
Abstract
This article studies three graphic memoirs by women, Marisa Acocella Marchetto’s Cancer Vixen, Sarah Leavitt’s Tangles and Leah Hayes’ Not Funny Ha-Ha, to explore the use of the graphic form in the narrating of an experience of illness. I argue here that these writers engage the graphic form to visualise female embodiment as always already pathologised, even prior to the onset of illness. By making explicit the medical and socio-cultural scrutiny of female bodily practices, these texts interrogate the unequal structural relationship between the sign of gender female and the healthy/sick binary set up by mainstream illness narratives. This article also proposes that these graphic memoirs of illness by women perform a resistant femininity in narrative by refusing a linear progression from diagnosis to cure. The texts instead make visible their myriad sources, in the form of incoherent speech, unedited data, photographs and letters among others, thus refusing unity and coherence in the narrating self.
Introduction
Women’s life writing in graphic form allows for the articulation/inscribing of multiple selves, permits the exploration of typically private subjects like the body, sexual trauma and taboo, vehemently makes visible what otherwise ought not to be, or cannot be, seen and instantiates an eversion of states of interiority (Allison, 2014; Basu, 2007; Chute, 2008; Nayar, 2015; Squier, 2008). Hillary Chute has argued for the appeal of the graphic form in service of a feminist methodology (Chute, 2008, 2010). The graphic form is of particular value for articulating ‘feminist aesthetics’ as Chute terms it (Chute, 2010), especially in the case of the graphic illness narrative as it manifests a re-assertion of agency and allows for the enunciation of the voices of a community (Nayar, 2015). Feminist aesthetics for Chute is a distinctiveness in form and style that allows for the articulation of a hybrid and ongoing project of the self. Graphic narrative and comics are thus a very suitable form for women’s writing, especially about the subject of trauma.
Writing about the suitability of graphic narrative and particularly graphic memoir for conveying a story of illness, Nancy Miller highlights the genre’s ability to depict contradictory truths in a single panel, the body’s states of extremes that require something more than words or telling (Miller, 2014). Miller’s essay itself oscillates between criticism and graphic narrative as she appends her own attempts at collages made about her cancer diagnosis in 2011. This innovative mode, encapsulated in the recent Graphic Medicine Manifesto (Czerwiek et al., 2015), challenges the conventions of academic writing by demonstrating its limits. Miller, like the editors and writers featured in the Graphic Medicine Manifesto, participates in the symbolic practice of graphic narrative, refusing a separation between the form and the academic discourse it occasions. The critic thus becomes producer, in addition to being reader/consumer and widens the reach of academic discourse (by making it subjective, using a ‘popular’ visual medium) while demonstrating the ever-expanding lexicon of meaning that attaches to the signifier of a particular disease. Miller own graphic testaments to her shocking diagnosis demonstrate what is true for most graphic narratives of illness: they illustrate the inadequacy (or ‘aversion to’, to use Miller’s term) of language when faced with the particularity of an illness experience and the universalised generality of its medical prognosis. More importantly, Miller’s drawings in a critical essay about the genre’s suitability to certain subjects also signals to the particular relevance of form in communicating certain experiences.
This paper will attempt to explore the intervention made by graphic narratives of illness or ‘autopathographics’ (Waples, 2014, p. 159) in fashioning the ill-self in graphic memoirs authored by women. These narratives utilise the ill body and a certain representational mode to speak of the self. I focus here specifically on Marisa Acocella Marchetto’s Cancer Vixen, Sarah Leavitt’s Tangles and Leah Hayes’ Not Funny Ha-Ha to make a case for how the graphic form allows for the representation and exploration of a gendered experience of looking and being-looked-at during an experience of illness and its medical management. In narrating a particularised story of illness experience, these women authors illustrate through and are enabled by a form that allows the scripting of feminised modes of recording/narrating that in turn allows for the articulation of female subjectivity within illness and medical treatment.
I will now briefly detail the three autopathographics that I study here. Cancer Vixen narrates for the reader the period in Marisa Acocella Marchetto’s life when she battles her breast cancer diagnosis and its treatment. Cancer Vixen has received popular and critical/academic attention, defined as a ‘Cancer in the City’ tale that recalls the bright colour, glamour and couture of the television series Sex and the City by the NYU Literature, Arts and Medicine database and is reported to be in production with HBO for a television movie adaptation. 1 Marchetto, a cartoonist for The New Yorker, combines the satiric elements of the newspaper cartoon strip with autopathographic ‘reportage’ to map specific moments of diagnosis, treatment and eventual recovery. Marchetto is seen to eventually ‘triumph’ over her cancer but the novel ends with the recognition of the possibility of future recurrence. Tangles, in sharp contrast, maintains a very sombre tone and uses minimalist line-drawings to portray the author’s witnessing of her mother’s slow succumbing to Alzheimer’s and eventual death. Sarah Leavitt also testifies to keeping a journal and graphically represents her family’s experience of caring for her mother in addition to her various attempts at ‘documenting’ her mother’s condition. I use ‘testifies’ here to illustrate Leavitt’s positioning of Tangles as the culmination of various processes of documentation that were occurring simultaneously with her mother’s manifestation of the symptoms of Alzheimer’s.
Lisa Hayes’ Not Funny enters the conversation surrounding the subject of abortion by narrating two instances of experiencing/‘choosing’ a medical termination of pregnancy that are visualised in very intimate detail but are nonetheless universal. Hayes’ book graphically represents the story of two girls whom she titles Lisa and Mary and they have no defining features save for their choice of two very different methods of terminating pregnancy. Hayes informs the reader that these girls do not know one another and live in different places but have been brought together in this narrative on account of their shared context of unanticipated pregnancy. Not Funny is subtitled ‘A Handbook for Something Hard’ and does precisely this—it is like Cancer Vixen in its potential to reach the young woman reader (the ‘girls’ featured in the book are 23 and 31 years, respectively) for whom, Hayes states, it is paradoxically lonely to go through a procedure that many women undergo. Deciding to go through with an abortion, for instance, is not made easier by the knowledge that it is an experience shared by numerous others. These others are not only ‘unknown’ in the sense that there is often little public discourse about what to expect during an abortion (in contrast with widely advertised technologies for the treatment of infertility) and much public censure of the decision. The experience of medically terminating pregnancy is thus, for Hayes, a very lonely one and very individualistic in the sense that the physical and emotional trauma is seen to be borne (at least by the two characters in the book) in isolation. While each of these autopathographics are varied in their visual style and approach to narrativising the ‘self’ in the context of illness, they are considered together here because they perform in various ways, the anxieties regarding embodiment and representation in the socio-cultural or lived experience of illness as they pertain to women.
This article is located at the intersection of medical and cultural discourses that gender the body and practices of the gendered body that negotiate with and resist regulatory mechanisms within which they are inscribed. This is owing to the pathographics’ central focus on the body in the extremes of suffering in the experience and care of illness though visualised via a gendered lens. The body in the extremes of suffering in these narratives means not only the transformation of the individual and his/her everyday in advanced stages of illness but also the excessive nature of the practices that govern the gendered body in our contemporary context. In her examination of the history of knowledge produced about the biomedical body in Leaky Bodies, Shildrick argues that this predominantly ‘masculinist’ domain has tended to undervalue corporeality. She emphasises the importance of exploring the body ‘anew’ for a project of ‘resistant feminism’ (Shildrick, 1994, p. 7). An undervaluing of corporeality, Shildrick argues, hierarchised the difference between male and female bodies in Western cultural history. The woman’s body was seen to be ‘grossly’ material and thus an inferior paradigm of excess, liminality and indeterminate boundaries.
I will argue here that contemporary women’s autopathographics perform a resistant femininity in narrative, an instance of a textual bodily practice that nonetheless draws upon and influences the practical lives of women in illness and medical treatment. By a bodily practice that is textual, I mean a symbolic representation of embodiment that is informed not by norms and ideals, but particular, subjective experiences. Building on Michel Foucault, Susan Bordo draws attention in her Unbearable Weight to the primacy of practice over beliefs about the body. Prevailing norms about masculinity, femininity and selfhood are impressed upon us not primarily through ideology but through the regulation and organising of the ‘time, space and movements of our daily lives’ through which our bodies are trained and shaped (Bordo, 1993, p. 166). The regulation of the everyday is often greater in the lives of women, for whom a recent re-entry into the public arena has only meant an exacting focus on diet, dress and make-up that renders them very focused on the improvement of the self at the expense of the social. Moreover, the appropriateness of the self’s ‘surface presentation’ can now be learned directly through bodily discourse. This discourse is crystallised in the contemporary visual/image rather than the verbal, through which we learn what to wear, what body shape is desirable and what bodily movements and expressions are appropriate (Bordo, 1993, p. 170).
Autopathographics by women are thus an important locus for a resistant/individualised visual articulation of feminine bodily discourse. The study of autopathographics forms part of an emerging genre of criticism that Martha Stoddard Holmes titles ‘graphic body studies’ (Holmes, 2013/2014, p. 147). Graphic body studies explores the term ‘graphic’ itself, which signifies the subversive and scandalous possibilities that comics and visual representations of the body have shared historically as well as the practice of visually communicating embodied experience. Though Holmes is speaking with specific reference to ‘cancer comics’ (narrating cancer through sequential art has arguably been the most visible/popular within the graphic form and more generally, cancer stories abound in the larger corpus of cultural narratives about illness), I argue that autopathographics by women can also be productively studied for their aesthetic and socio-political reframing of the bodily discourse of illness and its treatment. The lived experience of illness is characterised by visible, often sustained, periods of physical transformation and graphic accounts can present the reader with a rich array of perpetually changing bodies—across panels, within a single page. The artist’s rendering of her own self is thus not unitary and poses intentional (creative, ironic) and unintentional (technical weaknesses inherent in hand-drawn images that may vary from one frame to another) challenges to the fiction of a unitary self. These morphing representations of feminine embodiment during illness are crucial texts for feminist engagements with health as they draw from anxieties, norms and existing cultural and biomedical practices concerning everyday experiences of health and disease (Donovan, 2014, p. 239).
Contemporary studies of women’s autopathographics are cautionary, however, rather than celebratory, in their exploration of the form’s possibilities. Regulatory norms, imposed by mainstream cancer writing, seek to discipline not only women’s bodies but their articulation of an illness experience too. Speaking of the ‘narrative norms’ of survival in the American public sphere, Waples argues that this constitutes a ‘simplified’ version of embodiment (Waples, 2013/2014, p. 50). Here, the experience of illness is ‘reworked’ by the narrating subject such that her demands are generic as well as gendered and re-integration into society is not about reclaiming health but heteronormative femininity. Schultz similarly identifies the ‘triumphant’ and ‘intact’ re-emergence of the self in many cancer narratives that elide the ‘psychological work’ that is surely occasioned by illness (Schultz, 2009, p. 376). The triumphalist individualism of mainstream cancer culture seeks to erase the intersectional nature of women’s embodiment in cancer and its treatment and to universalise the subjectivity of the ‘survivor’. This universalising tendency in mainstream cancer culture also finds echoes in Bordo’s critique of post-modern culture and its celebration of the endless possibilities afforded by the representational fluidity of the self. A liberating focus on the textuality of the body ignores its material limits and consequences. Bordo instead instructs an ‘embodied point of view’ that challenges the ‘view from everywhere’, where attention to the ‘actual’ (the particular, lived experience of the body) replaces the fantasy of an endless ‘possibility’ of interpreting the body-as-text (Bordo, 1993, p. 39).
In their introduction to the Tulsa Studies in Women’s Literature special issue on written and visual breast cancer narratives, DeShazer and Helle draw attention to the significant differences in breast cancer narratives written since 2000 (DeShazer & Helle, 2013/2014, p. 8). These contemporary narratives, they argue, are interested in de-centring ‘survivor discourse’ and challenging mainstream cancer culture. Moreover, given the technological advancements in the screening and medical management of cancer, there are also several identities, subjectivities and embodiments in categories like ‘previvors’, ‘patients’ and ‘former patients’. Contemporary texts like Cancer Vixen also engage with the growing disparity in the age groups of women now being diagnosed and treated for cancer—the text’s appeal to younger women readers is evidence of newer concerns for the contemporary woman writer/artist. A third-wave feminist agenda, Waples argues, must necessarily include the diversity inherent in contemporary cancer culture because of the significant differences in women’s embodiment in the medical management of cancer across age groups. She demonstrates how women in their twenties and thirties are not typically ‘screened’ for cancer through mammograms and thus face more aggressive treatments and tend to be less responsive to medical intervention (Waples, 2014, p. 49). This ‘younger’ segment of female cancer patients thus face an entirely different disease than their older counterparts, making age a very important variable for feminist scholarship on illness and its treatment.
Contemporary feminist scholarship also considers the politics of location and its influence on forms of embodiment. For instance, DeShazer and Helle also draw attention to contemporary feminists’ focus on women’s varied access to diagnosis and treatment across geographies, cultural location and generations (DeShazer & Helle, 2013/2014, p. 10). This recent recognition of the diversity in the lived experience of illness in women is demonstrated through the variable register of depicting female embodiment in the autopathographics studied here. Cancer Vixen, Not Funny Ha-Ha and Tangles can thus be productively studied together precisely because of their diverse depictions of female embodiment in the course of illness experience and management. As 21st century accounts of women’s illness experiences, these texts instantiate the graphic (visual) embodiment of resistance to previous modes of theorising and narrating female embodiment.
I will demonstrate here that the texts under study instantiate new modes of embodying women’s experience of illness by (a) visualising and gendering difference in the experience of illness and its medical management and (b) ensuring heterogeneous cultural and representational visibility for the bodily practices of women both within and outside the medical management of illness. These new modes of female embodiment that challenge the traditional binary of normal/pathological in narrating the experience of illness will be explored here in three main sections. Section I, Corporeal Embeddedness and the Pathology of the Feminine, will explore how the writers of autopathographics visualise the always already embedded nature of the female body, its pathological adherence to social roles and appearance (by the patients and carers depicted in the narrative) and its pathologised deviation from the norm (by the family and the medical institution). I will argue in this section that the pathological feminine precedes the condition/diagnosis of illness. Section II, Visualising Rupture/Separation, will describe how illness experience and its medical management is gendered and argue that the female body is thus doubly pathologised. The writers of autopathographics instantiate the suffering female body as a liminal or continuously morphing one to demonstrate anxieties relating to the structurally unequal relationship that the gender female sign has with the binary of normal/pathological. Section III, Towards a Resistant Feminist Narrative, argues that women’s autopathographics refuse narrative closure or linearity and instead present the reader with an array of ‘raw data’ that intrudes on the telling and consuming of the visual–verbal articulation of an illness experience.
Corporeal Embeddedness and the Pathology of the Feminine
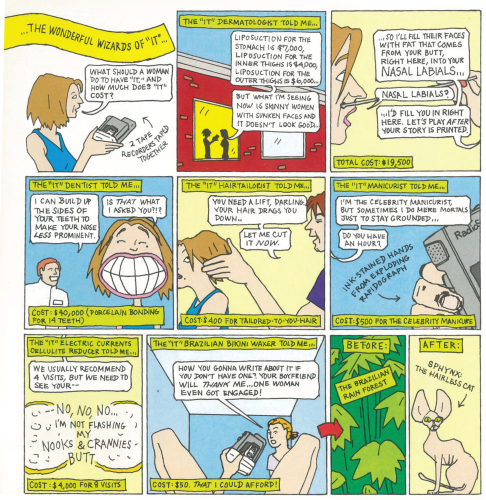
Each of the narratives studied here demonstrate that the female body is embedded in restrictive bodily practices within the family and immediate social milieu. Describing her life B.C. or ‘Before Cancer’ in August 2001, Marchetto tells us about the story she was working on for Talk magazine where how much being ‘it’ (‘it’ refers to the specific quotient that is needed or desired in the appearance of an elite New Yorker) costs. While she frames this story as being part of many superficial things she was caught up in, it nevertheless offers an insight into New York City life at the time (a state of affairs seen to be unchanging if not exacerbated even in the ‘present’ context of her breast cancer diagnosis and treatment). The ‘it’ story is about a range of body improvement practices seen as necessary for the elite female New Yorker and demonstrating her sincerity as a ‘reporter’, Marchetto immerses herself in the ‘it’ practices to write about them (see Figure 1).
Each panel of the ‘it’ story segment invites the reader to look at different parts of Marchetto’s body from the perspective of the various ‘it’ experts she’s visiting—dermatologist, dentist, hair tailorist, manicurist, cellulite-reducer, Brazilian bikini waxer and hair colourist. The female body under scrutiny is the focus here, although Marchetto eventually emerges from all these meetings having acquired ‘it’ because she’s covering the story. Calling these contemporary beauty ideals a ‘beast’ whose nature is to proscribe ‘flaws’ that require correction, Marchetto is sardonically drawing attention here to the obsessive scrutiny of the body’s surface appearance (she will eventually discover that what lurks within can be far more fatal). While Marchetto pathologises this cosmetic dismemberment of the body, she returns to the ‘it’ body later in the narrative to contrast the ‘reality’ of cancer with the ‘fiction’ of cosmetic perfection. When undergoing chemotherapy, Marchetto meets her doctor and nurse for dinner at Silvano’s restaurant, known to be populated with several ‘it’ girls. ‘This isn’t reality’ the nurse remarks while all of them stare at the thin waists in this panel’s foreground (Marchetto, 2007, p. 166). Interestingly, there is dismemberment here again, given that only the waists of these ‘it’ girls are visible to the reader. Marchetto, even while professing her past insecurity in the face of these ‘unreal’ bodies that parade in front of her husband, declares that cancer has now made her more secure. Citing her husband’s ‘choice’ of a woman with breast cancer over others who have been cosmetically altered to bear no relation to reality, Marchetto celebrates her security in being changed by illness. Thus, disease has here unified the body and made it ‘real’, challenging the dismemberment and superficial outcome of cosmetic alterations/enhancements.
The everyday practices that women aspire to in New York are pathologised yet again when Marchetto draws the women populating the lobby of The New Yorker’s offices (see Figure 2).

Marchetto is seen at the corner of the panel, looking on along with the reader, at very lanky stick figures in suits stepping into the elevator. ‘I felt like an alien and I liked it’, she says, setting up an immediate distinction between herself and these other women (Marchetto, 2007, p. 25). Marchetto subsequently meets Bob Mankoff, the cartoon editor at The New Yorker and the panel that depicts their meeting across a table is framed by a pile of Marchetto’s rejected cartoons that take up most of the table space. While Marchetto is dumbstruck by Bob’s review of her work, she lets us see what she was thinking at the time in a panel where a speech bubble reads ‘Look Bob, open your eyes, this is The New Yorker. I am drawing real New Yorkers’ (emphasis in the original) (Marchetto, 2007, p. 25). Marchetto thus believes that the lived practice of women’s bodies in New York is to be preternaturally thin and that this practice is sustained through a medico-cultural economy that sets standards while providing expertise.
At the start of Tangles, Leavitt visualises for the reader the corporeal demands of motherhood by likening her mother to Miss Clavel from the Madeline books (see Figure 3). Motherhood here is seen to be socially determined, as Leavitt first demands then comes to expect the comforting ritual of her mother tending to her anxieties at night.
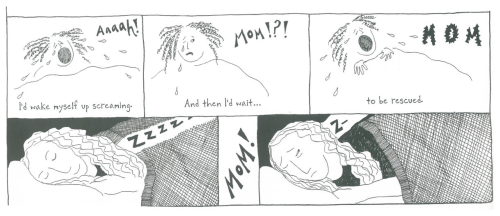
Young Leavitt, like Madeline in the books, confesses to having nightmares from which she expected to be ‘rescued’ by her mother every night through high school (Leavitt, 2012, p. 11). Miss Clavel, in the books, ran so fast down the hall that her ‘body got all stretched out’ (Leavitt, 2012, p. 11). Similarly, Leavitt narrates her mother’s embeddedness in a family unit of three sisters whose relationship is defined by ritualistic practices of care and its reciprocity. Recalling the time when her mother’s older sister Susannah’s husband died, Leavitt similarly depicts the physical toll exacted by care in a panel where her mother’s body stretches as she ‘ran’ to Sukie to ‘hold’ her and ‘cry’ with her and then ‘walked and walked’ with her (Leavitt, 2012, p. 14). At various points in the narrative, Leavitt emphasises the importance of ritualised practices of care that define a feminine role in the family unit—through a visualising of her own frequent phone calls, travelling to lend physical comfort and care (when her mother’s condition deteriorates, Sukey also visits frequently to care for her).
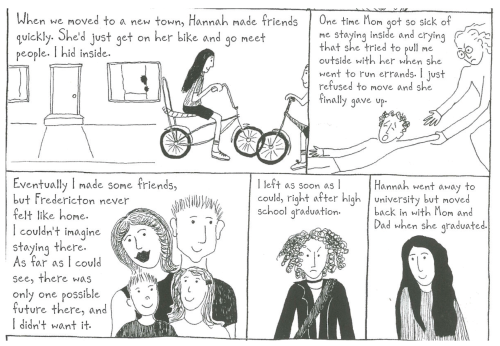
It is important to note here that we see Leavitt’s version of events in Tangles and thus view her mother’s body through her eyes—in this regard, this autopathograpic tells the story of a carer’s experience of illness as much as that of the patient (Leavitt’s mother, who is eventually diagnosed with Alzheimer’s). Leavitt’s visualising of the pathologised feminine thus explores the intersection of her own body with that of her mother’s. Tangles narrates the story of Sarah Leavitt’s discovery that she is a lesbian and her admission of the same to her parents. Thus, while reminiscing childhood memories and contextualising her mother’s corporeal embeddedness she simultaneously narrates her own alienation from life at Fredericton, where her family eventually settle. Consider Figure 4, for example, where Leavitt visualises her aversion to a conventional life narrative. The ‘possible future’ referred to in the panels in Figure 4 is the heteronormative family unit, which Leavitt sees as stifling and alienating. Speaking about how she and her sister were not a unit like her mother and her sisters, Leavitt describes how in her mind, ‘there was me and then the rest of my family, who I missed and felt liberated from at the same time’ (Leavitt, 2012, p. 15).
Leavitt thus pathologises the limits on possible ‘futures’ for the woman in the heteronormative family unit, choosing instead to leave home and rejects any notions of inherent filial cohesion. The studio portrait of a happy family visualised in Figure 4 is an instance of ritualised filial practices that work to confine modes of expressing gender and sexuality. As a member of this confining unit, Leavitt cannot wait to get away while simultaneously recognising her mother’s embeddedness in it—though the representative studio photograph in Figure 4 is fictional, her own visualising of her mother’s role in the family is similarly conventional. Consider, for example, Figure 5 as a contrast to the images of her mother’s body being ‘stretched’ through the physical toll of care seen in earlier illustrations.
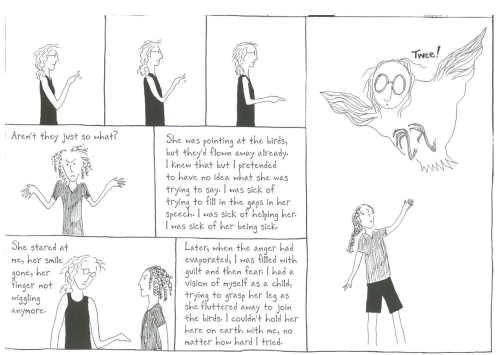
No longer able to recognise the filial demands on her body, Leavitt’s mother is now seen to morph into something other than human. Her body is now governed by ‘foreign’ laws and language that paradoxically release her from maternal duty. Leavitt’s ‘fear’ when she has a vision of her mother ‘flying away’ is from having to contend with an abandonment of routinised filial practices that determined her own identity as much as her mother’s.
Not Funny Ha-Ha similarly visualises the embedded reality of women’s bodies in a two-page spread that precedes the book’s narrative. These two pages are covered with drawings of oversized boxes of maxi-pads and tampons that float around in an empty space—the menstrual ‘cycle’ and its implications for reproductive potential is thus seen as an already present threat. The emphasis on reproductive potential also serves as a marker—fertility is here seen as the only acceptable marker of the feminine. The subsequent page depicts a couple, post-coitus, where the text in the woman’s speech bubble reads ‘… I think the condom broke’ (Hayes, 2015). The page following this (Leah Hayes book has no panels, it is rather akin to a sketch book where individual pages/sets of pages have a sketch/drawing accompanied by text or speech bubbles) depicts various reasons why a person may not be ‘in a place’ where it makes sense to have a baby.
Given that it is a ‘Handbook’, at this stage Hayes advises that when such an ‘accident’ occurs, one can pre-emptively take an ‘emergency contraceptive’ pill. She assures that the pill is generally effective and subsequently, there is a two-page spread with just the word ‘but’ pencilled in bold. She then says that if you act ‘later’ or when you ‘miss your period’ then abortion is the only option for preventing pregnancy. What is interesting here is that the word ‘but’ separates two possible situations that involve female embeddedness—the first situation seems ‘simpler’ in the sense that a pill is non-invasive and perhaps even ethically less complex than having an abortion after ‘discovering’ pregnancy in the second situation. However, Hayes is demonstrating here that both situations are virtually similar in requiring constant attention to and cognisance of the body’s boundaries being breached. In this case, as in the post-coital scene depicted earlier, medical intervention and monitoring the body is seen to be a ‘weight’ borne by the woman. Hayes too demonstrates that even in advance of finding out that you are pregnant when you do not want to be, women are already embedded in situations of high-risk. The emergency contraceptive pill is thus designed to ensure ‘safety’ in the case of an ‘accident’ but has a very stringent time-frame (typically 120 hours after the incident, although Hayes herself attests to how the sooner you take the pill, the greater its effectiveness). Hayes emphasises the culture of risk within which the woman’s body is situated, even in advance of an actual pregnancy and its medical termination. Graphic memoirs by women thus make visible and pathologise the body’s ‘weight’ even prior to the onset of illness.
Visualising Rupture/Separation
Writing about the importance of hair for the gender-female sign in her critical autobiographical essay on cancer, Schultz argues that having a full head of luxuriant hair has historically connoted femininity. Writing of instances where hairless female cancer patients were mistaken for men or even marked as ‘sick’ or ‘alien’ (even over male cancer patients in whom baldness is not necessarily always seen as a sign of cancer), Schultz argues that social responses to hairlessness can reveal a great deal about illness and its cultural encoding (Schultz, 2009, p. 373). Women’s autopathographics similarly question the binary of normal/pathological first by visualising the already pathologised sign of gender-female and second by making explicit, the socio-cultural norms that encode the ailing female body. Cancer Vixen details Marchetto’s chemotherapy sessions at St. Vincent’s Comprehensive Cancer Center or SVCCC as being personalised to her anxieties. When she first meets her oncologist Paula Klein, Marchetto tells her that she cannot afford to display any of the physical effects of cancer treatment, especially losing her hair, since she competes daily with the stringent norms of beauty embodied by the female customers that visit her husband’s restaurant. Her oncologist advises that she is suited to have a ‘light’ chemo because of being a stage-1, node-negative cancer patient—Marchetto thus doesn’t lose her hair during her cancer treatment. She even visits a hair colourist in advance of her chemotherapy sessions ‘on doctor’s orders’ as she says, thereby demonstrating the equal corporeal ramifications to identity that changes in appearance (and the regimen to keep up this appearance against a certain social ‘standard’) have for women cancer patients.
Marchetto discovers, however, that there are social norms that govern how ‘healthy’ one can appear while undergoing cancer treatment. At a fund-raiser for a book that details the basics of coping with cancer, Marchetto is shocked to discover that she stands out at an event that is attended mostly by cancer patients. Rather than finding comfort in a community of sufferers, Marchetto discovers that she is a target of hatred and anxiety as the only woman with hair. ‘But you still have your hair!’, one of the women at the party exclaim, before warning Marchetto that she is very likely facing recurrence with such a non-aggressive approach to treatment (Marchetto, 2007, p. 170). Here and at other points in the novel, Marchetto discovers that the norms of femininity are as changeable and alienating as medical protocol for the treatment of illness. More interestingly, however, Marchetto discovers that her insistence on retaining her feminine appearance is unique with respect to the larger socio-cultural narrative of battling cancer—the narrative of aggression, seriousness (she finds very few people willing to find humour in cancer), resilience and total victory of the self. Marchetto also genders the experience of illness in other crucial ways—her social identity as determinable by factors like financial stability, marriageability and status in an appearances-obsessed New York. She is seen to shrink back in horror for instance, when a passer-by on the streets mistakes her for a ‘bag lady’ or homeless person during her chemotherapy treatment and hands her some money (Marchetto, 2007, p. 180). Although Marchetto still has her hair when the passer-by offers her money, the panels make evident a difference in her demeanour with respect to others that throng the streets and department stores during Christmas season in New York.
By her own admission, Marchetto finds the shopping enjoyable but exhausting as she struggles with medical menopause during her chemotherapy. In addition, she struggles with the weight of her shopping bags as she can now no longer carry anything on her ‘surgery side’. Amidst a series of panels that depict the Christmas shoppers as blurry silhouettes in the background, Marchetto alone stands out as she sweats profusely, looks harassed by the weight of her shopping bags and eventually squats on the pavement surrounded by these, her hands covering her face. It is here, in a moment where she publicly succumbs to the physical and emotional weight of her illness and treatment, that she is mistaken for someone destitute. Her visible distress amidst a festive season results in misrecognition while simultaneously illustrating how she experiences constant surveillance. Even a brief lapse in appearance or an outwardly cheerful demeanour is thus pathologised in New York society. Marchetto later confesses to her embarrassment at being mistaken for someone destitute rather than for having her ‘real’ identity as a cancer patient found out. Her illness itself never faces a crisis of visibility. In contrast, her social roles—daughter, to-be wife, fashionista—appear to be fleeting unless they are constantly weighed down through a range of physical practices. These physical practices, whether they are external cosmetic interventions or the act of masking the pain of illness with the performance of cheer, are seen to require an immense expense of energy while also being discriminatory. Cancer Vixen repeatedly emphasises the range of normative ideals that constrain women rather than men and illustrates how these ideals are internalised and policed by New York’s elite. Marchetto similarly highlights the discriminatory mandates of medical science when she experiences her first mammogram. She visualises the hierarchical and discriminatory practices of diagnosing cancer that gender the subjects who are ‘screened’ (see Figure 6).
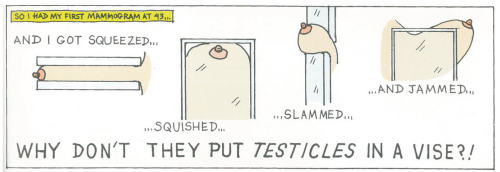
Marchetto is seen synecdochally in Figure 6 as a single breast that ‘got squeezed, squished, slammed and jammed’ (Marchetto, 2007, p. 85). This synecdochal breast represents the experience of all mammograms as cold, invasive and being akin to torture. Marchetto here stages a hierarchical relationship between the mammography machine (also seen as synedochal units performing an unfeeling and undiscriminating task) and the human subject it is probing. She signals to the paradoxical discrimination built into a seemingly unfeeling and unthinking device—it is designed specifically for a breast rather than to diagnose any high-risk portion of the body (like a testicle). The body is dismembered yet again by medical technology but is brought together in the experience of pain and a sense of injustice that Marchetto feels.
Tangles depicts the feminised embodiment of illness by focusing on the effects of Alzheimer’s on gender roles in the family. The disruption caused by illness in Tangles is most palpable in its effects on the heteronormative family unit, which is rendered increasingly unfamiliar. The contrast between Leavitt’s life in Montreal (symbolised by her discovery that she is a lesbian and her exposure to socio-cultural–economic inequalities) and that of her family’s in Fredericton is overturned by the illness. The home is thus no longer a place of confining heteronormativity but rather a liminal space that is continually rewritten by the demands of Alzheimer’s. In a section titled ‘Food’, Leavitt records her mother’s growing incapacity in the kitchen. Here, a series of panels depict Leavitt’s mother’s transformation from someone who provided the family with healthy food grown from seed to an Alzheimer’s patient who often doesn’t even feel hunger (Leavitt, 2012, p. 51). Leavitt’s mother’s stance in the first panel on the page is in striking contrast to the last, where she sits across from her husband smiling, presumably at mealtime, unmindful of an empty dining table. She is unable to cook or tend to the garden, where she, instead, begins to cause damage by her participation. A break-down in her social role of providing nurture automatically turns the home into a place of danger—‘Tools became weapons’ says Leavitt and to maintain stability, her mother is given a dull knife and a carrot so she could ‘help’ with the cooking (Leavitt, 2012, p. 51). The space of the home where domesticity is built around gender roles is thus threatened by change. Participation in the labour economy of the home is thus simulated here to ensure a continuing familiar role for her mother who is fast slipping from the visible signage of gender female.
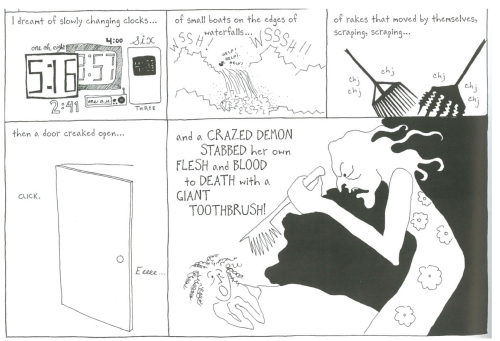
At various points in the narrative, Leavitt visualises the effect of her mother’s illness on the ability to perform/express one’s gender. Her mother’s declining abilities are seen as being most damaging to the family when they inhibit her identity/identification as a woman—she is unable to match her wardrobe to the season, she stops grooming her body, she starts give off bodily odours and is unable to discern them herself. For Leavitt, her mother’s transformation by illness is almost monstrous. In a section titled ‘Psycho Killer’, she describes how her mother stays awake one night and keeps the water running while she brushes her teeth so vigorously that the sounds reverberate through the house (see Figure 7). A series of panels in this section visualise Leavitt’s fear that night while she sleeps fitfully on account of the noises emanating from her mother’s room. In one of these panels she writes, ‘I could feel her restlessness, her sleeplessness, through the walls. The hair on my neck stood up every time I thought I heard her’ (Leavitt, 2012, p. 55). No longer cognisant of her motherly role, Leavitt’s mother now morphs into the very demons she saved her daughter from early in the narrative.
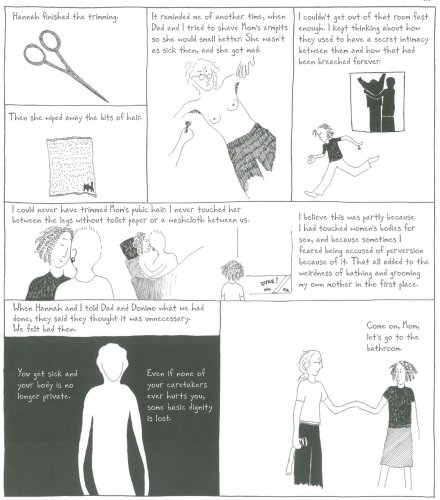
Most of the panels that depict her mother’s bodily transformation by illness are preceded by a brief visualising of past normalcy—grooming herself, caring for her children, being physically appealing to Leavitt’s father were elements of her mother’s everyday routine prior to her illness. Leavitt’s mother’s illness is thus coded through the social, where a fixed set of meanings produced through bodily practices have been ruptured. Her mother is monstrous now because she can no longer inhabit a gender feminine sign within the space of the home. As Alzheimer’s liberates Leavitt’s mother from a filially embedded identity, she becomes unrecognisable and occupies a liminal and monstrous space, unable to perform her role as woman, sexual partner (Leavitt witnesses how her mother often smells of sweat and faeces and imagines how this must affect her intimacy with and appeal to her father), mother and carer. While Marchetto demonstrates the instability brought on by cancer to the performance of femininity by making visible the effort involved in carrying on feminine bodily practices during her illness and its treatment, Leavitt recognises in Tangles the effect that a disappearing feminine identity has on personhood (see Figure 8).
Caretaking here becomes the socialising or re-socialising of the mother’s body—maintaining a feminised appearance, ensuring social and sexual appeal, re-articulating sexual taboos (Leavitt stops holding hands with her mother for fear of being mistaken as a sexual partner). In the panels visible in Figure 8, grooming the body is seen not as a choice but a necessity. To ‘smell better’ is to continue to be recognisable under a gendered sign—Leavitt mourns her mother’s slippage from being attractive to her father, possessing an element of ‘secrecy’ and ‘privacy’ as much as her declining abilities with the onset of illness.
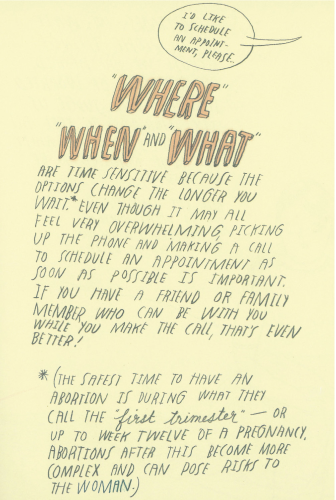
Not Funny Ha-Ha closes in on the particular, physical experience of pregnancy and its termination by emphasising the painful and emotionally gruelling nature of surgical and medical abortion. Illustrating the three most important things to consider, ‘where, when and what’, once the decision to terminate a pregnancy has been made, Hayes also emphasises their time sensitivity (see Figure 9). Hayes here makes visible the physical dangers involved in delaying the ‘decision’ to terminate pregnancy. Making a ‘choice’ here is seen to have corporeal limitations—the woman can only exercise agency about terminating pregnancy (with the surety of physical safety) within a very small window of physiological time.
Having made the timely decision moreover, Hayes demonstrates that achieving a medical or surgical abortion requires finances (both girls pay ‘up front’ before they consult their doctors at the abortion clinic and require several follow-up visits) and extensive support from friends and family (both procedures are physically debilitating and require some form of assistance). Just after taking the first round of her abortion-inducing pills, for instance, Mary is seen to be visibly distressed. On a page that frames Mary’s concerned friend standing outside a bathroom door, a speech bubble mimics retching sounds indicating the events transpiring inside. Subsequently, we see Mary’s hands holding up a paper she received from the clinic that details what she can expect during her medical abortion. This paper lists ‘cramping, nausea, vomiting, diarrhoea, heavy bleeding’ thus concretising all of Mary’s physical experiences, so far visualised only partially. The physical toll of the procedures is given more precedence in the narrative, demonstrating the inescapable corporeality of pregnancy and its termination whether one ‘chooses’ a medical or surgical procedure. All the autopathographics considered here thus visualise the corporeal violence of illness and its medical management on the woman’s body, concretising a rupture or separation in a simple binary of healthy/sick.
Towards a Resistant Feminist Narrative
I argue here that women’s autopathographics present a resistant feminist narrative in addition to gendering the experience of illness and its medical management. In various ways, these autopathographics resist narrative closure and linearity, to present instead, a catalogue of diverse narrative ‘potentials’. These narrative potentials take the form of raw data—like reproductions of photographs and hospital records in Cancer Vixen, excerpts from diary entries, letters and narrating failed alternate attempts at recording her mother’s illness in Tangles and deliberate omission of details like the events leading to pregnancy in Not Funny. Raw data indicate unprocessed information that has not been anchored by any one interpretation. It is available to the reader for use in any form while also testifying to the varied sources drawn on by the author. By narrative potentials I mean alternate possibilities that are hinted at but never explored while simultaneously offering sufficient details to the reader to destabilise any coherent picture of the details of illness and its medical management.
At various moments in Tangles, several kinds of narratives intrude upon the telling of a particular story. The most consistent example of this is excerpts from Leavitt’s mother’s letters and speech that are reproduced throughout the text. The letters and her mother’s speech become incoherent and difficult to decipher as her illness advances but also demonstrate her mother’s own attempts at narrating her experience. A half-page panel in a section titled ‘Waiting’ illustrates her mother’s attempts at cataloguing her headaches (see Figure 10). Leavitt herself has no knowledge of these headaches or even her mother’s attempts to keep track of them and she demonstrates an editorial distance from this narrative by drawing the headache journal in some detail.
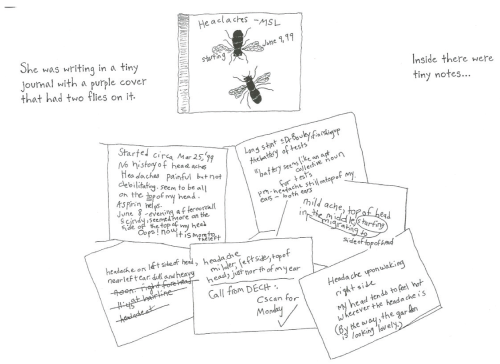
Her mother’s apt usage of ‘battery’ as a collective noun for a series of tests is thus preserved and Leavitt does not herself attempt to narrate the events described in the journal (Leavitt, 2012, p. 34). Tangles is narrated in an episodic format, where a set of events are illustrated in some detail and each event constitutes one individual ‘episode’. These episodes are always preceded and followed by interludes that depict a single scene, conversation, quote or song by Leavitt’s mother. The interludes are never explained or framed by commentary, even when they are exchanges that demonstrate very little narrative coherence. For example, consider the following ‘questions’ from an eponymously titled section: ‘Mom: Are you guys guy? So you don’t have to wonder about. Mom: Am I a stringle? Mom: Honey, can I open your voice?’ (Leavitt, 2012, p. 88). Leavitt makes explicit, the collaborative nature of framing a story by presenting her diverse source content unmediated to the reader. However, she demonstrates the unreliability and incompleteness of these sources as well.
Leavitt also provides excerpts for the reader from her own journal, where entries are juxtaposed concurrently with events—to indicate that they were being created at the time of actual events. These excerpts demonstrate the incompleteness of other source material visualised in the narrative but also threaten to destabilise the tone of the other episodic narrative of the text. For instance, in a section titled ‘Decision’, Leavitt’s diary entries form a much darker sub-text to the main theme of the section—the decision to institutionalise her mother when she was unable to walk anymore (see Figure 11). The ‘visible’ part of the entry reads, ‘I wish God would just let her die’ (Leavitt, 2012, p. 116). There is a caption above this entry that reads ‘Just like that. She never walked again’ (Leavitt, 2012, p. 116). While captions in the panels in Figure 11 report events as they occurred, the diary entry records ideas that are potentially subversive in their description of a ‘medical management’ plan.
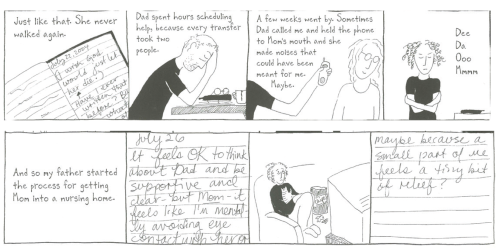
The diary entries thus provide a confessional sub-text of shame and guilt simultaneously with a set of captions that report facts and events—Leavitt records ‘avoiding eye contact’ with her mother and feeling ‘relief’ once she is institutionalised. Motherhood, daughterliness and care are interrogated here by visualising selfish, non-traditional responses alongside normative modes of grieving, empathy and guilt. Leavitt represents a resistant femininity by fashioning a daughter-self that would like to escape the burden of care and a mother-body turned monstrous by illness.
Like Tangles, Cancer Vixen also presents the reader with narrative odds and ends like prayer cards, pictures of saints (patron saints of cancer), reproduced photographs from Marchetto’s wedding, among other things. Marchetto’s resistant narrative is a denial of a linear origin story for her breast cancer diagnosis. In a two-page spread called the ‘Cancer Guessing Game’ that resembles any of several board games, Marchetto visualises the cyclical, repetitive and unstructured nature of making sense of a cancer diagnosis (Marchetto, 2007, pp. 34–35). The player is meant to start at the left-hand corner of this board game but his/her ‘movements’ on the abstract space of the board translate to re-visiting any of several known cancer-causing ‘acts’ that may have led to developing the disease. ‘Movement’ in the game’s logic is an unstoppable one, since every panel in this ‘game board’ directs you to a different panel/cause for cancer, thereby permanently deferring any one source of illness. Moreover, Cancer Vixen also demonstrates the ‘work’ performed by the cartoonist in generating a great volume of information while telling a story. For instance, Marchetto interestingly visualises for the viewer the process involved in ‘visual reportage’ in Cancer Vixen (see Figure 12).
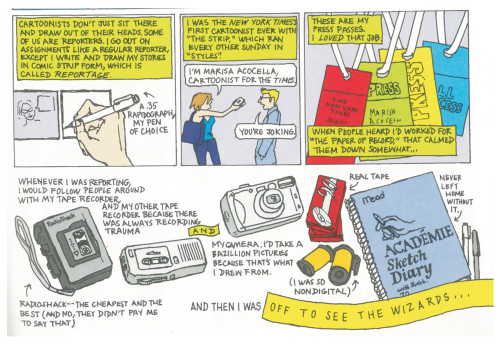
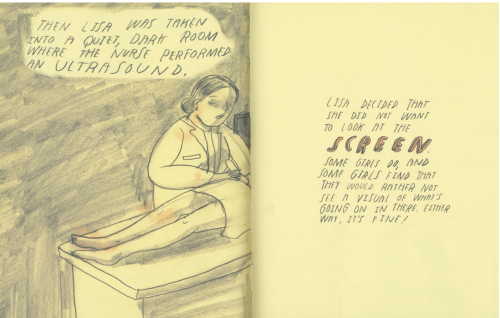
Figure 12 depicts various ‘recording’ gadgets that enable Marchetto to take ‘bazillion’ pictures and record everything people say. She emphasises here the volume of unprocessed data that she must edit for consumption. Marchetto is also drawing attention here to the ‘success’ of certain stories as opposed to others, given that readers only have access to the cartoons that newspaper editors agree to publish. For example, the page adjacent to her depiction of a cartoonists’ process illustrates her apartment before she meets her fiancé, prior to being diagnosed with cancer. Portraying a ‘typical’ cartoonist’s living room, Marchetto draws on one corner, ‘boxes and boxes and boxes and boxes of rejected cartoons’—a pile of rejected stories that she nonetheless preserves (Marchetto, 2007, p. 16). Marchetto thus draws attention to the vulnerable lives of stories in the public domain/media, where authors and readers have no control over the production and consumption of a particular narrative. Hayes’ Not Funny subtitled a ‘hand-book for something hard’ emphasises the unique feminine corporeality of medical and surgical abortion. Hayes refuses to narrate the ‘moment of’ or the ‘story behind’ the pregnancy itself, instead choosing to visualise how the decision or ‘choice’ to abort is both physically and emotionally that of the woman. The narrative demonstrates the particularity of shame/guilt with respect to women since the procedure of surgical abortion still involves an ultrasound, thereby necessitating the choice of ‘seeing’ or ‘not seeing’ the foetus (see Figure 13).
Some girls would ‘rather not’ see a visual of what is going on inside their womb, Hayes writes in the page adjoining the image of Lisa’s ultrasound procedure. In occluding the image/data from Lisa’s ultrasound, while acknowledging its presence in some form and space, Hayes draws attention to the intrusion by ‘potential narratives’ in a story that aims to be about ‘any’ woman undergoing abortion. The ultrasound forces a ‘particularity’ on Lisa and her foetus that Hayes rejects through narrative occlusion and by demonstrating the possibility that one may simply choose not to ‘see’ a medically aided imaging of the womb. Interestingly, Hayes also frequently warns the reader that Not Funny is only a ‘book’ which is to be therefore treated as such—one of an array of equally reliable or unreliable sources of medical advisory about abortion. A disavowal of the book’s singularity in offering information and advisory about abortion testifies to a resistance in claiming only one narrative possibility in illness experience and its medical management.
Conclusion
In a section titled ‘Why this Book?’ at the end of Not Funny Ha-Ha, Hayes highlights, very significantly, her interest in offering a ‘visual insight’ into the often-unseen physical process of experiencing medical/surgical abortion. This ‘visual insight’, I have argued in this paper, is what constitutes a resistant femininity in the autopathographics studied here. Women writers narrating the experience and management of illness in graphic form thus make visible the confining norms of femininity that pathologise the body even before the onset of illness. They expose the structural inequality of the female body with the binary healthy/sick by making visible a monstrous, liminal feminine that defies traditional responses to the ailing body.
Autopathographics by women, this paper has argued, make explicit the discriminatory and normative practices within which the female body is embedded, both prior to and during the experience and treatment of illness. While autopathographics have been studied for their suitability in exploring the myriad transformations of self during the experience and treatment of illness, this paper argues that women writers also harness the form’s potential for expressing a resistant femininity. This ‘resistance’ is towards being subsumed under universalising norms of mainstream modes of narrating illness that are inattentive to gendered modes of making sense of the ailing body. These mainstream cultures of narrating stories of illness valorise the survivor, assume equal access to treatment and screening technologies and present a unified self that emerges intact at the end of a linear progression from diagnosis to cure. The graphic illness narratives studied here instead make visible, the impossibility of narrating a linear story of diagnosis and cure. The graphic form is utilised here to instantiate the perpetually morphing female body that is at odds with the discourses of medicine, beauty and domesticity that proscribe modes of femininity. Illness and its medical management alone do not mark an invasion/interruption of the norm. Rather, the necessity to adhere to routinised practices that mark the body as inhabiting the gender female sign is visualised in these narratives as pathological.
Cancer Vixen, Tangles and Not Funny visualise the contexts within which their ailing female protagonists are embedded thereby making explicit the cultures of physical surveillance that define them. Within these cultures of surveillance, illness is seen to reveal a liminality that cannot be addressed by a linear narration of progress towards a cure. Marchetto’s cancer not only threatens to recur but has made her aware of the large percentage of women who did not survive from being uninsured. Leavitt’s mother in Tangles doesn’t survive her Alzheimer’s and is also unable to inhabit the space of the home once she ceases to identify and express as gender female. Hayes’ protagonists’ choice to terminate a pregnancy is seen to exist amidst a culture of criticism, shame and a severe lack of information and support. The graphic form enables these women writers to present the reader with ‘narrative potentials’ as an alternative to the mainstream story of ‘surviving’ an illness. These narrative potentials constitute graphic evidence of the many sources the writers draw upon, presented as unintegrated and unedited intrusions on a story that make explicit its tenuous unity. The graphic embodiments of ailing women in these texts, like the untold stories that form a visible source of the narrative, interrogate the complicated intersection between illness, its medical management and the lived practice of femininity.