
Abstract
An abdominal aortic aneurysm (AAA) is a potentially fatal vascular condition that often remains asymptomatic until rupture. Incidence of AAA remains higher among the elderly population, with smoking, hypertension, atherosclerosis and old age being the prominent risk factors. This disease tends to occur predominantly in males, but there are cases involving females.
A 56-year-old female presented with the sudden onset of back pain and breathlessness and was declared dead shortly after hospital admission. Autopsy revealed a giant AAA measuring 17 × 9 cm with rupture and retroperitoneal haemorrhage.
AAAs are established as one of the major catastrophes in older age group individuals and are found in 4%–7% of males and 1% of females aged 50 and above. As per the available literature, the present case appears to be very unusual in nature, considering the fact that it is more prevalent in males and rupture of the abdominal aorta is present only in 10% cases. A giant abdominal aneurysm amounts to a very rare entity. This case highlights the importance of early detection of AAA, especially in patients presenting with nonspecific symptoms such as abdominal or back pain.
Introduction
Abdominal aortic aneurysm (AAA) refers to an abnormal and localised dilatation of the aorta more than 3 cm in diameter or exceeding 50% of its normal calibre. The probability of AAA getting undetected until a tragic event occurs remains higher in view of the absence of clinical signs and symptoms. 1
Incidence of AAA remains higher among the elderly population, with smoking, hypertension, atherosclerosis and old age being the prominent risk factors. 2 Occurrence of AAA is recorded all over the world with significant variation, but usually remains undetermined in third-world countries due to restricted healthcare and diagnostic facilities. 3 Such cases constitute cases of sudden death coming to the emergency department and are considered as medico legal case.4–6
The majority of the cases of AAAs consist of no significant symptoms and tend to be detected accidentally while imaging for other conditions or on autopsy. Such a scenario is also depicted in cases of cardiac tamponade.7, 8 Incidence of rupture of the aorta relies on the size of the aneurysm and rate of expansion, with aneurysms larger than 5.5 cm having a higher probability of rupture. 9 Still rupture of a smaller aneurysm can occur sporadically, suggesting the role of patient-related factors in the fatality of the patients. 10
Rupture of AAAs leads to a life-threatening emergency condition as a result of severe blood loss, ultimately causing a high fatality rate. 11 Giant AAAs are considered to be those aneurysms having a diameter of more than 13 cm, constituting a very rare incidence but causing a very high risk of fatality. 12
The present case can be considered as one of the rare cases with unusual appearance due to its occurrence in a female patient, remarkably enormous size of the aneurysm and its uncommon site of occurrence. This case necessitates the vitality of earlier detection as well as more meticulous evaluation to be done in case of vague symptoms like abdominal or back pain.
Background
Fifty-six years old female was brought in with a history of sudden pain in the back and difficulty in breathing at midnight. She was admitted to the hospital and declared dead after some time while on treatment. There is also a history of suffering from hypertension and being on medication from a local doctor at the native place. There is also a history of pain in the abdomen and back in the past, for which she used to take painkillers from her general practitioner. As she was residing in a rural area, no investigations were done to suggest aortic disease. There is no history of tobacco smoking or chewing. There is no family history of cardiovascular diseases. There is no history of any other diseases or addictions.
Post-mortem Findings
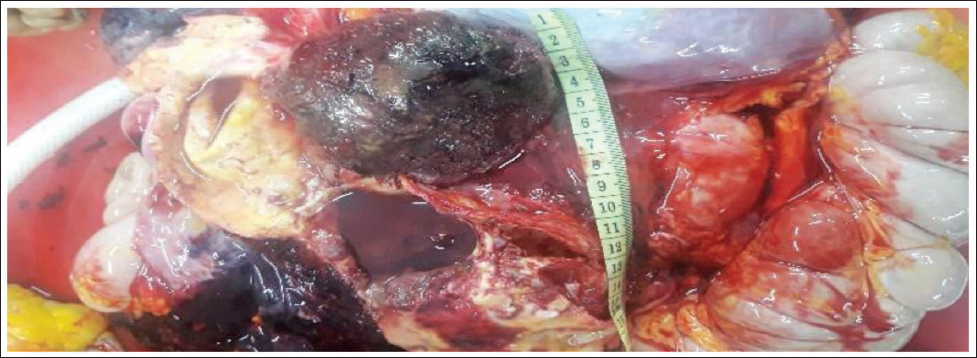
The deceased was thin-built and cachexic. On internal examination, the thyroid gland shows multiple cysts all over the gland. The abdominal aorta shows a fusiform-shaped aneurysm with multiple sacculations located in the upper part, situated 12 cm above the bifurcation of the aortas shown in Figures 1 and 2. One sacculation is present at the origin on the right side of the aorta, which is larger, while other sacculation present in the region of visceral artery ostia. All the arteries appear to arise from saccular outpouching. Part of it was covered with blood clots due to rupture. The size of the dilated cavity of the aneurysm was 17 cm × 09 cm. On opening the aorta, multiple atherosclerotic patches are present over the intimal surface of aorta. On opening the aneurysm in the second sacculation, a concavo-convex intraluminal thrombus mass was visible, which was whitish in colour on the concave surface and greenish-blackish in colour on the convex surface, weighing 120 grams, as shown in Figure 3. On incision over the mass, it shows multiple lamellae. The intimal surface of the aneurysm was showing multiple calcified atherosclerotic patches. Rupture present over the inferior aspect of the lower part of the aneurysm on the left side of size 01 cm × 0.5 cm. There were extravasations of blood and blood clots in surrounding tissues weighing about 500 grams on the left side of the aorta and around the left side of the kidney in the retroperitoneal space.
Location of Abdominal Aorta Aneurysm.
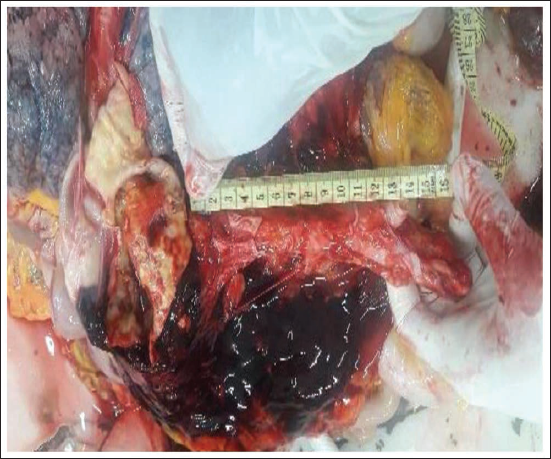
Abdominal Aortic Aneurysm.
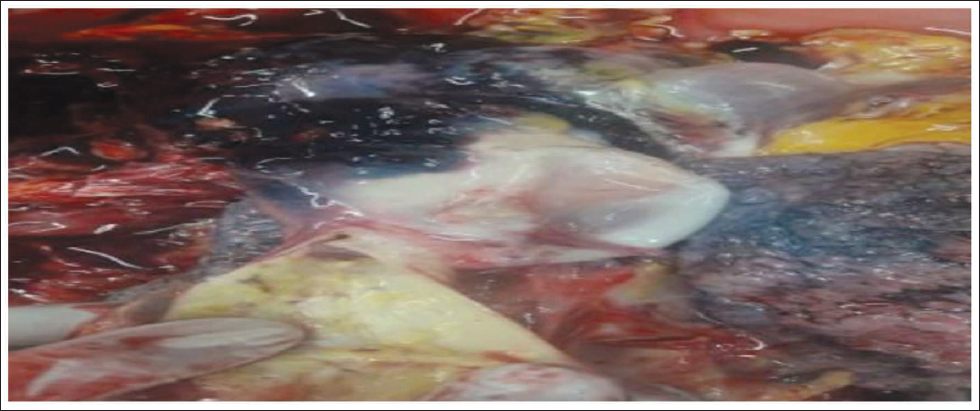
Intraluminal Thrombus in Aneurysm.
Both the kidneys were small, contracted, and the surface was granular. The spleen was congested, and subcapsular pus pockets were present.
Discussion
AAs are established as one of the major catastrophes in older age group individuals and are found in 4%–7% of males and 1% of females aged 50 and above. 13 Majority of the cases are from the age group of 55–65 years, while only 10% present in cases above 75 years. The male-to-female ratio was 9:1, clearly indicating male predominance. 14
Atherosclerosis is considered to perform vital role in dwindling the strength of the aortic wall, which was also evident in the present case.³ Present case shows the aneurysm measuring 17 × 9 cm, making it eligible to be classified as a giant AAA, which is extremely rare as well as associated with a higher risk of rupture. 12 Chronic nature of the thrombus can be inferred from the presence of laminated thrombus, which also contributes to the degeneration of the vessel wall. 10
Present case shows the location of the aneurysm being 12 cm above the bifurcation, which can be considered as unusual since the majority of AAAs are infrarenal. 9 This may have contributed to the delayed diagnosis. Significant blood loss results from rupture into the retroperitoneal space, as evident in the present case. 11 As per the available literature, the present case appears to be very unusual in nature, considering the fact that it is more prevalent in males and rupture of the abdominal aorta is present only in 10% cases. A giant abdominal aneurysm amounts to a very rare entity.
Conclusion
Rupture of a giant AAA appears to be a rare, catastrophic event with very high mortality. Dissemination of information about such catastrophic events, as well as regular screening, especially in rural areas, can be effective to curb such events in future.
Reduction of the incidence of deaths due to rupture of AAAs can be accomplished by ultrasonography, which can be a very valuable investigation in detecting any aortic aneurysm, especially in cases of abdominal pain or backache. Early Screening in Males >65 years with hypertension, Chronic Obstructive Pulmonary Disease can be helpful for early discovery of an aortic aneurysm.
Footnotes
Abbreviation
AAA: Abdominal aortic aneurysm
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Informed consent was taken from the participant.