
Abstract
Health systems with strong comprehensive primary health care (CPHC) are known to result in better health outcomes for people. In India, there is a recent push to strengthen CPHC through Ayushman Bharat. This study aimed to document lessons from successful CPHC initiatives in rural and urban India using a qualitative case study approach. A total of 72 CPHC initiatives were identified through desk review and 12 of these were studied as cases. The following two main models of CPHC delivery were seen in India: (a) a hospital or health centre with outreach and (b) social franchising model, prevalent in rural and urban contexts, respectively. Themes identified were related to organisation of services, workforce, financing and challenges in practice. Services being comprehensive, dialoguing with the community, addressing social determinants were themes under organisation of services. There is need for more generalists and training health professionals towards CPHC. Financing of CPHC especially in the rural context remains a major challenge and cannot be sustained with user fees. Leadership, values, team-based care and organisational culture play a vital role in the delivery of good quality CPHC. These findings contribute to the literature on what works and why, which could be used to design CPHC in India.
Background
Health systems with strong comprehensive primary health care (CPHC) delivery systems are known to result in better health outcomes for people (Macinko et al., 2009; Starfield et al., 2005). Many global health gains, such as increased life expectancy are a result of sustained inputs at primary levels of healthcare. There is renewed focus and attention to CPHC especially as it is recognised to be a key means towards achieving universal health coverage (UHC) and the sustainable development goal (SDG) 3, world over. The recently affirmed global declaration for primary healthcare at Astana, 40 years after the Alma Ata declaration, renewed global commitment (WHO, 2018).
The WHO defines CPHC as consisting of three components: (a) meeting people’s health needs through comprehensive promotive, protective, preventive, curative, rehabilitative and palliative care throughout the life course, (b) systematically addressing the broader determinants of health and (c) empowering individuals, families and communities to optimise their health (WHO & UNICEF, 2018). Healthcare delivery is envisaged closest to people’s home, as a hub to coordinate services, guiding people through the health system as they seek care (WHO, 2008). Primary healthcare, therefore, is well positioned to make a sustainable and meaningful impact on the health and well-being of populations.
Strengthening CPHC in terms of increased access, financial protection and improved quality of care is especially relevant for low- and middle-income countries (LMICs) like India. Studies estimate that scaling up primary healthcare interventions across LMICs could save 60 million lives and increase average life expectancy by 3.7 years by 2030 (WHO, n.d.).
India has shown commitment towards CPHC since the Bhore Committee report in 1946, that described primary care services as the backbone of healthcare (Bhore, 1946). India’s first National Health Policy (NHP), in 1983, emphasised CPHC and was strongly influenced by the Alma Ata declaration. There have been several such programs and policies that have shaped the landscape of CPHC in India thereafter. The National Health Rural Mission (NHRM) of 2005 and the introduction of the Accredited Social Health Activist (ASHAs) are landmark interventions that have had a significant impact. Most recently, the NHP 2017 has led to a wave of reforms aimed at strengthening government funded primary health centres (PHCs), such as the recently launched Ayushman Bharat. Ayushman Bharat is a program with two pillars, national financial protection scheme and CPHC at health and wellness centres. However, there exist many challenges in achieving quality CPHC. Inequitable health and the high out-of-pocket expenditure continue to plague the Indian health system with no easy solutions (Balarajan et al., 2011). Adding to these are new challenges such as the growth of the private sector with little or no regulation and the growing burden of chronic diseases (NSSO, 2020).
Strengthening CPHC in India needs a concerted and multi-level effort consisting of policies, reforms and continuous learning from existing models of primary healthcare delivery in local settings. There are several successful examples of government, private and non-governmental organisations delivering good quality primary care services that have resulted in improved health outcomes for the populations served.
Objective
The aim of this study was to identify successful non-governmental CPHC delivery examples, and study them to identify commonly experienced challenges, facilitators and models of service delivery. The findings are relevant to efforts for strengthening primary healthcare especially as India implements Ayushman Bharat.
Methods
Study design: In the first phase of this research study, an extensive desk review of literature, both published and grey, to identify organisations delivering CPHC in India was conducted. In total, 12 organisations were purposively selected as ‘cases’ for the second phase of the study. A case study approach was used primarily using qualitative methods for primary data collection. The case study approach was chosen to enable an in-depth understanding. Each case study was investigated using a systems thinking lens and went beyond the program elements to unpack the local context in which these are delivered.
The study received ethical approval by the Institutional Ethics Committee at Institute of Public Health (IPH), Bengaluru.
Phase One: Literature Search Methods
Yield from Searching Different Sources and Databases
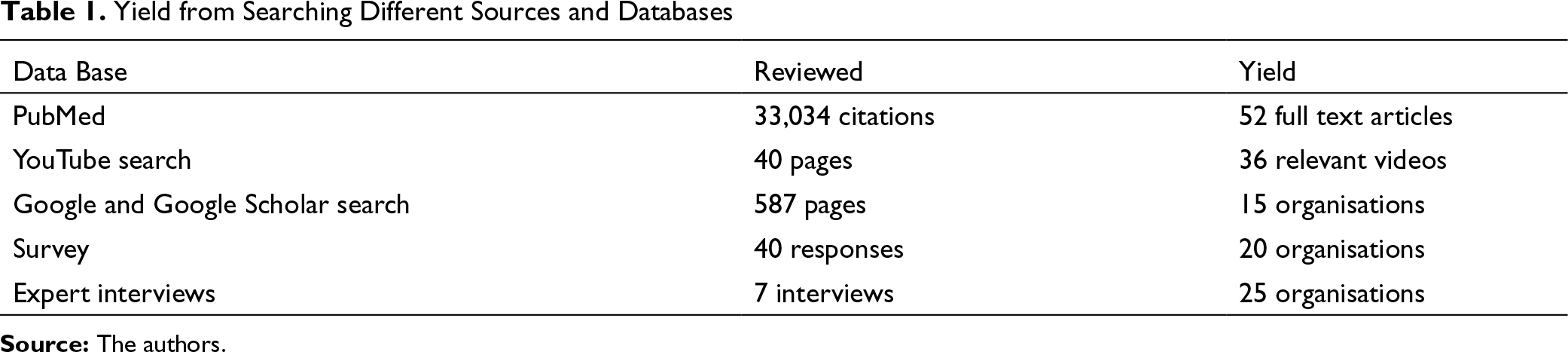
In addition, a rapid two-question survey was conducted using social media and email in networks of public health academicians, community health and family physicians. Participants were asked to list organisations they knew about that deliver CPHC in India. Informal conversations were also conducted with purposively selected public health experts to create a free listing of CPHC organisations. After removing duplicates from the multiple sources, 72 CPHC initiatives/organisations were identified. Characterisation of the 72 organisations was done in terms of the location (urban/rural), governance, financing, services provided, workforce, information system and community engagement to identify the model for organisation and delivery of services. Selection criteria were applied to this list, to purposively select 12 cases for Phase two of in-depth study.
Inclusion criteria
The organisation has a catchment area—rural or urban. The organisation provides CPHC, which includes preventive, promotive, curative and rehabilitative services as opposed to a single disease focus for primary care. The organisation is currently operational and has been since at least the last three years.
Exclusion criteria
Organisations operating in temporary project/research mode
Phase Two: Data Collection Methods
In Phase two, semi-structured in-depth interviews were conducted with the leader or founder of each organisation. An interview guide was used to conduct the in-depth interview. All interviews were conducted virtually and recorded after an informed consent process. Interviews were scheduled at a date and time that was convenient for the participants, and lasted for an average of 60–70 minutes. The interviews were led by team members trained in qualitative research methods. The data collection procedures were tailored to the circumstance of the ongoing pandemic. A questionnaire was used for extraction of secondary data available at the organisation and the leaders were requested to facilitate the process. The questions were regarding indicators, organogram, services provided by the facility, outputs, outcomes and published reports of the case studies.
Data Analysis and Theoretical Framework
All the interviews were conducted in English and transcribed verbatim. Thematic analysis was conducted. Codes were identified a priori using the Primary Health Care Performance Initiative (PHCPI) framework. The PHCPI Conceptual Framework has developed to describe the critical components of a strong primary healthcare system. The framework has resulted from an extensive search of literature and builds on existing frameworks for health systems performance assessment used in LMICs (The PHCPI Conceptual Framework, n.d.). The framework reflects an input process and outcome logic, identifying system, input, service delivery and output as dominant domains. There is an overall directionality of influence, where the system domain influences the inputs domain, which affects the complex interplay within the service delivery domain. Successful service delivery contributes to effective outputs that affect outcomes. The framework acknowledges that CPHC performance lies within a larger health system, which itself lies within wider political, cultural, demographic and socioeconomic contexts. Codes such as access, person-centred care, organisation, human resource, sociocultural context, organisation of services were inspired by the framework. New codes were identified for the data that did not fit the codes previously identified. Some new codes identified were training challenge, facilitators and values. NVivo software, QSR International Pvt Ltd. (2020), released in March 2020 was used for the qualitative data analysis. The quantitative data collected was highly heterogeneous, and therefore, it is not summarised across case studies. The quantitative data was used to triangulate the qualitative findings of each case study. There were no discrepancies in the data from different sources for each case study.
Results
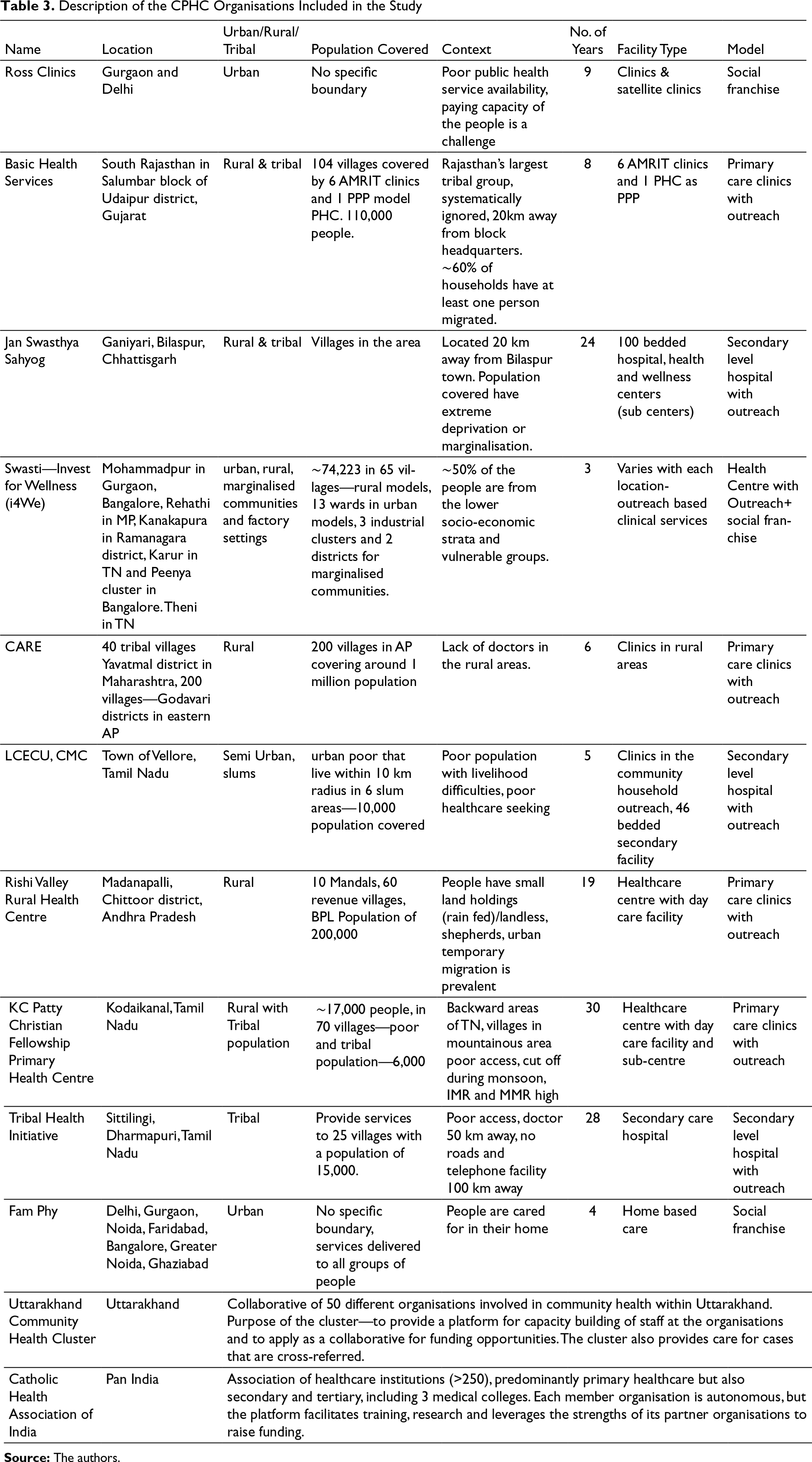
We first present the two models of CPHC delivery that emerged from a characterisation of the 72 models identified in the search. Next, the characteristics of the 12 organisations selected for in depth study, referred to as ‘cases’, are briefly described. Then, the main themes that emerged from the analysis of qualitative data are presented.
Reviewing the organisation of service delivery in all the 72 examples identified in this study, it appears that there are two main models of service delivery for CPHC in India. These models stand out despite the diversity in services and in the organisation of services. The aim was not to fit the many examples into tight descriptive models but to group them based on the commonalities of services and organisation. The two models that emerged were the hospital or clinic with outreach (hub and spoke model) and the social franchising model (or chain of clinics). The two distinct models are relevant to setting and have been applied within a certain context (Table 2).
Hospital or Clinic with Community Outreach and Community Development Activities
This model is the most widely implemented and is also how the government (public) healthcare in rural locations is organised. PHCs cater to a defined catchment area and are responsible for the health of that community. The health centre with outreach delivery model is based on the availability of secondary level services (including facility for surgical interventions) at sub-district or district level hospitals. In the absence of an accessible secondary level hospital for referral, some of these CPHC initiatives have evolved to secondary level hospitals and therefore cater to primary and secondary level of care for a defined population. This model is characterised by activities to reach out to the community. Most of the examples studied engage in community development activities and usually have community health workers and volunteers from the community in addition to doctors and nurses to deliver services.
Social Franchising for Primary Healthcare
Characteristics of the Models for Primary Care Delivery in India
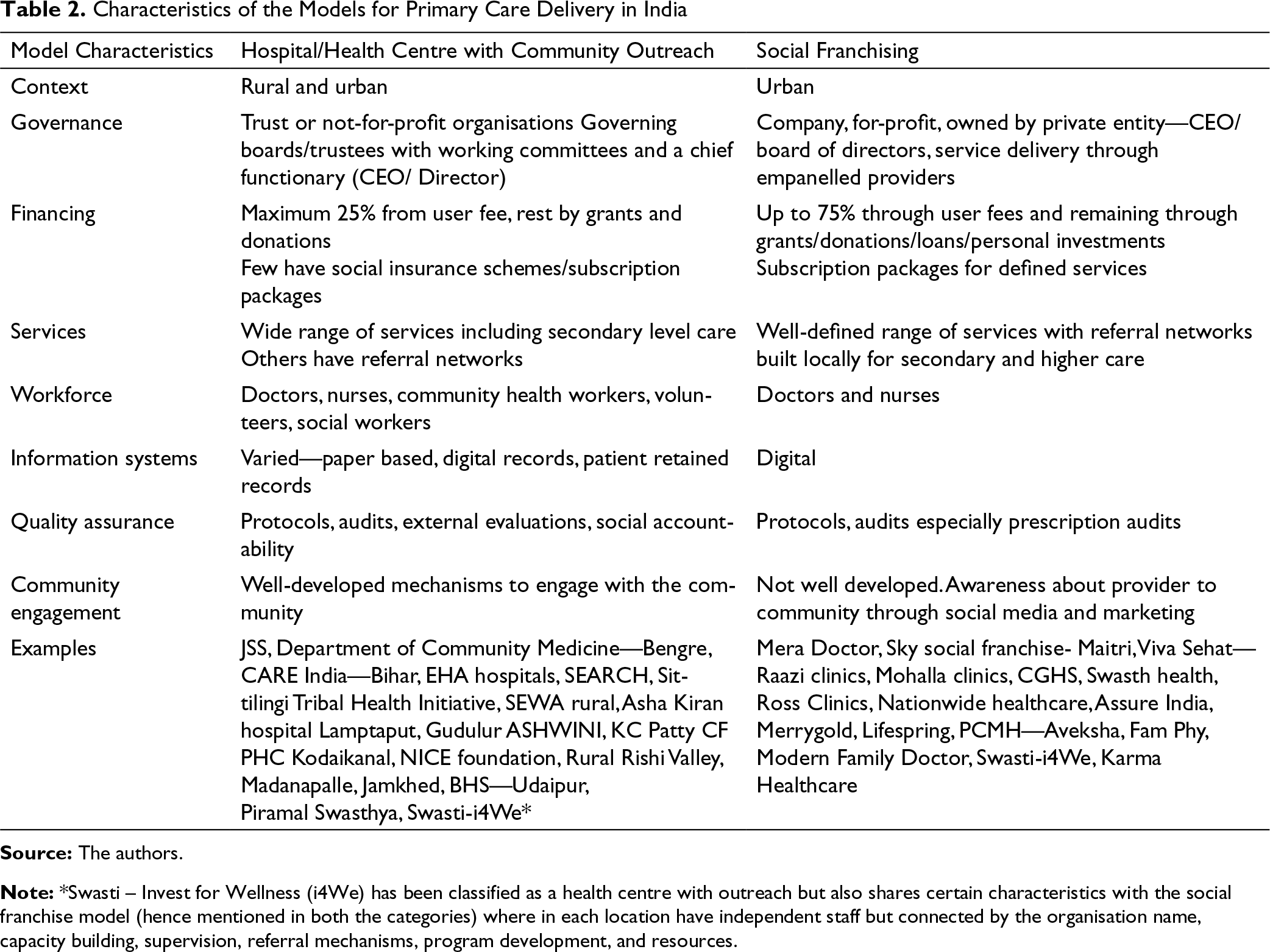
Note: *Swasti – Invest for Wellness (i4We) has been classified as a health centre with outreach but also shares certain characteristics with the social franchise model (hence mentioned in both the categories) where in each location have independent staff but connected by the organisation name, capacity building, supervision, referral mechanisms, program development, and resources.
Description of the CPHC Organisations Included in the Study
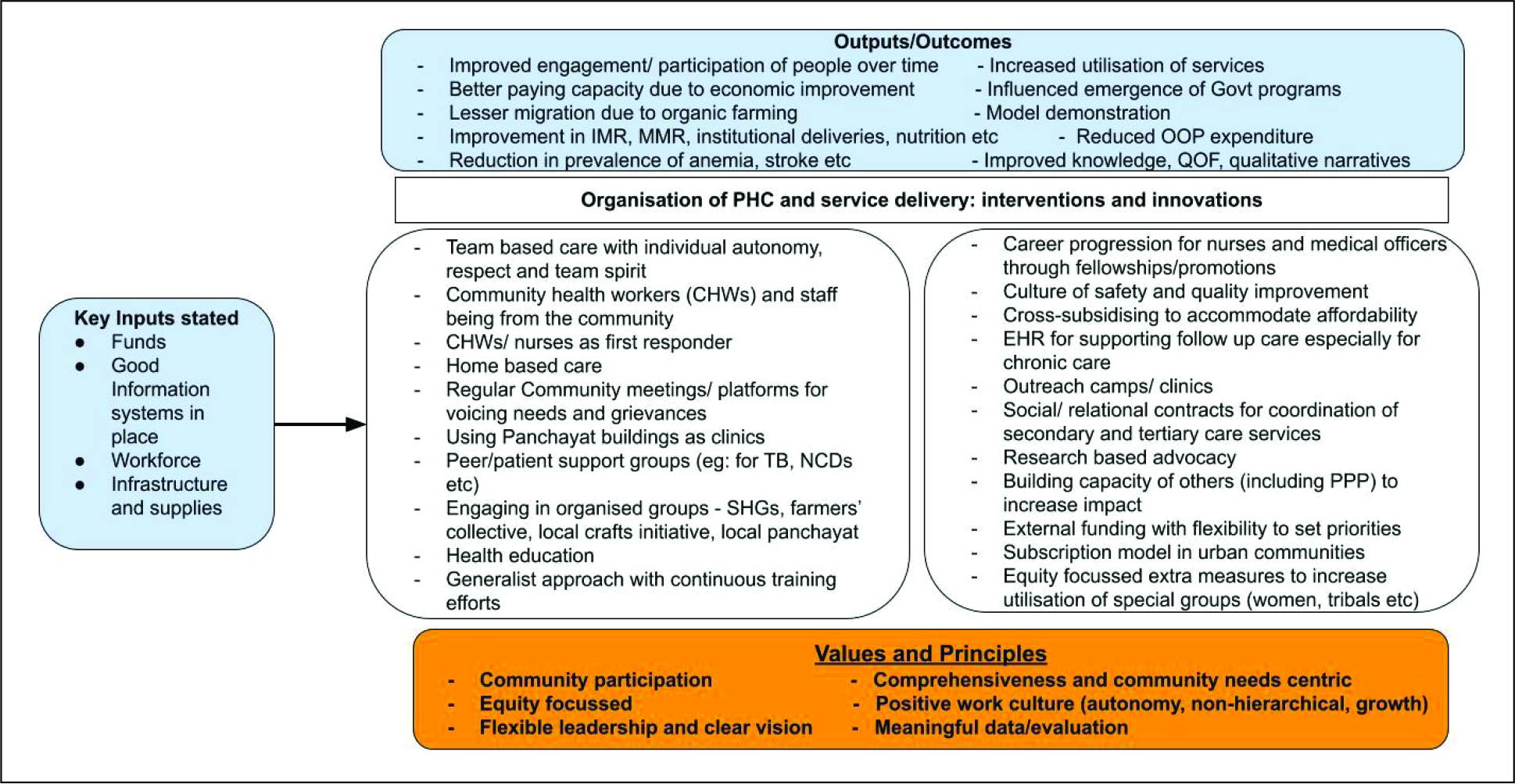
The major themes that emerged are discussed below and are related to the services delivered, community engagement, addressing social determinants, failure of current training for medical health professionals, team-based delivery, financing primary healthcare and the challenges in delivering primary care services (Figure 1).
Services Should Respond to the Needs of the Community and Should Not Be a Fixed Package
A major theme that emerged was that the vision of primary healthcare was comprehensive service provision. CPHC was articulated as health services that responded to all the needs of the community ranging from immunisation and maternal care to child health, non-communicable disease, eye care, dental care, mental healthcare and palliative care, depending on the needs of the community. A knowledge of the needs of the community was the starting point for most of the examples studied and they undertook a needs assessment of the area, before initiating services. Services delivered were not a static package but evolved in a continuous effort to respond to the local needs. Most of the examples in these case studies began with providing maternal and child health but had expanded to non-communicable disease care. The quotes below illustrate the vision for CPHC that most of them expressed:
Scope of services is defined by what the needs are, the needs include both what people need and epidemiologically what is the burden, the scope of services need to be defined by that and by comprehensiveness and not by focusing on a few sets of conditions.—M2 As the organisation goes along, thinking keeps changing, and I feel that it is a good thing that, thinking keeps changing, many people ask why are you changing it now, well…it was a need earlier and now it is not!—M9
In response to the question regarding a formulation for basic services or a basic package most models studied said that primary healthcare should not list a package of services. Instead, all health needs of a community should be addressed.
Dialogue with the Community and Building Trust is Key to Deliver Primary Healthcare
The importance of engaging with communities was a dominant theme that emerged. Varied strategies were described to engage meaningfully with people. They emphasised the importance of building trust and rapport with the communities while providing primary healthcare. Even before setting up formal services such as a clinic, most of the cases reported investing time to understand the local health needs of the community. Most cases reported a process of dialogue with the community that usually took many months to establish. The willingness for the agenda to be set by the community came out as an important factor in being relevant to the needs of the community. The process of continuous engagement with the community also ensured relevance and fostered the initial motivations in delivering primary healthcare:
Before we start any clinic, [we should] go to that community, talk to the community members, to panchayat members, to influential members and lay people, women and men, hold meetings, it is a process about three to six months.—M2 I think we need to form a rapport with the community, especially the vulnerable sections and make sure they feel at home first.—M9
Some ways in which a trustful relationship has been built with the community mentioned are as follows: Providing good quality care that was acceptable to the community, tailored to their needs. Saving a life in an emergency, especially of a child contributed to the building of trust. Getting involved in matters of the community such as farming and livelihoods. Responding to whatever needs the community has in a timely manner even if these are beyond health service provision.
Trust of the community in these organisations was demonstrated by people coming from long distances to access care and in their acceptance and compliance to treatments.
Addressing the Social Determinants of Health Makes Primary Care Service Delivery Meaningful
There was a clear emphasis on the need to address the social determinants of health such as income generation. An active attempt to get involved in livelihoods and social issues that impact health and wellness was made by most of the cases. There was a common understanding that CPHC is best positioned to get involved in these issues and has the potential for maximum impact on health. The common ways of involvement in improving the social determinants of health identified was through providing inputs in farming practices, encouraging handicrafts businesses and providing platforms, such as e-commerce platforms, to increase reach of homegrown products for the community:
So, it was the need coming from the community, help us with this, so, we were completely untrained, we had no knowledge of farming or agriculture, but we went and learnt, came back sat down with the farmers, we didn’t learn about farming, but we learnt about sales, marketing, you know all sorts of things…when we went into the craft initiative, we knew nothing about craft.—M9
Addressing deep-rooted issues of caste, alcoholism and other social evils were a concern for most organisations. Some of the cases did make attempts to address them with varying success. The pervasive nature of these social evils and the impact on health also is a source of frustration as expressed by many leaders in this study:
Consistent challenges around water sanitation, access to food, issues of gender-based violence, mental health and relationships. So, these are some of the other aspects to quality of life that we are also working on, with families, with groups of people, with the youth.—M4
Training for All Health Professional Cadres, Especially Doctors, Fails to Orient and Equip for Primary Healthcare Delivery; Need for Multi-Skilled Generalists and Family Physicians
A dominant expression from all the participants was the lack of skills among healthcare workers to respond to the needs and challenges of CPHC. The use of standardised protocols and guidelines was a measure taken to overcome skill deficiencies among health professionals. Almost all the organisations had their own in-house training programs that were based on the tasks and preferences or interests of staff. The collaborations included in the study identified capacity building initiatives as an important expectation and contribution of the collaborative:
They all have degrees, okay. They have a lab tech DMLT, or BSc lab tech or a BSc nursing, right, but they know nothing. So, you know, the quality of training is very, very poor in these colleges, so we train them here, we train them to what we want to.—M7
Most staff need to perform multiple tasks and be multi-skilled. Even if the doctors have a specialisation, they need to perform as generalists. The need for primary care family physicians or general practitioners that are multi-skilled was strongly emphasised:
Yes, but we strongly feel against specialisation in medicine. So, all the physicians who work here have de-specialised themselves. So, you know, if there is an obstetrician in our program, she will obviously handle all complicated surgeries including complicated caesareans…. But all physicians could be competent to be able to do a caesarean if necessary.—M3
The profile of a generalist needs to be raised so that more people train as family or primary care physicians. Further, the deficiency in the number of seats available for family medicine as compared to other specialties was also expressed. The lack of mentors for family physicians was another deficiency highlighted that could be overcome with increased attention to recruiting more family physicians:
It is all about giving respect, self-respect, the moment you do that, the moment you change that family healthcare will survive, if you do not do that, family healthcare will not survive.—M10
The need for career progression and pathways especially for nurses in primary care was also expressed. Most leaders felt this would enable more nurses and doctors to take up primary healthcare as a career.
Primary Care Leadership Needs to Facilitate Values-Based Team Delivered Care
Relational leadership that leads by doing and influences change in communities by inspiring the team emerged as a strong theme in the examples studied. Each of the leaders talked about leadership that was based on relationships and not on hierarchy. Each of them emphasised team-based care and the value of each member of the team. In most of the cases studied, the care was led by doctors or nurses; however, they all mentioned that team-based care was required to deliver or organise CPHC:
So, it’s not that they (leaders) don’t go to the community, they don’t do surveys on their own, they don’t run the peripheral clinics no, everyone, from the senior most person has to be part of the work.—M3
Doctors will be required to deliver primary care especially as prescribing medicines depends on them but there are many things in the delivery of primary care that nurses, community health workers, social workers can deliver. Nurses were an important input in the workforce models for primary care delivery and were crucial to the delivery of most healthcare needs of the community, including acute and chronic care. Community health workers also play a crucial role in most models and provide the essential connection with the community. Most models reported an additional role of volunteer health workers:
We need a doctor in primary healthcare, but not doctors determining and you know, always leading the work. So, the doctor yes but as a part of a team.—M3
The working culture because of the leadership pattern was an important theme that many of the leaders spoke of as critical to the process of providing CPHC. A working culture characterised by valuing all individuals, horizontal structure of organisation and an atmosphere of equality facilitated team-based care and was evident as illustrated by this quote:
It should be a joyful work environment, everybody should feel happy doing that, …we do expect certain rules, etc., but, we believe in responsibility where, you know, people are allowed space, to find out for themselves what works best within the certain parameters, a respectful, non-hierarchical work culture, …we enforce that, nurses doctors both of them are equal, and they work together with mutual respect for each other’s work.—M2
Each of the leaders expressed a deep motivation to serve the community, the underserved and marginalised as their source of inspiration. Many of them, interestingly, refer to a role model to shape thought and action such as Gandhi or deep religious convictions such as the desire to demonstrate love for neighbours. It was evident that this was reason why most of the leaders had chosen geographic areas to focus on the poor, marginalised and most deprived.
Primary Healthcare Delivery Cannot Raise Its Own Funds and Financial Investments Should Be Weighed Against Measurement of Gain Not Expenditures
A clear theme about financing of primary care was that preventive and promotive aspects of CPHC will always require external funding. Only acute medical care to some extent can provide for some of the finances required. Most of the case studies had received funding from a variety of sources such as corporate organisations, larger healthcare organisations and government insurance schemes:
Only about 25% is something that we can collect from the state schemes or from people…people that pay for the illness. For 75% we have to depend upon funding from, from well-meaning corporate organisations or foundations, as well as from…overseas collections from friends and from foundations that one feels comfortable taking money from.—M3
Primary care provision in urban areas on the contrary were models that financed themselves. This may, however, be due to the difference in the paying capacities of the urban versus rural populations. Rural primary care serves a greater proportion of people that are impoverished. The business model for primary care in urban areas was described as an asset-lite model. Investments on infrastructure, equipment and personnel were kept to a minimum. The concept of cross-subsidising, that is, charging those who can pay to create a surplus that can be used for those who cannot, is actively used in the urban models:
User fee, we are trying to optimise the user fee, because we have to, we charge them number one because we have to sustain, secondly the perception of urban India is also that you have to charge them. The voluntary work that we do is just voluntary, so that is a different thing altogether, but then, other people we charge them,—M10
Self-sufficiency for primary care would be at the cost of the poor that would be excluded, if there is a reliance on user fees or insurance schemes.
Primary Healthcare Delivery Is Challenged by the Factors Affecting Providers, Local Context, Financial Resources and the Measurement of Impacts (Figure 2)
Local contextual factors play an important role in the delivery of primary healthcare. The urban and rural contexts are very different and affect the delivery of services in different ways. In the rural areas that are usually remote and being the only service provider was challenging. Doctors and other staff work almost continuously and express physical tiredness in delivering care as the needs are overwhelming. The extent of depravity and social problems also have an emotional toll that health workers must handle:
But in primary care, you’re always on to be accessible to people. So, people come in different times, don’t have clearly defined shifts. So, it does take time, you might not be free during the day, and it’s only in the evening, when you think you can relax, but you can’t…it’s not so easy.—M8 I think the largest challenge, I would say is when you are faced with the level of deprivation that people have in central India, how do you restrict the scope of what you can do, as well as the geographical spread of the work, I think is, is a difficult decision and we don’t always come up with the right solution…it is overwhelming…the, the physical and the emotional for people who are working in it.—M3
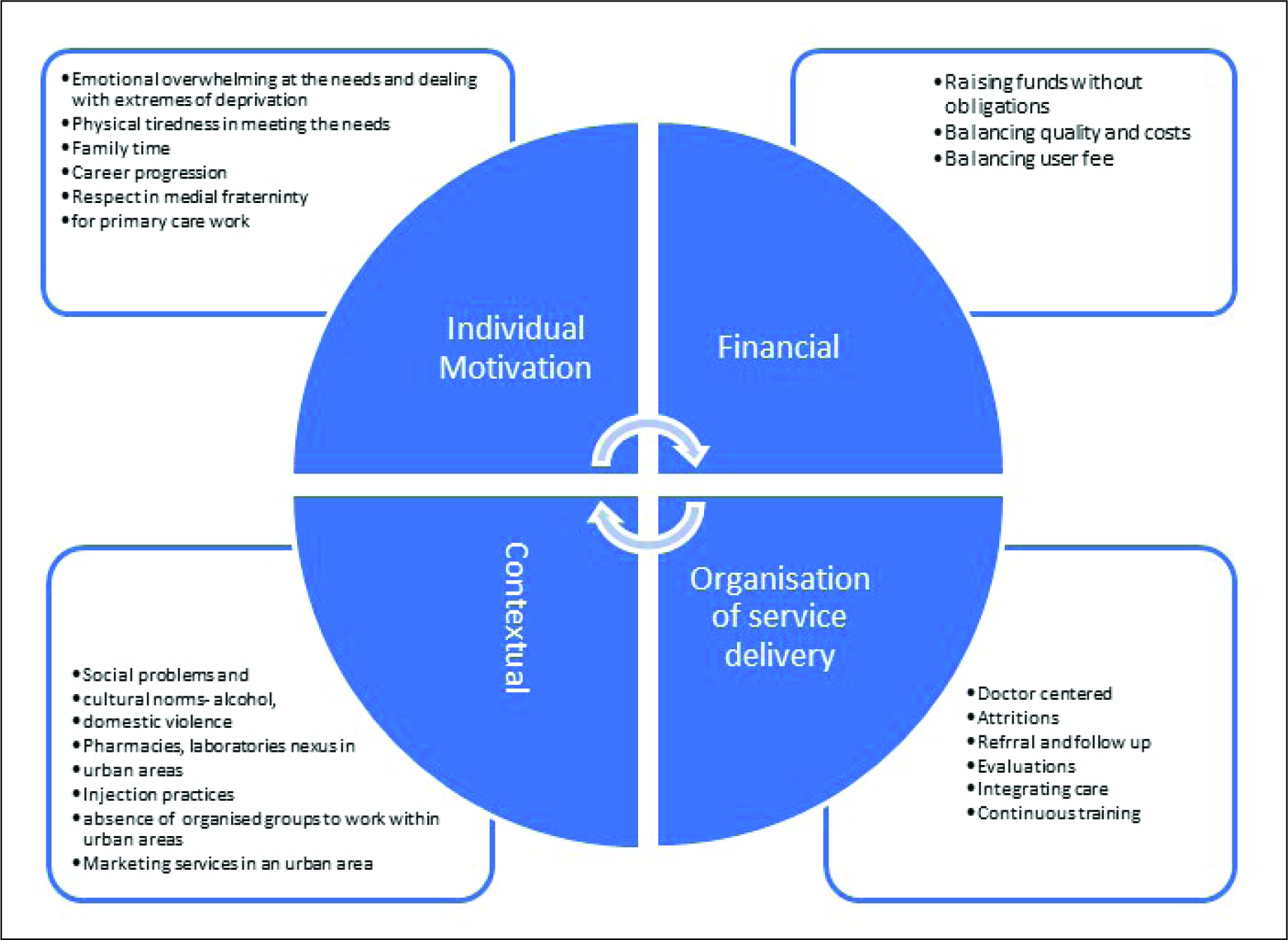
In the urban areas, the local context of competing with many different providers played a role. Ensuring ethical standards was a big challenge, influenced by the lack of regulation and direct marketing practices of pharmacies and laboratories:
This is a very complicated system, you have a lab which is directly marketing to a patient, I sent him for three tests, you are getting 52 tests done, now the main problem is, out of that 52 tests, in that 20 pages, he is showing me, look there is a black mark here, now you had a different problem and now I am looking at a different problem. So, the labs are marketing to the people directly, pharmacists are marketing to the people directly and so, the whole primary healthcare system is broken, we have no control, how can a lab, without a prescription just do tests—M10
Respect within the medical fraternity and lack of career progression are personal challenges doctors and other healthcare professionals face both in urban and rural areas. Financial resources for primary care are a consistent challenge in both urban and rural settings. The challenge in urban settings is not raising revenue or sustaining themselves financially but maintaining the balance in reaching out to all economic strata of the community.
In the organisation of primary healthcare services, referral to secondary and tertiary levels of care will be required, however, this was a challenge for all the cases in this study. Most spoke of informal networks, personal connections at secondary and tertiary level hospitals that they would use to ensure patients receive appropriate care. However, they acknowledged that many find it difficult to access and navigate care at the referral centres. Patients do return to the primary care facility after receiving interventions at the referral facility but more often fail to return:
You know, of course, this whole (referral system) can never become very smooth, because it is not in your control, despite your personal relations and your appeal to their better selves, there will always be, there are always gaps.—M2
The difficulties in referral are despite the clinical record for all patients. In some of the models there was a robust system to collect information at the household/family level within the catchment area. However, information across levels of care was challenging.
Each of the models studied had very varied measures to evaluate the work to assess impact. The CPHC performance indicators of access, coverage, health service indicators such as immunisation were not always systematically recorded or collected. The cases studied were dependent on other expressions of effectiveness which were not always quantifiable:
If you are looking at numbers, looking at numbers is definitely needed, because that is the only tangible thing that you can do, look at numbers, that is definitely needed but I think, even if your numbers are low, your numbers are not up to the mark but community has improved knowledge then those type of values should be taken for example, the involvement of the community for example in a discussion, how many people are actually voicing things should be considered.—M9
Discussion
In this study, major themes identified were regarding the organisation, financing and delivery of care as well as the main challenges in service delivery. Services should be comprehensive and not a fixed package, dialoguing with the community, addressing social determinants were themes related to the organisation of services. A major theme regarding the workforce was the need for more generalists and an orientation of training for health professionals towards CPHC. Financing of primary healthcare especially in the rural context is a major challenge and cannot be sustained from user fees; financial protection will be required to increase access. Lastly, leadership, values and organisational culture were critical in the delivery of good quality primary care.
Organisational culture and the values underlying primary healthcare have a very important role to play in realising the goal of CPHC. Values and organisational culture have often been referred to as the ‘software’ of service delivery and there is a growing awareness of its importance in shaping service delivery. CPHC envisioned at Alma Ata and reaffirmed at Astana in 2018 highlights a commitment to the fundamental right of every human being to the enjoyment of the highest attainable standard of health without distinction of any kind (WHO, 2018). Values in health systems have been conceptualised to underpin and determine all the other components of the health system including service delivery (van Olmen et al., 2012). The term ‘values’ is sometimes used to denote individual preferences (Shams et al., 2016) however, within health systems research it refers to the foundational normative beliefs underlying those preferences (Whyle & Olivier, 2020). This study found the underlying values of equity, social justice and service to the marginalised as important themes that shaped how the services were prioritised. It was also found that leadership of primary care teams that is relational contributes to a positive work culture that in turn contributes to the high motivation of individuals working at the primary care facilities. Team based care that values each member of the team and is oriented to whole person care was modelled by the leaders of successful primary care teams included in this study. There is a paucity of research that explores the underlying values and resultant culture in the Indian context. A recent study in Maharashtra, India highlighted the role of context including values in the implementation of primary healthcare. The study concluded that government PHCs despite having the infrastructure, drugs and equipment are unable to embody CPHC ideals (Ramani et al., 2019). Another study that explored primary healthcare for care of chronic conditions in rural south India highlighted the influence of hierarchies on service delivery (Lall et al., 2020). This research contributes to the understanding that focusing on underlying values and organisational cultures is a fundamental requirement of good quality primary care that should not be ignored (McWhinney, 1998). More research into the social organisation of PHCs, as well as in the testing of innovations to change and orient values towards CPHC, is required.
The findings of this study confirm the feasibility of a comprehensive range of services as opposed to a defined package of services for primary healthcare. Comprehensiveness refers to the provision of holistic and appropriate care across a broad spectrum of health problems, age ranges and treatment modalities and is associated with better patient experiences and decreased in patient service utilisation (Magnussen et al., 2017). Most of the case studies defined medical services based on the needs of the community, and responding to local needs-built trust and rapport between service providers and the community. Adapting to local needs and prioritising local needs instead of delivering a defined set of interventions for a set of health conditions demonstrated commitment to the community. There is a global emphasis on delivering comprehensive services at the primary level of healthcare. Global initiatives such as the PHCPI and the WHO Framework on Integrated People-Centred Health Services (IPHCS) have tried to define and measure CPHC specific to the context of LMICs (Bitton et al., 2019). Community engagement therefore is a crucial element in the delivery of CPHC (MacCormack, 1983). The IPHCS also emphasises this as an important strategic approach to achieving CPHC (WHO, 2016). In this research study, it was found that including the community in dialogues about healthcare was an important aspect of the community engagement strategy, which resulted in a focus on the social determinants of health.
The urban context in India is unique and most documented experiences in primary care delivery in India are in a rural setting. While principles can be applied across settings, the specifics of organising care for urban settings will be different. The rural model of hospital or health centre with outreach is not easy to replicate in urban areas. Social franchising or aggregation is a promising model and may be the way forward for the urban context. However, the effect of social franchising models for delivery of care has been mixed. Some studies report no difference in outcomes while others show improvements in health outcomes (Mohanan et al., 2016; Tougher et al., 2018). There are several examples of this model in India, and the experience can help develop a model to effectively deliver CPHC in urban areas. The lessons learnt about the social franchising model are related to the need for regulation and well-defined standards, ethical as well as quality standards. We found that family physicians are perhaps best suited as service providers in this model. Home visit based primary care in urban areas is impactful as it forces physicians to be cognizant of the social determinants of health. In both urban and rural contexts, we found generalists, including family medicine physicians were best suited. There is a need to raise the profile of generalists and reverse the generalist versus specialist imbalance in India.
The main challenges for the organisation of primary care that should be considered in the future design of primary care were maintaining and retrieving medical records, referral across healthcare levels and stable financing to ensure manpower, medicines and equipment consistently. Continuity of care is directly impacted due to a lack of records and referral follow up.
This study was limited by the ongoing pandemic, and it was not possible to conduct observations to triangulate the findings from the interviews. It was also difficult to get perspectives of patients and other team members as only the online mode was used for data collection. Both these would have added credibility to our findings. Secondary data collected in this study was dependent on whatever was available at the sites or was reported by the service provider. It was not possible to physically verify any of these reports. Since the context of each model is different in terms of the community they serve, the staff they have and services they provide, the lessons drawn from the study are context specific and may not be generalisable. However, the use of a theoretical framework to guide the inquiry enables us to draw lessons that may be applicable to other settings.
Conclusion
There is considerable experience with primary healthcare delivery in the private, non-governmental and public sectors of healthcare delivery in India. This study aimed to identify some lessons from non-governmental, not-for-profit CPHC models that can inform the strengthening of primary care delivery systems in India. This study used a qualitative approach to learn from local tacit knowledge and experiences of implementers in primary healthcare. We found two models for the delivery of healthcare services, in rural and urban contexts, respectively: the health centre and outreach model and the social franchising or chain of clinics model. The role and influence of values underlying the primary healthcare system should not be underestimated. Attention to teams, motivation, beliefs and values of the team are essential ingredients to impacting the health of the people. Reorientation of primary care teams to equity, social justice, respect for communities and responsibility for health of the community is required. Leadership of primary care to facilitate team-based care is essential to achieve the outcomes of CPHC. Lastly, a focus on quality of education to skill and equip workforce for primary care is a huge lacuna that needs to be systematically addressed. Challenges in delivering CPHC such as referral pathways and medical records will need contextual solutions and is an opportunity for further research. The move towards CPHC as in the recently launched Ayushman Bharat scheme in India is encouraging and its implementation would benefit from attention to the local knowledge of primary care implementers in India.
Footnotes
Acknowledgement
This study was funded by the Access Health International (AHI). We would like to acknowledge the help and support of the team at AHI, especially Maulik Chokshi and Arun Nair. We also would like to thank and acknowledge the inputs of Professor Sarang Deo and Preeti Singh at the Max Institute of Healthcare Management—ISB in the design and selection of cases in this study. We are grateful to the leaders of the organisations included in the study for their openness to discuss strengths and challenges in the delivery of CPHC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Access Health International (AHI).