
Abstract
Cultural humility, an approach to care that is rooted in self-reflexivity, regard for patients’ lay expertise, and openness to sharing power with patients, is pivotal in delivering health services to people with diverse sociocultural characteristics. Without cultural humility in clinical encounters between health care providers and patients, illnesses may be treated, but the patients are poorly understood. This work investigates the barriers to practising cultural humility among healthcare workers in Nigeria, a culturally diverse country. A qualitative online survey collected data from 52 health professionals between May and July 2024. Participants were recruited across primary, secondary and tertiary health facilities, as well as across the six geopolitical zones in Nigeria, to enable the transferability of findings. Purposive sampling was employed for selection. Thematic analysis was performed on the data, and member checks were used to ensure rigour and trustworthiness. The barriers are categorised into human resources for health, patient, and leadership and governance levels. The obstacles within human resources for health include the lack of training on cultural humility, shortage of health workers, low motivation among service providers resulting from poor remuneration, and limited cultural and religious diversity among providers, as well as among leadership actors in the health system. The patient-level hindrances encompass patients’ limited English proficiency and reluctance to engage in open dialogue about their cultural backgrounds and health care preferences during clinical encounters with health professionals. Finally, the barrier at the leadership and governance tier stems from hierarchical organisational culture. These findings not only underscore the urgency of reform but also provide a roadmap for fostering a culturally sensitive health system.
Introduction
In the health care setting, cultural humility refers to an orientation towards caring for one’s patients that is based on self-reflexivity and assessment, appreciation of patients’ expertise in the social and cultural context of their lives, openness to establishing power-balanced relationships with patients, and a lifelong dedication to learning (Kirmayer, 2012; Lekas et al., 2020; Tervalon & Murray-Garcia, 1998). Cultural humility encourages health service providers to reflect on their own beliefs, values and biases—explicit and implicit—through introspection, thus revealing their own culture’s impact on patients (Agner, 2020; Botelho & Lima, 2020; Lekas et al., 2020). It means admitting that one has limited knowledge or does not know and is willing to learn from patients about their experiences, while being conscious of one’s own embeddedness in culture (Lekas et al., 2020). It is different from cultural competence in that the latter often results in the reproduction of social stereotypes and imbalanced power relationships between service providers and patients, whereas cultural humility often results in an intrapersonal and interpersonal approach that cultivates person-centred care (Lekas et al., 2020). The call to abandon cultural competence and improve the practice of cultural humility among healthcare workers is well-supported in the international literature (e.g., Foronda et al., 2016; Lekas et al., 2020).
Nigeria is a culturally diverse country with over 250 ethnic groups. Given this, health professionals in the country may encounter patients from diverse sociocultural groups daily. These professionals in the country should practise cultural humility, as this is essential to delivering health services to people from diverse sociocultural groups (Tervalon & Murray-Garcia, 1998). In addition, culture shapes lifestyles and beliefs that affect people’s health, and without cultural humility in clinical encounters between service providers and patients, illnesses may be treated, but the patients are poorly understood (Chang et al., 2012).
Understanding the barriers to carrying out cultural humility among Nigerian health care providers can inform actions for improving its practice. We are not aware of any study conducted in Nigeria that explored the obstacles to practising cultural humility among healthcare workers. However, there are related Nigerian works, which underscore the need to improve the implementation of cultural humility in various care contexts, including cancer care (Nwozichi et al., 2021), eye care (Okoye et al., 2018) and mental health care (Lasebikan, 2016). There are also related Nigerian works that advocate for cultural competence practice among health service providers (Ogunlana et al., 2023). However, as mentioned, cultural competence is an orientation that must be abandoned.
This study aims to investigate the barriers to practising cultural humility among Nigerian service providers. It would also inform actions for enhancing its implementation during clinical encounters between providers and patients, thereby strengthening service delivery and patient outcomes in the country.
Methods
Design
The work employed a qualitative research design to gather in-depth insights from health care providers.
Sampling and Participants
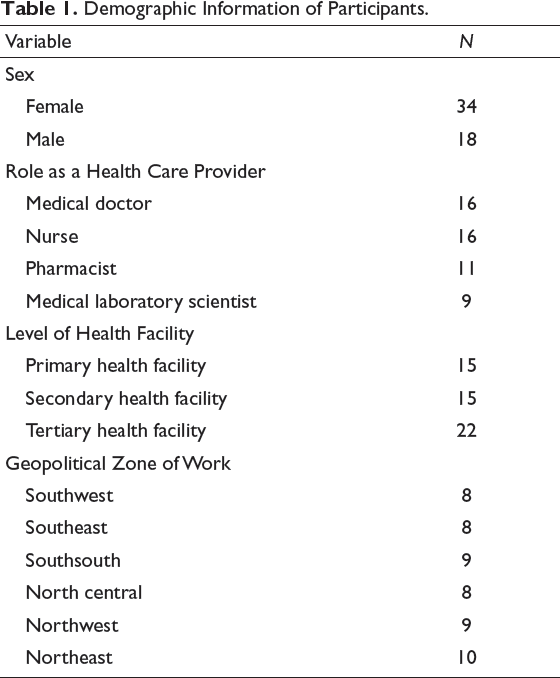
Purposive sampling was executed to enable the recruitment of health professionals with a wide range of demographic characteristics. Fifty-two participants with an age range from 24 to 64 years participated in this study. The participants included medical doctors (specialised in paediatrics, surgery, infectious diseases, palliative care, psychiatry or family medicine), nurses, pharmacists and medical laboratory scientists. All participants had received education from a tertiary educational institution. They were selected across primary, secondary and tertiary health facilities, as well as across the six geopolitical zones in Nigeria. The demographic information of participants is summarised in Table 1. Eligible participants were health care providers aged 18 years or above in the Nigerian health system.
Demographic Information of Participants.
Data Collection Tools
The study made use of a qualitative online survey created through Google Forms for data collection. The decision to use this lies in the authors’ intention to access providers with a wide range of demographic characteristics in a cost-effective manner. In addition, the recruitment of participants with a wide range of demographic information potentially enables the transferability of findings from this study.
The online survey encompassed three sections. All sections were compulsory to complete. The first section provided information on the meaning of cultural humility as well as the study’s aim. In addition, it obtained consent from participants and politely requested them to provide comprehensive responses. The second component elicited demographic data from participants, including sex, age, highest educational qualification, role as a health care provider, level of health facility that the participant works in and geopolitical zone of work. The third part contained the following questions to address our study’s aim:
Please describe the barriers you face to practising cultural humility during your provision of health care to patients. Please describe the characteristics of your patients that prevent you from carrying out cultural humility during your provision of health care to them. Please describe actions from your patients that prevent you from practising cultural humility during your provision of health service to them. Please describe factors within the leadership and governance of the Nigerian health system that hinder you from practising cultural humility during your provision of health care to patients. Are there additional contributions you would like to make to this topic? If yes, please do so!
The five questions were informed by the literature on cultural humility in the health care setting (e.g., Chang et al., 2012; Foronda et al., 2016; Foronda, 2020; Lechner et al., 2024; Lekas et al., 2020; Tervalon & Murray-Garcia, 1998). The authors read and discussed these works to design and develop the five questions. All survey questions were piloted and revised before the main study. The pilot phase was carried out among 11 providers from diverse contexts of care, and they were excluded from the main study. Ethics approval was received from the University of Ibadan, Nigeria.
Data Collection
The authors searched for Nigerian health professionals from a wide range of care contexts through LinkedIn. As the authors found the professionals, they carefully selected those who were diverse in several demographic variables beyond care contexts (e.g., sex, educational background, level of health facility and geopolitical zone of work). The selection implied sending these professionals a direct message (DM). The direct message contained a statement inviting participation in the study, information on the study’s aim, eligibility criteria, ethical considerations, and a link to access the online survey.
Fifty-two participants were contacted and all submitted complete responses. One response per participant was permitted in the study. Data sufficiency was determined through data saturation. At the commencement of data collection, the authors visually assessed and discussed the data weekly to ascertain saturation. When it was detected in the 52nd response, the collection of data was terminated. The data collection occurred between May and July 2024.
Analysis of Data
The first author (IAO) manually performed the data analysis using a data-driven lens. Thematic analysis informed by Braun and Clarke (2006) was the approach employed. This approach to data analysis was chosen to enable a succinct report of findings from the online survey (Braun et al., 2021). To carry out the thematic analysis, participants’ responses were downloaded in a Microsoft Excel file and transferred verbatim to a Microsoft Word document. Following this, a deep mental engagement with the data occurred through reading and rereading the data. During this process, themes were created, described and supported with quotes (Maguire & Delahunt, 2017).
The created themes were sense-checked by the remaining authors (RUM, ABO, AIB, OIE, and OOO) to inform refinement. Following this, the created themes were presented to six professors in health services research for further review and refinement. Eight participants also reviewed the themes and suggested areas for refinement. These reviews and refinements added rigour and trustworthiness (Tobin & Begley, 2004), and led to the finalisation of themes (Braun & Clarke, 2006). The standards for reporting qualitative research were adhered to in the current work (O’Brien et al., 2014).
Findings
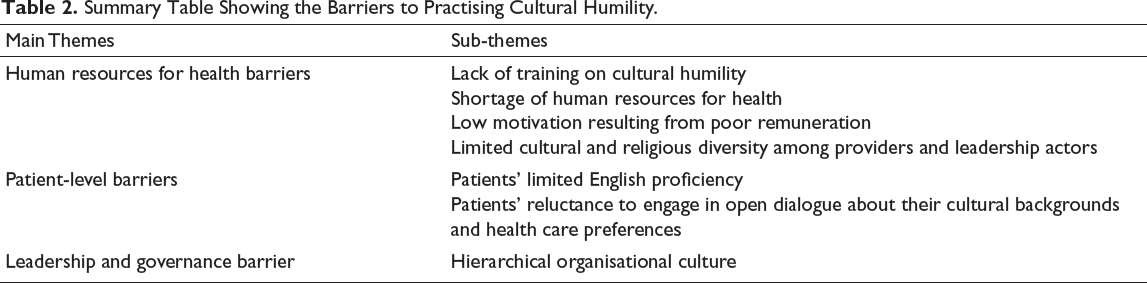
This section reports findings (main themes and sub-themes) on the barriers to practising cultural humility. No barrier was unique to any demographic information of the participants. Table 2 presents a summary of the findings.
Summary Table Showing the Barriers to Practising Cultural Humility.
In the report of findings below, a single quote was often used to provide more information on the themes to enable a lucid report of data.
Human Resources for Health-level Barriers
Most participants reported barriers at the human resources for health level. The barriers were in four subsets. First was the lack of training on cultural humility for healthcare workers, underscoring the need for human resources for health development programmes to prioritise training on cultural humility.
An obstacle I encounter to doing this (cultural humility) in health service provision primarily stems from my lack of personal experience (including training) on cultural humility. [Medical doctor, Female, 35 years]
Second was the shortage of healthcare workers, highlighting the need for human resources for health sufficiency.
High workload and limited time for provider-patient interaction, which are due to inadequate staffing, hinder us (health care providers) from wanting to understand patients’ culture and how it affects their health. This is because when you are the only health care provider in the ward, and you have over 20 patients to see, you would want to be fast in your provision of health care rather than provide individualised care. [Medical doctor, Male, 40 years]
Third was low motivation among health service providers, resulting from poor remuneration. The finding highlights the role of fair remuneration in providing well-motivated health workers and better service delivery.
Health professionals are underpaid. For this reason, most of us are unmotivated to provide culturally appropriate care to patients. All we care about is that our patient’s symptoms are treated. [Nurse, Female, 64 years]
Last was limited cultural and religious representation among providers, as well as among leadership and governance actors in the health system
A lack of heterogeneity (including cultural and religious) among health care staff (e.g., doctors or nurses in the ward) contributes to monocultural perspectives, thereby hindering the implementation of cultural humility among the staff. [Medical laboratory scientist, Female, 61 years]
Limited cultural diversity in leadership roles - A lack of cultural diversity among individuals performing leadership functions within the healthcare system results in similar cultural perspectives dominating decision-making processes, overlooking the importance of cultural humility in patient care. [Pharmacist, Male, 47 years]
Patient-level Barriers
Many participants highlighted two obstacles at the patient level. First was the patients’ limited English proficiency (LEP).
Language barrier – many times, we have patients who cannot communicate using the English language. As a result, we find it hard to align with such patients’ cultural perspectives and to have equal power interactions with them. [Pharmacist, Male, 24 years]
Last was patients’ unwillingness to communicate their cultural backgrounds and health care preferences during their clinical encounters with service providers.
Patients are reluctant to engage in open dialogue about their cultural backgrounds and health care choices, representing barriers to executing cultural humility. [Medical doctor, Female, 58 years]
Leadership and Governance-level Barriers
Finally, participants reported hierarchical organisational culture, which limits communication and collaboration between providers and patients, as a hindrance at the leadership and governance tier. The finding suggests the need for a positive organisational culture that promotes open dialogue and partnership between service providers and patients.
Hierarchical organisational culture is common in the Nigerian healthcare system. This kind of culture discourages honest conversations and alliance between healthcare workers and patients, making it difficult to address cultural issues that affect patient care. [Nurse, Female, 42 years]
Discussion
To the best of our knowledge, this is the first study to identify the barriers to practising cultural humility among health care providers in Nigeria, a culturally diverse country. Fifty-two providers with a wide range of demographic characteristics participated in this qualitative work. The findings reveal that the barriers to implementing cultural humility include factors at the human resources for health, patient, and leadership and governance levels.
The hindrances within human resources for health encompass a lack of training on cultural humility, a shortage of healthcare workers, low motivation among providers resulting from poor remuneration, and limited cultural and religious diversity among providers, as well as among leadership and governance actors in the health system. These barriers are well-known problems in the Nigerian health system literature (e.g., Ogueji, Motajo, et al., 2024; Ogueji, Ogunsola, et al., 2024a); however, the current study extends the literature by linking these problems to cultural humility. In addition, the barriers support the World Health Organization’s assertion that health care providers must be culturally equipped, sufficient, and well-motivated to provide health services that are appropriate and acceptable to the sociocultural expectations of patients (World Health Organization, 2016).
The patient-level barriers are patients’ LEP and reluctance to engage in open dialogue about their cultural backgrounds and health care preferences. The barrier of LEP corroborates the work of Allen et al. (2020), which noted the need for language interpreters and translators in health care contexts. The finding that patients are reluctant to engage in open dialogue about their cultural backgrounds and healthcare preferences suggests that patients are stakeholders in health service delivery, aligning with the work of Street et al. (2012).
The obstacle at the leadership and governance tier includes the presence of a hierarchical organisational culture. Indeed, hierarchical culture in health care settings can hinder culturally appropriate care and lead to adverse patient outcomes (Braithwaite et al., 2017).
The current study has some limitations. Although the online survey resulted in the recruitment of providers with a wide range of demographic characteristics, it might give room for missed insights from those without or with restricted internet access who had different perspectives. Cultural humility is a bi-directional process, requiring equal investment from healthcare workers, patients and their families, and the community (Chang et al., 2012). As the present research did not include all of these groups, future work should examine strategies for improving cultural humility from the perspectives of patients, their families, and relevant community stakeholders. Additionally, healthcare workers such as clinical/health psychologists and social workers who also engage in provider-patient interaction were not represented in the study. Further research can address this gap. Despite the limitations, this study adds to the limited global discussion on cultural humility in health care contexts, and it can be used to foster a culturally sensitive health system. The present research also supports the cultural humility theory by showing that factors such as diversity and provider-patient partnership are linked to the implementation of cultural humility (Foronda, 2020).
Implications
The government, health service managers, professional associations and relevant stakeholders must address the barriers to enhance the practice of cultural humility, thereby strengthening health service delivery and patient outcomes in the country. To tackle the barriers, we offer some suggestions.
Continuing professional development (CPD) programmes aimed at training providers on cultural humility must be prioritised in the health system. The training should focus on the meaning of and how to practise cultural humility. Professional associations can organise such programmes. Additional research is needed to understand what drives patients’ reluctance to engage in open dialogue about their cultural backgrounds and health care preferences during clinical encounters with providers. Insights from such research should guide the design and execution of interventions to address the issue.
The size of the healthcare workforce needs to be improved. In a recent study, Ogueji, Ogunsola, et al. (2024b) suggested that understanding the drivers of health staff shortages and formulating policies to address them are essential to strengthening staff size. Future works should act on this suggestion. Furthermore, service providers must receive fair remuneration. The World Health Organization (2016) recommends that efforts to ensure fair remuneration should consider the appropriateness of the remuneration to skills and contributions. In addition, the efforts should regard timely and regular payment as a basic principle, meritocratic reward systems, and opportunities for career advancement.
The finding of limited cultural and religious diversity among health service providers, as well as among occupants of leadership roles in the health system, contradicts the country’s rich cultural diversity and implies that it is yet to reap the full benefits of its cultural diversity. Hence, additional research should investigate hiring processes, as well as career development and mentorship factors that hinder cultural and religious representation among providers and leadership actors in the Nigerian health system. Positive organisational cultures that discourage power imbalances and encourage honest conversation and collaboration between healthcare workers and patients are called for. Finally, professional language interpreters and translators must be present across health facilities to enable communication between providers and patients from a wide range of cultural backgrounds.
Footnotes
Acknowledgement
The authors thank the participants of this study for their time.
Authors’ Contributions
IAO: Conception, study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article, and final approval of the version to be submitted.
RUM: Study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article, and final approval of the version to be submitted.
ABO: Study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be submitted.
AIB: Study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be submitted.
OIE: Study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be submitted.
OOO: Study design, data collection, data analysis and interpretation, drafting the article, critical revision of the article and final approval of the version to be submitted.
The content of this article is solely the responsibility of the authors and does not represent the views of their affiliations.
Consent to Participate
Consent was obtained from all participants prior to data collection.
Consent for Publication
All authors consent to the publication of this article in the Journal of Health Management. All participants consent that findings from their data should be published in this article.
Data Availability
The data associated with this study are available from the corresponding author upon request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Declaration
This study was in accordance with the 1964 Helsinki Ethical Declaration, its later amendment, or a comparable standard.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.