
Abstract
This exploratory study aims to assess Africa’s lagging position in global health in relation to some healthcare infrastructure before critically examining the situation of Africa in the light of pressing COVID-19 healthcare infrastructural needs in terms of the number of hospital beds, intensive care units beds and ventilators per 100,000 people. A comparative analysis is provided to showcase which regions are leading in the health facilities in the world in general and Africa, in particular, as well as countries that are lagging in the attendant healthcare facilities. Analytical insights are provided to illustrate that the COVID-19 pandemic has revealed how Africa cannot reach most Sustainable Development Goals (SDGs), especially SDG-3 on health and well-being. Moreover, corresponding inferences suggest that the continent is unprepared for future pandemics in terms of health facilities.
Introduction
At the time of writing, the COVID-19 pandemic is spreading in the world at an alarming rate of contamination. Fortunately, in Africa, the number of deaths and positive cases has not been consistent with the expectations of most scholars and policymakers such as World Health Organization (WHO) authorities. However, recently, the population of the continent has been concerned that COVID-19 new cases and severe infections are accelerating especially given that the pandemic is threatening fragile health systems (Asongu et al., 2021, 2020; Diop et al., 2020). Mcaffrey (2020) in April 2020 established that Sierra Leone, the Central African Republic and Burkina Faso had one, three and eleven ventilator(s), respectively. While the fragility of Africa’s health system is no secret, the pandemic has exposed the true face of healthcare infrastructures. The present exploratory study aims to assess Africa’s lagging position in global health in relation to healthcare infrastructure before critically examining the situation of Africa in the light of pressing COVID-19 healthcare infrastructural needs in terms of the number of hospital beds, intensive care unit (ICU) beds and ventilators per 100,000 people.
The positioning of the present study departs from the extant literature which has not been premised on a critical assessment of the healthcare infrastructure in Africa. Accordingly, a large body of the extant studies has been concerned with how governments have responded to the COVID-19 pandemic on the one hand and the socio-economic consequences of the pandemic on the other (Agbe, 2020; Bisong et al., 2020; Farayabi & Asongu, 2020; Nicola et al., 2020; Ozili, 2020; Price & van Holm, 2020). Some examples of the extant studies include; Amankwah-Amoah (2020) who has focused on how the environment has been affected by the COVID-19 crisis; Obeng-Odoom (2020) assessing nexuses between the novel coronavirus, income distribution and social stratification; Ataguba (2020) on the scholarly and policy perspectives on the economic ramifications of the COVID-19 crisis; Ozili (2020) examining the avenues, policy initiatives and socio-economic measures that are associated with the underlying pandemic; Bisong et al. (2020) on the incidence of the crisis on remittances flows; Agbe (2020) who has examined how the pandemic has affected childhood poverty and; Adekola et al. (in press) and Odeyemi et al. (2020) who focus on the modelling of infectious diseases by means of mathematics as well as laboratory responses to the COVID-19 pandemic.
In the light of the above, to the best of our knowledge and as far as we have reviewed, the extant literature has not focused on the problem statement being envisaged by the current study which aims to assess the lagging status of Africa in the light of the growing health challenges confronting the continent. The rest of the study is structured in the following manner. The section ‘Presentation of Data and Methods’ discusses the data and corresponding methods. The section ‘Results and Discussion’ presents the results and the attendant discussion. The section ‘Concluding Implications and Future Research Directions’ concludes with policy implications and future research directions.
Presentation of Data and Methods
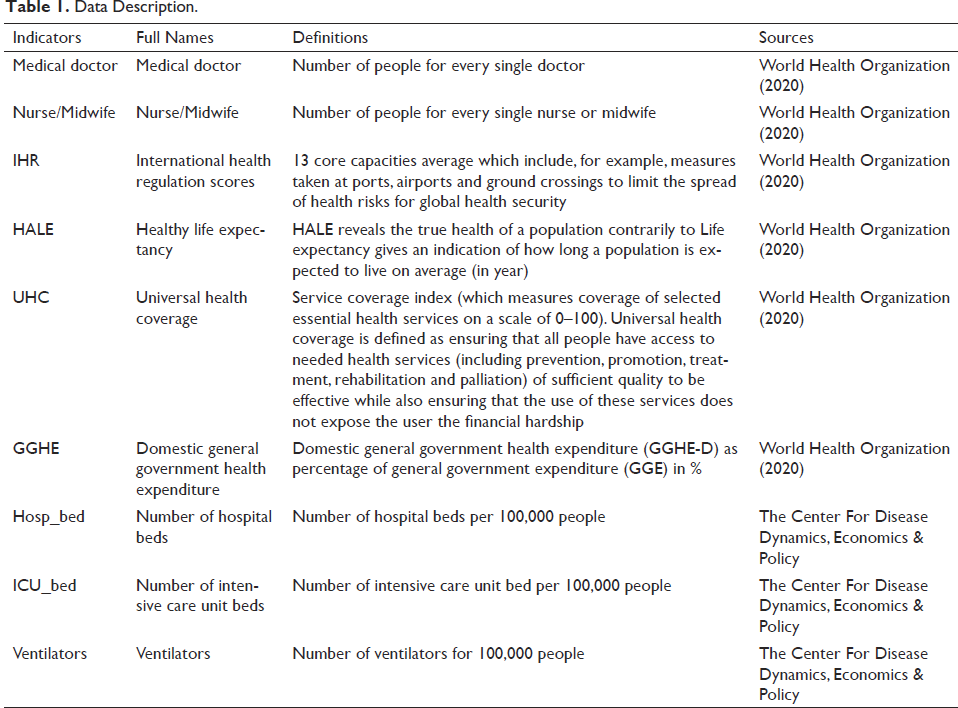
In this article, two categories of data are used for African countries. The first is from the United Nations (UN) Sustainable Development Goals (SDGs). These data can help us to understand how equipped the health systems are to meet the challenges of guaranteeing that all people enjoy greater peace and prosperity by 2030. Among these indicators, we have a selected number of people for every single doctor (Medical Doctor), number of people for every single nurse or midwife (Nurse/Midwife), International Health Regulation scores (IHR), Healthy Life Expectancy (HALE), Universal Health Coverage (UHC) and Domestic General Government Health Expenditure (GGHE-D), which are used to depict the health infrastructure level in African countries.
The second group of data are those discovered with the COVID-19 pandemic of which, the most popular are the number of Hospital beds (Hosp_bed), number of ICU_bed and number of ventilators. It is worthwhile to note that with the COVID-19 pandemic, there is a strand of literature on the availability of these health tools and critical care capacity (Craig et al., 2020a, 2020b; Ma &Vervoort, 2020; Weissman et al., 2020; White & Lo, 2020; Diop & Asongu, 2020) which has not critically engaged Africa as done in the present study. The definitions and sources of the variables are disclosed in Table 1.
Data Description.
As for the methodology, given that the study is exploratory, we rely on exploratory descriptive analysis based on tables, summary statistics and maps to depict the lack of health infrastructure made more apparent, by the COVID-19 pandemic in African countries.
Results and Discussion
We start by analysing the global trends of health statistics from the UN SDGs by regions. Most of these indicators are proxies for monitoring SDG 3 pertaining to health and well-being (ensure healthy lives and promote wellbeing for all at all ages). Table 2 reveals that, overall, all signals are in the red in Africa. We employ the number of medical doctors and nurses or midwives as a proxy for health workforce. The results show dramatic disparities across different world regions and an unacceptable scarcity of healthcare workers in Africa. By way of illustration, the number of people for every single medical doctor is more than eleven times higher in Africa than in Europe. Moreover, Africa earns the lowest IHR scores (44/100) in relation to health workforce. The IHR scores relate to an agreement between 196 countries and territories for global health security. It measures the country’s ability to prepare for and respond to health emergencies. A low score from Africa could indicate why the WHO predicted in March 2020 that the virus would spread rapidly in Africa and cause millions of deaths. Instead of life expectancy, which gives an indication of how long a population is expected to live on average, we use the HALE, which reveals the true health of a population. We note a clear difference between Africa (53.80) and Western Pacific (68.90) or Europe (68.40). Regarding the UHC, the results show that African citizens do not have access to needed health services of sufficient quality without financial hardship. Finally, we appeal to a macroeconomic indicator. The GGHE-D as a percentage of General Government Expenditure is lowest in Africa (7.20%). Americas (13.2%) and Europe (12.3%) are the top-performing regions.
Health Statistics by Regions.
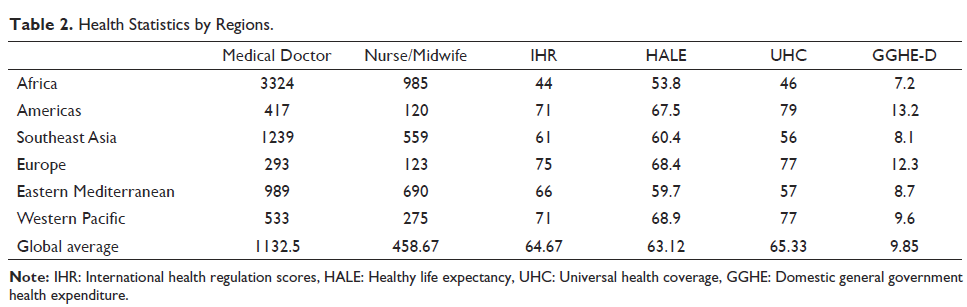
Table 3 summarises the variables in direct link with the COVID-19 pandemic in African countries. It is apparent from Table 3 that there is a considerable degree of dispersion especially in the number of Hospital beds per 100,000 people. The minimum of hospital beds is 10.00 (Mali) and the maximum 630.00 (Gabon) with a mean of 133.60. The minimum of ICU beds per 100,000 people is 0.00 (Djibouti) while the maximum is held by Seychelles (33.07). Regarding the number of ventilators per 100,000 people, the mean is 0.95 and the values are ranged from none (Djibouti) to 9.19 (Cabo Verde).
Descriptive Statistics.

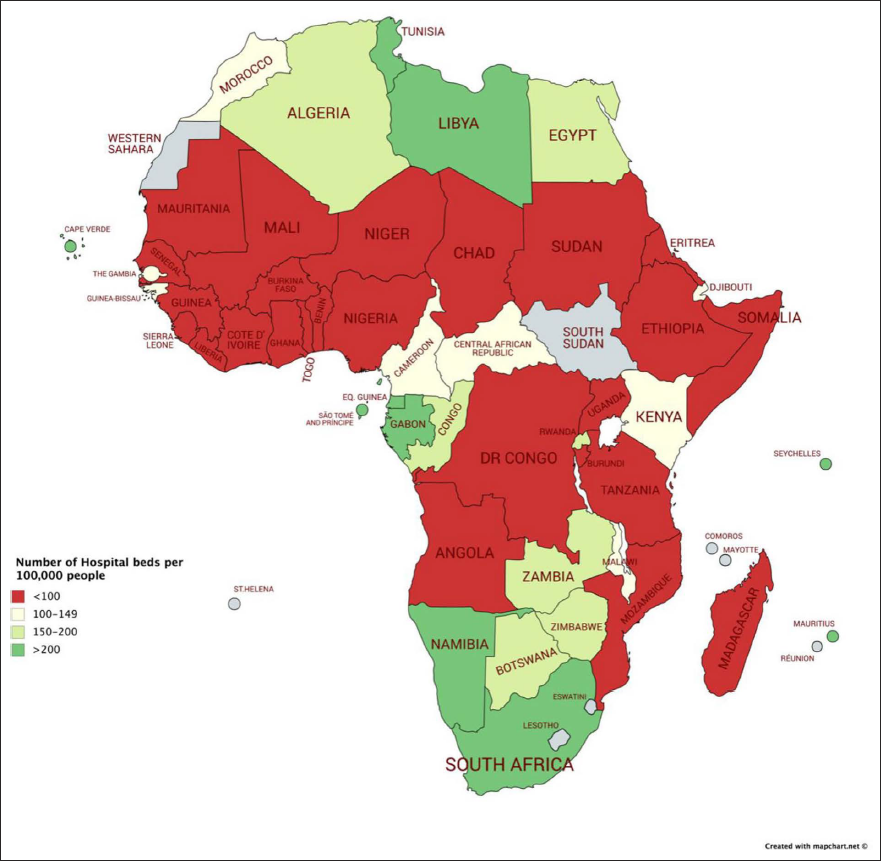
To highlight the lack of health infrastructure in African countries, we mapped national patterns of the current available critical care infrastructure with a focus on the distribution of hospital beds, ICU beds and ventilators. Figures 1–3 provide the density of the hospital beds, ICU beds and ventilators. An exploratory analysis of Figure 1 shows a spatial distribution of the number of hospital beds per 100,000 people. Countries with a number of hospital beds higher than 150 are clustered in Northern (Tunisia, Libya, Algeria and Egypt), Central (Sao Tomé, Equatorial Guinea, Gabon and Congo) and Southern (South Africa, Namibia, Botswana, Zimbabwe and Zambia) Africa. Although there is no global norm for the density of hospital beds in relation to total population, this figure reveals a very low density. For example, the countries with the highest density of hospital beds worldwide include Japan (1310), Korea (1230), Russia (8100) and Germany (8000), contrary to Africa, where out of the 51 countries in our sample, only one exceed 500 beds per 100,000 people.
Number of Hospital Beds per 100,000 People.
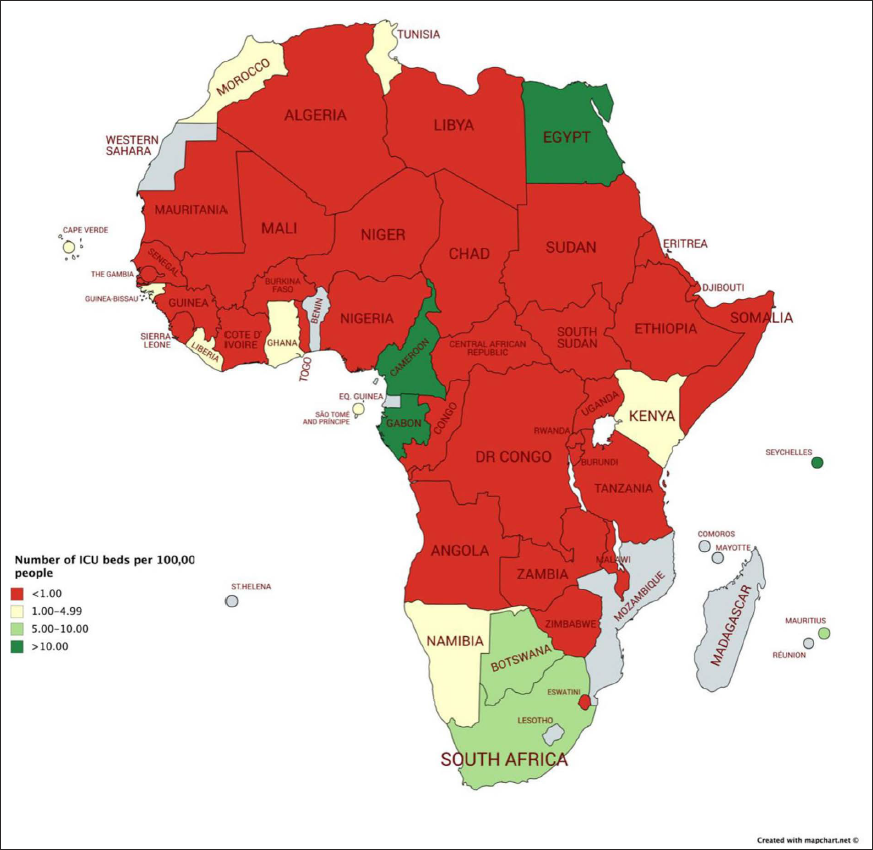
Number of ICU Beds per 100,000 People.
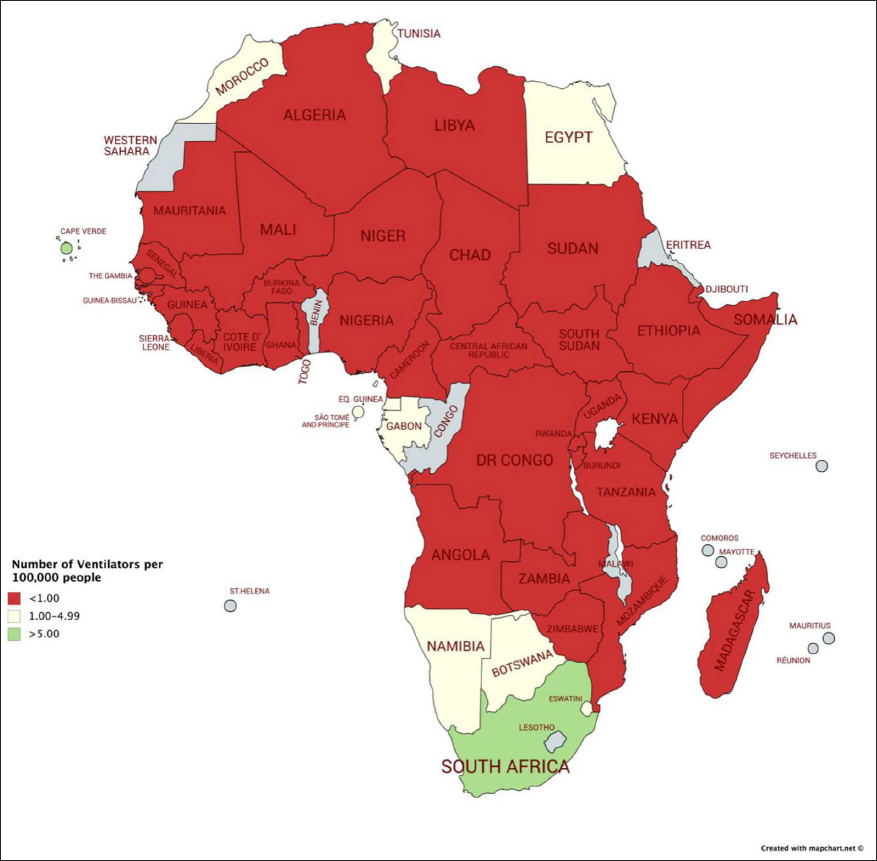
Number of Ventilators per 100,000 People.
In Figure 2, we mapped the distribution of ICU beds per 100,000 people. It is worthwhile to note that only four countries (Egypt, Cameroon, Gabon and Seychelles) have a density of ICU higher than 10 ICU beds per 100,000 people. The availability of beds per 100,000 people ranges from none (Djibouti) to 33.07 (Seychelles). Again a further analysis of the figure shows that more than 92% of African countries have a number of ICU beds per 100,000 people that is less than 1. These statistics show that the density of ICU beds is at an alarming level in Africa compared to the rest of the world. For instance, in Americas and Europe, the density is higher than 5 (Ma & Vervoort, 2020). Estimating the critical care capacity needs and gaps in Africa during the COVID-19 pandemic, Craig et al. (2020a) find that even if only 30% of patients with severe cases seek health services at the outbreak peak, then 71% of the countries would not have a sufficient number of ICU beds per 100,000 people to handle projected needs.
Figure 3 shows the availability of the number of ventilators per 100,000 people in Africa. The situation is more alarming for this indicator. Globally, at least 3 out of 4 countries have a density of ventilators less than one ventilator per 100,000 people. The availability of ventilators ranges from none (Djibouti, Guinea Bissau) to Cabo Verde (9.19). Apart from Cap-Verde and South Africa (5.54), all African countries had ventilator density of less than five beds per 100,000 people. The exploratory analysis of the availability of ventilators means that African countries are not yet prepared if the number of severe COVID-19 cases increases. According to Craig et al. (2020a), only four countries (South Africa, Egypt, Gabon and Cabo Verde) have ventilator numbers that are sufficient in view of meeting the projected needs at the national level.
Concluding Implications and Future Research Directions
This exploratory study aims to assess Africa’s lagging position in global health in relation to some healthcare infrastructure before critically examining the situation of Africa in the light of pressing COVID-19 healthcare infrastructural needs in terms of the number of hospital beds, ICU beds and ventilators per 100,000 people. A comparative analysis is provided to showcase which regions are leading in the healthcare facilities in the world in general and Africa in particular as well as countries that are lagging in the attendant health facilities.
Overall, this exploratory statistical analysis reveals that the COVID-19 pandemic highlights another pandemic crisis in Africa. In fact, our results find the unacceptable scarcity and lack of care capacity and infrastructure in African countries. The lack of critical care capacity with a focus on the distribution of hospital beds, ICU beds and ventilators means African healthcare systems are not adequately prepared for the present wave of the COVID-19 pandemic, a second wave of the underlying pandemic as well as a future pandemic. Moreover, the COVID-19 pandemic may further amplify disparities, socio-economic inequalities and prevent Africa from attaining SDGs. Hence, this study has provided both scholars and policymakers with analytical insights into how the COVID-19 pandemic has revealed the manner in which Africa cannot reach most SDGs, especially SDG-3 on health and well-being. Moreover, the continent is unprepared for future pandemics in terms of health facilities. Furthermore, the comparative analysis provides policymakers with insights into how resources can be allocated to countries in terms of which countries need more health facilities relative to others.
Future studies can improve the extant literature by assessing the financing gap of healthcare needs in African countries as well as mechanisms by which these attendant needs can be funded. It is also worthwhile for future research to examine how traditional medical facilities (being explored in many African countries to fight the COVID-19 pandemic) can limit some needs for modern health facilities on the one hand and prepare African countries for future pandemics on the other.
Authors’ Contribution
SD participated in the drafting of the manuscript. SSA participated in the supervision of the manuscript. All authors read and approved the final manuscript.
Availability of Supporting Data
The data for this article is available upon request.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.