
Abstract
Comprehensive Human Immunodeficiency Virus (HIV) services are seldom found within a single organisation. This motivates organisations to form partnerships to achieve optimal outcomes. However, the complexity of inter-organisational relationships can hinder the process of achieving an effective and coordinated response to the HIV epidemic. Understanding the evolution of these inter-organisational relationships can shed light on ways to improve the delivery of these service provisions. This study examines the organisational networks of the HIV care landscape in the Chicago area across 3 years (2015–17). The results of longitudinal analysis indicate that although most organisations still perceive this landscape to be moderately competitive, they have developed more formalised ties and increased their collaborations across 3 years. Further, with passage of time, this organisational network has become denser with no organisational isolation, indicating connection between all organisations in this landscape. Practical implications for organisations are discussed.
Keywords
Introduction
Despite four decades of medical and scientific advances, the Human Immunodeficiency Virus (HIV) epidemic continues to have a significant and profound impact in the United States (US) with 34,800 new diagnoses in 2019 alone (CDC, 2020a). Critically, while the overall number of new HIV infections has decreased over time, it has remained stable or increased among historically marginalised and underserved groups, including Black and Latinx sexual minority men (BLSMM) and transgender individuals (CDC, 2020a). Existence of such disparities indicates that healthcare’s current system-level approaches to HIV prevention and treatment must continue to be improved.
HIV service organisations have implemented and delivered a multitude of HIV prevention and treatment strategies to address the HIV epidemic (Phillips et al., 2022). These include strategies to facilitate access to biomedical prevention and treatments, such as pre-exposure prophylaxis (PrEP) for people vulnerable to HIV and antiretroviral treatment (ART) as prevention (TasP) among people with HIV (PWH) (Cohen et al., 2012; Holt, 2014; Nunn et al., 2017). Other approaches include behavioural intervention strategies, like condom distribution, medication counselling, comprehensive sexuality education and HIV-testing programmes (CDC, 2020b). Structural interventions which focus on capacity building, community mobilisation, increasing access to care or prevention, modifying social determinants of health or altering policy have also gained increased attention (Adimora & Auerbach, 2010; CDC, 2020b). Aligned with this comes a proliferation of recent initiatives aiming to address the epidemic; multiple plans, including Getting to Zero-Illinois (GTZ-IL), the Ending the HIV Epidemic (EHE) Plan and the We the People Plan, are currently active in the state of Illinois.
Despite these extensive efforts, outcomes for both PrEP and HIV care remain suboptimal as evidenced by high drop-off in patient engagement even at early stages of the care continuum (Liu et al., 2019). Particularly, even when a large number of individuals are identified as good candidates for PrEP or ART, very few end up filling a prescription or taking the medication with sufficient regularity to be effective (Laborde et al., 2020). In addition to limited awareness of the value of PrEP and TasP (Eaton et al., 2017; Holt, 2014) and low rates of testing among vulnerable populations (Ham et al., 2016; Phillips et al., 2015), delayed linkage to care following a positive HIV test prevents optimal care engagement (Thompson et al., 2012). Further, even when referrals are provided and linkage achieved, competing needs and structural barriers prevent necessary treatment engagement (Wood et al., 2019).
While individual-level factors such as substance use (Friedman et al., 2009), food insecurity (Colasanti et al., 2017), housing (Schwarcz et al., 2009; Thakarar et al., 2016; Wolitski et al., 2007) or employment (Gayles et al., 2016) in unsuccessful engagement with healthcare or HIV prevention activities are very well studied, the role of organisational factors such as instability in inter-organisational relationships and networks remains severely understudied. This lag in literature becomes the point of departure for this study.
Organisational Networks and HIV Service Provision
Existence of various approaches, initiatives and organisations makes the landscape of HIV prevention and treatment services diverse (Fisher et al., 2018; Smith et al., 2020; Zuma et al., 2019). Typically, a combination of Community-Based Organisations (CBOs) and healthcare centres, such as hospitals or clinics, provide unique and complementary services aimed at treatment, prevention and support of PWH and people vulnerable to HIV (Shapatava et al., 2018). Whereas larger health centres can offer comprehensive health services in a single location, they typically struggle to engage particularly more marginalised populations. CBOs, in contrast, often shoulder the majority of advocacy and outreach work involved in supporting patient engagement and are uniquely well-qualified to oversee such community engagement activities. Still, they are often unable to provide necessary treatment services (Pinto & Park, 2020).
Given that comprehensive HIV services are rarely found within a single organisation (Beach et al., 2018), formalised collaborations may be necessary to achieve optimal care continuum outcomes. This premise is supported by research outside of the HIV sector, which has emphasised the importance of inter-organisational collaboration in achieving crucial planning and health outcomes (Cooper & Shumate, 2012; Michener et al., 2012; Provan et al., 2005) and by prior research with HIV organisations specifically (Phillips et al., 2022). Unfortunately, in dense metropolitan jurisdictions, complex organisational relationships can hinder the process of achieving an effective and coordinated response to the HIV epidemic.
Generally, organisational relationships and broader networks are formed via exchange of services (Tajoli et al., 2021). These exchanges have been deemed a natural reference point for various mechanisms that incentivise user participation and improve the efficiency of such networked services (Georgiadis et al., 2015). Therefore, a focus on the nature of service exchanges between organisations can improve understanding of the roles that different organisations play in the landscape of service delivery (Yip et al., 2002). Additionally, informal connections between organisations, often developed and fostered through personal relationships, can threaten the stability of collaborations due to staff turnover (Veniegas et al., 2009). Understanding the evolution of these complex inter-organisational relationships can guide efforts to solve such problems (Harini & Thomas, 2020).
Network science methodology offers a valuable approach to solving this problem. Tangible, quantitative network metrics have been found to produce meaningful information for the evaluation and improvement of service delivery. These include network density, centrality, homophily, heterophily and descriptive information regarding specific ties (Lorant et al., 2017; Mays et al., 2010; Popp et al., 2013; Retrum et al., 2013). These metrics are particularly useful in highlighting gaps in collaboration, which allow partner institutions to consider how to more effectively and efficiently administer much-needed services in a comprehensive and collaborative manner (Bevc et al., 2015; Provan et al., 2005; Radcliff et al., 2018). For example, a network without any isolated organisations suggests network coherence.
Although more commonly used to examine individuals’ social, sexual or drug use networks and their relationship to HIV risk (Birkett et al., 2018; Egan et al., 2011; Kelly et al., 2010; Latkin et al., 2013; Mustanski et al., 2018; Salamanca et al., 2018), network analyses of HIV-organisations have already yielded valuable insights into how best to improve comprehensive service delivery (Bradford et al., 2007; Thompson et al., 2012) and achieve optimal care continuum outcomes (Phillips et al., 2022). With such data, HIV sector institutions have an opportunity to rigorously and insightfully evaluate the state of HIV service provision in their area and to take the necessary steps to close critical gaps and improve patient engagement and HIV outcomes overall.
To date, the majority of organisational network studies examine relationships at a single point in time rather than as a dynamic process (Morisse et al., 2014). While this approach provides significant, useful information, it is limited in its ability to evaluate the factors which influence network change or to assess the stability of extant relationships. When exploring the relationships of international HIV/acquired immunodeficiency syndrome (AIDS) nongovernmental organisation networks, Shumate et al. (2005) found that looking at the evolution of these networks over time revealed significantly different patterns than a cross-sectional view. Exploring these changes is crucial to accurately understand the processes which facilitate inter-organisation collaboration and to leverage this information to more effectively address gaps in service capacity or availability. Longitudinal analyses of organisational networks provide an opportunity to explore the nature and importance of changing collaboration within the HIV sector. Using data collected from a multi-year, multi-site evaluation of health department-funded organisations within Chicago, this study builds on prior network analyses (Phillips et al., 2022) to shed light on how a local network of HIV service organisations evolved over time, including implications for HIV epidemic response and recommendations for network approaches to improving service provision.
Method
Data for the current study were collected as part of the Center for the Evaluation of HIV Prevention Programs in Chicago (Evaluation Center) project. The Evaluation Center was funded by the Chicago Department of Public Health (CDPH) to support and evaluate prevention interventions through Comprehensive High-Impact HIV Prevention Projects for CBOs (Phillips et al., 2019).
The Evaluation Center conducted three annual organisational network surveys with grantees to investigate changes in formalised connections, competition and collaboration in the network and types of services being provided and received among the 20 funded projects and 57 other HIV service organisations in Chicago.
Public Health Context
Chicago HIV patterns largely mirror national trends; BLSMM bear a significant burden of the disease, and individuals aged 20–29 years are the most frequently diagnosed (CDPH, 2019). For example, as of 2018, there were 23,580 PWH in the city, of which 49.9% were Black and 19.9% were Latinx/Hispanic. Further, 63.9% were males who acquired HIV through sexual contact with another male. Recording the fewest new diagnoses of HIV in Chicago since 1990 in 2018 (CDPH, 2019), Chicago remains a leader in the response to the HIV epidemic and boasts a large complement of HIV treatment and prevention activities (Phillips et al., 2022). However, the widespread segregation present in the city (Moore, 2016) as well as competition between different CBOs and service providers (Phillips et al., 2022) may lead to critical gaps in care and service access.
Survey Development and Administration
The organisational network survey was developed and deployed in REDCap (Harris et al., 2019). One representative from each of 20 HIV-prevention projects funded by CDPH was invited to complete the survey, representing 15 different CBOs. Participants responded annually (2015–2017) to questions about the current collaborations their agency had with other HIV-service organisations in Chicago, including information on type, length and strength of relationship.
Measures
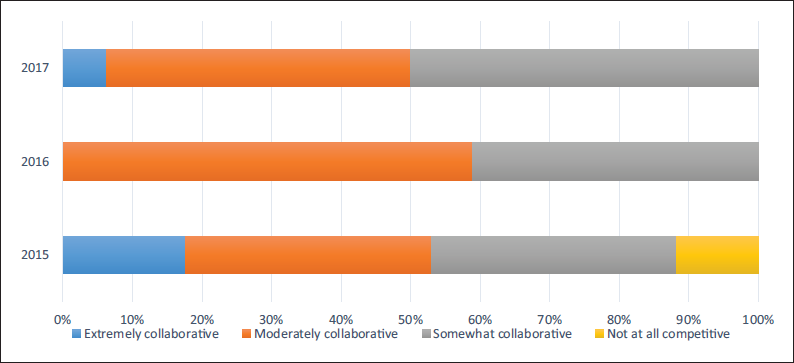
To define the collaborative versus competitive nature of the landscape, respondents were asked to ‘rate the current level of collaboration among HIV service organisations in Chicago’ on a four-point scale from ‘Not at all collaborative’ to ‘Extremely collaborative’. Informal partnerships were defined as ‘things like sharing information about available programmes or assisting with recruitment activities without a formal agreement obligating the organisation/project to do so’. Formal partnerships were ‘things like having a memorandum of understanding (MOU), subcontract, or grant partnership in place’. To define the strength of project’s relationship with formal partners, respondents were asked to rate the strength on a three-point scale from ‘Very strong’ to ‘Not at all strong’.
Respondents were asked to respond to a series of questions about exchange of services between organisations. For each formal partnership, respondents were asked ‘What type(s) of support or services does your project provide to [organisation name]?’ and ‘What type(s) of support or services does [organisation name] provide to your project?’ Respondents could choose from a list of 16 options that included funding, data resources, community connections, leadership, advocacy and trainings. Consistent with the principles of organisational sciences (Tsoukas & Knudsen, 2005), services that facilitate the proper exchange of experiences and lessons learned between partnered organisations were re-classified as ‘knowledge management’ (Bennet & Bennet, 2004). Similarly, services that contribute to advancement of organisational goals were re-classified as ‘mission advancing’ (Sagawa & Segal, 2000).
Data Analysis
Basic descriptive statistics were generated using SAS® software 9.4 (2013 Cary, NC). Additional analyses were conducted to measure network density and degree. Any organisations that appeared multiple times within the combination of individual networks were merged into a single node to create a macro-network (Stolbova et al., 2018). Density was measured by examining local clustering coefficients for each participating organisation (Opsahl, 2013). This is measured by calculating the ratio of triangles out of all triplets centred around the given node (Wasserman & Faust, 1994). Basic network statistics were assessed using Gephi v0.9.2, which was also used to produce visualisations.
Results
Collaboration vs. Competition
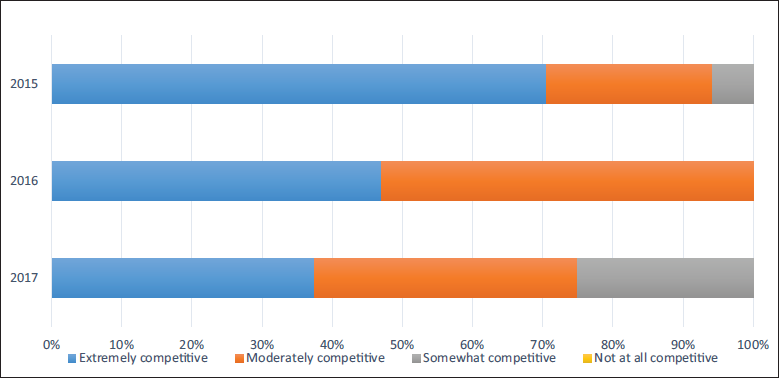
Across all 3 years, approximately 50% of participants thought the HIV landscape in Chicago was extremely or moderately collaborative; there were no significant differences across the 3-year period (p = .46, Figure 1). Contrastingly, virtually all participants felt the landscape was extremely or moderately competitive, but mean perceived competition significantly decreased between 2015 and 2017 (p = .01, Figure 2).
Level of Collaboration across 3 Years.
Level of Competition across 3 Years.
Formal Relationships vs. Informal Relationships
In 2015, 59 organisations reported 199 partnerships, of which 29.6% were reported as formal relationships. A year later in 2016, 167 partnerships were reported between 57 organisations; 41.9% of them were identified as formal. In 2017, the final year of the survey, 143 partnerships were identified between 57 organisations with 53.8% reported as formal relationships. The year-to-year increase of approximately 10% in proportion of formal partnerships was a significant change.
Network Attributes
Across all 3 years, HIV prevention/treatment organisations presented in this study could all be connected into a single component (Figure 3). This shows a lack of organisational isolation with the HIV prevention landscape of Chicago from the initial year of this study. However, over the same time period, the networks between these organisations evolved to become more centralised and denser, which indicates an improvement in service delivery (Bunger et al., 2014). In 2015, the mean degree of the network (i.e., number of connections to other organisations) was 2.76, showing an average connection of one organisation with at least three others. In 2016, this number increases to 5.86, showing that every organisation, on average, was connected with almost six other organisations. Not much change is shown between 2016 and 2017, as a year later, the mean degree network is reported to be 5.09, showing an average connection to at least five other organisations.
Network Attributed of HIV Prevention Landscape of Chicago across 3 Years.
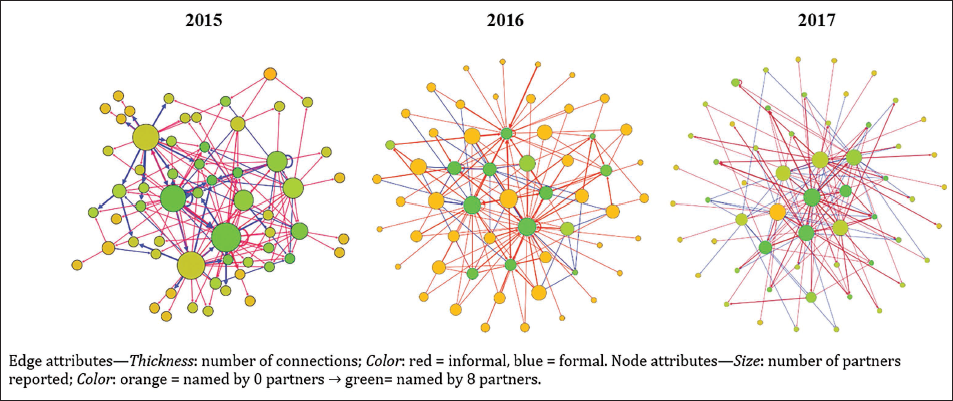
Similar changes can be seen in the reported network density. In 2015, organisations reported an extremely low density (0.048), indicating few potential connections had occurred, which is indicative of selective partnering in the HIV prevention landscape of Chicago. In 2016 and 2017, the network density doubled to, respectively, 0.096 and 0.085 compared to 2015.
Exchange of Services
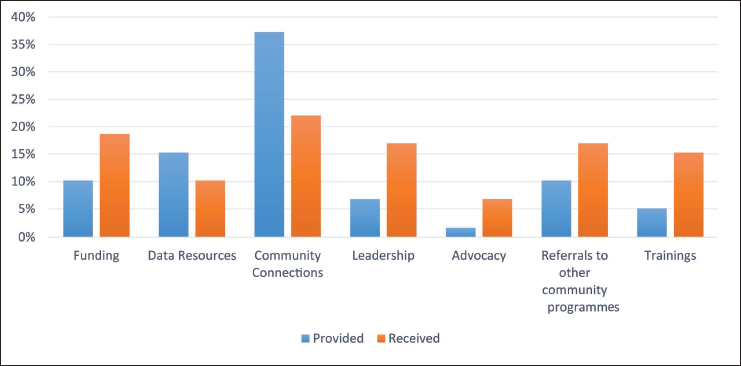
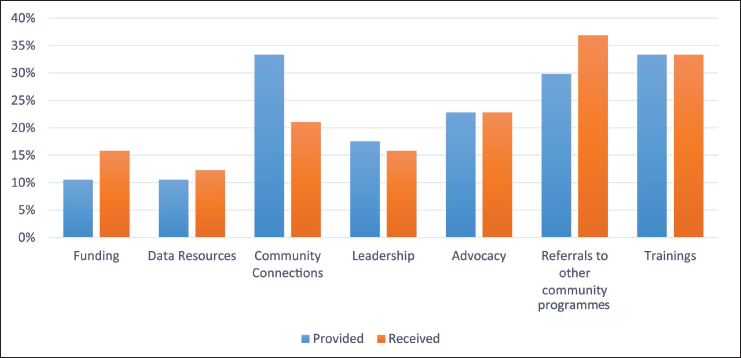
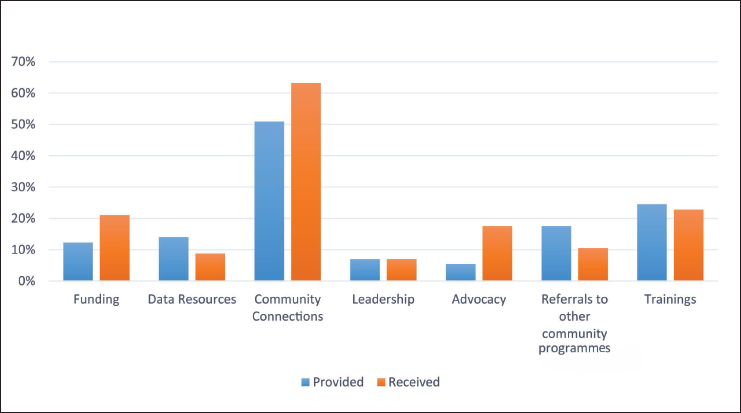
Presented in Figures 4–6, the exchange of services between partnering organisations increased over time, with number of services provided exceeding the number of services received by 2017. In 2015, organisations reported providing 113 services and receiving 127 services; these numbers increased in 2016 to 191 services provided and 165 services received. This change from more services provided than received continued into 2017, where organisations reported providing 179 services and receiving 161 services.
Exchange of Services in 2015 (%).
Exchange of Services in 2016 (%).
Exchange of Services in 2017 (%).
Data Resources
In 2015, 15% of organisations reported providing data resources to their partners, while 10% reported receiving such resources. Although the numbers were nearly equal in 2016 (11% providing and 12% receiving), a similar gap of 5% was seen in 2017 (14% providing and 9% receiving). The results show that organisations are more likely to share data resources than to receive them; however, the proportion of both providing and receiving remained relatively similar across all 3 years.
Leadership
Nearly one-fifth of agencies (17%) reported receiving leadership support from their partners in 2015. Although the level of received leadership was similar in 2016 (16%), it substantially decreased in 2017 to 7%.
Training
In 2015, 15% of organisations received training resources, while only 5% reported providing them. Later, in contrast, organisations report a balance between receiving (33% in 2016 and 25% in 2017) and providing (33% in 2016 and 23% in 2017) training services.
Funding
In 2015, 19% of organisations reported receiving funding support from their partners as opposed to 10% that reported providing funding. These numbers remained consistent across all years as 16% and 11% in 2016 as well as 21% and 12% in 2017 respectively reported receiving and providing funding.
Community Connections
In 2015, 22% of organisations reported receiving community connections from their partners, while 37% reported providing such resources. While these numbers remained consistent in 2016 (21% receiving and 33% providing), a dramatic increase for both numbers was reported in 2017 (63% receiving and 51% providing).
Advocacy
In 2015, 7% of organisations reported receiving advocacy support, while only 2% provided advocacy support. A substantial and reciprocal increase in both receiving (23%) and providing (23%) advocacy support was reported in 2016. Although proportion of organisations receiving advocacy support in 2017 was comparable, there was a considerable drop in providing advocacy support to 5%.
Referral to Community Programmes and Healthcare Providers
In 2015, 17% of organisations reported receiving referrals to community programmes and healthcare providers, while only 10% provided such services to their partners. While a noticeable increase in these levels were reported in 2016 (37% receiving and 30% providing), the 7% gap between providing and receiving these services remained similar to those of 2015. In contrast, in 2017, 18% of organisations reported providing referrals, while only 11% reported receiving them.
Discussion
Our organisational network analysis of the HIV prevention landscape in Chicago shows significant change over the 3 years of study. In addition to noting the absence of organisational isolates, longitudinal data showed substantial increases in network centrality and density. This growth in network density shows how, over the years studied, HIV prevention organisations in Chicagoland formed more ties relative to the total number of possible relationships.
Evolution of Formal Relationships
Further, data show a significant growth in formal relationships across 3 years. This is an important change in the HIV care delivery system, as past network analyses have shown ad hoc relationships are a weakness of inter-organisational relationships in this sector (Kwait et al., 2001; Thomas et al., 2007). One explanation for this substantial change across the 3-year period may be that organisations of all sizes realised the vulnerabilities of relationship-based agreements and took steps towards formalising their collaborations, removing the potential for disruptions due to personnel turnover. Hawthorne effect can play a role in this change as well (Leonard & Masatu, 2006). Simply asking about the strength of ties may have encouraged organisations to form stronger ties with their partners. This indicates that a more comprehensive programme evaluation can impact organisational relationships and services.
Changes in Organisational Exchange
Organisational relationships, especially in health services (Valaitis et al., 2018), are heavily influenced by the balance between the availability of resources and an organisation’s needs (Russo & Cesarani, 2017). Studying organisational exchanges across time illuminates the balance between available resources and the needs of partnering organisations (Roehrich et al., 2020).
Data Resources
With this, data show a limited sharing of data resources across organisations. Since data-driven decision-making has a critical role in the fight against HIV (Davis, 2017; Logan et al., 2005) and most funders require data management infrastructure for grantees (Oomman et al., 2007), it is not unexpected to see limited need or need to share data resources among HIV service organisations in Chicago.
Leadership Resources
Exchange of leadership resources declined across 3 years. This is possibly evidence of a successful knowledge transfer in leadership (Fang et al., 2013), resulting in a certain degree of confidence in this domain after initial sharing. It is very likely that organisations are more interested in learning from their peers than in providing their partners with their own leadership expertise. Further, organisations reported a stabilised increase in exchanging training resources, which is best explained by stages of knowledge transfer (Sohi & Matthews, 2019). Since 2015 was the first year of relationship assessment, organisations were likely in the formative phase and actively learning from their partners, resulting in reciprocated exchanges in later years.
Funding Resources
Exchanges of funding showed stable growth over time. This reflects the critical role of availability of funds across all organisation years for the HIV service landscape of Chicago, consistent with claims from past works (Albritton et al., 2017; Nguyen et al., 2021). Access to funds, at least in Chicago, remains a key element for collaborations to fight the spread of HIV (McGillen et al., 2017) and requires specific attention from funding agencies like Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH) and Health Resources and Services Administration (HRSA) (Brown, 2017). With this, funding agencies can develop, advertise and provide more funding to meet the general and specific needs of these organisations; more resourceful organisations can do the same by developing grant programmes specifically for their formal partners. There was a dramatic increase in sharing community connections over the course of 3 years. This growth shows how community connections can get saturated over time, highlighting the importance of partnerships for reaching minoritised populations vulnerable to HIV Latinx communities (Guilamo-Ramos et al., 2020) or transgender migrants (Azadi et al., 2020). Similarly, as HIV care and treatment service organisations diversify their offerings, the need for new connections becomes more evident.
Advocacy Resources
Exchange of advocacy resources showed an unstable growth and decline over the course of 3 years. Possibly, this is evidence of the ideal outcome of advocacy over time (Honeycutt & Strong, 2012). More specifically, in the absence of solidified inter-organisational relationships, organisations show a reluctance in offering advocacy services to their partners. This also shows the persistent need to receive advocacy support from organisational partners even though the capacity to provide the same support might diminish at times. This was similar for exchange of referral to community programmes and healthcare providers. Perhaps this unstable growth and decline attest to the efficacy of an integrated network in creating connections between multiple partners (Dufays & Huybrechts, 2014), as in time organisations became better equipped to provide rather than receive referrals.
Limitations
This study is not without limitations. Our limited focus on CDPH-funded organisations resulted in a limited picture of the HIV prevention landscape of Chicagoland. Consequently, incomplete access to all HIV prevention organisations prevented a comprehensive analysis of network metrics. Organisations were not asked about their pathways to partnerships or information on their informal relationships, which barred us from exploring how these relationships are formed or maintained. Finally, due to either social desirability bias or issues with recalling details of a partnership, organisations might not have included information about less-than-ideal or less memorable partnerships, which might have skewed this data towards an optimistic end. Future studies need to further investigate the initiation and evolution of these inter-organisational relationships. To illustrate a full picture, these studies are encouraged to go beyond publicly funded organisations and to include collaborations around disproportionally impacted communities.
Conclusion
Plans to promote ending the HIV epidemic in the United States have proliferated in recent years and have provided guidance towards optimising existing prevention and treatment systems. These plans have also been crucial in expanding the focus from individual-level behaviour change interventions to structural- and systems-level interventions, acknowledging the diverse challenges minoritised populations face in accessing and staying in healthcare. This current study explores one approach to understanding the systems involved in HIV care and prevention activities—the study of changes in HIV organisational networks over time. Results show substantial changes over the 3-year period, many of which are in line with predicted changes in improving the strength and quality of network connections. Organisations perceived less competition and more collaboration in Chicago over time, and this was reflected by a significant increase in proportion of formalised partnerships between 2015 and 2017. Further, organisations reported a stronger exchange of funding, knowledge transfer and sharing of advocacy resources over time. Future studies that explore pathways in formation of both informal and formal inter-organisational relationships are encouraged.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
Due to the nature of this research, the participants of this study did not agree for their data to be shared publicly; therefore, supporting data are not available.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project was supported by a grant from the Chicago Department of Public Health (RFP # DA-41-3350-11-2014-003). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agency.