 The findings therefore support viewing integrity and dishonesty not as fixed categories but as dynamic positions along a moral continuum that may shift across situations, career stages, and organizational contexts.
Furthermore, the leaders’ use of softened terminology, such as “cutting corners” or “bending the rules,” reflects a process of moral reframing. 27 Linguistic minimization does not merely describe behavior; it can shape how actions are interpreted and judged. By reducing the perceived severity of a transgression, such language may subtly shift moral evaluations and attenuate accountability. 28 In this sense, discourse itself becomes part of the ethical environment, influencing whether dishonest behaviors are confronted, tolerated, or implicitly justified.29,30
When systems shape moral choices
The leaders’ accounts suggest that dishonesty does not emerge solely from moral deficiency but from a dynamic interplay between personal disposition and structural opportunity. Competitive academic environments, heavy workloads, and ambiguous regulations may create conditions in which dishonesty is perceived as a rational (or at times even necessary) strategy. When these contextual pressures intersect with prior experiences of unpunished dishonest acts, they can reinforce patterns of normalization. In this sense, dishonesty becomes not merely an individual lapse but a predictable outcome of certain organizational conditions. Thus, integrity cannot be understood purely as an individual trait; it is co-constructed within systems that either constrain or enable ethical action.
This systemic dimension becomes even more apparent when examining how organizational responses (or the lack thereof) shape ethical boundaries in practice. If structures create opportunities for diffusing dishonest acts, 31 institutional reactions determine whether those opportunities solidify into norms. Beyond individual interpretations, the findings highlight the powerful role of organizational culture and systemic arrangements in shaping patterns of integrity and dishonesty. Participants repeatedly described institutional leniency, limited enforcement tools, and procedural complexity as factors that indirectly sustain dishonest conduct. When leaders hesitate to initiate disciplinary processes due to insufficient evidence or fear of ineffective outcomes, a silent message may be conveyed: that certain behaviors are known yet tolerated. Such dynamics contribute to what might be termed an “ethics gap” 32 —a discrepancy between espoused professional values and enacted organizational practices.
This ethics gap is particularly significant in nursing, a profession grounded in trust and accountability. 33 When formal codes emphasize integrity, but everyday practices reflect compromise or inconsistent enforcement, ethical standards risk becoming symbolic rather than operational. 34 Over time, this misalignment may erode both cognitive and emotional trust. 35 Importantly, students and junior nurses learn not only from curricula but from observation. 36 When they encounter inconsistencies between declared principles and actual conduct, they may adopt a pragmatic understanding of ethics, one guided by feasibility and survival rather than principled commitment.
Educating integrity in imperfect contexts
Participants advocated a balanced approach that integrates enforcement with education and individualized consideration. Their rejection of rigid zero-tolerance policies reflects an understanding of ethical development as dynamic rather than static. 37 By recommending case-by-case evaluation and opportunities for reflection, leaders positioned integrity as something that can be cultivated over time.
This approach resonates with contemporary models of professional identity formation, which view it as evolving through clinical supervisors’ mentorship, ethical competence, structure and cooperation. 38
At the same time, the findings reveal a persistent tension between ethical ideals and professional realities. Consistent with evidence that organizational constraints, moral distress, power imbalances, and resource limitations can threaten nurses’ integrity, 39 many participants acknowledged that complete transparency is not always feasible in complex clinical and managerial contexts. The candid admissions of senior leaders that they themselves had not always acted with full integrity underscore this complexity. Such reflections suggest that much like the principle that “to err is human,” 40 deviations from complete honesty may also reflect the imperfect nature of human practice rather than deliberate moral disregard. This perspective suggests that integrity is a developmental process rather than an expectation of flawless conduct from the outset. Expecting flawless ethical behavior from students or new graduates may be unrealistic; integrity develops over time through experience, reflection, mentorship, and ongoing engagement with ethical challenges.
In summary, the senior nursing leaders’ reflections suggest that absolute directness may be an aspirational ideal rather than a constant reality. Clinical work, managerial responsibility, and interpersonal dynamics often require discretion, partial disclosure, or strategic communication. In such contexts, rigid notions of truthfulness may collide with competing obligations, such as protecting patients, staff, or institutional stability. These tensions do not necessarily indicate moral failure but rather the inherent ambiguity of professional practice.
Implications
For educators
The findings highlight the need to conceptualize integrity as a developmental process rather than a fixed attribute. This developmental perspective suggests that ethics education should not be confined to undergraduate nursing programs but should continue throughout professional careers as part of lifelong learning. Nursing education programs should move beyond a solely rule-based approach and incorporate reflective ethics education that addresses ambiguity and real-world complexity. Integrating case-based learning using authentic clinical scenarios may help students understand the consequences of dishonest behaviors. Educators should explicitly address the “continuum” of integrity identified in this study, helping students recognize how minor academic dishonesty may translate into professional conduct. Finally, faculty must be aware of their role-modeling influence and strive for consistency between declared ethical standards and their own behaviors.
For hospital leaders
Hospital leaders play a critical role in shaping ethical climates. Cultures that tolerate minor deviations or inconsistently address dishonesty may normalize it. Leaders should strengthen ethical infrastructures with clear policies, consistent enforcement, and safe reporting channels. Balanced approaches combining accountability with learning and rehabilitation may be more effective than purely punitive strategies. Leadership programs should emphasize ethical decision-making, transparency, and role modeling to influence staff behavior.
For policy makers
At the policy level, the study emphasizes aligning regulations with real-world complexities. Policies should clearly define dishonest behaviors while allowing case-by-case flexibility. Strengthening enforcement and reducing regulatory ambiguity may help close the “ethics gap.” National policies should foster collaboration between educational institutions and healthcare organizations to maintain ethical standards across the academic-clinical continuum. Supporting systems like training, reporting structures, and leadership accountability can enhance integrity and patient safety.
For professional nursing codes
The findings of this study have implications for professional nursing codes of ethics. Overall, participants’ perspectives strongly align with core ethical principles embedded in existing codes, particularly regarding patient safety, accountability, and commitment to professional standards. At the same time, the findings highlight that ethical practice in real-world settings often involves navigating ambiguity, contextual pressures, and a continuum between integrity and dishonesty, rather than clear-cut categories. This suggests that while current codes provide essential foundational guidance, they may benefit from greater acknowledgment of the complexity of ethical decision-making in practice, particularly in relation to gray areas and systemic influences on professional conduct.
Strengths and limitations
This study has several strengths. It provides in-depth insights from senior nursing leaders across academia, clinical practice, and national policy, offering a comprehensive view of integrity across the educational-clinical continuum. The qualitative phenomenological approach enabled rich exploration of complex ethical perceptions, and participants’ extensive leadership experience enhances the findings’ relevance for decision-making and policy development.
However, there are limitations. The purposive sample may limit generalizability, reliance on self-reported perceptions may introduce social desirability bias, and findings may be influenced by cultural and organizational factors specific to the study setting.
Conclusions
The findings highlight that senior nursing leaders view integrity and dishonesty as complex and multifaceted. While integrity remains a central value, ethical decision-making often occurs in challenging, nuanced circumstances. Leadership involves balancing aspirational standards with everyday clinical and organizational realities.
Participants noted that pressures may lead to adjusting, withholding, or reinterpreting information, reflecting inherent tensions in decision-making rather than disregard for ethics. Recognizing that flawless conduct is difficult underscores the need for grounded, reflective approaches supported by organizational structures. Nursing leadership, therefore, promotes awareness, responsibility, and systems that minimize harm, framing integrity as an ongoing professional commitment shaped by real-world practice. Rather than expecting ethical perfection, educational and healthcare systems should support the continuous development of integrity throughout the professional lifespan.
Footnotes
Acknowledgments
We would like to thank and acknowledge all the senior leaders nurses who participated in this study.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that supports the findings of this study are available from the corresponding authors upon reasonable request.