
Abstract
Mother–child is an integral part of overall global development planning, as evident from substantive investments, lasting socio-economic priority and the thorough implementation of various public policy programmes like the National Health Mission (NHM). There is a need to impregnate evidence about the acceptability, cost-effectiveness and scalability of transformative public health programmes like NHM through management sciences and by impact evaluation and implementation studies.
The study examines the implementation dynamics of the NHM programme in the context of maternal and child service architecture and measures the average impact of NHM on maternal and child health outcomes. This study uses a multilevel, mixed, cross-sectional field design of impact measurement, using a multiphase approach to devise impact models from interrupted time series longitudinal panel data, and uses counterfactual impact model development using autoregressive integrated moving average (ARIMA).
The findings of the study show that there has been a significant decline in mortality indicators of maternal and child health, with NHM having the maximum positive impact on institutional deliveries and deliveries by skilled birth attendants. The study shows that NHM has proved to be a successful population-level health interventional programme and has emerged as a crucial structural-equity modelling reform programme. The policy implication is that a broad-based approach with the inclusion of socio-structural determinants is needed for improving the health of the mother–child ecosystem, with access to basic comprehensive maternal emergency care.
Keywords
Introduction
Even after seven decades of implementing health policy programmes related to reproductive, maternal and child health (MCH), India still contributes around 12 per cent of the global maternal mortality and one-fifth of child mortality (Hemalatha et al., 2020). Together, maternal–perinatal health conditions constitute around 12 per cent, while childhood diseases constitute 5 per cent of the global disease burden in India (Sharrow et al., 2022). The recent COVID-19 pandemic has resulted in major disruptions to healthcare services, and it is expected that, due to COVID-19 in India, maternal mortality will increase by 15 per cent and child mortality by 10 per cent, which would be the highest globally (UNICEF, 2021), depicting the low resilience of the MCH care ecosystem.
A large group of approximately 71.4 per cent of the population in developing countries constitutes the mother–child dyad, which is considered a vulnerable risk group. In India, 22.2 per cent of the population are women (15–44 years) of reproductive age, and children under 15 years constitute 35.3 per cent of the total population, together making up 57.5 per cent of the population.
The policy interventions to ameliorate MCH are a global priority. Over the years, there have been continuous public health policy commitments and interventions, such as the National Health Mission (NHM), to address the lack of high-quality health care and to scale down mother–child mortality. The progress has gathered momentum over the years but has been uneven and suboptimal, especially during the pregnancy and intrapartum phases. The MCH care is witnessing an asymmetrical distribution of efficiencies, services and performance across the country (Singh & Vellakkal, 2021). Maternal mortality ratio (MMR) reduction has shown wide variation, with some states already achieving the sustainable development goals (SDG) 2030 targets, while some states are lagging behind (Bhatia et al., 2021). If the trends observed up to 2017 were to continue, India would meet the SDG-2030 target for the under-five mortality rate (U5MR) but not the neonatal mortality rate (NMR) target; 34 per cent of the districts in India would need a higher U5MR reduction, and 60 per cent of the districts would need a higher NMR reduction to individually meet the SDG targets by 2030 (Dandona et al., 2020).
NHM, being in its terminal phase of implementation, has discorded, sparse and poor-quality data, with minimal evidence available on the effectiveness of NHM in terms of its contribution and its impact on improving the MCH outcomes. The resilience, disparity–inequality within the health delivery system, structural determinants and social constructs-drivers at the community level have immensely contributed to and shaped the outcomes in the MCH ecosystem, which have been persistently ignored at the policy, planning and implementation levels (Singh et al., 2014). Most of the literature reflects a lack of evidence-based implementation approaches, adaptations and iterative solutions related to service delivery processes, programme strategies and technological approaches aiming for universal health coverage (UHC) within the ambit of NHM and National Health Policy. There is a need to find the impact of NHM and the changes it has produced for clients and the population, both through factual and counterfactual estimation, and to provide an opalescent policy and programme approach for scaling up programme implementation.
NHM—Implementation Framework and Evaluation Strategy
The NHM is the largest global composite community-based health intervention programme, introduced in 2005, with the aim of bringing structural and financial transformation to the Indian health care ecosystem. The programme envisaged inclusivity, equity and quality among the marginalised and vulnerable groups, specifically oriented towards maternal and child wellbeing. NHM is augmented through an amalgamation of multiple initiatives and mutually interlinked activities to address the beleaguered healthcare needs of the rural–urban population. But still, after 19 years of the implementation of the NHM programme, the health care ecosystem is witnessed by underutilisation of MCH services and skewed distrubution of human logistic resources and non resilient emergency obsteric care (Singh & Vellakkal, 2021). The achieved outcomes have been divergent, especially in states with marginalised and vulnerable populations (Bhatia et al., 2021).
Evaluating the NHM programme’s impact on MCH outcomes is complex due to its many interconnected and mutually linked strategies. To assess effectiveness, the study uses a context–mechanism–outcome (CMO) configuration indicator log frame model, which involves gathering evidence, understanding the programme theory and evaluating outcomes. Indicators are divided into process-outcome and impact indicators, following the WHO logic model (1993). The evaluation employs multiple MCH core impact indicators, diverse methods, comprehensive demographic surveys, giving the widest outreach of NHM, and multi-level approaches to ensure a robust assessment.
Conceptual Framework and Methodology
The conceptual framework of this study, as shown in Figure 1, is based on the typology of the mixed theory approach given by Creswell (2014) and Teddlie and Tashakkori (2011), which combines evidence from multiple approaches and methods of assessment. The study uses a programme theory-driven methodology, including objective and subjective (Chiba et al., 2012), primary and secondary data sources and the use of counterfactual estimation. The mixed approach in the study recouped the technical and data gaps that could be encountered in using only one method and compensated for each other’s methodological weaknesses, resulting in information–conclusions that were rigorous, impactful and added credibility judgment to impact evaluation.
Conceptual Framework of Study.
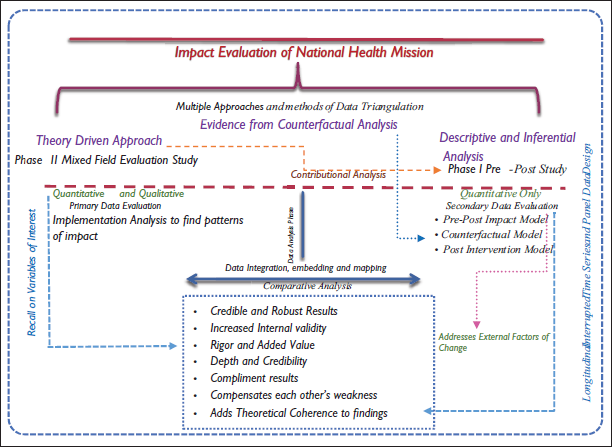
The mixed approach based on theoretical coherence was necessary in the study to understand whether the NHM has operated as intended, in addition to analysing how efficiently resources and knowledge were transferred, and how complex structural determinants and social dynamics are operating within the NHM context.
Study Phases
The study included two phases: Phase I included desk-based impact model estimation through interrupted time series (ITS) and panel data analysis with counterfactual estimation, augmented by a theory-driven approach based on the programme theory of NHM. The secondary data sets from the National Family Health Survey (NFHS) and Sample Registration System (SRS) were used.
Phase I of this study is a population-level impact evaluation with a natural quasi-experimental-observational design, with the same population itself acting as both a control and treatment group, thus cancelling out time-invariant factors. Phase I uses longitudinal panel data for outcome indicators and time series data for impact indicators. The pre–post design approach used two epoch periods running from 1995–2005 to 2006–2016, depicting pre-NHM and post-NHM periods. The aim of this phase was to measure the average magnitude of change through statistically creating an impact model of NHM and producing a counterfactual outcome model based on data sets from the pre and post-periods to compare it with the factual estimation of the programme.
Phase II of the study included a cross-sectional field validation survey based on primary quantitative and qualitative data collection to measure dimensions and capacity of the MCH delivery system in the functional areas of service delivery, structure and processes. It included both implementers’ and beneficiaries’ subjective assessments by field observations using checklists, rating scales and mixed structured and semi-structured questionnaires. Phase II added theoretical coherence, tried to elaborate on how and why beneficiaries react to programme content and activities, and assessed the changes or impact at the basic service delivery units from both the implementers’ and client’s perspectives (patterns of change).
Units of Analysis
The union territory (UT) of Jammu and Kashmir was taken as a sample region, and a field survey was administered across 12 districts, including the hilly and tribal regions of Ladakh. Study being a population-level impact evaluation, the selected units of analysis were:
Jammu and Kashmir UT population (theoretical impact population). Public health facilities and programme management units (service delivery and implementing units). Mother–child dyad as end-users (beneficiaries population-sample unit). Community linkage worker—ASHA worker (community linking social unit – sample unit)
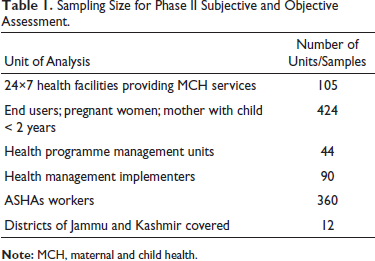
During phase II, field survey quantitative–qualitative information was collected using both probabilistic and non-probabilistic sampling techniques. The data were purposively collected from 24×7 health facilities providing MCH services. Furthermore, four beneficiaries (two pregnant women and two mothers who had deliveries in the last 24 months) were randomly interviewed as exit end-users after availing themselves of the services from selected health facilities. Four ASHAs were interviewed at selected health facilities in their coverage area who were present during the antenatal check-ups (ANC) and immunisation service days. The detailed sampling scope and size are given in Table 1.
Sampling Size for Phase II Subjective and Objective Assessment.
Measuring Indicators and Data Sets
NHM has a comprehensive database of measuring indicators related to inputs, processes, outputs and outcomes, which indicate service access, availability, delivery, behaviour–knowledge, utilisation and coverage. During phase I of the study to measure the impact of NHM exclusively on MCH at the population level, five primary indicators of outcome and coverage were measured to represent proxy variables for impact, in addition to the measurement of four core impact indicators related to MCH: MMR, infant mortality rate (IMR), U5MR and total fertility rate (TFR).
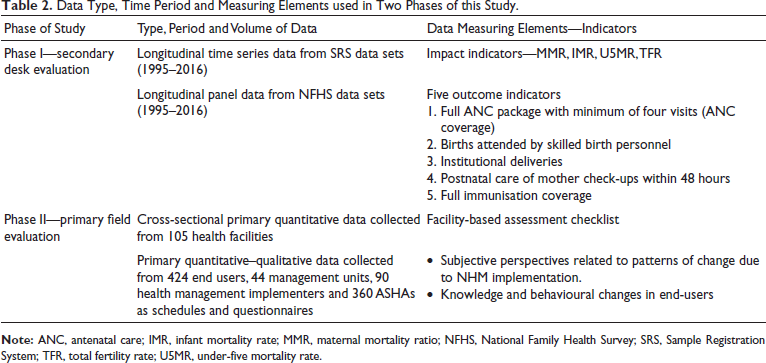
In order to ensure robustness and counter validity threats in the assessment of impact, the study used multiple cross-sectional data period sets, which helped us to apply a quasi-experimental longitudinal time series and panel data approach. We examined the time series data across the periods of pre-NHM (1995–2005) and post-NHM (2006–2016), with balanced data sets having 11 data points in each epoch for impact indicators. The amount of data structure, period and volume used, along with measuring elements, is shown in Table 2.
Data Type, Time Period and Measuring Elements used in Two Phases of this Study.
Measuring Impact and Model Analysis
To measure the average impact of the NHM programme, we estimated the average change in the pre-intervention and post-intervention measurements of indicator outcomes. The data sourced was put to descriptive analysis and hypothesis testing. Three different models of impact were devised for measurements; regression was used to explain whether the NHM intervention had any impact on the maternal child indicators during the 2006–2016 period.
Impact Estimation Techniques and Measuring Models
Interrupted Time Series Analysis Design (ITS-SLR)
In the impact evaluation of a naturally running programme, the use of longitudinal data is considered the best way to exploit the nature and outcomes in a population and is the most appropriate statistical tool for evidence-based implementation studies (Creswell, 2014; Winship & Morgan, 1999). Literature has defined the ‘ITS’ approach as the best methodological approach in mixed designs for evaluating health programmes with population-level data (López Bernal, 2018). It is the most robust and relevant research design in implementation sciences for public health programmes (Kontopantelis et al., 2015) and arguably the strongest research design when there is no control over the intervention and it is non-randomised, as in the case of NHM (Dimitrov & Rumrill, 2003). The inbuilt nature of the universality-operalisation of NHM into the existing health structure of the country and having a well-defined onset timeline and programme theory made ITS an ideal choice for impact assessment in this study.
Devising Impact Model for Measuring Change
The time series nature of impact variables with the repetition of cross-sectional data (panel data) of outcomes and covariates of the population made us to introduce the ‘fixed effect’ panel parameter, which allowed us to control for error terms and unobserved population heterogeneity in the regression equation, such as the time-invariant factors like geographical, demographical, political and cultural practices or changes that might have affected the impact or health outcomes.
The impact model was devised by using the advanced ITS segmental linear regression method to produce the most precise, unbiased estimation of impact and its magnitude. In this regression model, the controlling of time-varying measurable confounding factors such as maternal education, economic status [gross state domestic product (GSDP) used as proxy] and access to sanitation and drinking water facility was introduced to provide better model fitness (R2) and to reduce the measure of variability or variance on impact due to these factors.
‘Time’ was used as a proxy for the presence or absence of NHM exposure, using it as a dummy variable in regression analysis. It contributed to controlling for lurking exogenous, non-measurable, latent or unknown exposures, such as unrelated programmes, schemes or competitive interventions, as well as the introduction of newer health technologies that could affect health outcomes over the period and to also control for secular trends in data sets. Various sensitivity tests like the LM test and Hausman test were performed to confirm whether to go for fixed or random effects. To check for heteroscedasticity and serial autocorrelation, the Breusch–Godfrey test and White test were performed. Data of dependent variables were transformed to a logarithmic scale, and to reduce multicollinearity to less than variance inflation factor (VIF) of 5 in explanatory variables, they were either transformed into dummy variables or insignificant variables were removed from the model.
In this model, the ‘time’ proxy for NHM intervention was divided into the following periods, as per the segmental linear regression equation as:

Yt is outcome at time t, rate/ratio; ß0 = baseline data of outcome or variable of interest; ß1T1Xt=0 = change in outcome at pre-NHM period 1, ß2T2Xt=0 = change in outcome at pre-NHM period 2; ß3Xt= change in outcome at onset of NHM programme; ß4T1Xt=1 = change in outcome at post-NHM period 1; ß5T2Xt=1 = change in outcome at post-NHM period 2; εpt = error term.
Through the impact model, we were able to measure changes in the pre-NHM and post-NHM phases, quantify them, depict levels (intercepts), trends (slopes), and change scores-rates, correlate background and outcome variables with impact indicators, conduct attributional analysis of NHM, and ultimately compare and measure the sustainability of impact or outcome of the intervention.
Counterfactual Model of Estimation
One of the best ways to estimate changes from intervention is by measuring and comparing outcomes in the pre and post-programme periods, but such estimation is based on the assumption that outcomes in such a population would have remained unchanged in the absence of the intervention or such programme. However, to overcome such implicit unrealistic assumptions, we need to estimate the impact on a population in the absence of NHM intervention or how the population would evolve in absence of the NHM programme. This was done by constructing statistically counterfactual outcomes—multiple baseline pre-intervention observations were used to extrapolate and estimate the possible outcomes in the absence of the programme, assuming the future is like the past or controlling for secular trends and confounding factors in the future.
Counterfactual impact was estimated by using the autoregressive integrated moving average (ARIMA) method in the ITS model, which is ideal for time series panel data where autocorrelation is a common phenomenon with stochastic error terms. This model controlled for error terms, special non-measurable time-invariant exogenous factors and potential heteroscedasticity and the non-stationary nature of the data. The data were transformed to a natural logarithmic scale to make it skewness and variability free. An appropriate ARIMA model (1,1,1) was selected using the Box–Jenkins methodology (Gujarati & Porter, 1999) by analysing the autocorrelation function and the partial autocorrelation function. All diagnostic tests favoured the selected ARIMA model, with all values and parameters lying within the acceptable range. The time series data sets from 1995 to 2005 of four core impact indicators were used in the estimation of counterfactual values of impact indicators from 2006 to 2016 that would have occurred in the absence of NHM intervention or programme.
Results
The findings of this study were drawn from interpretative phase I secondary data analysis of NFHS-SRS data sets through three models of impact estimation, along with phase II attributional primary quantitative–qualitative data through objective and subjective assessment. The combined findings from phases I and II were done to arrive at a conclusion as to whether the NHM had an impact on the population or not and by what magnitude.
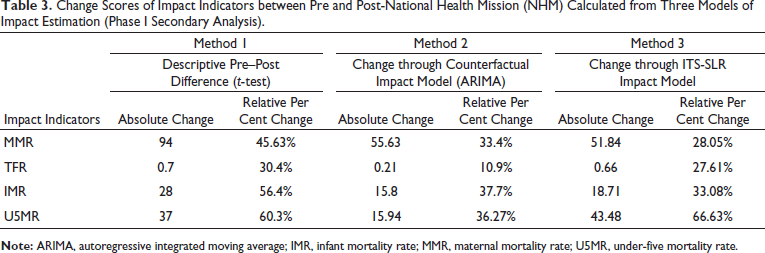
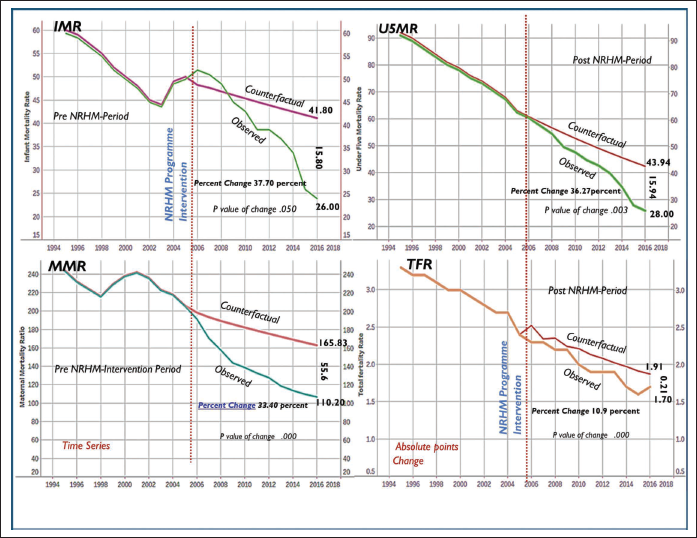
The findings from the phase I pre-post descriptive model, ITS-SLR model and counterfactual impact ARIMA model showed that all the four impact indicators of mother and child (MMR, IMR, U5MR, TFR) have reduced after the implementation of NHM, with the maximum change seen in MMR and U5MR. The absolute and relative change scores from all three models of impact (phase I analysis) are shown in Table 3.
Change Scores of Impact Indicators between Pre and Post-National Health Mission (NHM) Calculated from Three Models of Impact Estimation (Phase I Secondary Analysis).
The change during the early phase was slow, followed by a rapid and steady fall in the mid-phase, followed by stagnation and reduced annual reductions over the final phases of NHM implementation. The findings from the counterfactual ARIMA impact model have shown that there is a significant change in all four impact indicators. Figure 2 elaborates on the slope and intercept changes, along with the magnitude change between the observed values and the counterfactual values, as modelled by the ARIMA impact model.
Autoregressive Integrated Moving Average (ARIMA) Impact Model showing Intercepts, Slopes, Change Scores or Magnitude of Difference in Four Impact Indicators between National Health Mission (NHM) Intervention Outcome and in its Absence (Counterfactual Outcome).
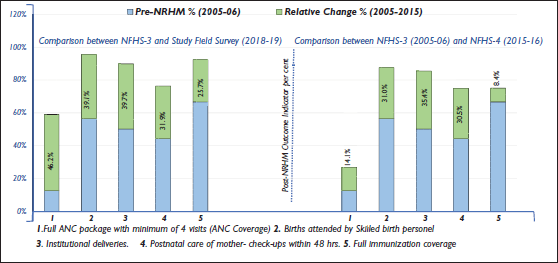
The phase I longitudinal panel data analysis of NFHS secondary data sets and phase II field assessment primary data revealed that the coverage of outcome indicators (also used as a proxy for impact or change) has improved due to the implementation of NHM, and the relative change percentages in five outcome indicators are shown in Figure 3. The maximum impact of NHM has been seen on institutional births as per the comparison between NFHS-3 (2005–2006) and NFHS-4 (2015–2016) data sets, whereas, as per the comparison between NFHS-3 and phase II field survey (2018–2019) of this study, the maximum change was seen on full ANC package content delivery. The study findings reveal that the most significant outcome indicators, which had an impact on mortality (MMR, IMR, U5MR), were births by skilled birth attendants (SBA) (p value < .019) and institutional deliveries (ID) (p value < .010).
Findings from both phases I and II of this study showed that NHM has increased the utilisation and coverage of services with better MCH outcomes like institutional deliveries and deliveries by professional attendants. The correlational and regression analysis of data sets has shown that exogenous factors like maternal education (Pearson Co. value 0.88), fertility rate (0.95), economic status (0.90), drinking water facility (0.90) and improved sanitation (0.73) have significantly contributed to a decrease in MMR over the intervention period and are the most important predictors for the utilisation of MCH services. These findings, which are consistent with the NHM theory of change, suggest that we must view the NHM strategy through the lens of social determinants, which are at work during the time of delivery and within the initial 7 days of the life of a newborn.
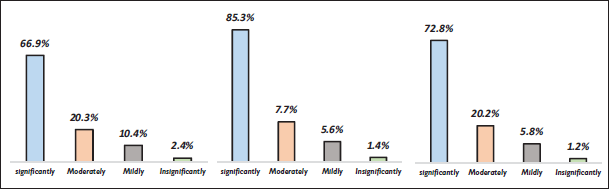
The phase II attributional mixed analysis measured the direct impact of NHM on beneficiaries and provided an understanding of the patterns of implementation and changes by NHM. Analysis showed that 67 per cent of beneficiaries (PW and mothers) are of the view that NHM had a significant positive impact on their lives, and around 85 per cent of ASHAs are of the opinion that NHM has a positive impact on the community they are serving with respect to MCH care. From the implementers’ perspective, 73 per cent are of the opinion that NHM has made a significant change in health behaviour–knowledge, and NHM has had the intended impact as per programme theory. These findings are consistent with the p values of change got through significance tests for different change scores. The findings are summarised in Figure 4.
Further findings with regard to structural factors have shown that there is a considerable increase in the number of health institutions, especially at lower levels of interventions like primary health centres and sub-centres, due to the NHM. Sub-centres providing basic reproductive and ANC services have increased from 368 to 2,805 (2005–2016) (six times increase) and primary health centres (PHCs) from 222 to 637 (three times increase). The number of health facilities per population has expanded over the years, and the coverage is more than the recommended norms. While the ratio of doctors to the population covered by our sampled health institutions was 1:2,200, as against the WHO recommendation of 1:1,000. Findings of the study showed that there is a lack of specialists like gynaecologists and paediatricians at district hospitals, while at PHCs there is a lack of lady doctors. The number of district hospitals has increased by 42 per cent; community health centres (CHCs)—first referral units with dedicated obstetric emergency services to manage maternal complications and provide neonatal services—have increased from 65 per cent to 91 per cent.
Discussion and Conclusion
Extensive research has been done on MCH outcomes, especially within the ambit of NHM from 2005 till date, but most of it has either examined a single intervention or used a limited number of impact indicators. Most of the studies undertaken were based on data sets from the early to mid-implementation (2007–2015) period of NHM; only a few studies (Ali et al., 2020; Kumar, 2021; Prinja et al., 2021) were undertaken during the final implementation stages of NHM. Most of the studies that reported no or limited impact were mostly based on the post-NHM data of 2007–2012. The two major studies conducted during the final implementation phase of NHM aimed to assess the impact of NHM, using limited indicator time series data of maternal–infant mortality (Kumar, 2021) or using only a single impact method (Prinja et al., 2021). One of the latest systematic reviews done on the impact of NHM (Singh & Vellakkal, 2021) has revealed that most of the studies on the effect of NHM had applied non-experimental designs with limited or no qualitative nature, and most studies assessed the impact on the intermediate outcomes of MCH rather than the long-term outcomes.
This study measured the levels, trends and changes in impact and outcome indicators of MCH at the population level in the pre-NHM and post-NHM periods, and further understanding of the implementation framework of NHM at different levels of functionality was done to augment the findings of the impact model analysis, find out the level of agreement, and to get a broader picture of the impact at the ground level. This study tried to overcome the methodological impact estimation limitations, as seen in many studies (Doke, 2016; Khurmi et al., 2015; Kumar, 2021; Kumutha et al., 2014; Prinja et al., 2021; Singh et al., 2014), by not only using longitudinal time series and panel data but also simultaneously using mixed primary cross-sectional field data with a theory-driven approach. This study showed that the simultaneous use of triangulated approaches, along with the use of time series and counterfactual estimation, can be used successfully for the impact evaluation of health programmes like NHM.
This study, through its mixed methodological findings from all three impact models of estimation along with the attributional phase, showed that there is a significant increase in MCH outcome indicators and a decrease in impact indicators, and these findings are consistent with other studies on the effect of NHM on maternal, neonatal and child mortalities (Kumar, 2021; Prinja et al., 2021).
Systematic review studies done on MCH outcomes have shown that the various components of NHM have increased antenatal care, institutional delivery, skilled birth attendance, postnatal care and other MCH indicators (Glassman et al., 2013; Singh & Vellakkal, 2021), and outcomes are shaped by a complex set of social and healthcare system barriers, facilitators and predictors (Hunter et al., 2017), which are consistent with the findings of this study.
The most important factors and activities that have contributed to better health outcomes in mother–child are the institutionalisation of births (a proxy for safe births) and delivery by a skilled health worker, which is proxy for complication-free deliveries; both have significantly decreased mortalities. Many studies have shown similar results, associating NHM with increased institutional and skilled birth deliveries, especially in rural and socially privileged communities (Agarwal et al., 2019; Ali et al., 2020).
This study further attributes the success of NHM at the implementation level to the flexibility of operations, the outreach mode of implementation, incentivisation of services, improvement in structural determinants and the communitisation of health service delivery at doorsteps, especially provided by ANMs and ASHAs, as also shown by various other studies (Gupta et al., 2012; Singh et al., 2014). This study showed that the implementation of NHM over the years has led to a quantitative improvement in the number of health facilities, especially lower-level health facilities, and the recruitment of additional staff has resulted in greater annual reductions in impact indicators.
The attributional and contextual findings of this study have shown that there are operational gaps in time adequacy–attentiveness, communication quality, access to diagnostics–drugs given to beneficiaries (PW and mothers) and postnatal stay at the hospital after delivery, which have affected their utilisation of services and resulted in a low percentage of postnatal indicator coverage.
Finally, with respect to mortality indicators of MCH, this study has shown through its models of impact that these have significantly declined due to the implementation of NHM over the years. Similar positive findings have been given by other studies also (Kumar, 2021; Pandey & Mohan, 2018; Prinja et al., 2021).
Policy Implications
The findings of this study have important policy implications both at the regional and country levels by providing evidence-based strategies and relevant information, as per the assertion already made in the NHP 2017 and UHC 2030, which suggest strategies to strengthen the health system through the supply side, improving infrastructural and service inequities and demand side projections, with financial risk security, especially for underprivileged sections, leading to increased access and utilisation (Singh & Vellakkal, 2021).
Improving the health of the mother–child ecosystem, with access to basic comprehensive primary health and maternal emergency care at its core, can make substantial improvements in MCH outcomes, ultimately translating into long-term benefits like increased economic growth, stronger societal bonds, improved community resilience, better lifetime earnings, increased capital productivity (Kagitcibasi et al., 2009; Richter et al., 2017; Yousafzai et al., 2014) and the value of life years saved (Cropper et al., 2011). Mortality and other health ailments of reproductive women have adverse ramifications on the economic and social structure of their family and community and have been reflected in poverty and up to a 20 per cent decrease in family earnings (Victora et al., 2015). Also, low spending by the government has resulted in more out-of-pocket expenditure (OOPE) by health consumers, resulting in a large cohort of population (nearly 30 per cent every year) being thrown into poverty. This reduced public expenditure has acted as a barrier to universal access and affordability of health care.
The study also highlights that to have a holistic development of MCH, we need a broad-based approach with the inclusion of local community priorities, inclusion of socio-structural determinants, reduction of OOPE related to birth, strengthening of the management capacity of health information and monitoring-evaluation systems, supply chain service infusion strategies and quality enhancement through multi-skilling and multitasking to optimise service quality deliverance, which should be effective, equitable and affordable. Early, continued and sustained physical and financial investments during the life course of maternal–infant health will avert around 50–75 per cent of maternal deaths and around 60–90 per cent of deaths in children (Bhutta et al., 2013).
Limitations of Study
The average impact of NHM interventions may be influenced by other concurrently running socio-economic programmes that may affect the outcomes of NHM and produce heterogenous impact, and it is preferable to identify and include these lurking programme variables as part of the theory of change.
Conclusion
The UT of Jammu and Kashmir has already achieved MCH targets of millennium development goals (MDG) and is on the path towards achieving SDG goals. The NHM in Jammu and Kashmir, through its multidimensional approach, has made a significant impact on MCH care despite the huge challenges of political fragility and harsh topography. The ‘brand NHM’ since its inception has emerged as a crucial financial and equity modelling reform programme, which has improved the utilisation of services, increased coverage and enhanced health awareness. The NHM continues to be a guiding framework towards achievement of UHC and has led to affluent investment and recognition in regenerating Indian public health care. There is a need to accelerate the service quality under NHM and evolve strategies that reemphasise from ‘birth preparedness’ to ‘complication preparedness’, in order to follow the SDG targets. Further, we need to rethink and reorient our public policy intervention programmes like NHM that have not been reoriented and reshaped based on evidence from implementation analysis and impact evaluations.
Future research needs to understand the interconnection between management strategies and health processes through impact evaluations using mixed qualitative approaches and focus on efforts that deliver sustained, cost-effective services and try to forge a data-driven model of implementation with quality-adjusted measures of MCH services and their continuum of care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.