
Abstract
Child immunisation is regarded as one of the most essential public health interventions for reducing morbidity and mortality among children. Despite several public healthcare initiatives, a considerable proportion of children are yet to be covered under vaccination service in India. This study attempts to examine the association between maternal exposure to intimate partner violence (IPV) and childhood immunisation in India. Data were drawn from the fourth round of the National Family Health Survey (NFHS-4), conducted in 2015–16. Bivariate and multivariate logistic regression models were employed to assess the associations. About 65% of sample children aged 11–23 months were fully vaccinated. After adjusting for socio-demographic factors, women’s exposure to emotional IPV was significantly associated with a lower likelihood of full immunisation (adjusted odds ratio [AOR]: 0.74, 95% confidence interval [CI]: 0.61–0.90) among children. However, physical and sexual IPV had no significant association with childhood immunisation status in the adjusted analysis. The findings suggest preventive measures against domestic violence to reduce the risk of poor child healthcare services. Furthermore, efforts should be taken for effective reproductive and child healthcare programmes, especially among socio-economically vulnerable women and children, to improve child vaccination coverage.
Introduction
Immunisation is regarded as one of the most essential public health interventions and a cost-effective preventive strategy for reducing the morbidity and mortality of children associated with infectious diseases (Acharya et al., 2002; Dayan et al., 2004). Every year, immunisation prevents two to three million deaths worldwide. However, vaccine-preventable diseases, such as tuberculosis, diphtheria, whooping cough, tetanus, polio and measles, remain well-known causes of child mortality (Levine et al., 2005). Approximately 5.3 million children under the age of five years died in 2018 globally. As per the recent estimate, 86% of children across the world received vaccines in 2018, while 19.4 million children, mostly from African and South Asian countries, did not receive any vaccine and remain vulnerable to preventive diseases (WHO, 2019). In India, around 2.6 million children have been reported as under-immunised during 2018.
A growing body of research indicates that the coverage of immunisation among children depends on various factors related to the accessibility and availability of healthcare facilities, density of health workers, knowledge and awareness of the parents, geographical location and socio-economic status (Antai, 2009; Cui & Gofin, 2007; Fatiregun & Okoro, 2012; Odusanya et al., 2008; Paulussen et al., 2006). In India, parental education and access to maternal healthcare services have a strong positive influence on vaccination coverage in children (De & Bhattarchaya, 2002). In Nigeria, mothers’ awareness and decision-making power are dominant factors of childhood immunisation (Babalola, 2009).
However, the linkage between maternal exposure to intimate partner violence (IPV) and preventive healthcare services including immunisation among children remains an obscure area of research in the existing literature. IPV is manifested in a complex pattern of physical aggression, sexual coercion and psychological abuse that has severe negative consequences on children’s health directly or indirectly (Garcia-Moreno et al., 2006; WHO, 2005). Several studies in developing countries have documented that maternal exposure to IPV is a risk factor for the morbidity and mortality of children (Ackerson & Subramanian, 2009; Åsling-Monemi et al., 2008; Ferdousy & Matin, 2015; Karamagi et al., 2007; Paul & Mondal, 2020; Silverman et al., 2009). To our knowledge, only one study in India has investigated the relationship between women’s victimisation of violence and the immunisation status of children (Sabarwal et al., 2012). However, this study was limited to the aggregate use of physical and sexual violence to examine the relationship between IPV and childhood immunisation. In order to get a more robust and vibrant relationship, we made a nuanced analysis where IPV was disaggregated into various forms of violence (e.g., physical, emotional, and sexual IPV). Moreover, we incorporated emotional violence in the present study that would add new dimension to the existing literature.
In India, the incidence of domestic violence perpetrated by the husband is rampant in society (Kimuna et al., 2013; Mahapatro et al., 2012). Also, the prevalence of infant and child mortality is unacceptably high in the country as 882,000 under-five deaths have been reported in 2018 (UNICEF, 2019). Against this backdrop, it is therefore imperative to explore the links between the maternal encounter to violence and preventive healthcare measures like child immunisation. Our study attempts to examine the association between maternal exposure to IPV and immunisation of children aged 12–23 months in India using the recent data of the National Family Health Survey 2015–2016.
Methods
Data Source
We used data from the fourth round of the National Family Health Survey (NFHS-4), conducted in 2015–2016. The NFHS-4 is a nationally representative large-scale sample survey comprising 601,509 households, 699,686 women aged 15–49 years with a response rate of 97%, and 112,122 men aged 15–54 years with a response rate of 92%. The survey was carried out across all the states and union territories of India to collect updated and reliable information on various aspects of population, health and demographic indicators, such as fertility, mortality, family planning methods, utilisation of maternal healthcare services, breastfeeding practices, nutritional status of the mother and young children, child immunisation, childhood morbidity and mortality, women autonomy, domestic violence against women, etc. The samples in NFHS-4 were selected using a two-stage stratified sampling design. In the first stage, the clusters were selected using the method of probability proportional to size (PPS). In the second stage, a complete household mapping and the listing was done in the selected cluster and 22 households were randomly chosen in each cluster in a systematic manner from the household listing. The sampling frame used in this survey was the 2011 Indian Population and Housing Census. A detailed description of the sampling design and survey procedure is provided in the NFHS-4 national report (IIPS & ICF, 2017).
Study Participants
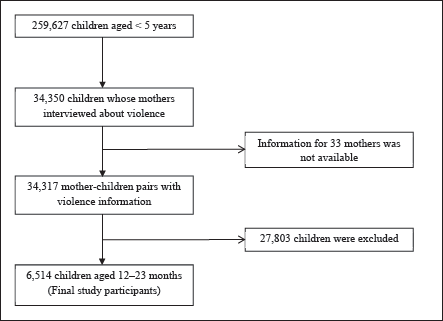
The NFHS-4 interviewed 259,627 children born to women aged 15–49 years in the past five years preceding the survey. Among these children, 34,350 had mothers who were selected and interviewed in the domestic violence module. However, complete and valid information about domestic violence is available for 34,317 samples. There were missing cases for data related to child immunisation as well. It is observed that 6,514 children aged 12–23 months had complete information on immunisation care in the NFHS-4 survey. Therefore, the missing cases were excluded from analysis, and the final statistical analysis of this study was restricted to these samples that had valid information about IPV of mothers as well as the immunisation of children. Therefore, the study participants in this article constitute 6,514 child-mother pairs (Figure 1).
Outcome Variable
The outcome variable of this study is complete/full immunisation among children aged 12–23 months. The basic immunisation care of children includes BCG vaccine for protecting against tuberculosis; DPT vaccine which protects against diphtheria, pertussis (whooping cough) and tetanus; polio vaccine and measles vaccine. Complete or full immunisation defines as a child who received one dose of BCG, three doses of DPT, three doses of polio and one dose of measles vaccines (IIPS & ICF, 2017). The information regarding the vaccination of children was collected either from the health cards or direct reporting from the mother at the time of the survey. For this study, a full immunisation variable was constructed from all eight basic vaccinations and dichotomised as fully immunised (coded as ‘1’) and not fully immunised (coded as ‘0’).
Predictor Variables
Women’s exposure to violence perpetrated by the current husband or the most recent husband is the key predictor variable in this study. Information about IPV was gathered from the ever-married women during the survey of NFHS-4 by asking a series of questions to the women. Three major forms of violence, physical, emotional and sexual, were identified in this survey. Physical violence was determined by a set of seven questions asking the women, whether the husband (a) pushed, shook or thrown something at her, (b) slapped her, (c) twisted her arm or pulled her hair, (d) punched her with his fist or with something that could hurt her, (e) kicked, dragged or beaten her up, (f) tried to choke or burn her on purpose or (g) threatened or attacked with a knife, gun or any other weapon. Sexual violence against women was measured by three questions, whether the husband ever (a) physically forced her to have sexual intercourse, (b) physically forced her to perform any other sexual acts or (c) forced her with threats or in any other way to perform sexual acts when she did not want to. Similarly, emotional violence was captured by three questions, whether the husband ever (a) humiliated her in front of others, (b) threatened to hurt or harm or (c) insulted or made her feel bad about herself. Furthermore, a final women’s exposure to IPV variable was developed and categorised into five groups: (a) experience of physical violence, (b) experience of sexual violence, (c) experience of emotional violence, (d) experience of all three forms of violence and (e) experienced no violence from the current or former husband.
Covariates
A wide range of socio-demographic characteristics was included as covariates in this study. Socio-demographic characteristics encompass child demographics, parental characteristics and socio-economic factors. Child demographics include sex of child (male and female) and birth order (<3 and ≥3). Parental characteristics comprise maternal age (15–24, 25–34 and 35–49 years), maternal education (illiterate, primary, secondary and higher) and father’s education (illiterate, primary, secondary and higher). Besides, socio-economic factors such as place of residence, caste, religion, household wealth quintile and region were considered as potential covariates. Place of residence was incorporated to determine rural and urban differences in immunisation coverage. Caste was considered a key predictor of childhood vaccination. In this study, caste was divided into three groups: Scheduled Caste (SC)/Scheduled Tribe (ST), Other Backward Classes (OBC) and ‘others’ (forward caste). Similarly, religious affiliation also plays an important role in the behavioural pattern of respondents towards receiving the vaccination for children. Religion was categorised into three groups: Hindu, Muslim and others. Household wealth seems to be a vital factor in seeking vaccination for children. The wealth quintile of households was measured from the ownership of household assets, dwelling characteristics and access to basic services such as drinking water and sanitation facilities. The NFHS-4 generated a score for each individual using principal component analysis (PCA) and then categorised into five quintiles ranging from 1 (poorest) to 5 (richest), where each quintile represents 20% of the total respondents. Further, to explore the regional variation in immunisation of children, the states and union territories of India were grouped into six regions based on geographical contiguity and cultural similarities (IIPS & ICF, 2017).
Statistical Analyses
Univariate statistics were carried out to show the percentage and frequency distribution of socio-demographic characteristics. To examine the differences in immunisation status of children by the predictor variables, bivariate percentage distribution was estimated, and then the differences were tested by Pearson’s chi-square statistic. The sample weight was used for the estimation of percentage distribution. Finally, bivariate and multivariate logistic regression models were employed to examine the association between maternal exposure to IPV and full immunisation of children. The regression results are presented by odds ratio (OR) with a 95% confidence interval (CI). The results of regression models were considered to be statistically significant at p < 0.05. All the statistical analyses were performed using STATA version 14.0 (StataCorp LP, College Station, TX, USA).
Results
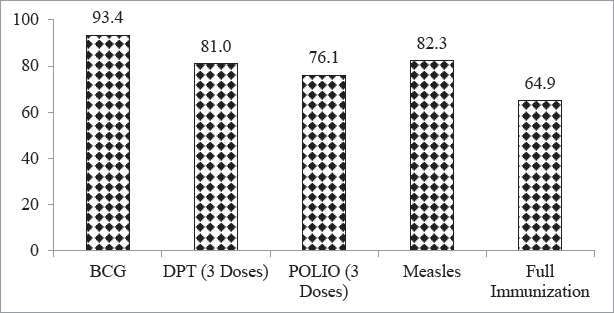
Among 6,514 living children aged 12–23 months, about 93.4% of them had one dose of BCG, 81% had three doses of DPT, 76.1% had three doses of polio and 82.3% received one dose of measles. Moreover, it is found that nearly 65% of children were fully immunised (Figure 2).
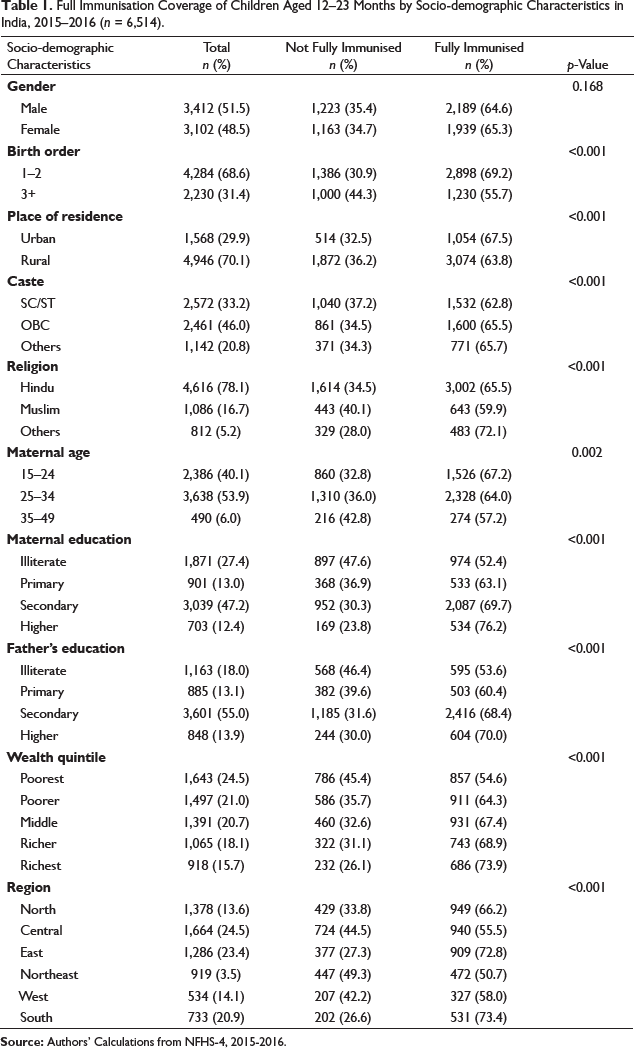
Full Immunisation Coverage of Children Aged 12–23 Months by Socio-demographic Characteristics in India, 2015–2016 (n = 6,514).
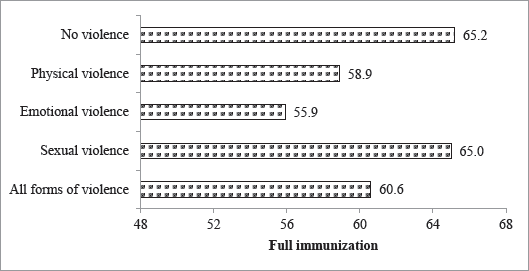
About 58.9%, 55.9% and 65% of children had fully immunised whose mothers experienced physical, emotional and sexual violence perpetrated by the partner, respectively. Moreover, full immunisation coverage was 60.6% among the children of mothers who experienced all forms of violence, as compared to 65.2% of children of non-abused mothers who were covered under vaccination (Figure 3).
We found marked differences in full immunisation coverage by socio-demographic characteristics. Full vaccination coverage was lower among children with three or more birth orders, those who lived in rural areas, belonged to SC/ST, were Muslims and resided in poor families. It is also found that immunisation coverage decreased with an increase in maternal age. Moreover, children of illiterate mothers were significantly lower recipients of full immunisation as compared to those mothers who attained the primary or above level of education. Similarly, the education of fathers was positively related to children’s immunisation coverage. Furthermore, immunisation coverage by geographical regions showed that it was the highest in the South region (73.4%) followed by the East (72.8%), while the lowest coverage was found in the Northeast region (50.7%) of the country (Table 1).
Bivariate and Multivariate Logistic Regression Analyses for Assessing the Association Between Maternal Exposure to IPV and Child Immunisation in India, 2015–2016.
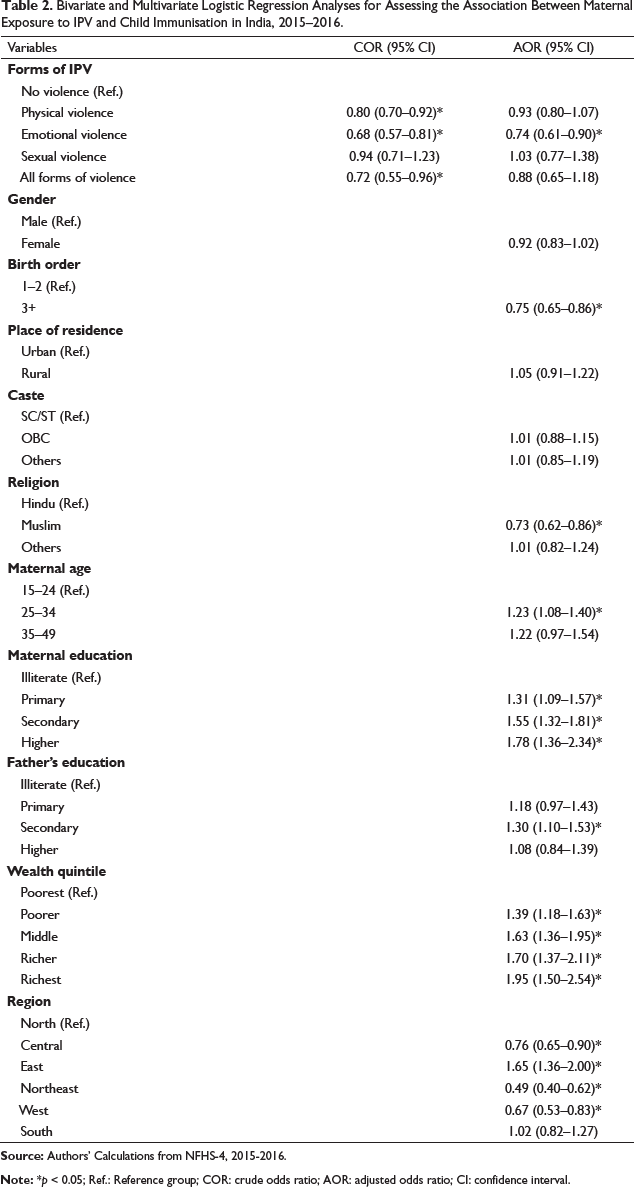
Results also indicated that children with higher birth order (three or more) were less likely to be vaccinated (AOR: 0.75, 95% CI: 0.65–0.86) than those with the first or second order. The odds of full immunisation were lower among Muslim children (AOR: 0.73, 95% CI: 0.62–0.86) as compared to Hindu children. Children of mothers aged 25–34 years were more likely to be immunised (AOR: 1.23, 95% CI: 1.08–1.40) compared to mothers aged 15–24 years. Parental education had a strong positive correlation with the complete vaccination of children. Children of mothers with primary education (AOR: 1.31, 95% CI: 1.09–1.57), secondary education (AOR: 1.55, 95% CI: 1.32–1.81) and higher education (AOR: 1.78, 95% CI: 1.36–2.34) were more likely to be fully vaccinated compared to those of uneducated mothers. However, the influence of fathers’ education on children’s vaccination coverage was found to be slightly lower. It is found that the secondary level of education of fathers was associated with a 30% (AOR: 1.30, 95% CI: 1.10–1.53) increased likelihood of childhood full immunisation as compared to illiterate fathers. Household wealth also had a strong association with vaccination coverage of children. Children from the richest wealth quintile were almost twice more likely to be fully immunised (AOR: 1.95, 95% CI: 1.50–2.54) than those from the poorest wealth quintile. Geographical regions also had a significant influence on child vaccination care. Compared to the North region, children from the Central (AOR: 0.76, 95% CI: 0.65–0.90), Northeast (AOR: 0.49, 95% CI: 0.40–0.62) and Western regions (AOR: 0.67, 95% CI: 0.53–0.83) were less likely and children from the Eastern region (AOR: 1.65, 95% CI: 1.36–2.00) were more likely to be fully vaccinated.
Discussion
The present study examined the association between maternal exposure to IPV and child immunisation status in India using a large-scale, nationally representative cross-sectional dataset. Despite several international and national efforts to eliminate the gruesome act of violence against women, it remains widespread in Indian society. Furthermore, the coverage of immunisation remains unsatisfactory in India, leading to a high incidence of childhood illnesses and mortality. According to recent NFHS-4, about 62% of children aged 12–23 months received full vaccination in 2015–2016 (IIPS & ICF, 2017). To achieve the target of the Sustainable Development Goal (SDG) in reducing the rate of child mortality, an accelerated improvement is required in vaccination drive of the country.
Our crude analysis indicated that maternal exposure to physical and emotional violence was significantly associated with a decreased likelihood of full vaccination among children. Moreover, the association between maternal encounter with emotional violence and childhood full immunisation remained significant even after adjusting for socio-demographic variables. We did not find any significant association between sexual violence against women and childhood immunisation. A previous study conducted in India reported that maternal experience of physical or sexual violence is associated with a 10% lower likelihood of childhood immunisation (Sabarwal et al., 2012).
Women’s exposure to IPV may affect child healthcare through several pathways. Evidence has found that IPV is associated with an increased risk of controlling behaviour of the husband (Antai, 2011). The controlling behaviour of the husband restricts women from access to financial resources, education, employment and healthcare that may affect child healthcare including receiving immunisation services. Additionally, abused mothers suffer from psychological stress, depression and anxiety (Beydoun et al., 2012; Campbell, 2002), which further results in maltreatment for their children (Renner & Slack, 2006; Zolotor et al., 2007).
In agreement with earlier research (De & Bhattacharya, 2002; Ghei et al., 2010; Parashar, 2005), the present study showed that children of higher birth order and being a Muslim are less likely to be fully vaccinated. We also found that parental literacy and children from the upper quintile of household wealth were positively associated with childhood immunisation coverage, which is also in line with several previous studies conducted in India (Parashar, 2005; Ghei et al., 2010; Sabarwal et al., 2012). Furthermore, our study found significant differences in childhood immunisation coverage by geographical regions. Inequalities in child immunisation status across geographical regions have also been reported in prior studies of India (Singh, 2011, 2013).
Limitations and Strengths
This study has some limitations. We could not draw the causal relationship between maternal exposure to IPV and child vaccination status due to the cross-sectional nature of the data. Earlier studies documented several other potential factors of child healthcare, for example, availability of health infrastructure and distance to the health facility, which may have a significant influence on child immunisation. We could not incorporate those important factors due to the unavailability of information in the NFHS-4 data. However, our study included relevant socio-demographic factors in the adjusted analysis to assess the net influence of IPV on child immunisation status. Most of the data used in this study are retrospective and self-reported; therefore, recall bias might have been occurred. Further research is required to explore the pathways explaining the association between maternal experience of IPV and childhood immunisation.
Despite the above limitations, this study provides recent evidence on the association between maternal exposure to IPV and child vaccination status. Our study added value to the emerging body of public health literature that could explain the potential mechanism of the association between maternal experience of domestic violence and mortality in children.
Conclusions
The present study has found that women’s exposure to emotional violence was associated with a decreased likelihood of childhood full vaccination coverage. The findings of this study highlighted that abusive behaviour against women by their partners leads to lower child healthcare, which may ultimately increase the risk of childhood morbidity and mortality. This study is important in low-resource settings like India, where a substantial proportion of children are not fully covered under vaccination and the rate of infant and child mortality is also alarming. Preventive measures should be initiated against domestic violence to reduce the risk of poor child healthcare. Furthermore, efforts should be taken for effective reproductive and child healthcare programmes, especially among vulnerable groups of women and children, to improve child vaccination coverage.
Footnotes
Acknowledgements
The authors are grateful the Demographic and Health Surveys (DHS) Program for granting access to the data used in this research.
Declaration of Conflicting of Interests
Funding
The authors received no financial support for the research, authorship and/or publication of this article.