
Abstract
This observational study assessed the psychological impact of COVID-19. 520 nurses (263 not involved in COVID-19 care and 257 involved) responded to an online survey. 24 nurses in Maharashtra (19 women and 5 men) were interviewed by telephone. Depression, anxiety and stress were measured using the Depression Anxiety Stress Scales (DASS-21)-short version PTSD with the Impact of Event Scale-Revised (IES-R). Descriptive, bivariate analyses and logistic regression were conducted. For the qualitative component, a qualitative-phenomenological approach was used. Higher mean DASS-21 depression, anxiety and stress subscale scores, and higher total IES-R and subscale scores were observed among nurses involved in COVID-19 care compared to those not involved. Qualitative findings indicate increased workload, longer distance from family and constant fear of infection and transmission, along with coping strategies. Screening and support mechanisms for nurses in COVID-19 care in India are needed to manage immediate and long-term psychological outcomes.
Keywords
Introduction
On 30 January 2020, the day the WHO declared the novel coronavirus (COVID-19 or SARS-CoV-2) a pandemic of worldwide concern, India reported its first case (World Health Organization, 2020). Since then, the disease has expanded throughout India, infecting 33.53 million people, 308,069 of whom have active cases; 32.78 million of whom have recovered; and 445,801 of whom have died as of 22 September 2021 (Worldometer, 2021). Similar figures were obtained for Kerala and Maharashtra: 4.55 million confirmed, 4.37 million recovered and 24,039 deaths for Kerala, and 6.53 million confirmed, 6.34 million recovered and 138,664 deaths for Maharashtra (India COVID-19, 2021).
Multidisciplinary teams were sent by the centre to Kerala and Maharashtra to help state governments effectively combat the pandemic (Dasgupta, 2020; Press Trust of India, 2021a). Under these conditions, healthcare workers, particularly nurses in the afflicted states, faced a severe workload (Archana, 2021). As of December 2020, over 3,744 nurses in Maharashtra had COVID-19 infections, and 11 of them died as a result of their infections (Mascarenhas, 2021). Approximately 23% of nurses in Kerala contracted the virus while performing their duties, primarily due to the inadequate availability of personal protective equipment (PPE) kits (Smitha, 2021). According to estimates provided by the Union Government, as of 5 February 2021, 116 nurses had succumbed to COVID-19 nationwide (Press Trust of India, 2021b).
Compared to other healthcare professionals, nurses have worse mental health and anxiety outcomes, especially those directly interacting with COVID-19 patients (Guo et al., 2020; Lai et al., 2020; Lu et al., 2020; Mishra, 2021; Sahebi et al., 2021; Zhang, Wang, et al., 2020; Zhu et al., 2020). However, research on the psychological effects of the COVID-19 pandemic on nurses in India is lacking (Mishra, 2021). Research on COVID-19’s mental health effects has focused on healthcare professionals (AlAteeq, 2020; Ali et al., 2020; Khanal et al., 2020; Lasalvia et al., 2020; Mathur et al., 2020; Suryavanshi et al., 2020; Tan et al., 2020). Most studies on nurses are cross-sectional (Hong et al, 2021; Jose et al., 2020; Sampaio et al., 2020; Sarboozi Hoseinabadi et al., 2020; Xiong et al., 2020; Zhan et al., 2020; Zhang, Wei, et al., 2020; Zheng et al., 2021). Only one Iranian study evaluated COVID-19’s effects on nurses performing COVID-19 tasks versus those who were not (Sarboozi Hoseinabadi et al., 2020). This study assessed depression, anxiety, stress, posttraumatic stress disorder (PTSD) and associated risk factors to evaluate COVID-19’s psychological impact in Kerala and Maharashtra among nurses involved and not involved in COVID-19 care.
Methods
Quantitative Study
This cross-sectional study used an online survey and was published in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (von Elm et al., 2007).
During the COVID-19 pandemic, nurses from public and private health institutions in Maharashtra and Kerala, India, were included.
Previous research on the psychological impact on nurses has reported varied sample sizes, ranging from 470 to 4,692 (Hong et al., 2021; Tan et al., 2020). However, these studies did not differentiate between nurses who provided care for COVID-19 patients and those who did not. Our primary challenge was to identify hospitals designated for COVID-19 care in Kerala and Maharashtra and subsequently contact their nursing staff. Due to the lack of available data on nurse employment in these states, we were unable to statistically determine the sample size. The questionnaires were distributed directly to the nurses or through nursing heads or societies.
Data collection using the online survey form was conducted in Kerala and Maharashtra between 8 September 2020 and 31 October 2020. The criteria included nurses in training or employed in selected institutions in these states, chosen based on the authors’ presence (SR, RL, SG, KST, MST and CV). The authors identified institutions where they had access to nursing heads or nurses through office members linked to nursing societies. A non-probabilistic snowball sampling approach was used through some contacted nurses to identify more nurses. Using these contacts, nurses’ email IDs were obtained. Data were collected using a questionnaire comprising two major headings: Background details (age, sex, marital status, education, residing with, monthly income and state) and occupation details (designation, specialty, institution, working hours/day, nature of duties and involvement in the care of persons with COVID-19) (Annexure 1). A Google Form was used to create an online survey questionnaire in English (Annexure 1). These were eventually translated into Marathi (for Maharashtra state) and Malayalam (for Kerala state). Members of the study team (SR, RL, SG and CV) mailed forms in both English and the local language to each nurse on their contact list in the chosen states. These activities were coordinated by two authors (CV for Kerala and SR for Maharashtra). To guarantee that these forms were accessible to the majority of nurses working in the states of Kerala and Maharashtra, the author team members (SR, RL, SG and CV) used their existing contacts with hospitals, nurses and nursing organisations. The survey also included nurses who were quarantined.
Depression, anxiety and stress were measured using the Depression Anxiety Stress Scales-short version (DASS-21). DASS-21 has no direct implications for the allocation of patients to diagnostic categories as described in the International Classification of Diseases and Diagnostic and Statistical Manual of Mental Disorders (Lovibond & Lovibond, 1995).
For our study, we used the validated Malayalam version of the DASS-21 (Manoj et al., 2018). Although we translated the Marathi version, all the responses were in English, as the respondents had the choice of using either language version. The Malayalam version of the DASS-21 had a Cronbach’s alpha of .85 for the depression scale, .85 for the anxiety scale, and .84 and .87 for the stress scale. Similar values for the Marathi version of the DASS-21 were .95, .92 and .94 for the depression, anxiety and stress scales, respectively. The Cronbach’s alphas of the three DASS-21 subscales across both language versions were .90 for depression, .89 for anxiety and .91 for stress.
The psychological impact of COVID-19 was measured using the Impact of Event Scale-Revised (IES-R) scale. The IES-R is a self-administered 22-item questionnaire that has been extensively used to determine the extent of psychological impact after exposure to a public health crisis, including infectious disease outbreaks (Reynolds et al., 2008; Wang et al., 2020). The total IES-R score is divided into 0–23 (normal), 24–32 (mild/moderate psychological impact, scores in this range suggest PTSD is a clinical concern), 33–38 (moderate psychological impact, scores in this range represent a probable diagnosis of PTSD) and >39 (severe psychological impact) (Christianson & Marren, 2012). DASS-21 and IES-R have been previously used in mental health research related to the COVID-19 pandemic (Sampaio et al., 2020; Tan et al., 2020).
Descriptive analysis was conducted to obtain the baseline characteristics of the nurses. In contrast, bivariate analysis was used to measure the mean and prevalence of depression, anxiety, stress and PTSD in nurses involved in COVID-19 care and not involved in COVID-19. Chi-square statistic test was used for prevalence ratio for categorical variables, while Student’s t-test was used to compare mean differences among continuous outcomes. Multivariable binary logistic regression was used to identify the factors associated with PTSD, depression, anxiety and stress. Missing data were not included in the analysis. Stata 13.1 (StataCorp., 2013) was used to conduct all statistical analyses.
Qualitative Study Methods
Semi-structured interviews (N = 24; 19 women and 5 men) using open-ended questions (Annexure 1) were conducted by a co-author (SR) via telephone in November 2020 to gain insight into nurses’ perceptions and feelings. Participants were encouraged to speak openly, highlight issues and use examples. They could withdraw consent anytime. Interviews were audio-recorded and confidential, lasting 20–40 min. Interviewers remained neutral, establishing rapport through acceptance, active listening and clarification to ensure authenticity and minimise bias. Care was taken to ensure respondents’ privacy before answering questions.
The interviews were transcribed by one author (SR) to identify key words and phrases. SR validated these transcripts telephonically with participants to reach consensus. Codes were assigned and arranged into theme categories. Core themes from the data were reordered conceptually and placed back into context, enabling integration of data and generation of abstractions. The study used a qualitative-phenomenological approach for an in-depth understanding of the phenomenon by exploring participants’ experiences. Analysis was conducted by a co-author (SK) using Microsoft Excel for coding, reported in accordance with the consolidated criteria for reporting qualitative studies (COREQ) checklist (Booth et al., 2014).
The study was approved by the Institutional Ethics Committee of Believers Church Medical College (IEC/2020/04/138). All procedures involving human participants followed the ethical standards of the 1964 Helsinki Declaration and its later amendments or similar ethical standards. Participants were requested to provide informed consent as the first part of the online Google Form prior to entering their personal information (Annexure 2).
Results
Quantitative Results
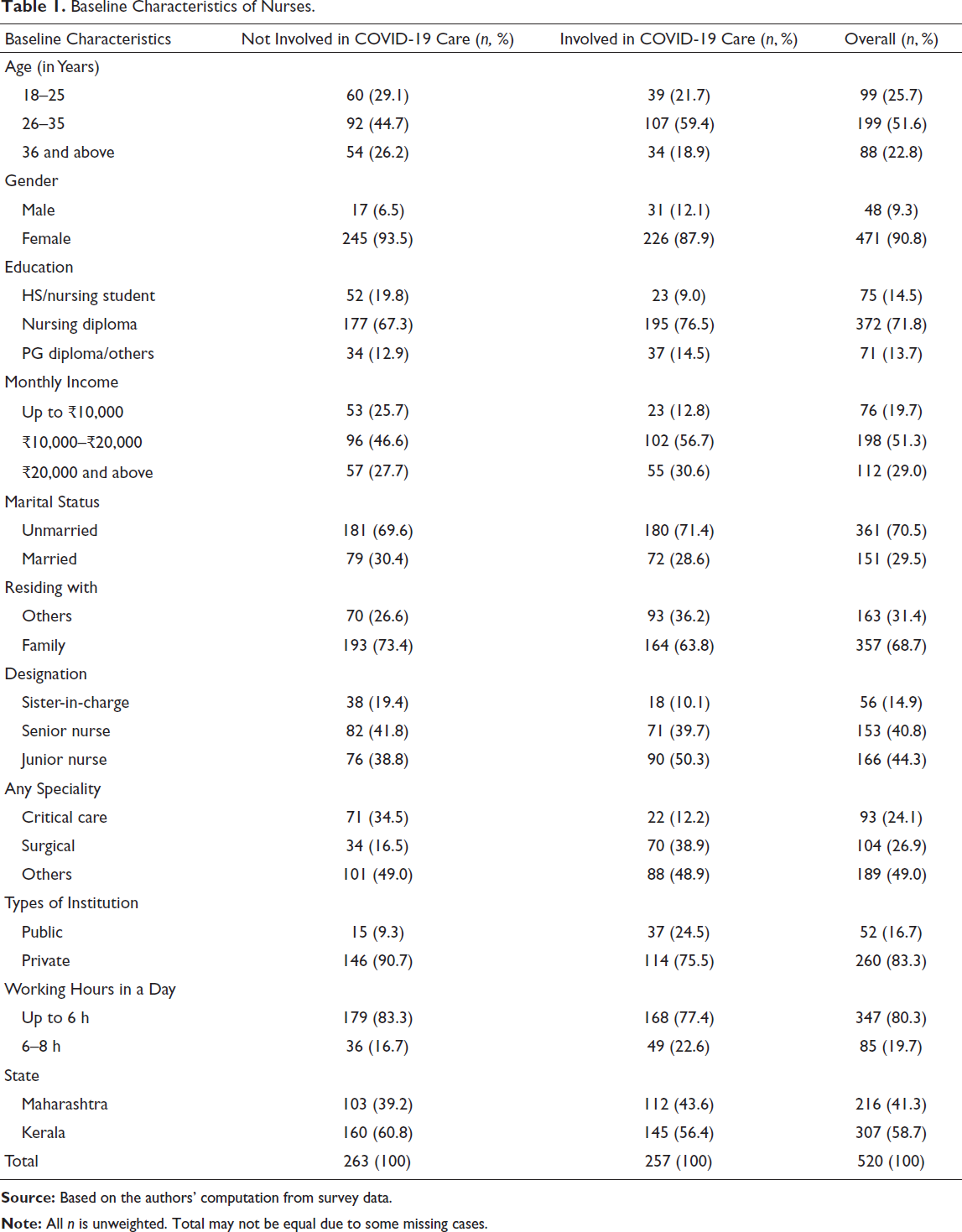
The sample comprised 520 nurses (263 not involved and 257 involved in COVID-19 care) (Table 1). In Maharashtra, 112 nurses were involved, and 103 were not in COVID-19 care. In Kerala, the numbers were 145 and 160, respectively. The majority of the nurses were in the 26–35 age group, with females comprising 90.8% of the total. Across both categories, most nurses had a nursing diploma, earned ₹10,000–₹20,000, were unmarried and lived with family. Over 50% of COVID-19 care nurses were junior, followed by senior nurses (39.7%). 15.6% were in surgical care and 12.2% in critical care. Most nurses worked in private facilities and worked for a minimum of 6 h daily across both categories.
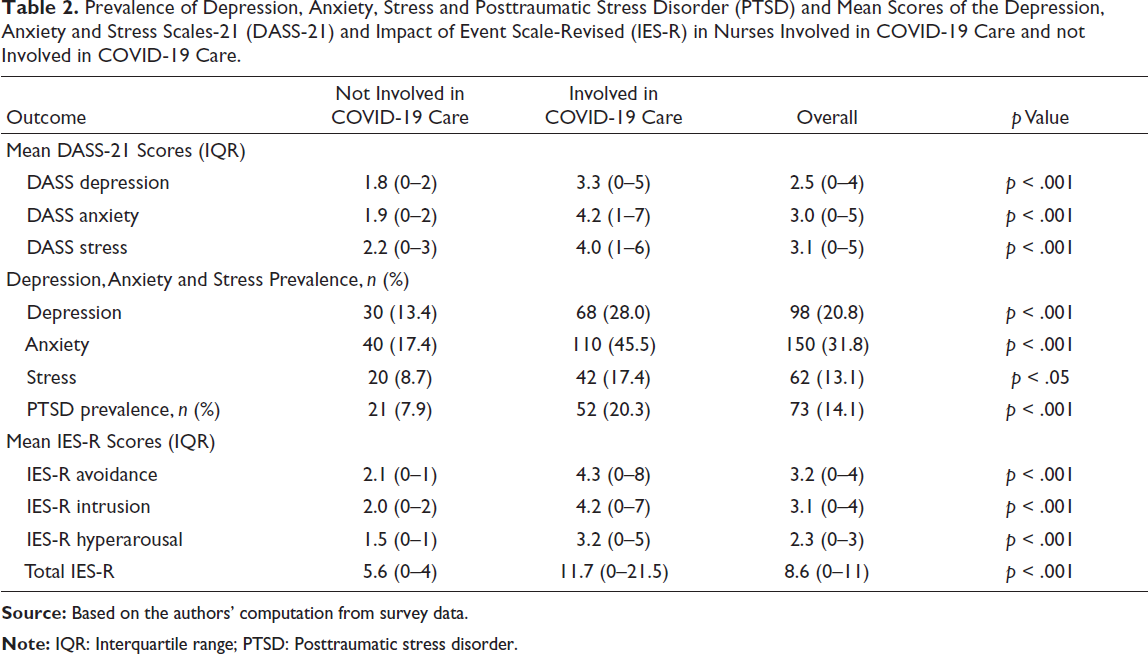
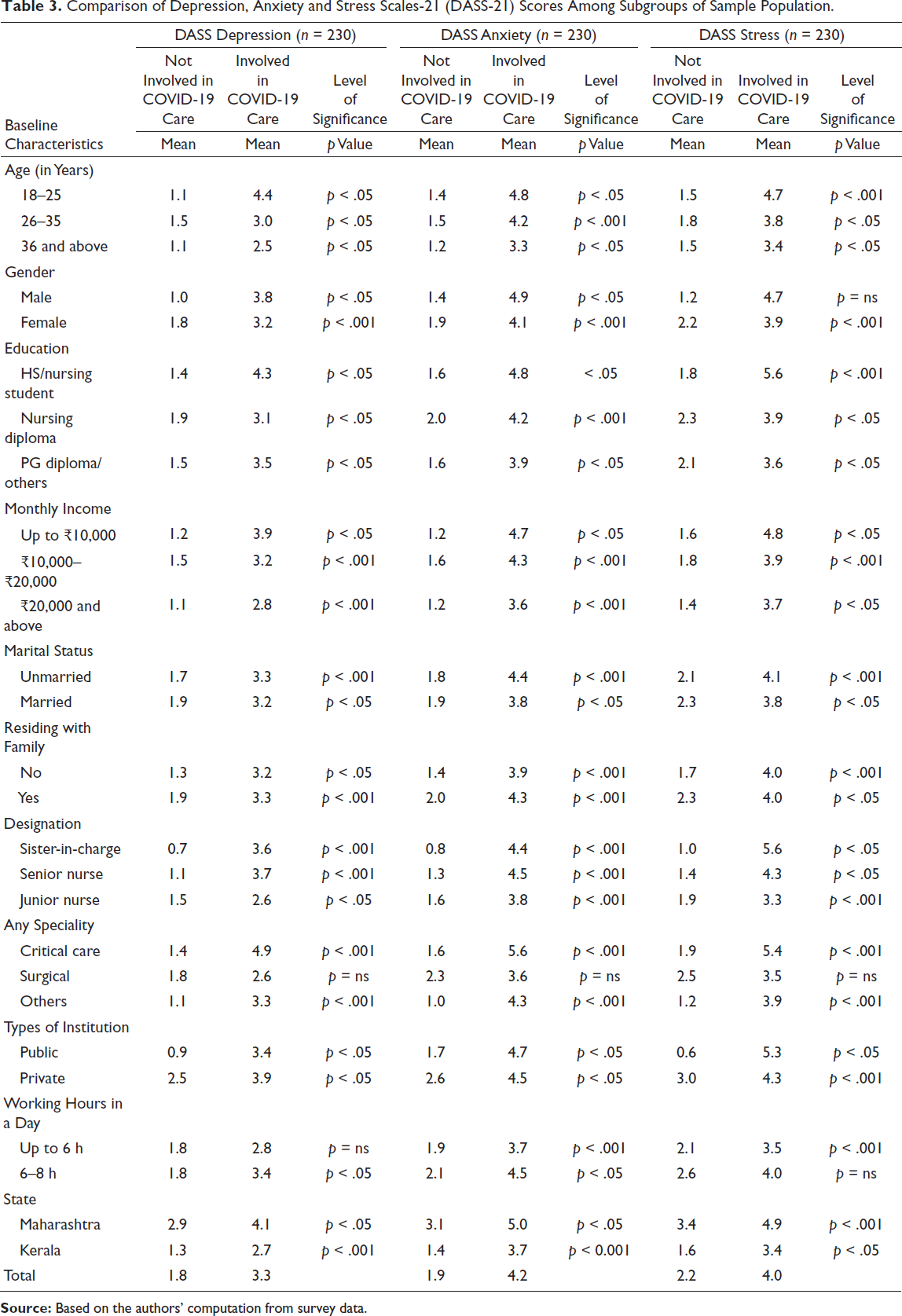
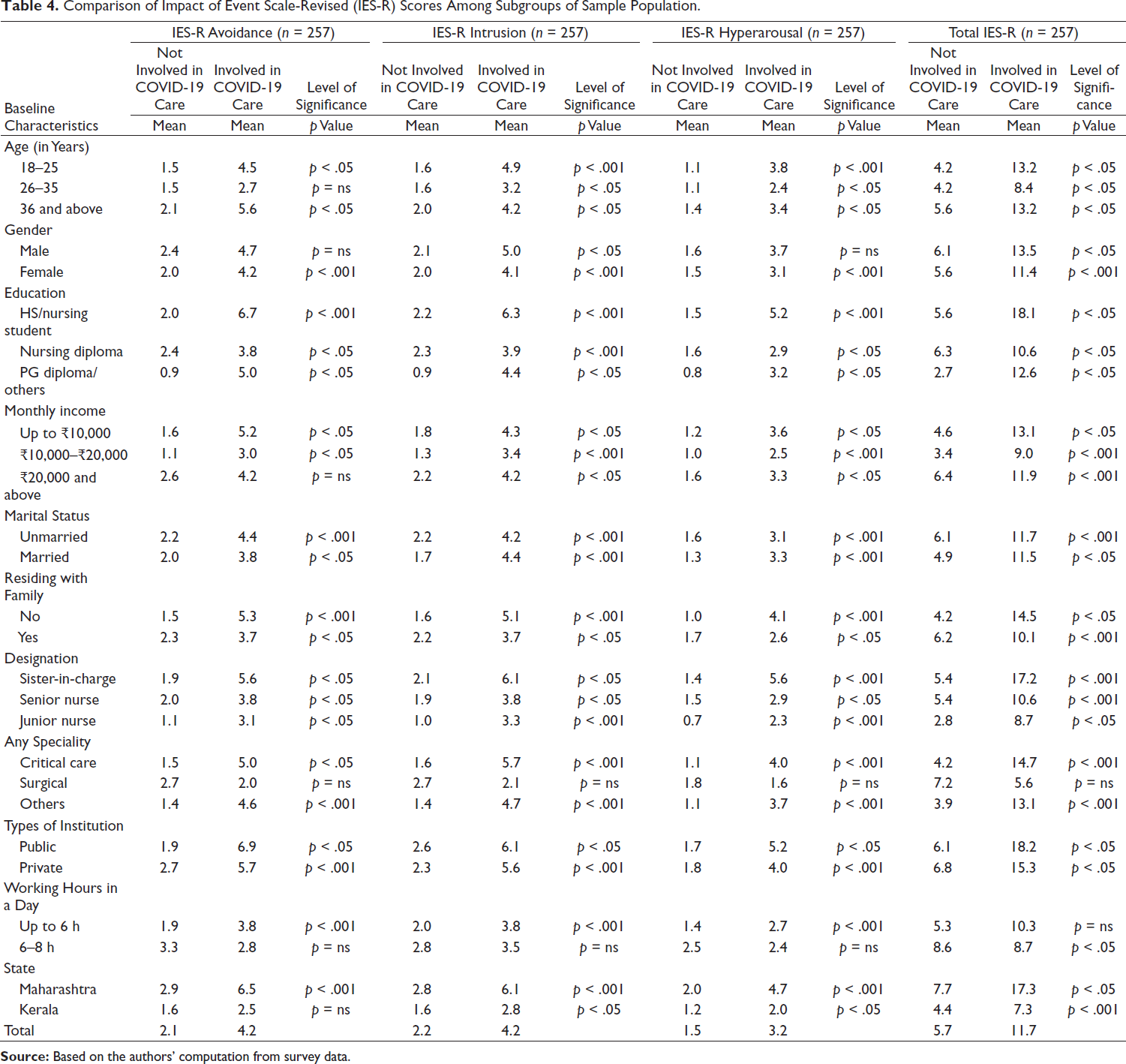
Among those who were not involved in COVID-19 care, 13.4% of participants screened positive for depression, 17.4% for anxiety, 8.7% for stress and 7.9% for clinical concerns of PTSD. In contrast, among the nurses involved in COVID-19 care, 28% screened positive for depression, 45.5% for anxiety, 17.4% for stress and 20.3% for PTSD (Table 2). DASS-21 mean scores for depression, anxiety and stress, and the IES-R avoidance, intrusion, hyperarousal and total subscale scores among nurses involved in COVID-19 care were significantly higher than those of nurses not involved in COVID-19 care. Mean scores for DASS-21 and IES-R using background details (age, sex, marital status, education, residing with, monthly income and medical condition), and occupation details (designation, specialty, institution, working hours/day and nature of duties) were found to be higher among nurses involved in COVID-19 care compared to those not involved in COVID-19 care (Tables 3 and 4). Compared to Kerala, nurses working in Maharashtra had higher mean scores for those who were involved in COVID-19 care. Those working in public hospitals reported significant PTSD (unadjusted OR, 95% CI: 2.5, 1.2–5.0, p value = .008) compared to those employed in private hospitals.
Baseline Characteristics of Nurses.
Prevalence of Depression, Anxiety, Stress and Posttraumatic Stress Disorder (PTSD) and Mean Scores of the Depression, Anxiety and Stress Scales-21 (DASS-21) and Impact of Event Scale-Revised (IES-R) in Nurses Involved in COVID-19 Care and not Involved in COVID-19 Care.
Comparison of Depression, Anxiety and Stress Scales-21 (DASS-21) Scores Among Subgroups of Sample Population.
Comparison of Impact of Event Scale-Revised (IES-R) Scores Among Subgroups of Sample Population.
Qualitative Results
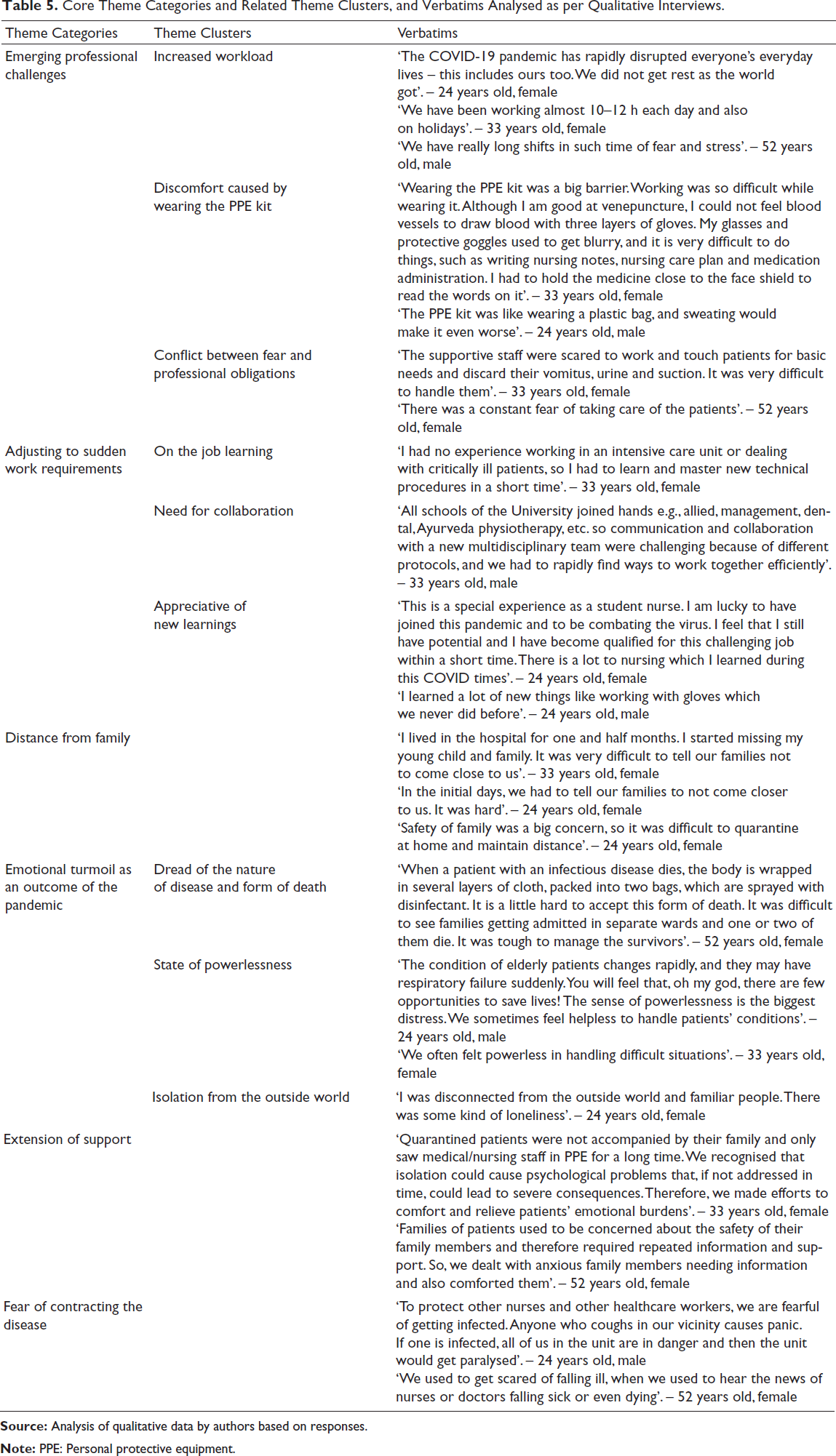
Table 5 provides the core theme categories and related theme clusters, and verbatims analysed as per the qualitative interviews conducted with the nurses. The participants shared challenges related to increased workload, longer distance from family and a constant fear of getting infected and transmitting the disease to others, along with how they dealt with these adversities.
Core Theme Categories and Related Theme Clusters, and Verbatims Analysed as per Qualitative Interviews.
Discussion
The spread of COVID-19 in India overwhelmed public health responses, raising concerns about infection control in hospitals. Nurses faced heavier workloads, increased infection risks and fear of transmitting the virus to families. In October 2020, the International Council of Nurses noted many nurses caring for COVID-19 patients suffer burnout, psychological distress and face abuse or discrimination (WebDesk, 2021). Our study, using validated psychometric tools, involved 520 nurses (50.57% not involved in COVID-19 care, 49.42% involved) in Maharashtra and Kerala, showed a higher percentage of nurses in COVID-19 care screening positive for depression, anxiety, stress and PTSD than those not involved. Mean scores for DASS-21 and IES-R with background details (age, sex, marital status) were higher among nurses involved in COVID-19 care.
A systematic review and meta-analysis of stress, depression and anxiety prevalence among frontline nurses reported 46%, 33% and 39%, and 43%, 37% and 35% among second-line nurses, respectively (Al Maqbali, 2021). Our study showed lower stress (17.4%) and depression (28%) but higher anxiety (45.5%) among COVID-19 care nurses. Previous systematic reviews found depression and anxiety prevalence of 25.8%–28% and 22.8%–30.30% among nurses (Pappa et al., 2020; Salari et al., 2020). The prevalence of depression was similar, but anxiety was higher at 45.5% in our study. Our PTSD findings matched those of Al Maqbali et al. (2021). Logistic regression indicated that COVID-19 duty significantly affected PTSD and anxiety.
Our study showed a significant difference between the DASS-21 and IES-R scores among nurses engaged in COVID-19 care in Maharashtra and Kerala. Working in Maharashtra also reported significant values related to stress, anxiety, depression and PTSD in our regression analysis. In Maharashtra state, only about 21% of nurses from the private sector and 7.5% from the public sector received their COVID allowances, could not get sanctioned leave and did not get adequate safety equipment (Pathare, 2021). In contrast, decades of investment in decentralised public health systems in Kerala have enabled better preparedness to manage the COVID-19 pandemic (Menon et al., 2020), thus reducing the occupational impact on nurses managing COVID-19 patients in the state to a large extent.
Correlational analysis of psychological variables and working conditions, and nurses’ coping methods and distress during past epidemics like SARS, showed that organisational support, trust in equipment/infection control and less contact with SARS patients predicted lower burnout and stress (Marjanovic et al., 2007). Our study found significant differences in depression, anxiety, stress and PTSD among nurses involved in COVID-19 care compared to those who were not. The pandemic has stressed nurses both at work and at home. For instance, PPE supplies are insufficient, nurses face violence or discrimination and have childcare issues (Reuters, 2021).
The qualitative findings point to the presence of various on-the-job challenges, such as an increase in workload due to long work shifts without breaks. Our findings are consistent with previous studies that found that healthcare providers experienced inordinately high levels of workload and feelings of losing control over the situation during the pandemic (Eftekhar Ardebili et al., 2020; Zhang et al., 2020). Furthermore, working in a PPE kit added to their problems and caused breathing difficulties, sweating and an inability to perform duties such as writing notes and nursing plans (Zhang et al., 2020).
During the COVID-19 pandemic, many nurses’ roles changed. They had to learn new skills and work in teams, often feeling powerless and doubting their effectiveness. Fear of contracting and spreading the virus made them apprehensive about handling COVID-19 patients and reluctant to interact with family, causing isolation. These findings align with earlier research identifying the risk of infecting loved ones as a major fear (Levkovich & Shinan-Altman, 2020). Similar concerns were noted in a UK study of healthcare workers about infecting residents and families (Nyashanu et al., 2020). Despite challenges, nurses valued their knowledge and prioritised patient and family comfort. Most studies on the mental health impact of COVID-19 have focused on healthcare workers in general (17–23) or, if focused on nurses, were cross-sectional studies (24–30). We identified one systematic review reporting six studies focusing on burnout during COVID-19 (Galanis et al., 2021) and will be incomparable to ours.
Our findings rely on a self-reported survey, raising concerns about response authenticity and recall bias. We did not collect data on participants’ past psychiatric history, a key risk factor for DASS-21 and IES-R, limiting our analysis. Logistic regression on socioeconomic characteristics was unfeasible due to sample size. During September–October 2020, COVID-19 cases in Maharashtra and Kerala were low (50 cases); recent surges impaired our findings’ generalisability (Hindustan Times, 2021). The purposive state selection may introduce selection bias, limiting national applicability. The qualitative-phenomenological approach offers insights but lacks generalisability. Our sample size of 520 nurses was insufficient to generalise the findings to the broader nurse population.
Conclusion
Our study in Kerala and Maharashtra, India, found higher depression, anxiety, stress and PTSD levels in nurses caring for COVID-19 patients compared to those not involved in such care. Despite guidelines for health workers’ mental health in India, regular screening and support mechanisms for nurses in COVID-19 care are needed to manage their psychological well-being.
Footnotes
Acknowledgements
The authors thank the participant nurses for their time and cooperation in this study. They also thank Dr Alice David for guiding them on some of the statistical analyses.
Authors’ Contributions
DJ and SR conceived the study. DJ and CV designed the study. CV led the ethics approval process. DJ and JY designed the statistical analysis plan. CV, SG, SR and RT led the data collection efforts. JY and SK analysed the data and developed tables, along with inputs from DJ. DJ and JY wrote up the initial draft of the manuscript. All authors contributed to and approved the final version of the paper.
Data Availability Statement
Data will be available upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee of Believers Church Medical College Hospital (IEC/2020/04/138). All procedures involving human participants followed the ethical standards of the 1964 Helsinki Declaration and its later amendments or similar ethical standards.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Participants were requested to provide informed consent as the first part of the online Google Form prior to entering their personal information.
Annexure 1: Survey questionnaire
Socio-demographic details
Background details
Name Age: years Sex: Male/Female/Transgender Marital status: Unmarried/Married/Separated/Divorced/Widow(er) Education Current address: Residing with: Nurses/Family/Friends/Alone Monthly income Medical Condition (if any)
Occupation details
Designation: Nursing Superintendent/Sister-in-charge/Senior Nurse/Junior Nurse Any specialty: Cardiac/Surgical/Neurosurgery/Paediatric/Critical Care Institution: Public/Private Name of institution Location of institution Hours of working/day Nature of duties Involvement in care of person with COVID-19: Yes/No If yes, In quarantine/In isolation/With symptoms needing care/In Intensive Care/In end of life care/In bereavement
Annexure 2: Interview guide
Thank you very much for your help.
Mental health and social stigma among nurses involved in management of COVID-19 in India
(for IRB approval)
The aim of this study is to understand the mental health status, social stigma, and coping behavior of nurses involved in either COVID-19 screening, testing or treatment.
We appreciate your interest in participating in this online survey. You have been invited to participate as you are a nurse who is managing COVID-19 at your facility.
You may ask any questions before deciding to take part by contacting the researcher (details below).
We __________________________________________________ (Name) at the____________________________________________________________________________________
(Name of the Institution/ Organisation and the address).
You will be given some questions and will be asked to answer questions on phone. This should take about ____ minutes. No background knowledge is required.
The survey is being done online because of compulsions of the lock down and because of the need to respect Human distancing while communicating.
The information given by you will be stored either in and/or as an electronic record with the researchers. The information will be available only to the researchers in an anonymized form. It will be submitted to the various government officials in a completely anonymised manner. Your identity and what you say will remain anonymous and protected.
Please note that your participation is voluntary. If you do decide to take part, you may withdraw at any point during the questionnaire for any reason.
Your answers will be completely anonymous, and we will take all reasonable measures to ensure that they remain confidential. The data collected may be used in academic publications. All questions are optional and you have the option not to answer a particular question. Research data will be stored for a minimum of three years after publication or public release.
The _______________________________________________________________________ and other institutions involved in the study, and as such will determine how the answers to your questions are used in the study.
We would also like your permission to use your anonymised data in future studies, and to share data with other researchers.
This survey/questionnaire/project may be used for another project.
This project has been reviewed by, and received ethics clearance through, the Institutional Ethics committee of Believers Memorial Church Hospital committee meeting held on 8th April 2020
If you have a concern about any aspect of this study, please speak to Dr Swati Rane, at E mail: and we will do our best to answer your query.
□ I certify that I am 18 years of age or over
These clarifications have been explained to me by ___________________________________________
Research assistant/ Counsellor______________________________
The oral consent templates below can be adapted to suit your study, but careful consideration is required to ensure that these are appropriate for the research and the participants.