
Abstract
For the first time since Independence, India’s urban population has registered a higher increase than the rural population. Increasing urbanbiased economic activity and job creation are leading to rapid urbanisation, and a greater number of poor people today are living in cities and towns in India. Slums, often the residence of migrants and urban poor, are underserved areas with poor housing, insufficient living space, basic infrastructure and services such as clean drinking water, drainage and electricity, and poor access to toilets and sanitation services. Urban poverty and life in slums significantly compromise the ability of women and girls to effectively manage menstruation. There are many factors that affect how women manage their monthly period, such as the lack of information and awareness on menstruation, unaffordability of menstrual products, poor access to water, sanitation and hygiene infrastructure and services, lack of privacy, safety and security. This article seeks to highlight the challenges faced in managing menstruation in the context of a slum/poor urban settlement and the need for a convergent and comprehensive approach involving key stakeholders including communities, civil society and government departments to ensure gender-sensitive, menstrual hygiene management-centric interventions.
Setting the Context—Urban Slums in India
I recently moved to Delhi from my village after marriage. Life here is very different from my home. My husband works as a labourer, and to supplement our income, I also have to work as a domestic help. Most of what we earn is spent on living expenses here in Delhi. We are also expected to send money back home. We live in a small room, getting water is difficult, community toilets are far away from the room and there are no spaces to go in the open.
This, in essence, describes the challenges of urban poor communities living in slums in Indian cities.
For the first time since Independence, India’s urban population has registered a higher increase than the rural population. The 2011 Census indicates a population increase of 90.99 million from 2001, representing a 31.8 per cent increase in the urban population. Estimates presented in the India Urban Poverty Report (Ministry of Housing and Urban Poverty Alleviation, 2009) indicate that by 2030, 41 per cent of India’s population would be living in urban areas. The National Sample Survey (65th round, Ministry of Statistics and Program Implementation, 2008–2009) also reports that over 80 million poor people live in cities and towns in India. Increasing urban-biased economic activity and job creation is leading to rapid urbanisation, and a greater number of poor people are living in cities and towns in India.
Slums, where the urban poor reside, are often the first destination for rural–urban migrants. Most persons living in slums are involved in informal and insecure occupations. Their access to various social benefits, government entitlements and financial security is constrained due to lack of information, agency and voice. The 2011 Census reports state that more than 65 million people live in slums in India, with housing unfit for humans, inadequate basic sanitation and without access to clean drinking water. In addition to the challenge of limited housing and basic public services, such as water, drainage and electricity, poor access to toilets and sanitation services make living conditions unhygienic and insanitary.
Women are often the worst affected by various dimensions of urban poverty and they have to balance their roles as contributors to the household income with their household responsibilities. The gender division of labour puts women in charge of ensuring the well-being, health and hygiene of their family. The burden that accompanies this responsibility is much heavier in communities without access to clean, safe water and toilets. Women and girls have to negotiate challenges to privacy, safety and security on a daily basis. A combination of the above factors, coupled with lower levels of support structures in urban areas (as compared to rural households) affect the role and quality of life of women and girls in urban slums.
MHM in Urban Contexts in India— A Brief Review of Literature
While several studies on menstrual hygiene management (MHM) have been undertaken in urban contexts in India, including in slums, most have focused on analysing age at menarche, knowledge of menstruation and menstrual hygiene practices (Dubey & Sharma, 2012; Rajagopal & Mathur, 2017) and are centred on adolescent girls as the respondent group. Nearly all studies assessed menstrual hygiene using one or more of the following factors—use and maintenance of menstrual products, bathing practices during menstruation, handwashing and cleaning of genitalia.
Cross-sectional studies undertaken in slums in Kolkata (West Bengal) and Bilaspur (Chhattisgarh) and a resettlement colony in Delhi assessed knowledge, perceptions of menstruation and menstrual hygiene practices among school and out-of-school adolescent girls (Bhattacharyya, Sen, Hazra, Sinha, & Sahoo, 2015; Jitpure, 2016; Sharma, Mehra, Kohli, & Singh, 2017). These studies highlight poor knowledge of menstruation, especially prior to menarche, the practice of several restrictions during menstruation, poor menstrual hygiene practices and associated morbidities. Significant use of sanitary napkins among adolescent girls was reported in all three studies (81% in Kolkata, 79% in Bilaspur and 63% in Delhi). The studies in Delhi and Bilaspur reported regular bathing, handwashing and cleaning of genitalia by adolescent girls during menstruation; however, a significant proportion continues to wash hands and genitalia without soap. The study in Kolkata showed that the prevalence of symptomatic leucorrhoea and vaginal itch/burning was significantly less among sanitary pad users. Studies undertaken among adolescent school girls (not necessarily in slums) in Kolkata (West Bengal), Bangalore (Karnataka) and Hyderabad (Telangana) and among out-of-school urban adolescent girls in Gandhinagar (Gujarat) also highlight similar issues (Ramachandra, Gilyaru, Eregowda, & Yathiraja, 2016; Prajapati & Patel, 2015; Sreedhar & Syed, 2014; Yasmin, Manna, Mallik, Ahmed, & Paria, 2013).
Comparative studies between urban and rural adolescent girls in Bareilly (Uttar Pradesh), Nagpur (Maharashtra) and Jaipur (Rajasthan) indicate a significantly higher usage of sanitary pads among urban adolescent girls compared to those living in rural areas (Dubey & Sharma, 2012; Kumar, Gupta, Danish, & Nipun, 2016; Patel & Kubde, 2014). Knowledge and awareness of adolescent girls in urban contexts was also reported to be higher than in rural contexts in the three studies. It is suggested that higher awareness levels in urban contexts could be due to higher socio-economic status and literacy of mothers. However, the need for more information and awareness among both adolescent girls and their mothers (who are the primary source of information), both in urban and rural contexts is indicated. Some of these studies, such as the one in Bilaspur (Jitpure, 2016) and slums in Kolkata also report high levels of gynaecological morbidity including menstrual disorders such as oligomenorrhoea, polymenorrhoea, dysmenorrhoea, irregular periods and leucorrhoea. Other associated morbidities including back and joint pains, fatigue, abdominal pain and bloating are also reported (Bhattacharyya et al., 2015).
Thus, most of the studies conducted so far focus on quantitative estimates of awareness, menstrual hygiene practices and morbidities. Mahon and Fernandes (2010) and Rajagopal and Mathur (2017) highlight the challenges faced by girls and women in managing menstruation—such as unsupportive environments, access to and use of products and unmet water, sanitation and hygiene (WASH) and health needs. The interlinkages of these factors often determine how women and girls manage menstruation and ensure hygiene. This article builds on the available body of literature to elicit the issues and challenges faced by menstruating women and girls living in urban slums while highlighting the interlinkages between these different factors. Urban slums present several challenges to women and girls—from the burdens of urban poverty to lack of familial support, lack of privacy, unsafe environments and vulnerability, poor infrastructure and services, poor health and sanitation, poor awareness and behaviours on menstruation and hygiene, all of which impact the ability of women and girls to effectively manage menstruation. Given the increase in rural–urban migration, the poor living and sanitation conditions in slum areas and the current policy focus on WASH (including WASH for MHM), this is an opportune time to understand the challenges faced by women and girls and enable gender-sensitive policy and programme interventions that address their sanitation and hygiene needs.
Research Methods and Study Locations
This article is based on three studies undertaken in Jaipur and Delhi between 2015 and 2017. The studies focused primarily on (a) assessing a community-based intervention in urban sanitation in Jaipur and Delhi (Rajagopal, Mathur, & Chakravarthy, 2017), (b) assessing the impact of menstrual hygiene interventions in Jaipur (Rajagopal, Mathur, & Sharma, 2016) and (c) analysing the awareness, perceptions and practices of adolescent girls on sexual and reproductive health (Joshi, 2015).
Each of these studies used primarily qualitative methods—focus group discussions (FGDs) and in-depth interviews—to understand perceptions on menstruation and challenges in MHM faced by women in the reproductive age (20–49 years) and adolescent girls (10–19 years). In addition to these studies, the authors also undertook FGDs on MHM in the same study locations in the early months of 2018, findings of which are also presented in this article.
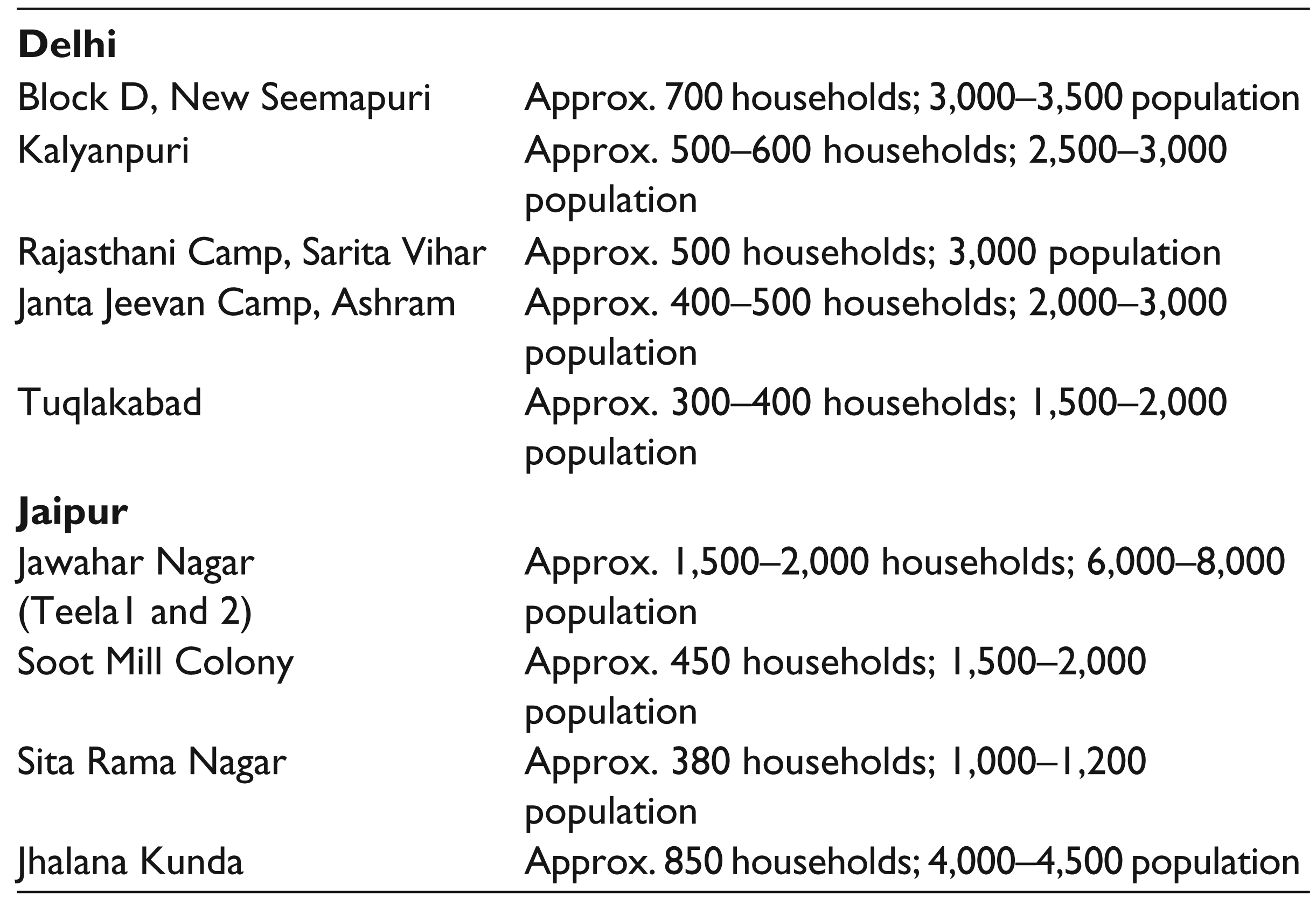
A total of 45 FGDs—35 with adolescent girls and 10 with women—was undertaken in five slum areas in Delhi and four in Jaipur. Table 1 provides the names of each of the locations, along with the approximate number of households and population, as reported by the women and girls. A total of 20 in-depth interviews was undertaken with representatives of local NGOs and government officials from the Delhi Jal Board (DJB), Delhi Urban Shelter Improvement Board (DUSIB), Municipal Corporation of Delhi (MCD) and Jaipur Municipal Corporation and members of Mahila Arogya Samiti 2 in Jaipur.
This article is divided into three sections. Section I provides an overview of the study locations, the socio-economic profile of households, existing infrastructure and WASH services. Section II outlines the challenges that women and girls face in managing menstruation and menstrual hygiene, given the contexts in these locations; Section III presents the conclusion and suggests some recommendations for policy and practice.
Study Locations
Overview of the Study Locations
The study locations mentioned above were spread across different parts of the cities of Delhi and Jaipur.
Socio-economic Profile
In Delhi, nearly all residents in the slums were migrants from other states (Uttar Pradesh, Bihar, Odisha, Rajasthan, West Bengal), who had either moved to the city recently or had been living in these locations for generations. In Jaipur, as well, slums had migrants from other districts in Rajasthan and from other states. Men and women were reported to be engaged as labourers, vegetable vendors, taxi drivers, auto rickshaw drivers, shop assistants, etc. The women were mostly engaged as domestic workers. The average household income reported during FGDs with women and girls ranged from ₹2,000 to 20,000 per month.
Housing
In all locations in Delhi and Jaipur, most housing was ‘pucca’ (proper brick structures); only 5–10% households across all locations were ‘kutcha’ as reported by the respondents. Observations indicate that the houses were often single rooms, which were 10 x 10 feet in size. Each household consisted of between two and six members. The same room was used as the sleeping area at night and as the kitchen and bathing area in the day. In all the locations, houses were built close to one another with narrow lanes, barely 5–6 feet in width, separating two rows of houses.
WASH Infrastructure and Services
A brief overview of the WASH infrastructure and services in these slums, as reported by residents is as follows.
Few households in slums across Delhi and Jaipur had access to individual toilets, owing to space, infrastructure and financial constraints. In Delhi, Community Toilet Complexes (CTCs) constructed by the DUSIB were available in all the locations investigated. In locations with a large population and sufficient space, such as Rajasthani camp, two CTCs have been constructed. In Jaipur, public toilets (PTs) have been constructed by the Jaipur Municipal Corporation over the last two years in various localities. In Delhi, CTCs charged a user fee of ₹1 for a woman and ₹2 for a man, and ₹5 for bathing. Users also had the option of making a monthly pass for the entire family. Government officials mentioned that despite the existence of CTCs, people continue to defecate in the open. Even in households with individual toilets, the habit of open defecation had not stopped, owing to the excessive cost of desludging septic tanks.
Shallow storm water drains run through each lane in the slums. Even though designed only for passage of rain water, all household liquid waste is discharged into these drains. In most locations, solid waste is also dumped in these drains. Consequently, dirty water from the drains often overflows into the lanes. According to the women and girls, this situation worsens during the monsoons. Cleaning of these drains by the civic authorities was also reported to be irregular. In several households that have constructed individual toilets, the septic tank is connected to the storm water drain to avoid costs of desludging. In such cases, faecal waste is discharged into an open drainage system. Households in D Block, Seemapuri in Delhi complained of the unpleasant odour. ‘At times, we are even unable to eat our food; and just the feeling of being close to a drain that has faecal waste [in it] is nauseating’ (Maya Devi, 42 years, Seemapuri, Delhi, May 2017).
Poor systems for solid waste management were reported by respondents. They said that there are designated spots for dumping waste in each slum, where all households throw their daily waste. In certain locations like Seemapuri, this dump had not been cleared for months. Respondents in South Delhi reported better systems of waste management. Large dustbins had been placed in each of the slums, which were cleared every two days by sanitary workers. Public dustbins were also reported in slums in Jaipur. In locations such as Rajasthani Camp (Delhi) and Soot Mill colony (Jaipur), NGOs are piloting community-managed household waste collection initiatives.
Women and girls reported access to water primarily through water tankers supplied by the municipal authorities. The frequency of supply through these tankers varied across locations. In locations where communities had a better rapport with the local authorities, the supply was more regular. On arrival of the tankers, women and girls line up to collect water in vessels. They reported spending between 0.5 and 2 hours for water collection every day. Several households had also set up boring systems to extract ground water (though not legal), as water collected from tankers was insufficient to meet household needs. Being saline, ground water was reportedly used only for bathing, handwashing, cleaning and other domestic purposes. Municipal water was used for cooking and drinking. Households that do not have boring systems buy ground water from neighbours for a fixed monthly fee. Very few households have piped water connection points within their houses.
External Environment
Women and girls in several slums reported fights, violence and sexual harassment in their communities. They said that it is often unsafe for women and girls to go to certain parts of the slum or to go out late in the evenings or at night.
Menstrual Hygiene Management: Issues and Challenges
Perceptions and Attitudes towards Menstruation
In nearly all FGDs, adolescent girls reported being unprepared for menarche. Fear and panic were the dominant reactions reported by many of them at the time of their first period.
I started menstruating in school. I was apprehensive and too scared to talk about it to anyone in my class. I was silent throughout the day. I went home from school and told my mother about it. She told me to use a pad and did not give any explanation. She just said that I will bleed every month.
While mothers were reported as being primary sources of information, this information was limited to explaining the use of cloth or a napkin to absorb menstrual blood. Interactions with women revealed that mothers were highly hesitant to provide information prior to menarche. They also felt that after menarche, it is important for girls to be modest and restrict their movements.
In our villages, our mothers did not tell us much about menstruation before menarche, and we don’t tell our girls either. But girls have access to TV, so they know. After menarche, we also tell them to behave properly, not go out late in the evenings and not to engage with boys. But many of these girls do not listen to us.
In the absence of significant or accurate information from their mothers, girls turn to friends and peers to seek information and talk about issues they face during menstruation. An NGO representative said that this exchange is often misinformed and leads to the perpetuation of several myths and taboos.
Interactions with the women and girls revealed that most of them understood menstruation as the expulsion of ‘dirty blood’ (ganda khoon) from the body. This deeply ingrained notion was associated with the perception of menstruation as impure and consequently, with the need to follow several restrictions. Women mentioned that in the village, they followed several restrictions during menstruation. They were not allowed to cook, did not interact with other members of the household, lived away from the house, etc. However, given the lack of space in urban slums, it was not always possible to observe these taboos.
In villages we used be isolated [during our period], but in urban locations, that is not possible—we have no space. And if we women don’t cook, how would people in the household eat? So we only follow what [restrictions] we can.
Women and girls observed a few restrictions that were feasible, such as not praying and participating in religious activities, not touching specific foods, such as pickles, not eating hot and spicy food and not washing their hair for the first three days of their period. Adolescent girls also felt that it was often difficult to talk about issues of menstruation at home and in schools. During an FGD with girls in Jawahar Nagar, one of the oldest slums in Jaipur city, the girls admitted that they could not talk openly about menstruation at home especially when male members were around (‘Gharwalon ke samne baat nahin karsakte; sharam ati hai’ Asha, 18 years, January 2018). Nor could they talk easily with other adults: One of the girls from Jaipur said that when she approached her teacher to discuss this issue, the teacher told her to go home and speak to her mother.
Thus, as highlighted in several studies, the culture of silence around menstruation was prevalent, and much of the information given to adolescent girls focused mainly on the need to restrict their movements and modify their behaviour (Rajagopal & Mathur, 2017). Apart from the relaxation of certain restrictions during menstruation due to practical considerations, living in urban locations and close to cities has not had much impact on social norms and practices around menstruation, except in areas where NGOs/local organisations were working with women and girls. For example, staff from the local NGO in Rajasthani Camp in Delhi said that initially both girls and women were very shy and hesitant to talk about menstruation. Constant engagement and persuasion on the part of the field staff was needed to break the silence and enable women and girls to open up and discuss the issue freely.
Access and Use of Menstrual Products
Nearly all adolescent girls, across slums in Delhi and Jaipur were reported to be using sanitary napkins to manage menstruation. In Jaipur, school-going adolescent girls reported higher pad usage, as compared to out-of-school girls. In both Delhi and Jaipur, mixed use of sanitary napkins and cloth was reported by girls in nearly all group discussions. While girls felt that ‘sanitary napkins’ were the ideal menstrual product, mixed use was reported as a practice to overcome financial constraints and the inability to purchase more than one packet of pads a month. In comparison with Jaipur, a greater number of women in Delhi and especially working women reported using sanitary napkins. Women from Janta Jeevan Camp, South Delhi said, ‘When we were in the village, we didn’t know much, and used cloth. However, here we use only pads, we now realise how unhygienic it is to use cloth’. In Delhi, adolescent girls encouraged the use of sanitary napkins among other women in their family. ‘We constantly used to tell our mothers to use pads as they are so much more convenient; initially they did not listen, however, once they started using it and saw the benefits, they became regular users’.
The interactions with women and girls made evident that four key aspects influenced product choice and usage:
Awareness of different menstrual products and their safe use: For instance, in one of the slums in Delhi, a local NGO trained women to make and use cloth napkins as a cheaper and more environmentally sustainable option. In this location, the NGO coordinator reported a greater uptake of cloth pads. According to her,
Before we did this training, most women and girls were using commercial napkins and old cloth. Napkins were often difficult to afford, and their disposal was a concern. We thus introduced this training, which has been a success, with several women having switched to manufacturing and using their own pads. Prior to this training, women were unaware that cloth could be made into easy to use and absorbent napkins. The NGO coordinator also added that awareness among women and girls using various products, such as different kinds of commercial pads and cloth pads, was very limited and that this restricted the type of products they use and how they use them. Availability of the products: Adolescent girls from Rajasthani Camp and Janta Jeevan Camp in Delhi mentioned that they attended a workshop, supported by the local NGO, where they were told about various kinds of menstrual products. While they were keen to use some of the products they had learnt about, these were not readily available and had to be ordered online, which was not a feasible option for them.
We would like to use some of the products that we saw and learnt about in the workshop; but they are not available here. We only end up using the local pads that can be bought easily from the market and are not very expensive. (Pinky, 16 years and Seema, 12 years; Delhi, May 2017) In Rajasthani Camp in Delhi, a local NGO began an intervention to introduce a cheaper, disposable sanitary napkin; however, assuring a regular supply was a challenge. Girls in Jaipur city who had received sanitary napkins in schools under the UDAAN scheme stated that the distribution was irregular. Affordability of products: Most women and girls mentioned that one packet of pads costing ₹30–35 was all they could afford to spend per month. While girls aspired to use various products, the lack of household financial resources was a concern. ‘I see those pads with wings and fragrance on the TV; I wish to use them; but my father is a rickshaw puller and mother a house maid, we cannot spend ₹100 on buying pads each month’ (Rani, 14 years, Rajasthani Camp, Delhi). Access to WASH infrastructure: Access to toilets, a regular supply of water and safe disposal facilities determined product usage (duration of use and disposal) and the ability of girls and women to manage their menstruation hygienically. This is further explained in the next section.
WASH Infrastructure and Services
Inadequate access to WASH infrastructure and services, and their poor quality, is one of the biggest challenges faced by women and girls in effectively managing menstruation and ensuring menstrual hygiene.
Access to Toilets
Access to toilets was one of the most critical challenges outlined by women and girls. As mentioned above, very few households in the locations studied have individual toilets. Women and girls use primarily CTCs/ PTs or they defecate in the open. There were several challenges associated with the use of CTCs/PTs. Except in a few locations, where authorities had found land for CTCs/PTs inside the slum, they are normally located on the boundaries of slums or at any location within a 1–2 km radius. In Seemapuri (Delhi), the CTC was located outside the slum on the main road, which was nearly a 1–1.5-km walking distance from households located in the last few lanes of the slum. Similarly, in Jaipur, PTs have been built on the main road. In addition to the distance from their households, the location of these toilet complexes on the main road was problematic for women and girls. They said that they were hesitant to go to the toilet that was on the main road, as everyone could see them and that there was no privacy. Further, they ran a risk of being sexually harassed by boys riding bikes near the main road.
The toilets are very far from our house. We have to walk quite a distance. They are also located right on the main road. How can we comfortably go there, when everyone on the road, in cars, etc. can see us go in and out? When we are menstruating, we have to hide and carry our pads with us as well. The distance and location make this difficult.
Factors like location and distance also present safety concerns for women and girls going to the toilets, particularly in the evenings.
There are always boys near the main roads, and the toilets are far. If our wives and daughters have to go the toilets, we have to accompany them. There is always a concern about their safety.
Thus, visits to the CTCs/PTs often have to be carefully planned, as it involves significant time, distance and security concerns. Women and girls thus tend to go to these toilet complexes just once or twice a day, for example, when they have to bathe or visit the market. For women with disabilities, elderly and pregnant women, the challenges are even greater.
In Delhi, there is a fee for using the CTC. One of the women pointed out that for a family of five, if each of them were to bathe once a day, it would cost ₹25; and it would cost an additional ₹8 if each of them were to use the toilet once a day. This was a cost too high for the family to pay. They thus, found ways of rationalising the costs and bathed in turns during the week or the women took turns to bathe inside the room once the men went to work. The woman also said that they would not be able to afford the cost of using the toilet several times a day during their period.
CTCs/PTs are often managed by caretakers and tend to be open only during the day. Women and girls in all locations said that toilet complexes followed fixed timings—mostly between 6 am and 10 pm. This limits access to toilets to the daytime, forcing women and girls to resort to open defecation at night. On normal days, women and girls said that they manage to avoid defecation in the night; if they had to relieve themselves, their only option was to go out somewhere close to the house. It is particularly difficult during menstruation, especially if they have to change their pads.
Here the toilets close at 10 pm. If we need to go after that we go close by. When menstruating, this is difficult, as it takes more time to change our sanitary napkins; and doing it in the open, we are often afraid that someone may see us; it is also unsafe. We usually avoid defecating and changing at night. Instead we do it in the evening and then in the morning.
Maintenance of CTCs/PTs is also a factor that inhibits their use. Girls from all locations said that the toilets are always wet, making them difficult and unpleasant to use; also, there are no dustbins to dispose of the menstrual waste, forcing girls to throw used sanitary napkins in the toilet complex.
Initially, there were no dustbins here in the toilet. We used to just throw the pads in the toilet and come away. The toilets were also always wet; we were constantly worried that we would soil our clothes, and when menstruating, wet clothes make us even more uncomfortable. After the intervention of a local NGO, we realised that we too have a role in the maintenance of the toilets. All of us got together and put old cardboard boxes in all the toilets lined with newspaper for the proper disposal of used menstrual pads.
In Jaipur, women added that toilets were not cleaned regularly and that there was no water connection. Kulkarni, Reilly and Bhat (2017) in their study of sanitation access of poor women in Jaipur city note that out of four slums covered, the PT in only one slum was found to be clean and usable .Similar issues were also reported by girls in schools: Poor maintenance of school toilets prevented them from using the toilets, especially during menstruation.
Collection and disposal of used menstrual pads strewn around toilets was a concern highlighted by one of the CTC caretakers in Delhi. He said that it often took significant persuasion and extra payment to get the cleaning staff to clear the pads. He felt that it was important for the community to accept ownership in ensuring maintenance of the CTCs.
They just throw the pads and go, it is so difficult and disgusting to pick up the sanitary napkins and clean the toilets. We have to pay the cleaning staff more money for this. Already we don’t make enough money, this adds to the problems.
Women and girls also mentioned that it would be good if there were hooks/places within the toilets where they could hang their bags/clothes. Especially during menstruation, they said they have to carry bags in which they can keep their pads. Changing the pad, while managing their clothes and an additional bag was a challenge.
Violence in and around CTCs/PTs was an issue mentioned by all stakeholders—women, girls, men, CTC caretakers and government officials. CTC care takers said that there are often efforts to steal the daily collections, or taps and pipes installed in the CTCs, leading to conflict and violence. This was also confirmed by DUSIB officials. For women and girls, this had implications for them in terms of usage. In Seemapuri, one of the women said that if she went to the community toilet when there was an ongoing fight, she would have to leave the place immediately and find another place to use. This was especially difficult when she is menstruating. Thus, despite having CTCs/PTs, their usage is circumscribed by various factors.
The alternative to toilets—open defecation—also poses several challenges.
Unlike in villages, open defecation in urban areas is very difficult. Slums are highly populated and located within the city, and often lack open spaces. There are only one or two spots where everyone goes to defecate.
To defecate in the open, women and girls need to find private and safe spaces within the slum, which is often hard. Due to all these difficulties, women and girls in all the locations mentioned that they use the toilets only once or twice a day. If they need to defecate badly, they look for a place near their house and defecate in the storm water drains or in available open spaces. This is especially difficult for menstruating women and girls, who expressed apprehension over blood discharge in the drains and the paucity of secluded areas. Changing sanitary pads in the open was also difficult, as they need privacy and time; finding a place to dispose of the menstrual waste is an additional problem. Women and girls therefore tend to minimise the number of times they change their pads. This in turn increases their risk of contracting reproductive tract infections. One solution women and girls have found is to go in groups of three or four to open sites nearby to ensure privacy while changing in the open.
For women who work as domestic help, access to toilets or spaces to defecate is limited during working hours. Women reported that they leave for work in the morning and come back in the evening; during the day, they go from house to house, with little time to spare in between and have no space to change their sanitary pads. They are forced to manage with the same material through the day. ‘We wear one pad in the morning when we leave for work at 6 am; and come back between 3 and 4 pm and then change’, said a woman engaged as a cook, who lived in Rajasthani Camp, Delhi.
Waste Management and Sanitation
Poor system of waste management in slums was an issue deliberated on by all stakeholders. While community members (women, girls and men) felt that greater effort by the concerned authorities was needed to enable better sanitation systems in slums, officials from the concerned departments had varying perspectives. One official felt that while efforts were being made to ensure regular waste collection and maintenance of toilets, communities also needed to take responsibility and not throw solid wastes into drains, but in designated spots/dustbins. The DUSIB had also engaged with NGOs in some slums to initiate door-to-door waste collection. According to a DUSIB government official,
Those living in slums can afford to pay a small amount for door to door collection; and if segregation and collection is done at the household level, we can effectively manage waste by recycling plastic wastes and composting organic wastes. If this is done, the slums would be much cleaner and more hygienic to live in…
A sanitary inspector in Delhi responsible for waste management highlighted several challenges in ensuring sanitation in slums. According to him, slum dwellers often extend their houses and build on top of the drains, making them impossible to clean. This was a concern mentioned also by women in some communities. He also stated that lanes in slums are narrow, making it difficult for cleaning vans to enter. Further, given the amount of solid waste dumped into storm water drains, it was not surprising that they overflow. The mindset and behaviour of communities with regard to sanitation also need to change. Officials felt that while most persons were concerned about the cleanliness of their own households, they had little regard for the cleanliness of drains and lanes outside their homes. Further, no one allows the construction of proper dumping sites (dhalao) in front of their houses, which makes it difficult to officially designate a spot for waste collection. Disposal of menstrual waste was a concern raised by all officials, citing limited solutions to tackle the issue. Officials also agreed that the poor sanitation conditions within slums caused various illnesses and that open dumping of used menstrual waste increased health risks.
In the context of dreadful sanitary conditions (overflowing drains, solid waste dumps, to name a few), women and girls found it difficult to find spots where they could defecate in the open, especially during menstruation. The disposal of menstrual waste was also a problem. Most women and girls said that it was important to dispose of the used pads where they would not be easily noticed by others or strewn around by stray animals. ‘We try our best to wrap the pads and throw them away, yet somehow the dogs and pigs manage to tear them, it is so disgusting’, said Manju, 15 years, D Block, Seemapuri, New Delhi.
However, in several slums, women also mentioned that they throw the pads near the garbage dump or wherever else they can. In Kalyanpuri, it was observed that many pads were just dumped in an open space. This space was frequented by pigs and dogs. While women and girls agreed that dumping of pads led to poor sanitation and consequent health risks in the slums, they did not have any other solution to effective and hygienic disposal. In a few locations where NGOs are working, efforts are underway to establish low-cost matka (earthen pots) incinerators for menstrual waste. The need for appropriate systems for menstrual waste disposal and for clean, private and safe spaces where pads can be changed was emphasised by all the respondents.
Thus, given lack of appropriate spaces for defecation, women tend to use menstrual products for long durations and dispose them inappropriately, adding to the insanitary conditions in the slums and health risks.
Housing
As mentioned in the preceding section, housing infrastructure is poor and space in each household is extremely limited, which in turn, limits the privacy that women and girls need during menstruation. Girls said that they are always careful to ensure that there is no staining. ‘Since our house is small, everyone would know, and the CTC is far, so changing pads or cloth is not easy’, said Kalyani, 16 years in Seemapuri, Delhi. Given the limited space between the houses and narrow drains, washing of used menstrual cloth was also a challenge.
It is very difficult to wash our used menstrual cloth here as everyone can see what we are washing. We have to hide and wash it; we are also always worried that if red-coloured water flows through the drains, someone will notice it. There is also very little space to dry the menstrual cloth.
Support from the Family
A shop owner in Janta Jeevan Camp, Delhi, mentioned that her husband is extremely supportive of her and encourages her to talk about her problems. This she says gives her the confidence to share all her concerns openly in the house, including any menstrual or health issues she faces. Since using the CTCs was difficult, she has built a toilet in her house with the support of her husband. It is now easy for her to manage her monthly period with some privacy.
However, only a lucky few have supportive families and spouses. Most women and girls said that they hide problems, until the issue becomes critical. Menstruation was only discussed with mothers and peers in the absence of male members of the household. Girls reported that a problem was mentioned to male members only when it was unmanageable and needed medical intervention, such as extreme vaginal itching.
It also emerged during discussions that in households where women were not involved in economic activity, they were dependent on men to give them money to purchase sanitary napkins. The kind of napkins that a woman could buy was limited by the amount of money her husband gave her each month. Another aspect mentioned by women that affects their ability to access toilets is the lack of help in looking after young children. Sita Devi, a resident of Rajasthani Camp, Delhi, said that she has to change her napkin close to the house and come back quickly as she has a young child and cannot leave him alone. She mentioned that this is also the reason why she does not go to the CTC.
To walk to the CTC and come back will take at least 25 minutes to half an hour; who would take care of my son when I am gone? I cannot take him with me and besides, where would I leave him in the CTC?
External and Internal Conflicts
Discussions with women and girls also revealed that the CTC/PTs are often spaces that are not safe for women. Fighting and violence are common around the CTCs/PTs. In Delhi, it was reported that men and boys usually gather around in the day and drink alcohol near the PTs. In Jaipur, one of the girls reported that boys and men congregate near the PTs and pass comments, making it difficult to use the facilities. Women and girls thus have to constantly be on guard, when walking within the slums, walking to toilets and defecating in the open—more so when it is dark. Menstruating women and girls have to search for isolated open spaces to change pads and reported that they are constantly worried for their safety.
NGO representatives from Tughlakabad noted that in slums, given small structures and cramped living spaces, girls had witnessed and/or experienced sexual abuse, domestic violence or intimate interactions. According to the Director of the NGO,
Girls have been exposed to sexual acts because spaces are very small. They are living in a house, half the size of a classroom. It could be their father, elder brother or sister. It is all under wraps. Many of them have also been exposed to sexual abuse by their relatives and they are not even aware if this is acceptable or not.
These external and internal conflicts faced and witnessed by women and girls in slums often place them in situations of stress and psychological duress, which impacts their ability to effectively cope with and manage routine activities such as menstruation and to negotiate for their needs and concerns. Kulkarni et al. (2017) noted that women living in slums face a multitude of psychological stresses due to unsafe, inadequate or absence of sanitation facilities. These ranged from preoccupation with safety to normalisation of harassment. In the study, women mentioned feeling stressed, traumatised, ashamed, anxious, guilty, embarrassed and violated.
Conclusion
Perspectives and challenges of women and girls presented in this article reveal several complex and interrelated aspects that have an impact on how women and girls manage menstruation in the context of urban slums:
Limited knowledge and awareness on menstruation and MHM, coupled with prevailing gender norms, limited agency and stressors faced by women in urban slums affect their ability to break the silence around menstruation and question myths and misconceptions—which in turn further reduces their voice and agency. Lack of knowledge and awareness impacts use of products (type of product and frequency of changing) and the health of women and girls (as a result of not understanding how to maintain hygiene during menstruation, understating symptoms, not knowing when to access healthcare, etc.). The financial status of households constrains the use of products, as well as access to household toilets, community toilets sand healthcare facilities. It also determines whether women need to work to enhance household income, in addition to undertaking all household chores which in turn has negative implications for their health and quality of life. Poor sanitation behaviours among community members lead to improper use of available infrastructure and exacerbate the insanitary conditions in slums. These have a negative impact on health and well-being. The lack of space and high population density in slums greatly limit the privacy, safety and security of women and girls, especially needed during menstruation. Lack of familial support for women increases their domestic responsibilities and circumscribes movement, making it more difficult for them to address their sanitation and hygiene needs.
Despite various challenges and constraints, women and girls have, to the best of their abilities, developed strategies to manage their monthly period. However, given the growing population of urban poor in India, there is a critical need to address these issues, to enable women and girls to attend to their needs in conditions of safety and dignity.
The complexity of these challenges and the interlinkages between them call for a comprehensive and holistic approach involving all relevant stakeholders. In this regard, the MHM value chain could provide a useful conceptual framework. It outlines the need for a holistic approach to MHM—from creating awareness and addressing gender inequities to enabling access to a basket of products and their appropriate use, ensuring availability and use of WASH infrastructure and services and appropriate systems for menstrual waste disposal. While bringing about improvements may be complex in contexts like Delhi, where multiple authorities/departments are responsible for different services within a slum, it is essential to ensure a convergent approach with clear roles and responsibilities across the value chain for various authorities/departments. Information, education and behaviour change relevant to MHM and sanitation are of paramount importance where the departments of education, health, drinking water and sanitation and women and child development have a key role to play. In the process, it is important also to engage with men and boys on issues related to menstruation and encourage adolescent groups in communities and schools to break the silence around menstruation. Ensuring WASH infrastructure and services that respond to the menstrual hygiene needs of women and girls, is a key. Improving these on a priority basis would significantly benefit women and girls. While designing and implementing interventions, the community must be included as a primary stakeholder in decision making on what would be appropriate for their context and community. Care should be taken to ensure that all sections of the community are represented, including the most vulnerable groups within and outside households. NGOs could play the role of building linkages between various government departments and communities to ensure that the needs of the most vulnerable are addressed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.