
Abstract
Sex estimation in forensic anthropology is essential for identifying human skeletal remains. However, there remains a need for cost-effective, simple, and reliable methods, particularly in cases where skulls are found at crime scenes or are damaged. This study analyzed 13 cranial parameters from 404 CT-derived skull images of Thai individuals (202 females, 202 males) using standard anthropometric techniques for sex classification. Discriminant analysis revealed that the 12-parameter model achieved a sex classification accuracy ranging from 57.8% to 77.6%. The accuracy significantly improved to 83.9% with the inclusion of six parameters: Biorbital breadth, basion–bregma height, maximum cranial length, mastoid height, lambda–opisthion chord, and foramen magnum length. These findings underscore the potential of cranial morphometric analysis via computed tomography imaging as a supplementary tool for sex estimation in Thai populations. To establish a population-specific standard, further research with larger sample sizes, additional morphometric landmarks, and expanded skull indices is necessary. Additionally, ensuring accurate nationality verification remains crucial for enhancing the reliability of this approach.
Highlights
CT-based cranial morphometry aids sex estimation in Thai forensic anthropology.
Analysis of 13 cranial parameters achieved up to 83.9% classification accuracy.
Lateral view parameters showed the highest accuracy for sex determination.
Minimal parameter sets improved classification efficiency in forensic applications.
Introduction
Sex determination is a fundamental step in the identification of skeletal remains, particularly in forensic contexts. While biological differences between males and females can often be observed, more objective and reliable methods are required for legal procedures and court presentations. Molecular approaches, such as sex chromosome analysis, are widely recognized for their high reliability; however, these techniques are costly and time-consuming.1, 2 Alternatively, forensic anthropologists often rely on morphological characteristics of bones to estimate sex. Although effective, this method is subjective and requires significant expertise. For instance, morphological assessments of skeletal features, such as the pelvis and skull. 3
Skeletal morphometric analysis offers a quantitative approach to osteological assessment, providing more objective results and serving as a supplementary method for estimating sexual dimorphism. However, forensic cases often involve incomplete or damaged skeletons due to dismemberment or decomposition, which limits the applicability of traditional methods. This necessitates the use of diverse osteometric measurements from different skeletal parts as substitutes. For example, studies on cranial morphometric analysis in Thai populations have demonstrated accuracy rates for sex determination, with parameters such as glabella prominence, zygomatic arch dimensions, and occipital condyle measurements showing high discriminatory power. These findings align with cranioscopy methods (Krogman’s traits) and confirm the skull’s utility as a reliable indicator of sex in forensic anthropology.3–5
Recent advancements in imaging technology have introduced computed tomography (CT) scans as a valuable tool for sex estimation. CT imaging enables precise morphometric analysis of skeletal remains, even in cases where physical access to the bones is restricted or the skeleton is incomplete. Studies have demonstrated the reliability of cranial morphometric analysis via CT imaging for sex determination across various populations.6–9 This approach not only enhances objectivity but also allows for the establishment of population-specific standards for sex estimation.
In this study, we utilize cranial morphometric parameters derived from CT images of Thai skulls to evaluate their effectiveness in sex determination. By analyzing 13 cranial parameters and refining models with additional variables, we aim to establish a reliable and practical method for sex estimation tailored to the Thai population.
Material and Method
Human Ethics and Consent to Participate Declarations
Study protocols were approved by the Human Research Ethics Committee of Thammasat University (Science), Thailand, in accordance with the compliance with the Declaration of Helsinki, the Belmont Report, CIOMS guidelines, and the international practice (ICH-GCP) (COA No. 081/2567,67AH085). This study does not involve clinical trials or direct participation in human subjects. The CT images and associated data (sex and age) used in this study were obtained from an internal anonymized database maintained by Thammasat University Hospital. All personal identifiers were removed prior to analysis.
Data Collection
All 404 Thai population skull CT images data from Thammasat University Hospital—the Premium Clinic Center and the Division of Diagnostic and Interventional Radiology, Department of Radiology—were compiled, accompanied by known age and sex data (202 females, age = 18–96 years old and 202 males, age = 19–92 years old). The exclusion criteria included specimens exhibiting pathological conditions or surgical alterations that result in skull deformities.
Measurement
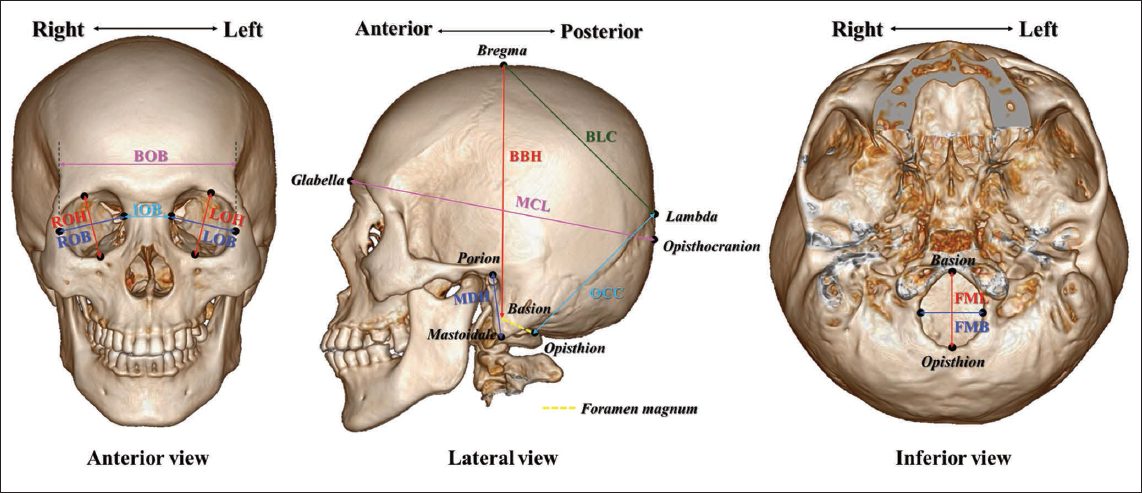
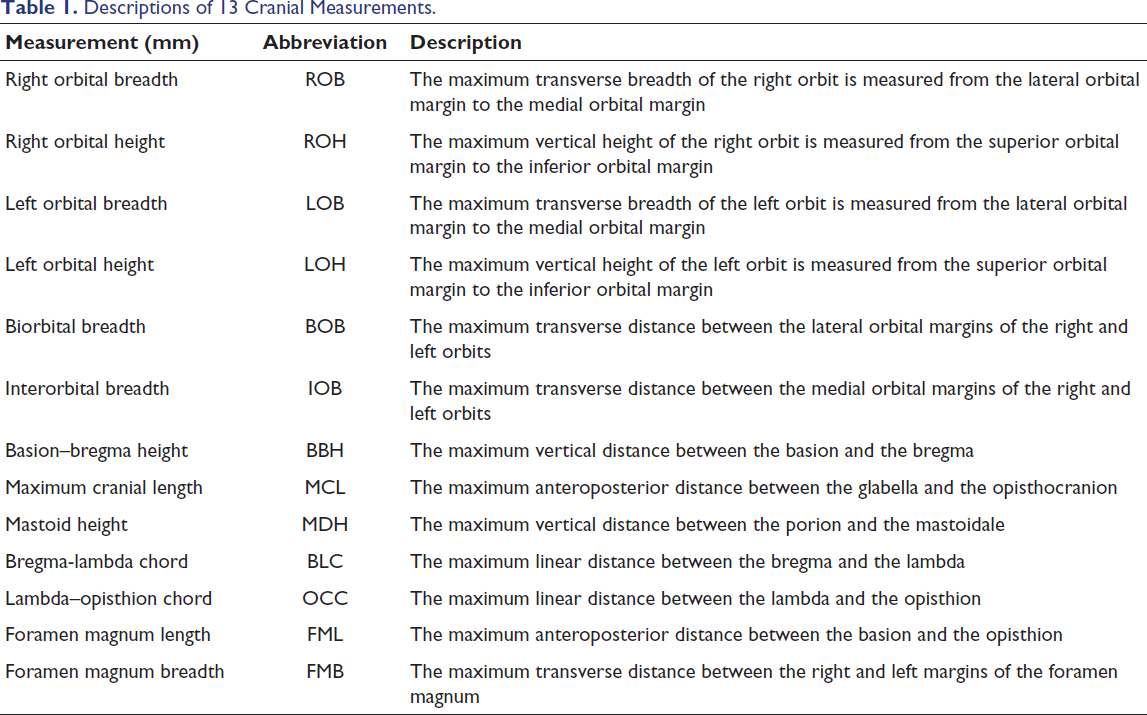
Thirteen cranial measurements were obtained from reconstructed 3D skull images, which were generated using cross-sectional data from brain CT scans acquired with the Philips Spectral CT 7000 series 256-slice system (Philips Healthcare, the Netherlands). The imaging data were processed to create 3D models of the skull, ensuring accurate anatomical representation. Measurements were performed on these reconstructed images using the Philips DICOM Viewer (Philips Healthcare, the Netherlands), allowing for precise identification and analysis of the 13 cranial parameters (Figure 1 and Table 1).10–12
The Positions of 13 Cranial Measurements in this Study: The Descriptions Followed by Table 1.
Descriptions of 13 Cranial Measurements.
Statistical Analyses
Inter-observer variation was assessed by having two independent observers—fourth-year radiological technology students (Observer 1 and Observer 2)—measure all subjects on the same day. Intra-observer variation was evaluated by repeating measurements on 10 randomly selected cases 1 month after the initial measurement. To assess accuracy and reliability, the relative technical error of measurement (rTEM) and the coefficient of reliability (R) were calculated. Statistical analysis was conducted using IBM SPSS Statistics version 26.0.0. Descriptive statistics were reported, including mean and standard deviation (SD). A Student’s t test was employed to identify significant differences between measurements by the observers and between sex groups, with statistical significance set at p < .05.
Grouping Matrix and Unknown Sample Test
A stepwise discriminant analysis was conducted to identify the most effective combinations of six parameters for sex classification. Combinations of two to five parameters were tested systematically, with variable inclusion guided by Wilks’ lambda and a significance threshold of p < .05. Final equations were chosen based on their ability to maximize classification accuracy and statistical significance.
To validate the models, the discriminant equations were applied to an independent validation dataset of 82 individuals (42 females, 40 males). Predictive performance was evaluated by comparing predicted versus known sex, with classification accuracy, sensitivity, and specificity calculated to evaluate the models’ reliability. The classification performance was adjusted for Thailand’s 2024 female prevalence (51.32%) to account for the validation dataset’s non-representative sex ratio, ensuring real-world applicability.
Result
Inter- and Intra-observer Reliability and Technical Error of Measurement
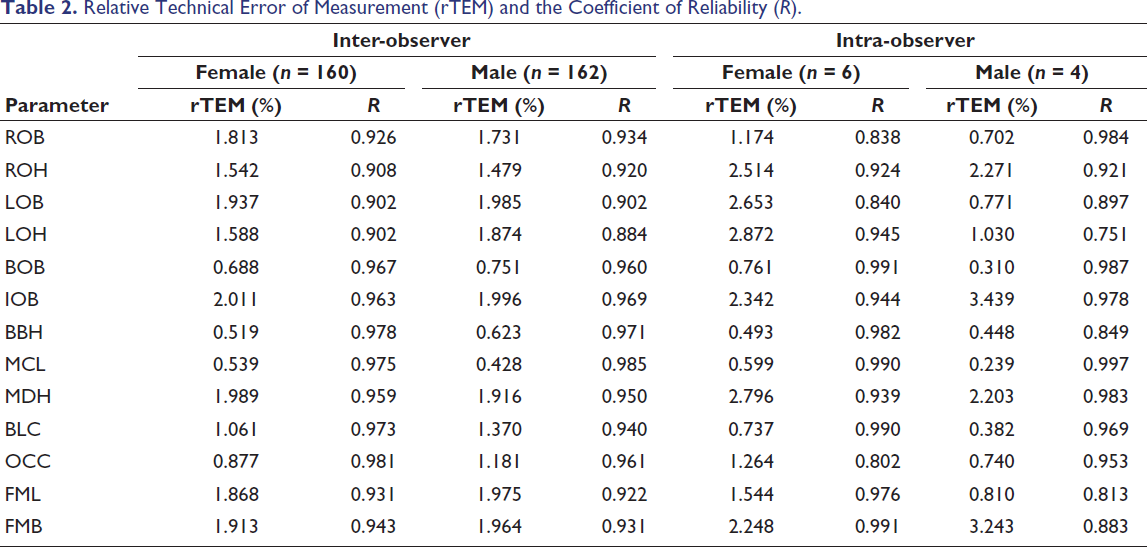
To evaluate the consistency of the 13 cranial morphometric parameters between two observers, the rTEM and the reliability coefficient (R) were calculated. For beginner-level measurements, acceptable rTEM thresholds were set below 5.0% 13 for both inter-observer and intra-observer assessments. Anthropometric precision was defined by R values greater than 0.75. 14 As detailed in Table 2, both inter-observer and intra-observer rTEM values fell comfortably within the acceptable range, and all R values exceeded the 0.75 threshold. These findings indicate a high degree of precision and reliability in the measurement methodology used in this study.
Relative Technical Error of Measurement (rTEM) and the Coefficient of Reliability (R).
The Relationship Between Cranial Morphometric Traits and Sexual Dimorphism
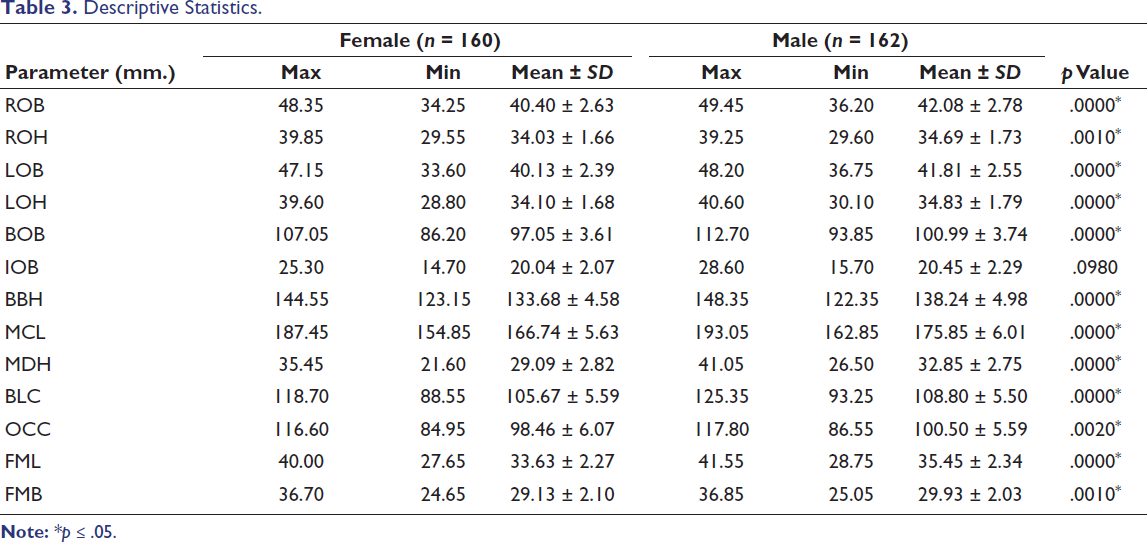
To examine the correlation between cranial morphology and sexual dimorphism, 13 cranial parameters were analyzed. Statistical summaries and the descriptive salient results of these cranial variables are presented in Table 3. The analysis revealed a strong pattern of sexual dimorphism, with males exhibiting significantly larger mean values across most cranial measurements compared to females (p ≤ .05). Notably, parameters such as maximum cranial length (MCL), basion–bregma height (BBH), and mastoid height (MDH) demonstrated the most pronounced dimensional differences between the sexes. Interorbital breadth (IOB) was the only parameter that did not yield a statistically significant difference (p = .0980).
Descriptive Statistics.
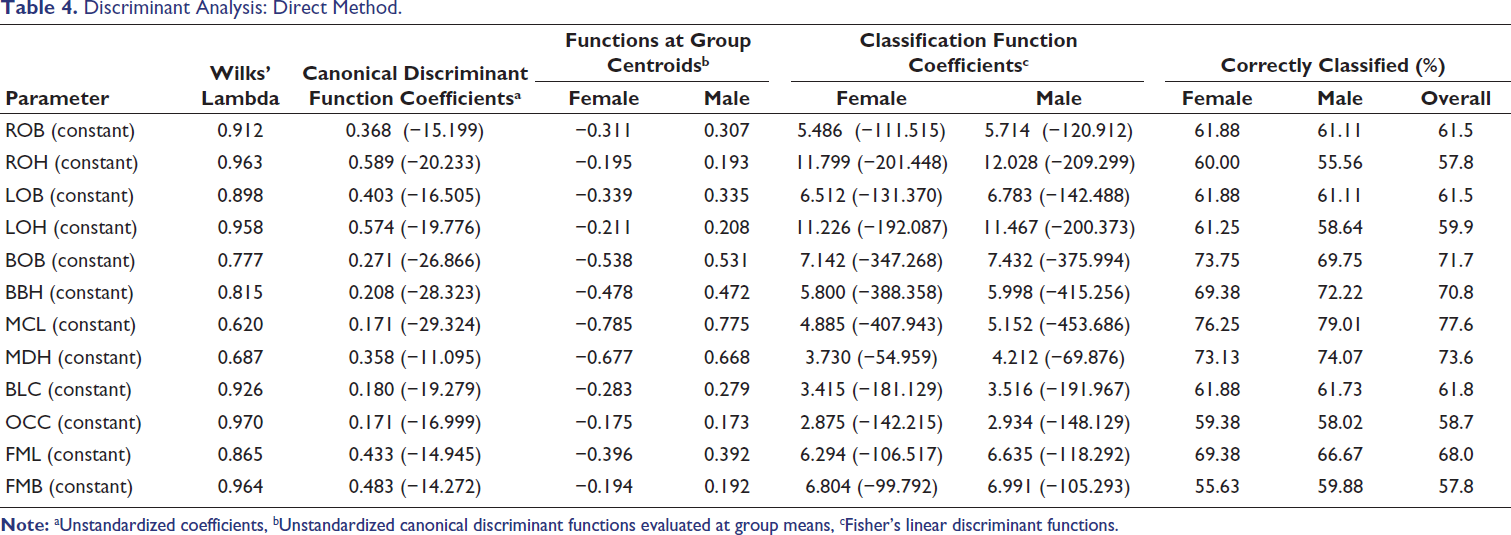
Subsequently, these sexually dimorphic parameters were utilized in a direct discriminant analysis for sex classification (Table 4). The results highlighted that biorbital breadth (BOB), BBH, MCL, and MDH were the most reliable individual predictors, each achieving a correct sex classification rate exceeding 70%. In contrast, the remaining single parameters demonstrated classification rates below 70%, with the weakest discriminatory power observed for right orbital height (ROH) and foramen magnum breadth (FMB), both at 57.8%.
Discriminant Analysis: Direct Method.
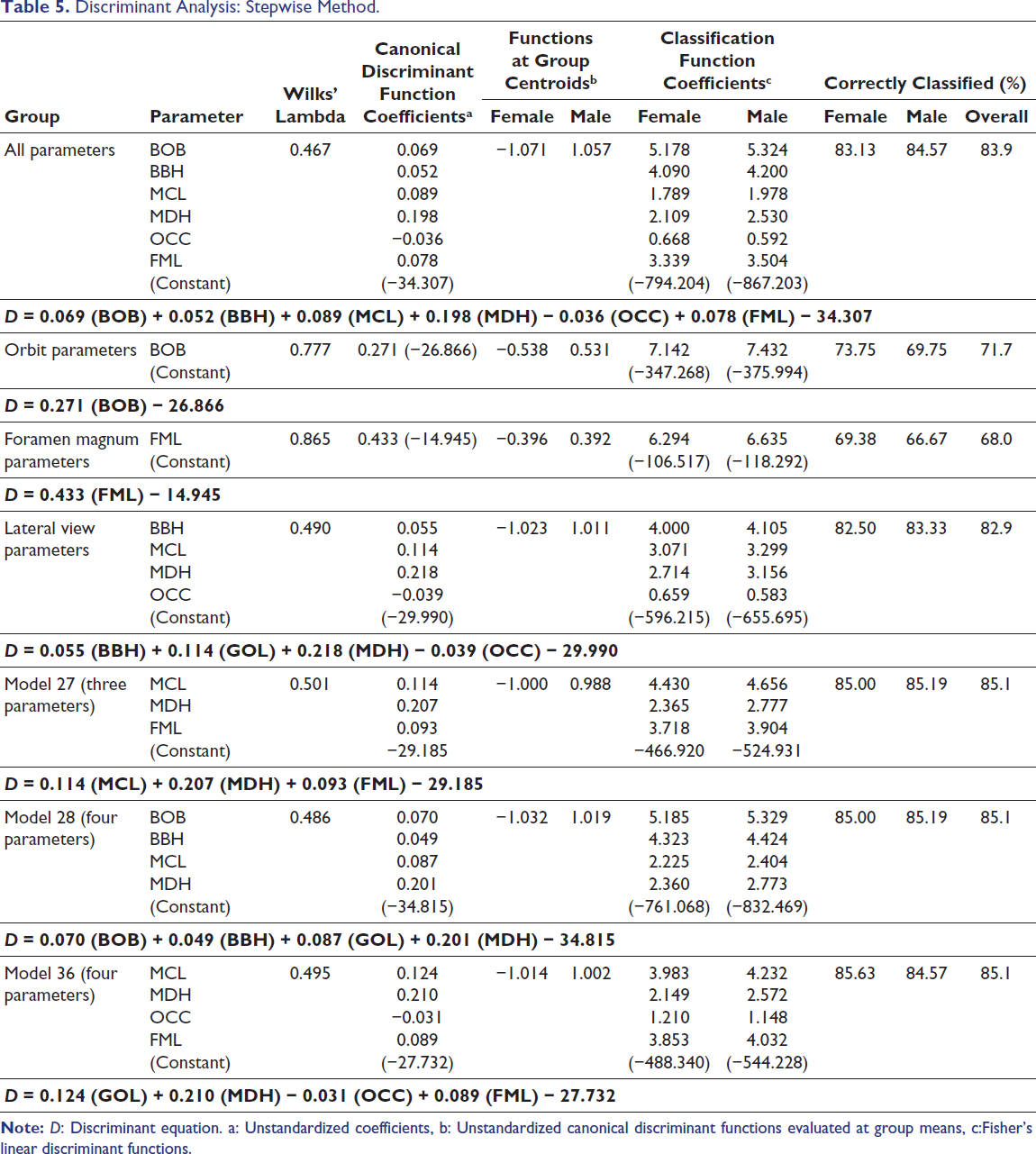
Furthermore, a stepwise discriminant analysis was conducted to determine the optimal multivariable set of skull parameters for sex classification. As presented in Table 5, the most salient finding is that integrating six specific parameters (BOB, BBH, MCL, MDH, lambda–opisthion chord (OCC), and foramen magnum length (FML) yielded the highest overall classification accuracy of 83.9%, utilizing the discriminant equation: D = 0.069 (BOB) + 0.052 (BBH) + 0.089 (MCL) + 0.198 (MDH) − 0.036 (OCC) + 0.078 (FML) − 34.307. When regional analyses were performed, the lateral view parameters (BBH, MCL, MDH, and OCC) provided an exceptional approximation to the full model, achieving an 82.9% accuracy. This indicates that the lateral aspect of the cranium holds robust diagnostic value. In contrast, analyses relying solely on BOB or FML parameters resulted in significantly lower classification rates (71.7% and 68.0%, respectively) (Table 5).
Discriminant Analysis: Stepwise Method.
Evaluation of the Model for Sex Determination
The predictive performance of various cranial parameter sets for sex classification was rigorously assessed using key diagnostic metrics on an unknown sample cohort (Table 6 and Supplementary 4). The most salient finding from this validation phase is that Model 28, which integrates four parameters (BOB, BBH, MCL, and MDH), demonstrated the most robust and reliable classification. It achieved an overall accuracy of 83.45%, alongside a perfect specificity (100%) and a 100% predictive value for females.
Diagnostic Test Evaluation of Unknown Samples.
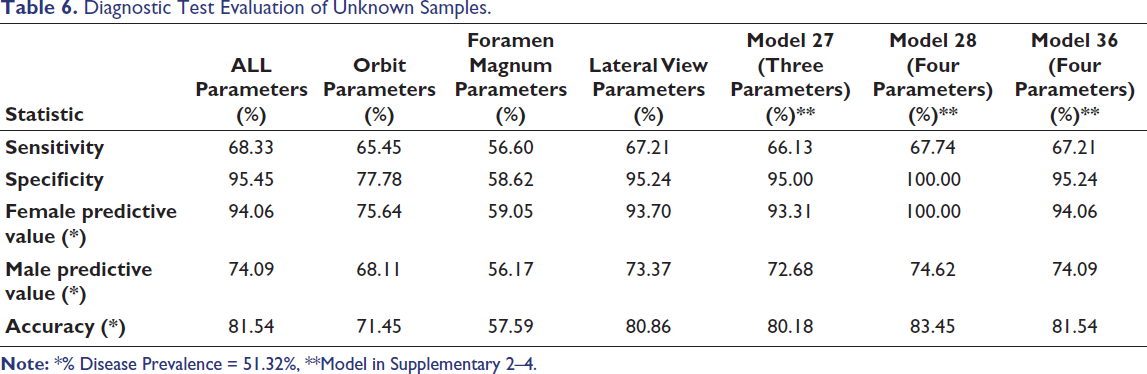
Additionally, the comprehensive six-parameter model (all parameters) exhibited strong overall performance, yielding an accuracy of 81.54% and the highest sensitivity among all evaluated models (68.33%). Conversely, models relying solely on foramen magnum parameters proved to be the least effective, generating the lowest classification accuracy at 57.59%.
Interestingly, the analysis of minimal parameter sets revealed highly promising results. Model 10, which utilizes only two parameters (BBH and MDH; detailed in Supplementary 2 and 3), achieved a baseline accuracy of 80.4% and an impressively high classification accuracy of 85.1% when applied to the unknown samples (Supplementary 4). This salient result strongly suggests that a carefully selected, minimal parameter set can achieve highly effective sex classification. Such streamlined models are particularly advantageous in forensic anthropology, where skeletal remains are frequently fragmented or incomplete, allowing practitioners to reliably estimate sex without requiring a perfectly intact cranium.
Discussion
The examination of differences in cranial morphometrics may be crucial in forensic anthropology when identifying the sex of a skull. Dimorphism in distinct areas of the skull has been supported by morphometric research conducted on different populations using various study approaches. 15 Previous craniometric investigations carried out in Asia, Europe, and Thailand have also started using CT imaging as sex determination gained popularity, proving its promise in the development of forensic anthropology.16, 17
This study underscores the potential of cranial morphometric analysis as a dependable method for sex determination in the Thai population, utilizing CT imaging. By investigating 13 cranial parameters from 404 CT-derived cranium images, the results demonstrate the accuracy with which cranial morphometric analysis with CT imaging can determine a person’s sex in Thai people. According to our findings, there was substantial sexual dimorphism in 12 out of 13 cranial measures (p < .05), and males consistently had higher mean values than females. One observation from the study’s results is categorized into three group parameters: orbit, foramen magnum, and lateral view parameters. For orbit parameters, the analysis indicated that BOB provides a sex classification, while the orbit zone demonstrated a low classification accuracy of 71.7%. This is consistent with earlier findings that suggest a relatively low accuracy rate for BOB, ranging from 50% to 72.3%.18–20
The parameters of the foramen magnum demonstrated limited effectiveness as isolated variables, yielding an accuracy rate of 68.0%. Previous investigations have highlighted the forensic significance of foramen magnum dimensions, noting a low classification accuracy ranging from 63.6% to 68%.21–24 To contextualize these findings within a broader Asian demographic, recent studies on Indian populations have also explored the diagnostic value of the cranial base, demonstrating that foramen magnum and occipital condyle measurements exhibit significant sexual dimorphism, achieving classification accuracies ranging from 70% to 94% depending on the multivariable combinations used.25, 26 This suggests that while the orbit or foramen magnum alone may not be a reliable indicator of sex, they can significantly enhance accuracy when used in conjunction with other morphometric traits.
In contrast, the lateral view parameters—specifically BBH, MCL, MDH, and OCC—proved to be significant contributors to accurate sex classification. When combined, these parameters achieved a classification accuracy of 82.9%, closely approximating the performance of the full parameter model (83.9%) and suggesting their potential utility when other cranial regions are compromised or inaccessible. The biological reasoning behind these observed sex differences—particularly the pronounced dimorphism in MDH and the occipital region—stems from distinct growth trajectories and biomechanical forces. Males typically experience a prolonged growth period influenced by hormones such as testosterone, resulting in greater overall cranial vault dimensions. Furthermore, stronger muscular attachments, such as the pull of the sternocleidomastoid muscle on the mastoid process, result in significantly larger and more prominent bony landmarks in males compared to females.
Discriminant analysis further demonstrated that classification accuracy significantly improved when multiple parameters were combined. The most effective model, which incorporated BOB, BBH, MCL, MDH, OCC, and FML, achieved an accuracy of 83.9%, surpassing or equaling the rates observed in previous studies utilizing traditional morphoscopic assessments.15, 27, 28 From a taphonomic perspective, the reliance on base-of-skull and lateral inner structures is highly practical, as these robust anatomical regions frequently survive degradation better than fragile facial bones. 29 This overarching trend of male craniofacial robusticity and the efficacy of multivariable CT analysis is corroborated by extensive studies across Asia. For instance, recent CT-based craniometric analyses in contemporary Japanese and Chinese populations achieved high sex classification accuracies (89.3%–93.9%) when applying stepwise multivariable models.10, 27 These East Asian studies, along with Indian research investigating maxillofacial dimensions and combined cranial data,30–32 consistently validate that integrating multiple parameters significantly enhances forensic reliability.
Interestingly, the classification accuracy can reach as high as 85.1% when utilizing carefully selected minimal parameter sets (e.g., two to four parameters) that perform higher than or equal to the full parameter or lateral view parameters. This enhanced accuracy underscores the significance of strategic parameter selection. However, despite the shared biological trends of sexual dimorphism across Asian populations, the specific parameters that yield the highest accuracy vary. While facial breadth might be highly dimorphic in Japanese populations (R7), our study highlights the lateral vault and mastoid regions in Thais. As highlighted by a recent systematic review of Southeast Asian populations, craniofacial traits are heavily influenced by a complex interplay of specific genetic, nutritional, and environmental factors unique to each region, making sex estimation inherently population-specific. 33 Therefore, applying diagnostic algorithms derived from Chinese, Japanese, Indian, or other foreign populations directly to Thai skeletal remains would likely yield suboptimal results. This highlights the absolute need for validation across diverse sample sets to establish robust, population-specific standards for forensic applications. Future investigations should delve into the predictive potential of minimal parameter sets within larger, more diverse populations to enhance and substantiate these findings further.
Conclusion
In conclusion, our study underscores the potential of cranial morphometric analysis via CT imaging as a supplementary method for sex determination in the Thai population. However, to establish a population-specific standard for sex classification using cranial morphometrics in Thailand, further research with larger sample sizes, additional morphometric landmarks, and expanded skull indices is necessary. Additionally, ensuring accurate nationality verification remains crucial for improving the reliability of this approach.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to the Premium Clinic Center and the Division of Diagnostic and Interventional Radiology, Department of Radiology, Thammasat University Hospital, for their support in providing CT images and analytical software used in this study.Final, thank you to Chutikan Chumnumporn, Jirarat Kwangnok, Napatsiri Khamsuk, Natnicha Khosungnoen, and Patiwet Sihanet for your help in collecting data.
Authors’ Contributions
Kochakorn Phantawong: Methodology, validation, investigation, resources, writing—review and editing; Kwanlada Mitpakdi: Methodology, investigation, resources, writing—review and editing; Sunisa Aobaom: Conceptualization, validation, formal analysis, data curation, writing—original draft, writing—review and editing, project administration, funding acquisition.
Clinical Trial Number
Not applicable.
Data Availability Statements
The data that support the findings will be available in Aobaom, Sunisa (2025), “Raw data of 13 Cranial Morphometric (F = Female and M = Male) n = 322,” Mendeley Data, V1, doi: 10.17632/wn2x8pb844.1
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Study protocols were approved by the Human Research Ethics Committee of Thammasat University (Science), Thailand, in accordance with the compliance with the Declaration of Helsinki, the Belmont Report, CIOMS guidelines, and the international practice (ICH-GCP) (COA No. 081/2567,67AH085). This study does not involve clinical trials or direct participation of human subjects. The CT images and associated data (sex and age) used in this study were obtained from an internal anonymized database maintained by Thammasat University Hospital. All personal identifiers were removed prior to analysis.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the financial support provided by the Faculty of Allied Health Sciences Research Fund, Contract No. AHSINTE 1/2567.
Informed Consent
Informed consent was obtained from Thammasat University Hospital at Premium Clinic Center, Radiology and Laboratory Patient Building, and Thammasat Medical Imaging and Intervention Center for all blind informative CT imaging.
Research Involving Human Participants and/or Animals
Not applicable.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.