
Abstract
No-show appointments result in wasted resources for health institutions and patients who need services. This study aimed to determine the reasons for no-show appointments and patients’ opinions on potential interventions to prevent them. This study was conducted at a university hospital in Türkiye and included 795 patients. The sample size was first distributed according to the weights of internal and surgical outpatient clinics, and patients from these clinics were selected using convenience sampling. A questionnaire was used to determine why patients did not attend hospital appointments in the previous month and their opinions about potential measures to minimise non-attendance. Possible reasons for no-show appointments, such as ‘forgetting’, ‘being somewhere else’ and ‘taking care of family’, came to the fore. Among the possible preventive measures, 24-h reminders, timely maintenance and repair of medical devices, notifying the patient of appointment cancellations/changes, advance planning of doctors’ meetings, easy access to the appointment cancellation system and informing patients about appointment cancellation methods were considered effective. However, measures such as temporarily denying appointments to patients who do not attend them and fees for missed appointments were observed to be less effective. In all, 41% of the patients requested reminders of their appointments via SMS and mobile phone. Determining patients’ opinions about the reasons for no-show appointments and potential preventive measures will contribute to a better understanding of the problem and the design of effective interventions.
Background
No-show appointments, defined as not using or not attending a planned appointment, constitute a significant obstacle to cost-effective healthcare (Kheirkhah et al., 2016). Missed appointments, on the one hand, lead to inefficient use of staff and lengthening of waiting lists and times (Karter et al., 2004; Murray, 2000). On the other hand, they interrupt the monitoring and control of patients’ health conditions (Karter et al., 2004). According to Moore et al. (2001), patients who fail to cancel or miss appointments endanger their health and well-being and impede the therapeutic efforts of service providers.
Appointment compliance is highly essential for chronic disease management, especially for the treatment of diseases such as diabetes and hypertension, as they trigger other health problems. Missed appointments reduce doctors’ opportunities to diagnose diseases in a timely manner and can pose serious health risks to patients (Gier, 2017). Although diagnostic tests and screenings can help diagnose patient complaints and symptoms early, diagnostic processes will be delayed when patients miss critical appointments (Kheirkhah et al., 2016).
In addition to the negative effects of missed appointments on healthcare delivery, they also negatively affect healthcare costs. Missed appointments can result in various social and financial costs for healthcare providers. Further, the social cost of missed appointments is the losses incurred due to unused or misused resources (such as personnel, equipment and facility capacity), resulting in lower productivity and wasted time (Alhamad, 2013; Bhatia et al., 2018). The financial cost of missed appointments is the loss of income to healthcare providers. If reimbursement is made on a per-service or per-case basis, third-party payers will not provide any reimbursement to service providers for missed appointments; therefore, they will experience a loss of income. When a person does not show up for an appointment, and there are no other income-generating activities (such as treating another patient), healthcare providers lose income. However, in many cases, a missed appointment may not necessarily result in financial loss (or social costs), as patients seeking care who do not have appointments can take the place of patients who do not show up within the scheduled time (Bech, 2005).
Furthermore, the cost of no-show appointments for specialist services is higher than that for primary care appointments (Aggarwal et al., 2016; Bech, 2005). Primary healthcare institutions can deal with missed appointments more easily because they normally receive a large number of walk-in patients during the day (Yan et al., 2014). In other words, while no-show appointments with healthcare providers such as general practitioners, dentists and physiotherapists may cause relatively negligible costs due to the constant patient flow and short appointment times, no-shows for treatments that require expertise may result in much higher costs. However, if no-show rates for primary healthcare services are high, service providers may incur significant costs (Bech, 2005). In a study conducted over 3 months in a psychiatric clinic in the USA, it was calculated that each missed appointment would cost the clinic $463, resulting in a loss of $17,131 in annual income (Clouse et al., 2017). In another study conducted at an academic medical centre in the USA, it was estimated that the missed revenue for radiology, imaging and diagnostic imaging appointments reached $1 million per year. It was stated that this missed revenue could cover the purchase of a new 3T magnetic resonance imaging (MRI) scanner every year (Mieloszyk et al., 2018). In a study conducted in a vascular laboratory in America, it was estimated that a 12% no-show rate caused an annual loss of $89,107 in laboratory revenue, and that by reducing the missed appointment rate to 5%, the revenue would increase by another $51,769 (Satiani et al., 2009).
On the other hand, failure to attend an appointment can often result in unnecessary use of more costly services, such as emergency health services (Kim & Giachetti, 2006; Samuels et al., 2015). A review of the literature found that patients who missed appointments were more likely to visit the emergency department and that missed appointments were a better predictor of future emergency department use than other variables such as chronic health conditions, psychiatric conditions and cognitive factors (Nguyen & Dejesus, 2010; Renee Miller-Matero et al., 2018).
It is stated that various interventions have been developed to prevent missed appointments in practice, but although these interventions do not completely eliminate the problem of missed appointments, they cause significant decreases (Vijayan, 2014). One of the strategies that can be employed to prevent no-show appointments is overbooking, which is used in traditional appointment planning. In this method, multiple patient appointments are scheduled for the same appointment interval with the expectation that there will be patients who do not attend their appointments; thus, it is thought that the loss of income and idleness of the health service provider that may arise from non-use of outpatient clinics can be prevented (Gebhart, 2017). Another strategy is a method called advanced access. In this method, each physician has appropriate appointment intervals, and priority is given to same-day appointments (Murray & Berwick, 2003; Murray & Tantau, 2000).
One of the most common reasons for missed appointments is forgetfulness (Hon et al., 2005; Mohamed & Al-Doghaither, 2002; Murdock et al., 2002; Neal et al., 2005; Skaret et al., 2000; Zailinawati et al., 2006). Any appointment reminder method (such as SMS, mobile phone or e-mail) can help reduce the no-show rate and the inefficiency and cost that may result from missed appointments. Reminding patients of their appointments using the methods they prefer will not only make it easier to reach them but also create an opportunity for patients who want to cancel their appointments (Gurol-Urganci et al., 2013).
However, in Türkiye, there is no data or information on the reasons why patients do not attend their appointments and the extent to which they consider potential preventive measures effective. Patients increasingly find it difficult to make appointments, especially in recent years, due to the increasing number of immigrant/refugee populations coming from Syria, Iran, Afghanistan and Pakistan and the number of Turkish physicians migrating abroad due to dissatisfaction with working conditions and other reasons. Therefore, it has become significantly more important to investigate the reasons for not attending appointments and the effects of interventions aimed at resolving this problem.
This study aimed to determine the reasons why patients do not attend outpatient clinic appointments at a university hospital and the extent to which they consider possible preventive measures effective. An in-depth understanding of these issues will contribute to the design of more effective political and managerial interventions.
Methods
Study Design
This study was conducted at the outpatient clinics of Hitit University Erol Olçok Training and Research Hospital, located in Çorum, a medium-sized city in Türkiye. To determine the sample size, the number of patients (N: 1,089,675) who made appointments from internal outpatient clinics (561,786 patients) and surgical outpatient clinics (527,889 patients) during the last 1 year (October 2018–September 2019) was considered. The sample size was calculated as 662 for a 99% confidence level and 0.05 error tolerance. However, because 20% non-response is usually encountered in such field studies, 20% non-response was added to the calculated sample size, and the final sample size was found to be 795. A two-stage sampling selection method was used to select the patients. First, the calculated sample size was distributed according to the weights of the internal and surgical outpatient clinics, and patients from these clinics were selected using convenience sampling.
Data Collection
A questionnaire was administered to determine the reasons why patients did not attend the appointments they had made during the previous month and the extent to which they considered preventive measures effective. The first part of the questionnaire included questions about the patients’ sociodemographic characteristics (gender, age, education level, working status, marital status and chronic disease).
The second part of the questionnaire included 23 possible reasons for not attending appointments. While developing the underlying reasons for patients’ behaviour of not attending appointments, literature on the subject was largely used, and some items were added by the researchers. Patients were asked to mark the reason(s) for not attending each appointment they had not attended in the last month.
The third part of the questionnaire included measures that could be taken to minimise no-show appointments. Patients were asked to rate 15 items in this section based on a five-point Likert scale (1 = not very effective, 2 = not effective, 3 = partially effective, 4 = effective and 5 = very effective). Among the 15 items, measures 1, 2, 7, 8 and 12 were adopted from Hussain-Gambles et al. (2004), whereas measures 3, 4, 5, 6, 9, 10, 11, 13, 14 and 15 were developed by the researchers.
The questionnaire was administered to patients through face-to-face interviews between 10 February 2020 and 10 March 2020, shortly before the COVID-19 pandemic appeared in Türkiye. It took approximately 10–15 min for each patient to complete the questionnaire.
Data Analysis
The entry and analysis of the research data were performed using SPSS (version 23.0). Descriptive statistics, such as frequency and percentage, were used for discrete variables, and means and standard deviations were used for continuous variables.
The questionnaire used in this study was evaluated in terms of content validity. For this purpose, a group of seven experts in the field of health management, consisting of five academicians, one hospital manager and one polyclinic services officer, was asked to evaluate the items in the questionnaire within the framework of the options ‘Appropriate’, ‘Appropriate, but should be corrected’ and ‘Not appropriate’. In the second part of the questionnaire, the following recommendations were made regarding the reasons for no-show appointments: The item ‘I didn’t go because of the negative attitudes and behaviours of the healthcare staff towards patients’ should be replaced with ‘I didn’t go because of the negative attitudes and behaviours I encountered before’. The item ‘I couldn’t go to my appointment because I went to another hospital’ should be replaced with ‘I had an appointment at two different hospitals/units at the same time’. The item ‘I was told not to come to my appointment because my doctor had another job’ should be replaced with ‘My appointment was cancelled/postponed by the hospital because my doctor had another job’. In addition, the majority of experts recommended that the item ‘I didn’t think the appointment was necessary’ should be removed from the form, and it was suggested that the item ‘I gave up going because the complexity of the bureaucratic procedures at the hospital intimidated me’ should be added to the form.
The opinions of patients about the measures for no-show appointments in the third part of the questionnaire were evaluated by experts as follows: It was suggested that the ‘letter’ in the statement ‘Patients who don’t attend their appointments should be sent a warning letter warning that work will be disrupted if they don’t cancel their appointments’ be changed to ‘message’ since it is not widely used in today’s context. The item ‘Healthcare personnel should be attentive to patients, be courteous and friendly’ should be replaced with ‘In order to ensure that patients come to their appointments, healthcare personnel should be more attentive to patients’, and the item ‘In case doctors attend meetings such as congresses or workshops, patients who have made an appointment with that doctor should be informed about the cancellation of the appointment’ should be replaced with ‘In order not to cause appointment cancellations due to doctors’ participation in meetings such as congresses and workshops, such meetings should be planned beforehand’. In addition, experts suggested that the item ‘The number of previously missed appointments should be displayed in hospital waiting rooms so that patients are aware of appointment cancellations’ should be removed from the questionnaire. Accordingly, the questionnaire items were rearranged in line with expert opinions, resulting in their final form.
After the necessary revisions were made to the questionnaire form in line with the recommendations of the experts, it was pilot-tested with 15 patients on 20 May 2019, in a hospital other than the one where the main research was conducted, in order to test the clarity of the expressions and whether the questions worked.
In this study, the reliability of the answers provided by the participants regarding the measures for no-show appointments was evaluated based on the internal consistency coefficient and test–retest methods. The internal consistency coefficient was 0.77, and the test–retest result for 25 patients was 0.85.
Results
Table 1 presents the sociodemographic characteristics of the 795 participants who responded to the questionnaire and had at least one no-show appointment in the last month.
Sociodemographic Characteristics of Patients.
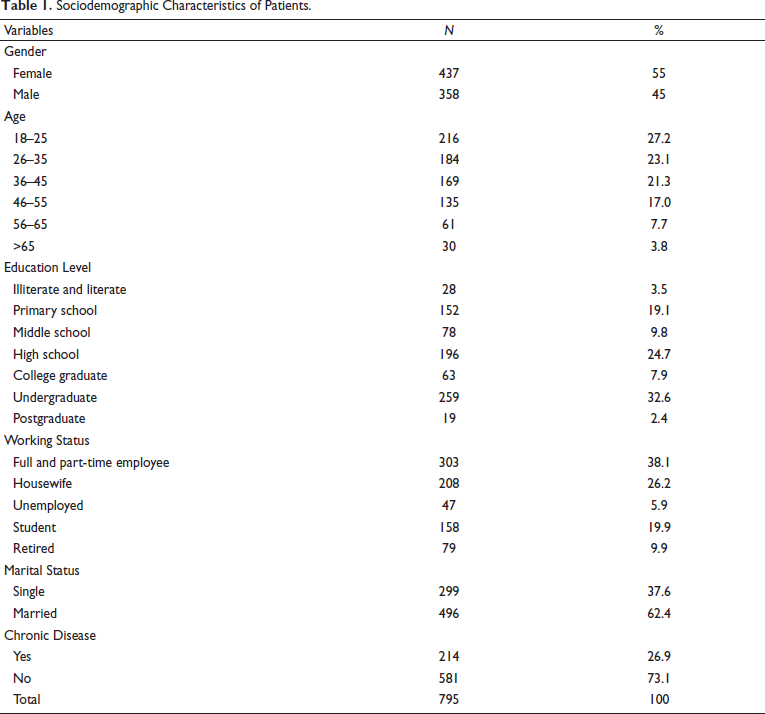
As shown in Table 1, 55% of the participants were women, and 88.5% were between the ages of 18 and 55. Moreover, 62.4% were married, and 42.9% were in the college or higher education group. Regarding their employment status, 38.1% worked full- or part-time, and 26.2% were housewives. Of those who responded to the questionnaire, 73.1% did not have any chronic diseases.
Table 2 presents the descriptive findings regarding the reasons underlying the participants’ behaviour of not attending an appointment in the last month. While 88.7% (n: 705) of the patients stated that they had not attended only one hospital appointment in the last month, 10.8% (n: 86) stated that they had not attended two appointments in the last month, and 0.5% (n: 4) stated that they had not attended three appointments in the last month. Participants stated one or more reasons for each appointment that they did not attend. While 21.5% of the participation in reasons were related to the health system (reasons numbered 3, 4, 7, 8, 19, 20, 21, 22 and 23), 76.6% of the participation were not (reasons numbered 1, 2, 5, 6, 9, 10, 11, 12, 13, 14, 15, 16, 17 and 18).
Descriptive Findings Regarding Reasons for No-show Appointments.
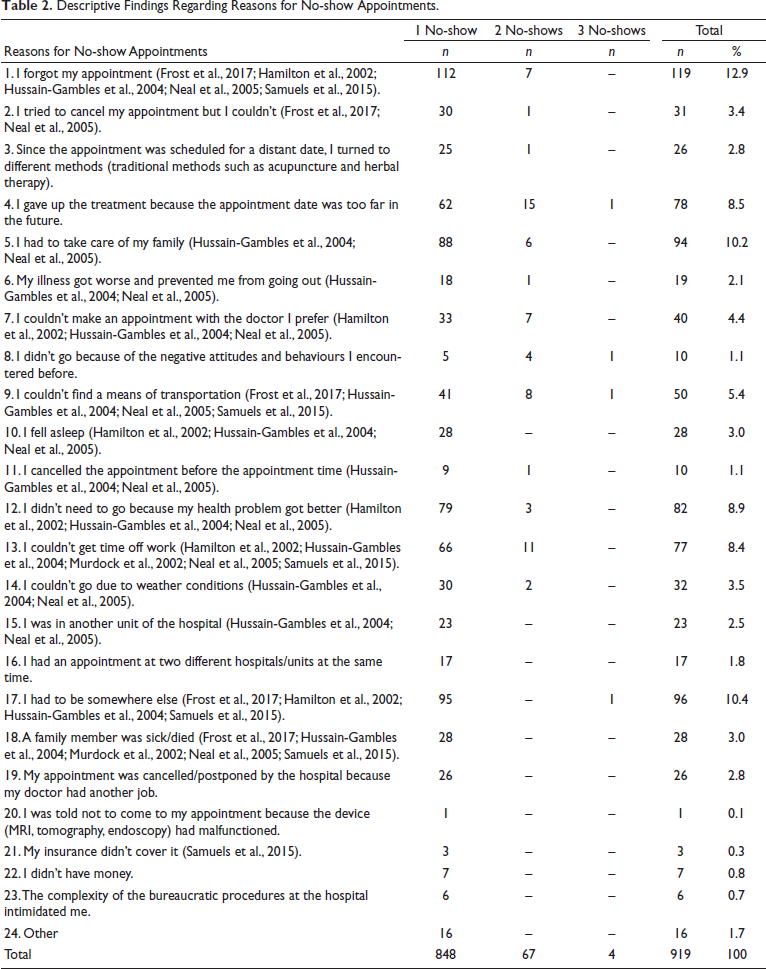
It was observed that the most stated reason for not attending appointments in the last month was ‘I forgot my appointment’, as shown in Table 2, and 12.9% of the missed appointments were explained by this reason. This was followed by ‘I had to be somewhere else’ with 10.4%, ‘I had to take care of my family’ with 10.2%, ‘I didn’t need to go because my health problem improved’ with 8.9%, ‘I gave up the treatment because the appointment was scheduled for a distant date’ with 8.5% and ‘I couldn’t get time off work’ with 8.4%. It has been observed that these six most frequently repeated reasons explain approximately 60% of the missed appointments.
Table 3 presents descriptive findings regarding patients’ opinions on measures that can be taken to minimise missed appointments. As shown in Table 3, of the patients participating in the study, 96.9% said, ‘To prevent patients forgetting their appointments, a reminder should be sent 24 h before the appointment’; 95% said, ‘In order to avoid appointment cancellations due to reasons such as malfunction of medical devices and equipment, maintenance and repairs of such devices should be carried out in a timely manner’; 93.6% said, ‘Appointment cancellations or changes due to the doctor or device malfunction (MR, tomography, endoscopy) should be communicated to the patient’; 93.1% said, ‘In order not to cause appointment cancellations due to doctors’ participation in meetings such as congresses and workshops, such meetings should be planned beforehand’; 92.8% said, ‘Patients should be able to easily access the appointment cancellation system’ and 92.7% said, ‘Patients should be informed about appointment cancellation methods’. They considered these ‘effective’ and ‘very effective’ in preventing no-show appointments. On the other hand, 47.7% and 28.8% of the patients who responded to the questionnaire evaluated the suggestions ‘Additional co-payment must be collected from patients who do not cancel their appointments’ and ‘Patients who do not attend their appointments should not be given an appointment for a certain period of time’ as ‘effective’ and ‘very effective’, respectively.
Descriptive Findings Regarding Measures for No-show Appointments.
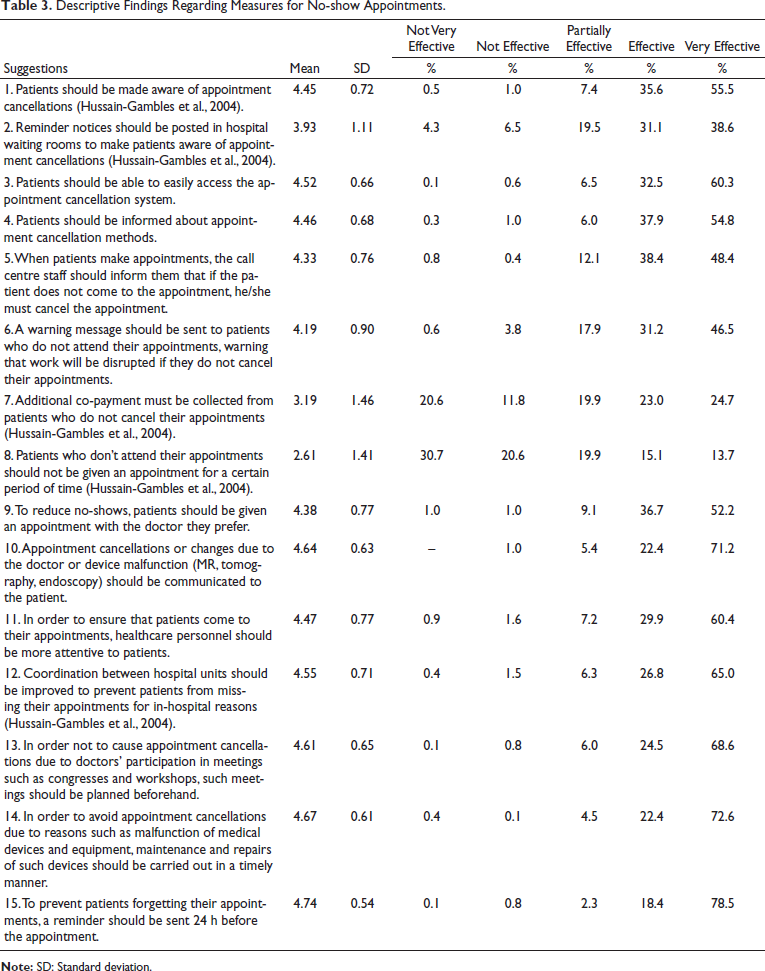
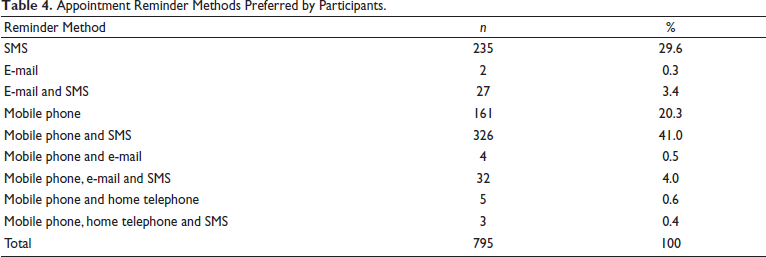
Table 4 shows the appointment reminder methods preferred by the participants. As shown in Table 4, 41% of the participants preferred to be reminded of their appointments via both SMS and mobile phone, whereas 29.6% chose SMS alone. Moreover, 20.3% preferred the reminder option via mobile phones only.
Appointment Reminder Methods Preferred by Participants.
Discussion
When patients do not attend their scheduled outpatient clinic appointments, many negative consequences arise, such as encountering more costly treatment (Foushee, 2020), interruptions in appointment schedules, idle resources (inefficient use), delays in other patients in need of healthcare receiving the service on time and decreased income for hospitals (Kheirkhah et al., 2016; Marbouh et al., 2020). To deal with these undesirable consequences, it is important to examine the reasons for no-show appointments and measures for reducing no-show rates.
In this study, when the reasons why patients did not attend outpatient clinic appointments were examined, the reason ‘I forgot my appointment’ came to the fore. This was followed by reasons such as the need to be somewhere else, family responsibilities, believing that the health problem had improved, inability to get time off work, rescheduling appointments to a distant date and inability to find a means of transportation. Based on these findings, it is noteworthy that patients do not attend their appointments because of reasons unrelated to the healthcare system; their reasons rather stem from individual conditions. In a study conducted by Hamilton et al. (2002) regarding services received from general practitioners, ‘forgetting an appointment’ was found to be the most common reason for not attending an appointment. This was followed by application errors, mixing up the days, not being able to get time off work and having to be somewhere else (Hamilton et al., 2002). Similarly, Samuels et al. (2015) in a study conducted in a primary care paediatric clinic, found the following common reasons for not attending an appointment: Forgetting, transportation problems and inability to get time off work. Another study conducted in a primary healthcare centre stated that the two most common reasons for not attending appointments were forgetting and communication problems (Kaplan-Lewis & Percac-Lima, 2013).
In both this and similar studies, patients stated that ‘forgetting’ was the most common reason for not attending an appointment. In this study, most patients preferred appointment reminders via SMS and mobile phone. In a study conducted by Gurol-Urganci et al. (2013) to examine the effects of text messages and phone reminders on improving attendance in primary healthcare services, it was found that the no-show rate was lower in the patient group that received reminders via text messages and phone calls than in the patient group that did not. While the attendance rate for clinical appointments was 67.8% in the group that did not receive any reminder, the attendance rate was 80% in the group that did. In a study conducted to compare the effectiveness of SMS and telephone reminders in improving appointment attendance rates at a health promotion centre in China, 1,848 participants who were eligible for analysis were divided into three groups: SMS reminder, telephone reminder and control group (no reminder). The results showed that appointment attendance rates were significantly higher in the groups reminded via SMS (OR = 1.698; p = .001) and telephone (OR = 1.829; p < .001) than in the control group (Chen et al., 2008).
In our study, it was observed that among the measures for no-show appointments, sanctions (not giving an appointment for a certain period and a fee for a missed appointment) were considered less effective than other measures. However, patients are more supportive of measures to be taken in terms of the health system, such as training and information for patients and improvements in appointment planning, in reducing the no-show rate. It is known that payment of fees is used as a managerial intervention tool to reduce missed appointments in order to optimise health resources and ensure the appropriate use of health funds (Bech, 2005). In a study conducted by Mäntyjärvi (1994) in which patients who did not attend their appointments were charged a fee, the situation before and after the intervention was compared, and it was reported that the no-show rate decreased from 6.4% to 5.5% after charging fees. Lesaca (1995), on the other hand, found that the no-show rate decreased from 20.1% before the intervention to 9.2% after the intervention. Although hospitals, clinics and other medical care centres prefer charging fees for missed appointments as a solution to reduce the no-show rate, it should be noted that this approach is a less desirable solution for patients because it may limit access to care, especially for patients with limited income (Daggy et al., 2010).
The literature indicates that information and patient training alone are not effective in reducing no-show rates; however, it is recommended that various appointment-scheduling strategies be considered in conjunction with text messages and phone reminders. In a study conducted by DuMontier et al. (2013) in a clinic providing services in an urban area, the effects of interventions such as patient training and organising appointment schedules on reducing the no-show rate were examined, and it was reported that the no-show rate in the cohort group decreased from 33.3% to 17.7%, and the general no-show rate decreased from 10% to 7%. In another study on family medicine services, in a patient group who made an appointment for the first time and were informed about the negative aspects of no-show appointments after the examination, there was a 29% decrease in the probability of missing the next appointment. It was stated that this corresponded to a 5.2% decrease in the absolute no-show rate (Guse et al., 2003). Additionally, the literature indicates that improvements in attendance rates can be achieved through training designed based on different methods. DuMontier et al. (2013) carried out a three-stage mixed study at a family medicine centre affiliated with the University of Wisconsin: The first stage was the implementation of an educational program in which the effects of missed appointments were discussed for the patient group who did not attend their appointments, the second was double booking in the schedules of healthcare providers and the third was the implementation of an advanced access system in which the traditional appointment planning method was changed. The results revealed that the largest improvement in attendance rates was achieved after the implementation of the advanced access system, and the no-show rate of the patient group decreased from 33.3% to 17.7% (DuMontier et al., 2013). Guse et al. (2003) investigated the effect of patient training in the form of interviews at the end of the examination in a family medicine centre on the no-show rate and found a significant decrease in the no-show rate in the group that received training (OR = 0.71; p = .04).
Conclusions
Since outpatient clinic appointments missed by patients for various reasons negatively affect the efficiency and financial situation of health institutions, the reasons for no-show appointments must be identified and measures taken.
In this study, the most common reason for no-show appointments was ‘forgetting an appointment’. Appointment reminders can be provided at regular intervals to minimise the number of patients who forget their appointments. Reminders can be made by considering patient preference methods for receiving them (SMS and mobile phone preference rates were 41%).
Since patients consider systematic arrangements to be a much more effective intervention to address the problem of no-show appointments, health institutions should provide information about appointment-making and appointment cancellation methods and ensure that patients understand the possible negative consequences of no-show appointments. For patients with children who are unlikely to attend appointments because they need to take care of their families, play and activity areas can be created within the hospital where they can leave their children.
Since this study was conducted cross-sectionally only at a university hospital, it is essential to conduct large-scale studies that reflect Türkiye in general, including public and private hospitals, to obtain study findings with high external validity.
Footnotes
Acknowledgments
This study was produced from researcher Nursel Tuncer’s master’s thesis.
Data Availability Statement
Research data are not shared.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics Statement
The study was approved by Hacettepe University Non-Interventional Clinical Research Ethics Committee on 22 October 2019 (Ref No: GO 18/954).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.