
Abstract
The use of adequate reproductive healthcare services is critical to mothers and newborn babies. This study aimed to examine the facilitators and barriers to maternal healthcare utilisation in the Empowered Action Group (EAG) states. Data were drawn from the fourth round of the National Family Health Survey, 2015–16 (n = 103,984). In this study, full antenatal care (ANC), delivery assistance by the skilled birth attendant (SBA) and postnatal care (PNC) within 2 days of delivery were taken as indicators of maternity care. Overall, approximately 13% of women received full ANC, 69.4% were delivered by SBA and 57.7% had PNC within 2 days of delivery. The findings of this study reveal that urban residence, higher education, wealthier economic status, exposure to mass media and contraceptive use are the facilitators of maternal healthcare utilisation. On the contrary, low levels of education, poverty, marriage during childhood, having a large number of children, belonging to socioeconomically backward castes, having difficulties related to healthcare-seeking and unwanted pregnancies are some of the major barriers to the use of maternity care. This study suggests that policymakers and public health practitioners should design proper healthcare policies and programs to provide quality reproductive healthcare services, particularly among socio-economically vulnerable women.
Introduction
Globally, approximately 810 women die every day due to preventable causes that are related to complications from pregnancy and childbirth. Over 90% of all maternal deaths occur in low and lower-middle-income countries (World Health Organization [WHO], 2019). This high incidence of maternal mortality in low-income countries could be averted by adequate utilisation of maternal healthcare services. Maternal healthcare has three major components—antenatal care (ANC), delivery care, postnatal care (PNC). The World Health Organization (WHO) has recommended that continuum of care is essential for the survival of mothers and newborn babies (WHO, 2019). The United Nations’ (UN) Sustainable Development Goal (SDG)-3 aims to reduce maternal mortality to less than 70 per 100,000 live births and under-5 mortality to at least as low as 25 per 1000 live births and to ensure universal access to sexual and reproductive healthcare by 2030.
Previous studies have identified multiple factors of maternal healthcare services in low- and lower-middle-income countries. Among demographic factors, women’s age, age at marriage and birth order are considered as important factors (Paul & Chouhan, 2020; Rai et al., 2012; Singh et al., 2012a, 2012b). Previous studies also found that the use of maternal health services significantly differs by rural–urban residence (Celik & Hotchkiss, 2000; Chanda et al., 2020). Education and wealth status are frequently reported as strong predictors of maternity care in many earlier studies (Babalola & Fatusi, 2009; Bhatia & Cleland, 1995; Paul & Chouhan, 2020; Rai et al., 2013; Singh et al., 2012a, 2012b; Terekegn et al., 2014). For instance, Paul and Chouhan (2020) carried out a cross-sectional study using the National Family Health Survey (NFHS-4) data to assess the socio-demographic factors of maternal healthcare services where it is yielded that education and wealth status are the most prominent determinants of maternity care services. In addition, caste and religion are also considered as important structural factors that determine the use of maternal healthcare services which is evident from past research (Navaneetham & Dharmalingam, 2002; Singh et al., 2012a, 2012b, 2014, 2019). Studies also indicated the role of the village and community-level factors such as school facility, electricity, transport facility and distance to the health facility in determining maternity care services (Mistry et al., 2009; Singh et al., 2014; Vidler et al., 2016). Mass media exposure and women’s autonomy or decision-making power are identified as key facilitators of maternal healthcare utilisation (Mistry et al., 2009; Singh et al., 2012a, 2012b; Terekegn et al., 2014; Vidler et al., 2016). The influence of geographical region also emerged as a crucial determinant of maternity care (Mistry et al., 2009; Paul, 2020; Singh et al., 2012a, 2012b).
Since independence, India has started several family welfare programs to strengthen maternal and child healthcare services in the country. In 1997, the Reproductive and Child Health (RCH) program was initiated to improve the quality and utilisation of maternal healthcare services. This integrated program also aimed to provide child survival services for newborns and infants. In addition, the government of India has started National Rural Health Mission (NRHM), in 2005 to provide equitable, affordable and quality healthcare to the rural women, especially to the vulnerable groups. In addition, Janani Suraksha Yojana (JSY) is implemented as one of the safe motherhood interventions under the umbrella of NRHM to reduce maternal and neonatal mortality by promoting institutional deliveries among poor pregnant women (Gopalan & Varatharajan, 2012).
Despite various interventions made by the government, a considerable proportion of women are still lagging in the use of maternal healthcare, particularly the marginalised section of women. Earlier studies have indicated that complications related to pregnancy and childbirth which are the leading causes of maternal mortality and adverse birth outcomes, such as preterm births and low birth weight and neonatal mortality are associated with inadequate utilisation of maternal healthcare services (Singh et al., 2012; Thaddeus & Maine, 1994). Although India has made considerable achievements in reducing maternal mortality over the last few decades, it remains widespread in socioeconomically backward states (SRS, 2019).
We conducted the current study in the most socioeconomically backward states of India, referred to as the Empowered Action Group (EAG) states. The incidence of maternal was highly prevalent in the EAG states, ranging from 216 per 100,000 live births in Uttar Pradesh to 76 per 100,000 live births in Jharkhand in 2015–2017 (SRS, 2019). Based on the current maternal and child mortality levels, the EAG states required an accelerated improvement to achieve the targets of Sustainable Development Goal (SDG)-3. Therefore, adequate utilisation of maternal healthcare is highly important in the study setting. Most of the earlier studies conducted in India and South Asian countries primarily focused on demographic and socioeconomic factors of maternal healthcare utilisation. Recently, only a few studies investigated the enablers and barriers to maternal healthcare services, however, limited to the utilisation of ANC services (Chanda et al., 2020; Ogbo et al., 2019). In the present study, we made a comprehensive assessment to examine the facilitators of and barriers to maternal healthcare utilisation in the EAG states, using the most recent nationally representative demographic survey of India.
Methods
Data Source
We used data from the fourth round of the National Family Health Survey (NFHS-4), conducted in 2015–2016. The NFHS-4 is a large-scale, nationally representative population and health survey conducted as part of the demographic and health survey (DHS) program. The NFHS-4 was conducted under the stewardship of the Ministry of Health and Family Welfare (MoHFW), Government of India and the International Institute for Population Sciences (IIPS) was designated as the nodal agency to conduct the survey. Technical assistance was provided by the ICF International of Calverton, Maryland, USA, and the survey was funded by the U.S. Agency for International Development (USAID) and various other organisations. This survey covered 601,509 households, 699,686 women aged 15–49 years with a response rate of 97%, and 112,122 men aged 15–54 years with a response rate of 92%. The samples were collected using a two-stage stratified sampling design. The 2011 Census of India was used as sampling frame of this survey. Villages are served as primary sampling units (PSU) in rural areas and census enumeration blocks (CEB) considered as PSU in urban areas. The fieldwork was completed in 28,522 clusters. In the first stage, the clusters were selected using the method of probability proportional to size (PPS). In the second stage, a complete household mapping and listing were done in the selected clusters and 22 households were selected with an equal opportunity systematic selection from the household listing. The sampling design and survey procedure have been discussed in detail in the national report of NFHS-4 (IIPS & ICF, 2017). We retrieved the data from the DHS program website which is publicly available and can be accessed at
Study Setting and Sample Size
The present study was carried out in the EAG states, which is considered as the most socioeconomically backward region of the country. The EAG region comprises eight administrative states, namely Bihar, Chhattisgarh, Jharkhand, Odisha, Madhya Pradesh, Rajasthan, Uttar Pradesh and Uttarakhand. These EAG states are characterised by a high level of poverty and illiteracy, a high burden of malnourished children, and an alarming rate of maternal and neonatal mortality. The NFHS-4 collected information regarding the utilisation of maternal healthcare for 190,898 ever-married women aged 15–49 years who had a birth in the past 5 years preceding the survey for the whole country. Among these women, the EAG states comprised 103,984 last birth women in the past 5 years. Therefore, we restricted our analysis for 103,984 sample women with the most recent birth in the past 5 years prior to the survey.
Analytical Framework
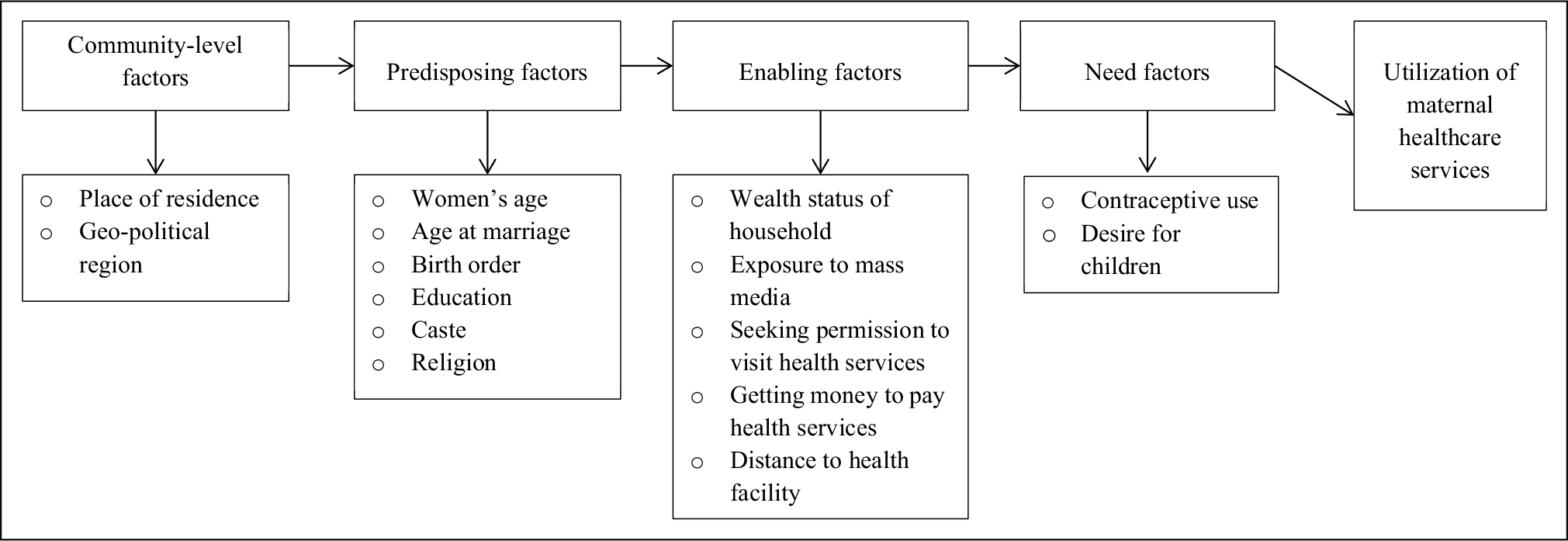
We adopted Andersen’s behavioural model to assess the factors associated with the utilisation of maternal healthcare services (Andersen, 1995). This study selected a wide range of factors that have a potential influence on maternity care services. The selection of these variables is based on the evidence of earlier studies. The selected factors are categorised into four groups: (a) community-level factors, (b) predisposing factors, (c) enabling factors and (d) need factors. The framework of this present study is provided in Figure 1.
Dependent Variables
Utilisation of maternal healthcare services is the outcome of interest in this study. For this study, full ANC, delivery assisted by skilled birth attendants (SBA) and PNC of mothers within 2 days of delivery were selected to determine the utilisation of maternal healthcare services. Women who received at least four ANC visits, at least one tetanus toxoid (TT) injection and iron-folic acid tablets or syrup for 100 or more days are considered to have full ANC. Skilled health personnel includes doctor, auxiliary nurse midwife, nurse, midwife, lady health visitor and other health personnel. PNC check-up within 2 days of delivery was taken as a PNC indicator.
Independent Variables
A wide range of independent variables was included to examine community-level, predisposing, enabling and need factors associated with the utilisation of maternal healthcare services. Community-level variables include place of residence and geo-political region. Place of residence was categorised as urban and rural. Earlier studies have yielded the importance of geopolitical regions on maternal healthcare services (Singh et al., 2012a, 2014). Geo-political region was considered as eight administrative divisions of the EAG states: Bihar, Chhattisgarh, Jharkhand, Odisha, Madhya Pradesh, Rajasthan, Uttar Pradesh and Uttarakhand.
Predisposing factors include women’s age, age at marriage, birth order, education, caste and religion. Studies have indicated that maternal age is significantly associated with the utilisation of maternal healthcare services (Paul & Chouhan, 2020; Singh et al., 2012a). In this study, women’s age was categorised into three groups: <20 years, 20–34 years and 35+ years. The influence of child marriage on maternity care has been reported in many prior studies (Paul & Chouhan, 2019; Sekine & Carter, 2019). Child marriage is defined as any formal or informal marriage under the age of 18 (for women) and 25 (for men). Here, we intended to determine the impact of child marriage on the utilisation of maternal healthcare. For this purpose, age at marriage of mothers was classified as below 18 years and 18 years or above. Studies also indicated that birth order is an important influential factor in maternal healthcare (Singh et al., 2012b, 2014). Birth order variable was categorised into first, second, third and fourth or more. Several studies in India have demonstrated that education is an important determinant of maternity care services (Bhatia & Cleland, 1995; Navaneetham & Dharmalingam, 2002; Paul & Chouhan, 2020). Educational attainment of women was classified as no education, primary, secondary and higher. In addition, the influence of caste and religion also indicated by many studies conducted in India (Navaneetham & Dharmalingam, 2002; Paul & Chouhan, 2020; Singh et al., 2012a, 2014). Caste variable was divided into four groups: forward caste, Scheduled Caste, Scheduled Tribe and Other Backward Classes. Religion affiliation of women was classified as Hindu, Muslim and others.
Among enabling factors, women’s exposure to mass media and various accessibility-related factors were included. Mass media exposure was derived from three variables: frequency of listening to the radio, frequency of reading newspapers/magazines and frequency of watching television. Each mass media variable was dichotomised into yes and no to determine the influence of each mass media exposure on maternal healthcare services. Other enabling factors include permission to visit health services, getting money to pay for health services and distance to the health services. These factors would reflect the accessibility of healthcare services in the study setting.
Contraceptive use and desire for children were included as need factors. The contraceptive use variable was dichotomised into not using and using contraceptives. Child wantedness/desire for children was categorised as wanted then, wanted later and wanted no more.
Statistical Analyses
Descriptive statistics were carried out to understand the distribution of study participants. Bivariate percentage distribution was estimated between dependent and independent variables. The significance level of association between dependent and independent variables was tested by Pearson’s chi-square statistics. Finally, binary logistic regression models were executed to assess the factors associated with all three indicators of maternal healthcare services. The results of binary logistic regression analyses were presented by odds ratio (OR) with 95% confidence interval (CI). The significance level for logistic regression was set at P <0.05. Any collinearity between independent variables has been checked and none was evident in the analysis. The appropriate sample weight has been used to perform the analysis. All statistical analyses were carried out using STATA version 12.1 (StataCorp LP, College Station, TX, USA).
Results
Background Characteristics of Respondents
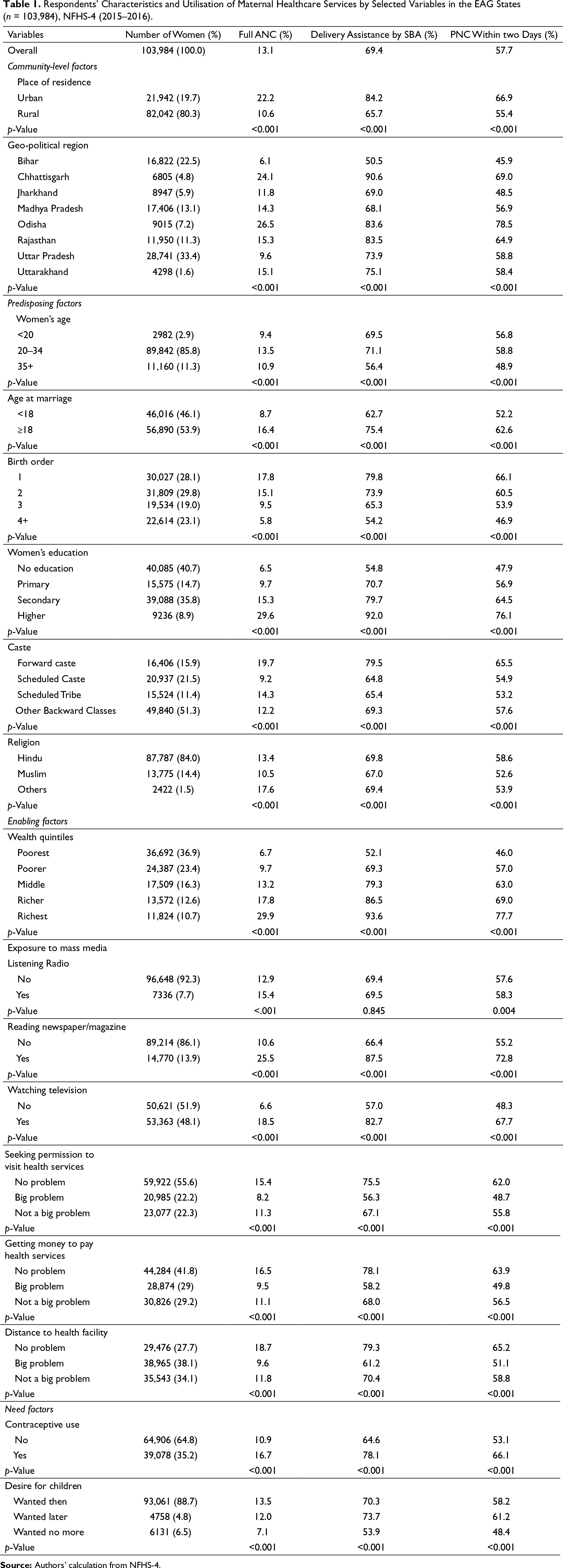
In this study, a total of 103,984 ever-married women with the most recent live birth were included as study participants (Table 1). The majority of respondents (80.3%) resided in rural areas. Approximately one-third of the respondents (33.4%) lived in Uttar Pradesh, followed by Bihar (22.5%) and Madhya Pradesh (13.1%), while Uttarakhand (1.6%) had the lowest share of study participants. Approximately 85.8% of women belonged to the age group of 20–34 years. A large proportion of women (46.1%) were married under the age of 18. Women with first (28.1%) and second-order birth (29.8%) constitute nearly approximately one-third of all respondents. A substantial proportion of women (40.7%) had no formal education, while only approximately 9% of women had higher level of education. In regard to caste group, over half of the respondents (51.3%) belonged to Other Backward Classes. Most of the women were Hindu (84%). It is noticed that the distribution of participants decreased from bottom to upper quintile of household wealth where over one-third of women (36.9%) were from the poorest quintile, while only 10.7% of women belonged to the richest household wealth quintile. Regarding exposure to mass media, most of the respondents had exposure to the radio (92.3%) and newspapers/magazines (86.1%). Moreover, nearly half of the women (48.1%) had exposure to television. Approximately 55.6% of women reportedly have no problem in seeking permission to visit health services. Over one-third of women (38.1%) reported that distance to the health facility was a big problem. Slightly above one-third of women (35.2%) had used contraceptives. The majority of women (88.7%) reported that they desired for their last child.
Respondents’ Characteristics and Utilisation of Maternal Healthcare Services by Selected Variables in the EAG States(n = 103,984), NFHS-4 (2015–2016).
Utilisation of Maternal Healthcare Services by Various Factors
Overall, only approximately 13% of women received full ANC, 69.4% of women delivered by SBA and 57.7% of women had PNC within 2 days of delivery (Table 1). We found significant differences in all three indicators of maternal healthcare services by various community-level, predisposing, enabling and need factors. The proportion of full ANC, delivery assistance by SBA and PNC was significantly lower among women residing in rural areas compared to its urban counterparts. The percentage of women using maternal health services also differed across geopolitical regions.
Women’s age, age at marriage, birth order, women’s education and wealth quintile were significantly associated with Full ANC, SBA and PNC of women. The proportion of maternal healthcare utilisation was found to be lower among women who married below 18 years, had higher birth order, uneducated and economically poorer section of women. The results also showed that women’s exposure to mass media and contraceptive use were positively correlated with the utilisation of maternal health services.
Logistic Regression Analyses
We carried out bivariate and multivariate logistic regression models to examine the community-level, predisposing, enabling and need factors associated with full ANC (Table 2), delivery assisted by SBA (Table 3) and PNC within 2 days of delivery (Table 4).
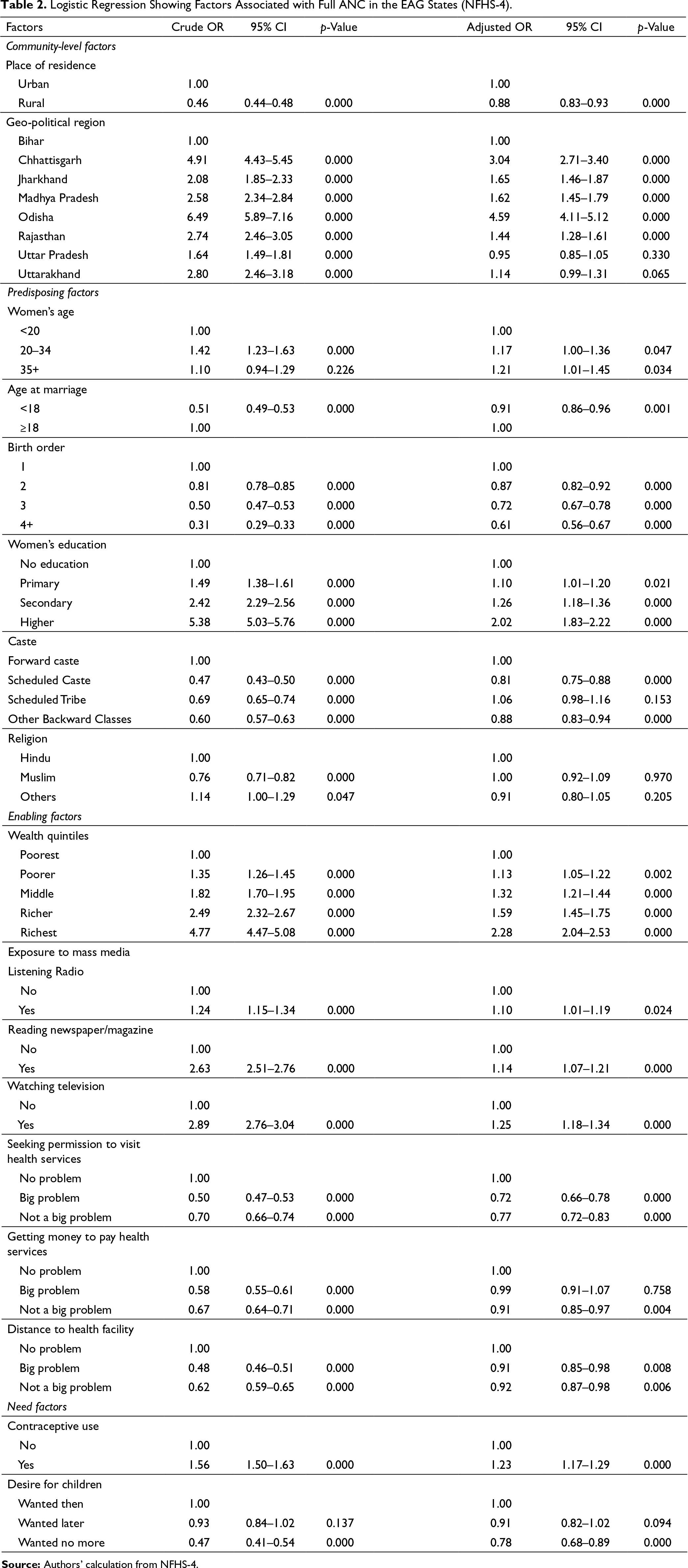
Logistic Regression Showing Factors Associated with Full ANC in the EAG States (NFHS-4).
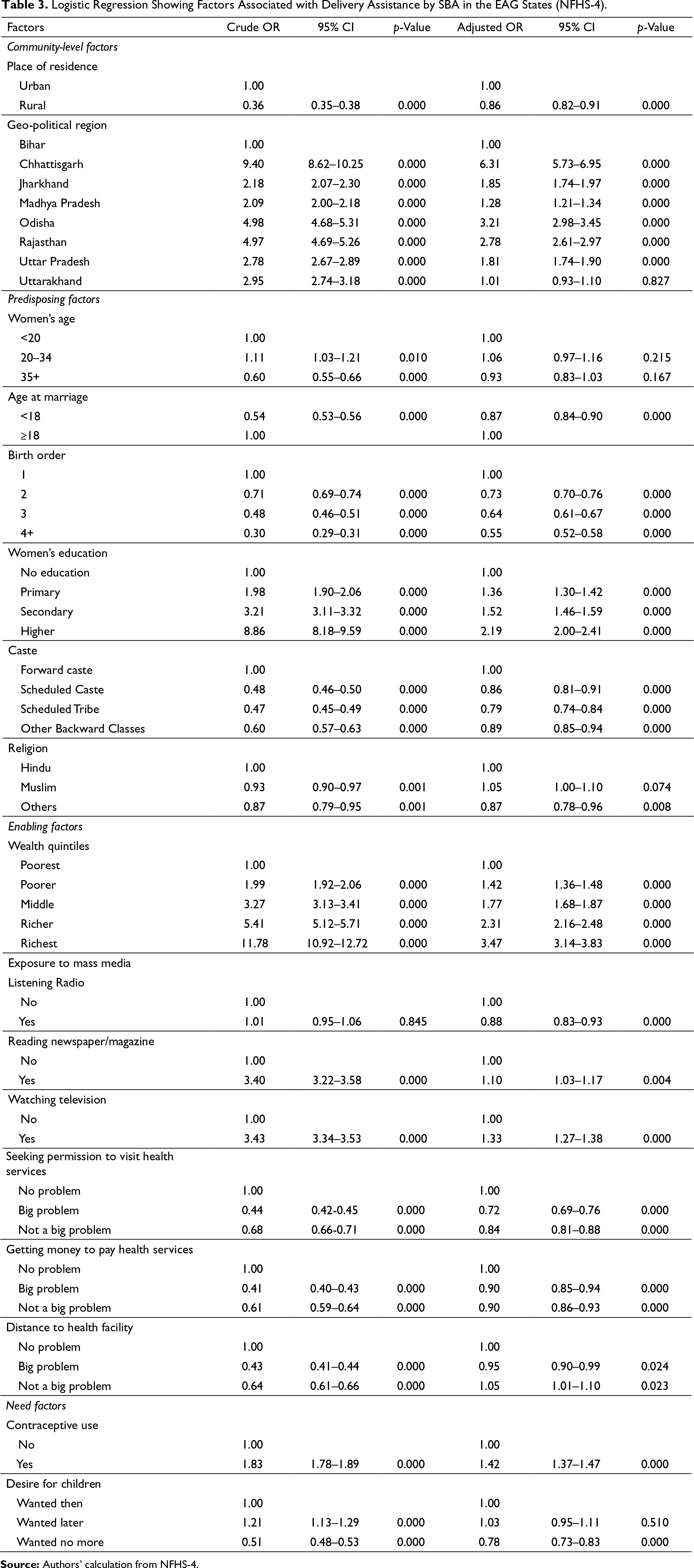
Logistic Regression Showing Factors Associated with Delivery Assistance by SBA in the EAG States (NFHS-4).
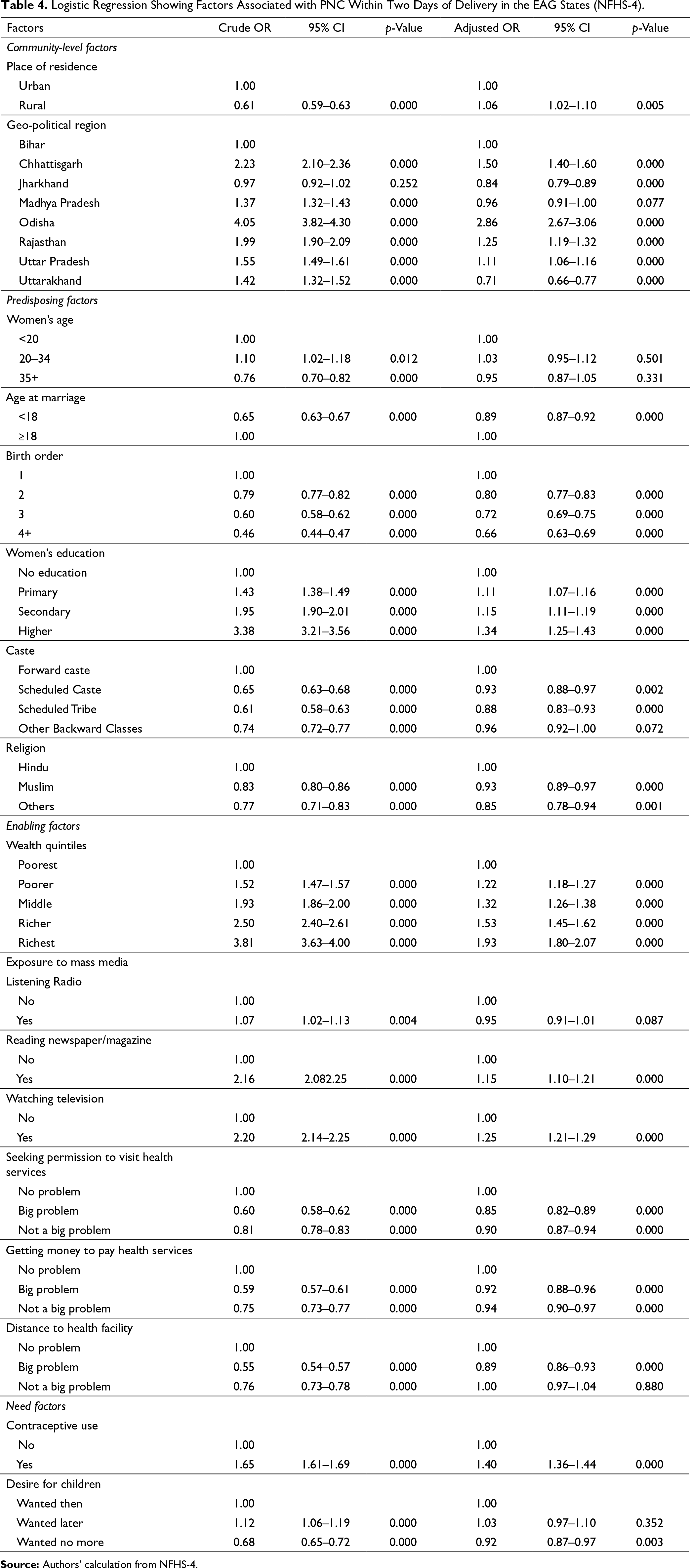
Logistic Regression Showing Factors Associated with PNC Within Two Days of Delivery in the EAG States (NFHS-4).
Factors Associated with Full ANC
Women living in rural areas were less likely to have full ANC (AOR: 0.88; 95% CI: 0.83–0.93) compared to women who lived in urban areas. Compared to women from Bihar, women resided in Chhattisgarh, Jharkhand, Madhya Pradesh, Odisha and Rajasthan were 3.04 (95% CI: 2.71–3.40; p < 0.001), 1.65 (95% CI: 1.46–1.87; p < 0.001), 1.62 (95% CI: 1.45–1.79; p < 0.001), 4.59 (95% CI: 4.11–5.12; p < 0.001) and 1.44 (95% CI: 1.28–1.61; p < 0.001) times more likely to receive full ANC, respectively. Women in the age group of 20–34 years and 35+ years were 1.17 (95% CI: 1.00–1.36; p = 0.047) and 1.21 (95% CI: 1.01–1.45; p = 0.034) times more likely to have full ANC compared to women aged <20 years. The likelihood of full ANC was significantly lower among women who married under the age of 18 (AOR: 0.91; 95% CI: 0.86–0.96; p = 0.001) than women who married at 18 years or older. The odds of full ANC decreased with mothers having higher birth order children. Women’s education was found to be an important determinant of full ANC. Women with primary, secondary and higher education were 1.10 (95% CI: 1.01–1.20; p = 0.021), 1.26 (95% CI: 1.18–1.36; p < 0.001) and 2.02 (95% CI: 1.83–2.22; p < 0.001) times more likely to receive full ANC, respectively, compared to women with no education. Women belonged to Scheduled Caste (AOR: 0.81; 95% CI: 0.75–0.88) and Other Backward Classes (AOR: 0.88; 95% CI: 0.83–0.94) were less likely to attend full ANC compared to forward caste women. Household wealth quintile was found to be a vital predictor of full ANC. Women in the richest quintile were associated with more than twice an increased likelihood of receiving full ANC (AOR: 2.28; 95% CI: 2.04–2.53; p < 0.001) than women in the poorest quintile. Women’s mass media exposure was positively correlated with attending full ANC. Women who exposed to radio, newspapers/magazines and television were 1.10 (95% CI: 1.01–1.19; p = 0.0024), 1.14 (95% CI: 1.07–1.21; p < 0.001) and 1.25 (95% CI: 1.18–1.34; p < 0.001) times more likely to attend full ANC, respectively, than those who did not expose to mass media. Women who reported having problems in seeking permission to visit healthcare, getting money to pay for health services and distance to the health facility were less likely to attend full ANC compared to women who had no such problems. The use of contraceptives was associated with increased odds of full ANC (AOR: 1.23; 95% CI: 1.17–1.29; p < 0.001) among women. Women who wanted no more child were less likely to attend full ANC (AOR: 0.78; 95% CI: 0.82–1.02; p < 0.001) than those who wanted a child.
Factors Associated with Delivery Assistance by SBA
The odds of SBA for women living in rural areas were significantly lower as compared to their urban counterparts. Women resided in Chhattisgarh, Jharkhand, Madhya Pradesh, Odisha, Rajasthan and Uttar Pradesh were 6.31 (95% CI: 5.73–6.95; p < 0.001), 1.85 (95% CI: 1.74–1.97; p < 0.001), 1.28 (95% CI: 1.21–1.34; p < 0.001), 3.21 (95% CI: 2.98–3.45; p < 0.001), 2.78 (95% CI: 2.61–2.97; p < 0.001) and 1.81 (95% CI: 1.74–1.90; p < 0.001) times more likely to deliver by SBA, respectively, compared to women from Bihar. Women who married below the age of 18 years were less likely to attend by SBA (AOR: 0.87; 95% CI: 0.84–0.90; p < 0.001) than those who married at 18 years or older. The odds of SBA decreased with women having higher-order children. Women having 4+ order children were 45% less likely to deliver by SBA (AOR: 0.55; 95% 0.52–0.58; p < 0.001) compared to women who had the first order child. Women’s education was found to be a strong predictor of SBA. Women with higher education were associated with more than twice an increased likelihood of SBA than those who had no formal education. Compared to forward caste women, women in Scheduled Caste, Scheduled Tribe and Other Backward Classes were less likely to deliver by SBA. Among enabling factors, wealth quintile was found to be an important determinant of SBA where women from the richest quintile were 3.47 times (95% CI: 3.14–3.83; p < 0.001) more likely to deliver by SBA than women from the poorest quintile. Moreover, women’s exposure to newspapers / magazines was positively associated with SBA. Women who reported having problems in seeking permission to visit health services and getting money to pay for health services were less likely to attend by SBA compared to women who did not have those difficulties. Among need factors, women who used contraceptives were 1.42 times (95% CI: 1.37–1.47; p < 0.001) more likely to deliver by SBA than women who did not use contraceptives. Furthermore, women who wanted no more children were less likely to attend by SBA (AOR: 0.78; 95% CI: 0.73–0.83; p < 0.001) compared to women who wanted children.
Factors Associated with PNC Within Two Days of Delivery
Women living in Chhattisgarh (AOR: 1.50; 95% CI: 1.02–1.10), Odisha (AOR: 2.86; 95% CI: 2.67–3.06), Rajasthan (AOR: 1.25; 95% CI: 1.19–1.32) and Uttar Pradesh (AOR: 1.11; 95% CI: 1.06–1.16) were more likely to attend PNC, while women from Jharkhand (AOR: 0.84; 95% CI: 0.79–0.89) and Uttarakhand (AOR: 0.71; 95% CI: 0.66–0.77) were less likely to attend PNC than women from Bihar. Among predisposing factors, age at marriage, birth order, women’s education, caste and religion were significantly associated with PNC of mothers. Women who married prior to 18 years were 11% less likely to attend PNC (AOR: 0.89; 95% CI: 0.87–0.92) than women who married at 18 years or later. Women with 4+ birth order were 34% less likely to have PNC (AOR: 0.66; 95% CI: 0.63–0.69) compared to women having a first-order child. Women who had higher education were 1.34 times (95% CI: 1.25–1.43) more likely to attend PNC than women who had no education. Compared to forward caste women, women belonged to Scheduled Caste (AOR: 0.93; 95% CI: 0.88–0.97; p = 0.002) and Scheduled Tribe (AOR: 0.88; 95% CI: 0.83–0.92; p < 0.001) were less likely to have PNC. Moreover, compared to Hindu women, women affiliated to Muslims (AOR: 0.93; 95% CI: 0.89–0.97; p < 0.001) and others religion (AOR: 0.85; 95% CI: 0.78–0.94; p = 0.001) were less likely to have PNC. The odds of PNC increased from bottom to upper quintile of household wealth. Women in the richest quintile were associated with an almost two-fold increased likelihood of PNC (AOR: 1.93; 95% CI: 1.80–2.07) compared to women in the poorest quintile. In regard to mass media exposure, women who had exposure to newspapers/magazines and television were associated with 15% (AOR: 1.15; 95% CI: 1.10–1.21) and 25% (AOR: 1.25; 95% CI: 1.21–1.29) higher likelihood of PNC, respectively, than those who had no exposure to such media. Women who reported having difficulties in seeking permission to visit health services and getting money to pay for health services were less likely to attend PNC than women who reported no such problems. Similarly, women who had big problems regarding distance to the health facility were less likely to have PNC compared to women who had no problems. Regarding need factors, contraceptive use increased the likelihood of PNC by 40% (AOR: 1.40; 95% CI: 1.36–1.44; p < 0.001). Moreover, women who wanted no more children were less likely to attend PNC (AOR: 0.92; 95% CI: 0.87–0.97; p = 0.003) than women who wanted children.
Discussion
This study has investigated the community-level, predisposing, enabling, and need factors associated with full ANC, delivery assisted by SBA and PNC within 2 days of delivery. The findings of this study reveal that approximately 13% of women received full ANC, 69.4% of women delivered by SBA and 57.7% had PNC check-ups in the EAG states. It is evidenced that the level of maternal healthcare utilisation is substantially lower in the EAG states compared to the national average (IIPS & ICF, 2017; Paul & Chouhan, 2020).
Considering community-level factors of maternal healthcare utilisation, the findings reveal that women living in rural areas were less likely to receive maternal healthcare services than their urban counterparts. Rural–urban differences in maternal healthcare services have also been reported in other studies (Paul & Chouhan, 2020; Singh et al., 2012). The lower access to maternal healthcare in rural areas could be due to lack of healthcare facilities, unavailability of trained health personnel, lack of medicine in the public healthcare centre, least access to information and lack of transport facility. On the contrary, better healthcare at both public and private facilities, greater access to health information and better social amenities contributed to higher use of healthcare services in urban areas. Maternal healthcare use also differed across geopolitical regions. Women residing in Chhattisgarh, Jharkhand, Madhya Pradesh, Odisha and Rajasthan were more likely to attend full ANC and SBA compared to women from Bihar. Similarly, the likelihood of PNC utilisation was higher among women from Chhattisgarh, Odisha, Rajasthan and Uttar Pradesh, while women from Jharkhand, Madhya Pradesh and Uttarakhand were less likely to receive PNC than women residing in Bihar. Differential use of maternity care across geopolitical regions may be due to state-specific differences in economy, education, women’s autonomy, health infrastructure and accessibility and availability of healthcare facilities.
Among predisposing factors, women’s age at marriage, birth order, education and caste were significantly associated with all the three components of maternal healthcare services. The findings reveal that women who married before 18 years of age were less likely to have maternal health care services compared to women who married during their adulthood. This finding is in line with several other studies (Paul & Chouhan, 2019, 2020; Singh et al., 2012a). It is evidenced that women who married in childhood have lower educational attainment and are more likely to live in poverty (Paul, 2019; UNICEF, 2005). Moreover, child married women have a low level of decision-making power regarding their healthcare, which further could result in lower access to healthcare facilities (Paul & Chouhan, 2019). Education was found to be an important facilitator of maternity care services. Women having higher education were more likely to receive full ANC, SBA and PNC check-ups compared to women who had no formal education. This finding is in the line of several earlier studies conducted in India and other developing countries (Ahmed et al., 2010; Celik & Hotchkiss, 2000; Navaneethem & Dharmalingam, 2002; Singh et al., 2012a). Educated women are more aware of the implications of healthcare use than their uneducated counterparts. Moreover, highly educated women could make decisions on healthcare that may have a positive influence on healthcare utilisation. Furthermore, caste and religion are important structural factors which found to have a significant influence on maternal healthcare services in the present study. The results reveal that women who belonged to Scheduled Caste and Other Backward Classes were less likely to access full ANC service compared to forward caste women. Similarly, women belonging in socio-economically backward caste groups had a lower likelihood of SBA and PNC than forward caste women. A previous study conducted in India also found similar results (Singh et al., 2012b).Our study also found that Muslim women were less likely to receive PNC service than women affiliated to Hindu religion. This finding is also in accordance with a previous study of India (Paul, 2020).
Among enabling factors, household wealth quintile, exposure to mass media and various accessibility-related factors were significantly associated with the utilisation of maternal healthcare services. Wealth status had a strong positive relationship with maternity care services. Women from wealthier economic strata were more likely to have full ANC, SBA and PNC services compared to economically weaker women. This finding is aligned with many previous studies (Ahmed et al., 2010; Paul & Chouhan, 2020; Singh et al., 2012a). A possible explanation is that wealthier women generally have greater access to healthcare facilities because rich families can spend a higher proportion of their earnings on healthcare compared to poor families (Paul, 2020; Paul & Chouhan, 2020). The findings of our study also highlighted the importance of mass media (radio, newspapers / magazine and television) in maternal healthcare utilisation. Likewise, several prior studies reported a positive impact of mass media on maternal healthcare utilisation (Paul & Chouhan, 2020; Rai et al., 2012; Singh et al., 2012a). In addition, seeking permission to visit health services, getting money to pay the health services and distance to health facility have a significant influence on the use of maternity care. An earlier study conducted in rural India found that women’s autonomy and distance to health facility have a significant impact on maternal health service utilisation (Mistry et al., 2009). Our study underscores the need to improve the decision-making autonomy of women in the household and to reach information about the importance of healthcare use through awareness campaigns, especially among disadvantaged groups of women.
Our study also found that the use of contraceptives was operated as a facilitator of maternal healthcare services. Women who used contraception were more likely to attend for maternity care services. This finding is also aligned with a previous study conducted in India where contractive use acted as an enabler of ANC utilisation (Ogbo et al., 2019). This finding is suggesting for greater access to contraceptive methods among reproductive women, particularly among socio-economically vulnerable women. Similarly, women’s desire for children was found to be a significant determinant of maternal healthcare utilisation. Consistent with past research (Paul, 2020; Ogbo et al., 2019), our study also found that women who did not desire children were less likely to attend for maternity care services compared to women who had a desire for children.
Strengths and Limitations
This study used nationally representative data with a large number of samples. Due to an adequate number of samples, region- and state-specific analysis could be done with high precision. This study provides evidence on various factors of maternal healthcare services for the most socio-economically backward region of India. Therefore, the study provides an opportunity for policymakers and public health practitioners to make effective interventions to address the underutilisation of maternal healthcare services among the vulnerable section of women.
This study also has some limitations. First, this is cross-sectional research; therefore, a causal relationship could not be established between the dependent and independent variables in this study. Second, data are self-reported which are prone to recall bias and social desirability bias. Indian society is by and large a male-dominated patriarchal society. Therefore, maternal healthcare-seeking could be influenced by various cultural and behavioural factors. We could not include those factors in the analysis due to the paucity of information in the dataset.
Conclusion
This study highlights that the utilisation of maternal healthcare services remains poor in the EAG states of India. The findings reveal that urban residence, higher education, wealthier economic status, exposure to mass media and contraceptive use are the facilitators of maternal healthcare utilisation. On the other hand, low levels of education, poverty, marriage during childhood, having a large number of children, belonging to socioeconomically backward castes, having difficulties related to healthcare-seeking and unwanted pregnancies are some of the major barriers to the use of maternity care. The findings of this study suggest that increasing access to female education, prevention of child marriage, promoting women’s autonomy and addressing socioeconomic vulnerabilities are required in order to improve the utilisation of maternal healthcare services. Policymakers and public health practitioners should design proper healthcare policies and programs to provide quality reproductive healthcare services, particularly among socio-economically vulnerable women.
Footnotes
Data Availability Statement
The data that support the findings of this study are openly available in the Demographic Health Survey (DHS) Program at
Declaration of Conflicting of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Statement
The ethical approval of the National Family Health Survey (NFHS-4) was obtained from ethics review board of International Institute for Population Sciences (IIPS), Mumbai. This survey was also reviewed and approved by ICF International Review Board (IRB). Respondents were provided written consent to participate during the survey.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.