
Abstract
Daily dietary habits of mothers have a major impact on both their own and their children’s overall growth and development during lactation, as well as lowering the likelihood of unfavorable birth outcomes when the focus shifts to the first 1,000 days of life. This community-based cross-sectional study aimed to assess the prevalence of minimum dietary diversity (MDD) in lactating mothers aged 17–39 years from the Mishing tribe in two districts of Upper Assam. MDD for women was determined by using indicator and scoring guide provided by the Food and Agriculture Organization of the United Nations and FHI 360 (2016, Minimum Dietary Diversity for Women: A Guide to Measurement). MDD is an indicator of micronutrient sufficiency in daily diets and is particularly significant due to high rates of maternal undernutrition and anemia in Assam. The study included 361 lactating mothers and used a predesigned semi-structured interview schedule to collect data on socio-demographic and maternal variables, knowledge and practices on nutrition, and maternal health care service utilization. Data were summarized with descriptive statistics and multivariable logistic regression to predict the association between dependent and independent variables. Results showed that MDD was substantially associated with current age, education and occupation, socio-economic status (SES), antenatal care (ANC) visits, anemic conditions, current nutritional status, and nutritional knowledge. The mean MDD score was 5.35, and slightly over half of lactating mothers who had adequate recommended minimum dietary intake were deficient in non-staple food groups like vitamin A-rich fruits, dairy, eggs, nuts, and seeds. Most underweight and anemic mothers had inadequate dietary diversity, unaware of tri-color foods, because the tiranga bhojan approach is yet to gain popularity in Assam. The study pointed that mothers may benefit from varied dietary counseling when visiting a primary health center (PHC) for ANC utilization as those who completed four recommended ANC visits were 6 times more likely to had adequate MDD than those who never utilized ANC facilities in their last pregnancy (AOR: 6.03, 95% CI [2.97–12.08]) ensuring nutrition-specific intervention among the lactating mothers.
Keywords
Introduction
Daily dietary habits of mothers have a major impact on both their own and their children’s overall growth and development. Adequate maternal nutrition is critical to improving a child’s nutritional health and lowering the likelihood of unfavorable perinatal and health outcomes when the focus shifts to the first 1,000 days of life after birth (Kavle & Landry, 2018). Inadequate nutrition brought on by a poor diet causes stunting and other growth problems. It also has a negative impact on children’s cognitive and educational development, which can have long-term social and economic repercussions. Research has shown that a varied and nutrient-rich diet, particularly during pregnancy and lactation, is essential for a child’s healthy physical and mental development throughout life (Schwarzenberg et al., 2018). In India, the various states have varying rates of anemia among postpartum women, ranging from 26.5% to 96.4% (Selvaraj et al. 2019). NFHS-5 (International Institute for Population Sciences (IIPS) and ICF, 2021) revealed that Assam is the worst performer in improving education for women, reducing infant mortality rate, under-five mortality rate, malnutrition in children under 5 years of age and mothers, and an increase in the number of pregnant women who were anemic (54.20%) in NFHS-5 than NFHS-4 (44.80%) (International Institute for Population Sciences (IIPS), & ICF, 2017). It has been established that consuming a variety of foods directly contributes to better nutritional results for both women and children. The dietary diversity score (DDS) is one of the most often used metrics to evaluate the diversity of diets over a specific period that will ensure an adequate intake of nutrients. Additionally, the Indian Council of Medical Research (ICMR) advised lactating mothers to consume an additional 600 calories each day (Indian Council of Medical Research [ICMR], 2010). If these demands go unmet, lactating mothers may experience malnutrition, specifically deficiencies in certain micronutrients. Additionally, a poor diet may affect the breast milk’s nutrient quality (Innis, 2014) and therefore, the physical and cognitive development of the child, not only in the critical window period of 100 days, but also the adverse consequences are carried to the adult phase and to the subsequent generations. Studies carried out in several Asian countries indicate that the minimum dietary diversity (MDD) could vary between 55.2% and 87.8% (Henjum et al., 2015). Dietary diversity serves as a “proxy indicator” for the micronutrient sufficiency of an individual’s diet. It reflects the availability, utilization, and accessibility of food, which are regarded as the three pillars of food security (Parappurathu et al., 2015). Though in India, some studies on MDD of pregnant women and women of reproductive age have been conducted, there is a dearth of information for the same targeting lactating mothers. This study investigated the factors affecting MDD of lactating women belonging to the Mishing tribal community in Assam, and to the best of our knowledge, this study is one of the foundational to identify the causes of MDD among the tribal lactating mothers in Assam. Due to remote topography, North-East India adheres to distinct socio-cultural customs from the national average (Singh et al., 2015) and therefore, possesses unique prospects and issues of diverse ethnic communities. This study would add knowledge to the gap/scant quantitative evidence in North-East India in assessing diet diversity among lactating mothers. This is especially significant given the high rates of maternal undernutrition and anemia in Assam. This study aimed to assess the prevalence of MDD and associated factors among the Mishing tribal (the second largest scheduled tribe, plains) lactating mothers in two districts of Upper Assam.
Materials and Methods
Study Population
This is a community-based cross-sectional study on the lactating mothers belonging to the Mishing tribe aged 17–39 years having a child of 0–23 months at the time of the survey. The Mishing tribe in Assam mainly inhabits the riverine areas of the Brahmaputra River and along its tributaries in Upper Assam. The total Mishing population in Assam was 683,170 (Census of India, 2011), and the district-wise population shows that their highest concentration is found in Dhemaji district (278,592), followed by the Lakhimpur district (177,324) (Census of India, 2011). Therefore, these two districts were selected for the present study. A multistage sampling procedure was adopted to finally select 361 eligible Mishing women, starting with the selection of the districts, followed by the selection of the blocks with a higher concentration of this tribe. Women from three blocks of Dhemaji district, namely, Bordoloni, Dhemaji, and Sissiborgaon blocks, and three blocks from Lakhimpur district, namely, Naoboicha, Bihpuria, and Lakhimpur, were selected. In the third stage, households with lactating women having at least one living child of age 0–23 months were identified.
Sample Size
The sample size was determined by the Cochran method, N = Z2P (1 − P)/E2, where Z = 1.96 (95% confidence interval [CI]), P = estimated proportion of Mishing women (267,520), and E (level of precision) = 0.05. The estimated total sample size was 384 women, with a non-response rate of 6%, finally 361 lactating mothers were found eligible for the present study.
Data Collection
A household-level demographic survey was conducted in the areas to identify lactating women and children aged 0–23 months. Another predesigned and pretested semi-structured interview schedule was used to collect data on socio-demographic and maternal variables, and on the knowledge and practices on nutrition and maternal health care service utilization. In the present study, MDD for lactating women was accepted from the guide of FAO and FHI 360 (2016), which stated, “as the consumption of at least five of the ten food groups specified in the list through the previous day and night (24 h period) preceding the day of the survey.” The minimum dietary diversity for women (MDD-W) was determined by using indicator and scoring guide provided by FAO and FHI 360 (2016) on a 10-food group women dietary diversity score (WDDS) which is based on a 24-h (and 7 days) dietary recall method using a list of foods that are commonly consumed and locally available in the community, based on information gathered during a pilot study. The WDDS is a standard indicator for assessing diet diversity and food access (Leroy et al., 2015). It is calculated by counting the number of food groups consumed by an individual or family over a specific duration. The mothers were asked to recall all foods consumed on the previous day, and according to the MDD-W guide, either “yes” or “no” responses were noted. A received “yes” response was put as score “1” and a “0” score was given on receiving “no” response. The total score was obtained by adding all the individual scores against each food category, which was further categorized into adequate and inadequate dietary diversity based on the MDD-W guide. A mother with a total DDS of less than 5 was denoted as having “inadequate” dietary diversity, and those with scores of 5–10 were denoted as having “adequate” dietary diversity (FAO & FHI 360, 2016). Data was collected on all days of the week since people may eat differently on different days of the week. All interviews were conducted at the households of the study participants.
The primary health centers (PHCs) lacked details regarding each mother’s hemoglobin (Hb) levels at various stages of pregnancy, and many did not approach for antenatal care (ANC) utilization during pregnancy. As a result, the mothers who approached the PHCs for their first ANC visit and had a record of Hb level in the first trimester (≤13 weeks) were included in the study for the Hb level parameter. Thus, data on Hb level in the first trimester were obtained from 268 mothers. Maternal anemia is defined using the WHO criteria as Hb value <11 g/dL, which is further subclassified as mild (Hb = 10–10.9 g/dL), moderate (Hb = 7–9.9 g/dL), and severe (Hb < 7 g/dL) in pregnant women (World Health Organization [WHO], 2011). To assess undernutrition in lactating mothers at the time of the study, the body mass index (BMI) was used, calculated by dividing weight in kilograms by the square of standing height in meters (BMI = weight in kg/(height in m2). BMI standard cut-offs used were as follows: Underweight (<18.5 kg/m2), normal (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥25.0 kg/m2) (World Health Organization [WHO] Expert Consultation, 2004).
The nutrition knowledge score was measured using knowledge on six variables: Knowledge on tri-color food in daily diet, awareness on anemia, heard of iron and folic acid (IFA) supplementation, heard of albendazole, and causes and preventive measures of anemia. The first four variables were taken as dichotomous variables, labeled as “1” if they knew and “0” if they did not know. The causes and the preventive measures were scored separately. Mothers who know more than two causes/preventive measures were labeled as score “2,” if they know one or two cause(s)/preventive measure(s) were labeled as score “1,” and those who did not know anything were denoted as score “0.” The cumulative score was determined by adding all the scores of variables and was categorized into 4 groups. Mothers who scored “0” were termed as with “no knowledge,” scores “1” as with “low knowledge,” mothers with scores “2–5” as “medium knowledge,” and scores “6–8” as “high knowledge.” The socio-economic status (SES) of the households was generated by using per-capita monthly income (in INR) and categorized as per B. G. Prasad’s modified classification for October 2023 (Mahantshetti et al., 2024). Household size of the respondents ranged from 3 to 13, and were classified into three categories: Small (3–5 members), medium (6–8 members), and large (more than 9 members).
Statistical Analysis
The data analysis was performed using SPSS version 18. Univariate analysis was done to determine the socio-demographic profile of the mothers, and Pearson chi-square test was performed to understand the association of dependent (MDD-W) and independent variables (nutritional). To identify the effect of various independent factors such as current age of the mothers, their education and occupation, ANC visits, parity, anemic conditions, current nutritional status, and nutrition knowledge on MDD intake, only those variables with a p value of .05 during bivariate analyses were selected for further analyses using multivariable logistic regression to control the confounders and detect variables significantly associated with the dependent variable. The estimated adjusted odds ratios (AOR) and 95% CI of the association were declared statistically significant at p < .05.
Results
The age range of the 361 lactating mothers who had a child of 0–23 months was 17–39 years at the time of the survey (Table 1). Most of the mothers were in the age group of 30–34 years (30.75%), followed by 25–29 years (25.21%) and 35–39 years (24.10%). It is pertinent to note here that 6.65% of lactating mothers were still in the adolescent phase of growth at the time of the survey (< 20 years). About half of the mothers had less than 10 years of formal schooling, and 12.74% never attended a school. A higher percentage of husbands (46.81%) had attended more than 10 years of formal schooling compared to the mothers (36.29%); however, the majority of the mothers (77.56%) and their spouses (77.01%) were engaged in cultivation compared to petty business and service. Nearly half of the lactating mothers (47.92%) belonged to the upper-middle class of SES, followed by the middle class (35.18%), and mostly lived in joint/extended families (61.77%). Most of the mothers were multiparous (76.73%) and did not receive the recommended minimum of four ANC visits to the nearby PHC (78.39%). Less than one-fourth (14.40%) had received the recommended minimum four ANC visits, and a considerable number of mothers did not approach the PHC for ANC utilization (7.20%) (Table 1). Based on data harnessed from PHCs for 268 lactating mothers who approached for ANC utilization in the first trimester, 36.19% were reported to be anemic, of which 22.76% were mild, 10.07% were moderate, and 3.36% were severely anemic. Nutritional status based on BMI of the mothers (n = 361) at the time of the survey estimated 23.36% to be underweight and 6.38% to be overweight; no instance of an obese lactating mother was found in the study.
Socio-demographic and Other Background Parameters of the Lactating Mothers of the Present Study (n = 361).
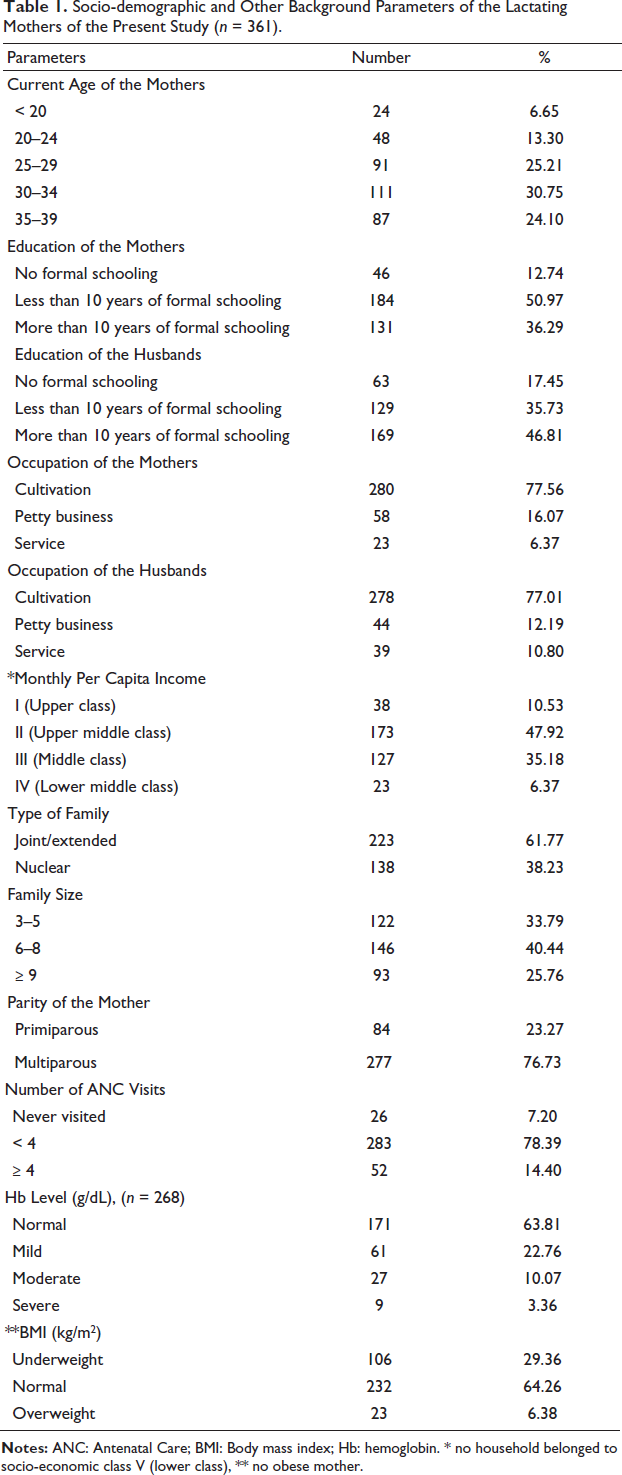
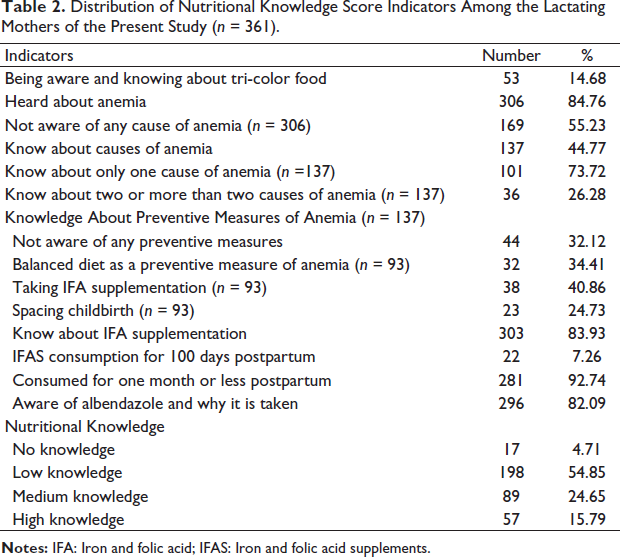
Nutritional knowledge score indicators reported that less than one-fourth (14.68%) of the lactating mothers were aware of tri-color food/tiranga bhojan (Table 2). This is quite astonishing because most of the mothers heard of anemia (84.76%) from the PHC or other health professionals and were diagnosed as normal (63.81%) or anemic (36.19%) at the time of pregnancy (1st trimester), but more than half of the mothers (55.23%) who heard of anemia did not know the cause of anemia. Of the 44.77% of lactating mothers who were aware of causes of anemia, most of them knew only one cause, which was heavy bleeding during menstruation (73.72%); only 26.28% were aware of two or more causes of anemia. Most of the mothers (40.86%) regard taking iron and folic acid supplements (IFAS) as one of the preventive measures of anemia, but most of them lack the knowledge of locally available food resources that are rich in iron content. A balanced diet, which is an important way of maintaining iron and other micronutrient balance in the body, was known by only 34.41% of mothers, though there were a considerable number of lactating mothers who were underweight (29.36%) (Table 1). Many of the mothers (83.93%) were aware of IFAS and albendazole tablets (82.08%) distributed by Accredited Social Health Activist (ASHA) workers and obtained information during ANC visits, but most of the mothers did not comply with the recommended duration of IFAS consumption (92.74%). Nutritional knowledge score indicated that more than half of the lactating mothers (54.85%) had low knowledge on the six nutrition variables under study (Table 2), followed by 24.65% who had medium knowledge, and less than one-fourth (15.79%) had high knowledge.
Distribution of Nutritional Knowledge Score Indicators Among the Lactating Mothers of the Present Study (n = 361).
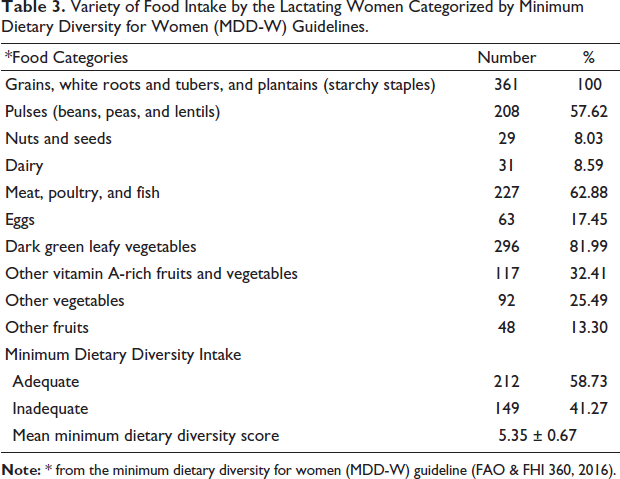
All the lactating mothers consumed starchy staples (rice/tubers/potato/taro) on the previous day of the survey, but interestingly, slightly more than half of them consumed any form of pulses (57.62%) (Table 3). Most of them were reported to consume dark green leafy vegetables (81.99%) either raw or in boiled form. Though certain food taboos were reported to be attached to exclusive breastfeeding up to 3 or 4 months after childbirth, about 62.88% were found to consume meat, poultry, or fish (fresh/fermented). Only a small proportion of the mothers were reported to consume nuts and seeds (mainly sesame seeds, green gourd seeds, and pumpkin seeds in grinded form and sometimes cooked with vegetables) and dairy products by the least (8.59%). They were found to consume locally available and seasonal vegetables and fruits (32.41%) rather than those that were brought from other parts and available in the markets. Based on the MDD score of each, more than half of the total mothers (58.73%) had adequate dietary intake, and 41.27% consumed inadequate dietary diversity. Mean MDD score of the total mothers of the present study was observed to be 5.35 out of the 10 food groups recommended by FAO and FHI 360 (2016).
Variety of Food Intake by the Lactating Women Categorized by Minimum Dietary Diversity for Women (MDD-W) Guidelines.
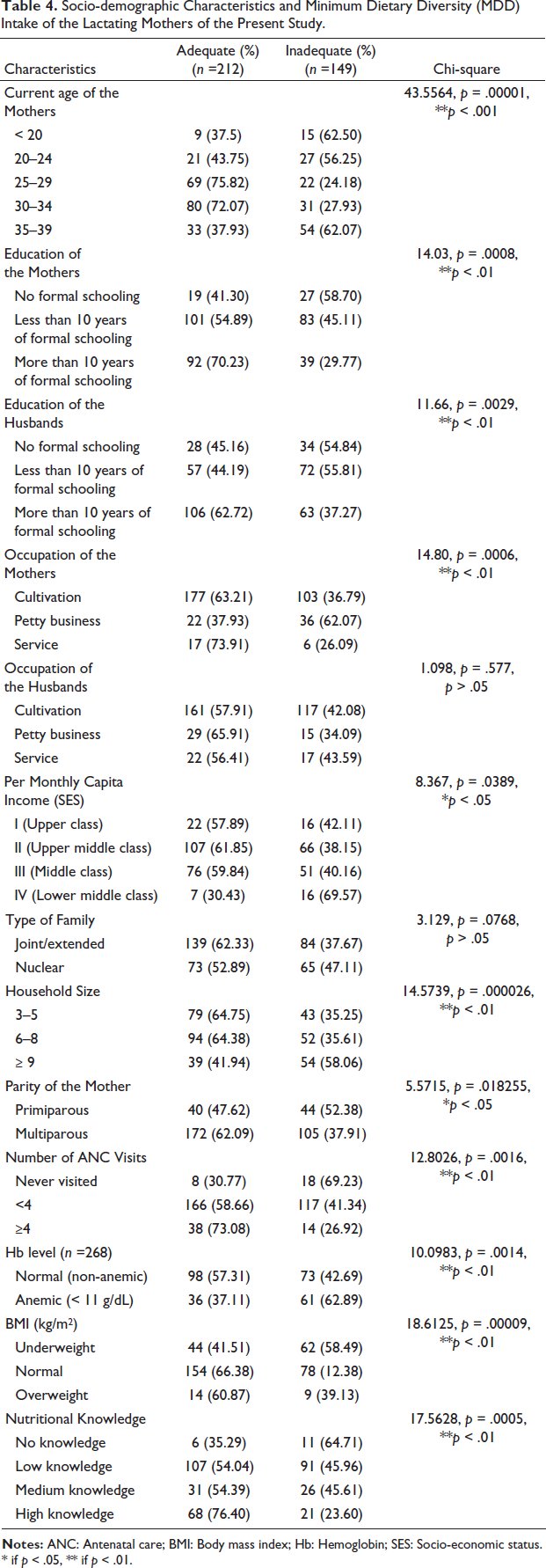
The percentage of lactating mothers who reported adequate dietary diversity intake were significantly high in the age groups of 25–29 years (75.82%) and 30–34 years (72.07%), on the other hand, inadequate dietary diversity intake was significantly high among the adolescent (62.50%) and the middle-aged adult lactating mothers (35–39 years; 62.07%) (p < .001) (Table 4). Similarly, a higher percentage of mothers and their spouses with higher educational attainment and SES (Class I, II, and III) showed adequate MDD intake, thus an association with education and SES was found. The percentage of lactating mothers in the lower-middle socio-economic class (Class IV) significantly reported inadequate dietary diversity intake. Significantly higher numbers of lactating mothers residing in joint/extended family structures (62.33%) with household sizes fewer than nine family members (64.38%) reported adequate dietary diversity intake compared to nuclear family structure (52.89%) and joint/extended family structures (62.33%) with household sizes more than nine family members (41.94%). Thus, household size seemed to have an association with adequacy of MDD. Interestingly, a significantly higher percentage of multiparous lactating mothers reported adequate dietary diversity intake (62.09%) compared to primiparous lactating mothers (47.62%). Majority of lactating mothers who had completed four recommended ANC visits (73.08%) and with high nutrition knowledge (76.40%) had adequate dietary diversity. On the contrary, the majority of lactating mothers who were anemic during pregnancy and underweight at the time of the survey had significantly higher inadequate dietary intake, and this may be the reason for their malnutrition and anemic condition, and vice versa, showing a vicious cycle of inadequacy of MDD and anemia. Type of family and occupation of the husbands were not found to be significantly associated with MDD status of the mothers (p > .05) (Table 4).
Socio-demographic Characteristics and Minimum Dietary Diversity (MDD) Intake of the Lactating Mothers of the Present Study.
Factors that were significantly associated with the MDD status of lactating mothers were incorporated into further statistical analysis to understand the association and possibility of occurrence of the outcome variable on the status of MDD intake (Table 5). In the bivariate logistic regression analysis, current age, years of formal education of the mothers as well as their spouses, occupation of the mothers, SES, household size, ANC visits, anemic conditions, current nutritional status (BMI), and nutritional knowledge were found to be significantly associated with MDD intake status of the lactating mothers. The multivariable logistic regression analysis reported that current age, years of formal education, and occupation of only mothers, SES, ANC visits, anemic conditions, current nutritional status (BMI), and nutritional knowledge were significantly associated with MDD intake status of the lactating mothers. Education of the husbands, household size, and parity of the mothers did not show any association to adequate MDD status (Table 5).
Association of Variables with Minimum Dietary Diversity (MDD) Status of Lactating Mothers of the Present Study.
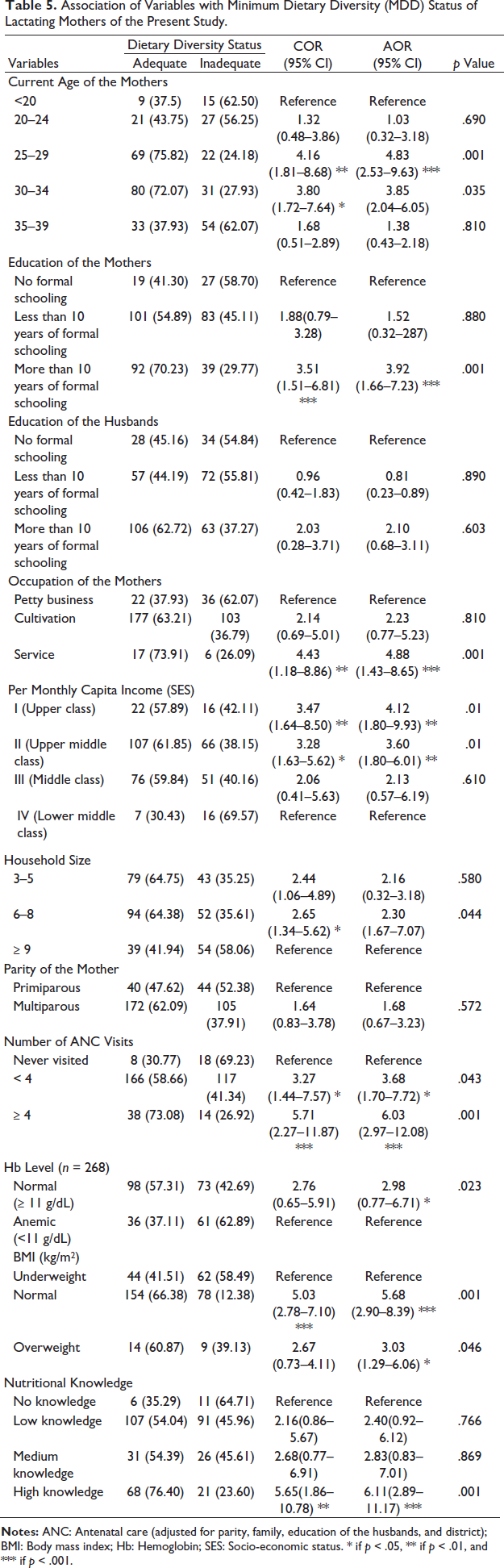
Lactating mothers who were in the age group of 25–29 years were 4.83 times (AOR: 4.83, 95% CI [2.53–9.63]) more likely to have adequate dietary diversity intake than adolescent lactating mothers. Mothers with more than 10 years of formal schooling were 3.92 times (AOR: 3.92, 95% CI [1.66–7.23]) more likely to have adequate MDD intake compared to illiterate mothers (Table 5). Mothers who were in service were 4.88 times more likely to have adequate dietary intake than in petty business (AOR: 4.88, 95% CI [1.43–8.65]) and mothers in higher SES (Upper Class) were 4 times more likely to consume adequate MDD intake compared to lower middle class (Class IV) (AOR: 4.12, 95% CI [1.80–9.93]). Regarding ANC utilization, those who had completed a minimum four recommended visits were six times more likely to consume the recommended adequate MDD than the mothers who never utilized ANC facilities in their last pregnancy (AOR: 6.03, 95% CI [2.97–12.08]). Similarly, the mothers who were non-anemic during the first trimester of last pregnancy were twice more likely to consume adequate dietary diversity and the anemic mothers were reported to have inadequate dietary diversity at the time of the survey also, and the mothers who had adequate nutritional status and normal weight were 5 times more likely to have adequate dietary diversity intake compared to underweight mothers (AOR: 5.68, 95% CI [2.90–8.39]). It was apparent that the lactating mothers with high knowledge on nutrition were 6 times more likely to have adequate MDD intake than the mothers with no knowledge on nutrition (AOR: 6.11, 95% CI [2.89–11.17]) (Table 5).
Discussion
As per the available literature on MDD, this study can be regarded as a pioneering one in identifying the causes of MDD among the tribal lactating mothers in Assam. This study highlighted that MDD is substantially associated with the current age of the mothers, years of formal education and occupation of the mothers, SES, ANC visits, anemic conditions, current nutritional status (BMI), and nutritional knowledge. Education of the husbands, household size, and parity of the mothers did not show any significant association with adequate MDD status. Studies so far conducted abroad and in India have reported that consuming an assortment of food is linked to improved nutritional outcomes among women and children (Chandrasekhar et al., 2017). Improving food intake, particularly during the first 1,000 crucial days after childbirth, is one of the most effective nutritional strategies for preventing deficits and correcting nutritional inadequacy in women of reproductive age and their children (Getacher et al., 2020). Lactating women’s dietary diversity has been linked to their children’s healthy growth and development, and to combat micronutrient deficiency. In the current study, slightly greater than half of lactating mothers had adequate recommended MDD and hence are more likely to consume sufficient micronutrients than their counterparts with insufficient MDD. To maintain optimal micronutrient adequacy, the FAO recommends that all pregnant and lactating mothers meet the minimal DDS. They must consume at least 5 of the 10 food groups (MDD-W) (FAO & FHI 360, 2016). In this study, the mean MDD score was 5.35, which is slightly above the minimum recommended score derived by Gupta et al. (2020) on women in rural India (WDDS = 4.3). Thus, the mothers of the present study consumed one food group higher than the DDS for rural Indian women. Another recent study reported that one food group was higher than the DDS of the present study among the lactating women in Haryana state of India (6.35) (Shumayla et al., 2022). Nongrum et al. (2022) reported significant differences in the dietary diversity among the Khasi and Garo indigenous women of Meghalaya, with one-third (37%) of the women attaining a MDD of five or more food groups in a day, with a MDD score of 4.22, which was lower than the present study. They found an inverse association between the number of land uses and dietary diversity. Other studies conducted in the neighboring countries like Bangladesh (mean DDS 4.28) (Shamim et al., 2016), Nepal (DDS 3.9 ± 1.0) (Henjum et al., 2015), and Pakistan (mean food group diversity score 4 ± 1) (Brazier et al., 2020) on lactating, pregnant, and reproductive women reported a lower DDS score than the present study on the Mishing tribal lactating mothers. Though a considerable number of lactating mothers were underweight and diagnosed with anemia, only a half of them consumed the adequate dietary diversity and a small number of them were aware of tri-color foods in daily consumption in the present study because the tiranga bhojan approach is still to be disseminated in the communities in Assam by various governmental/non-governmental agencies to combat malnutrition and anemia ensuring that saffron, white, and green foods are included in each meal. Less awareness of tricolor food among lactating mothers was also found by other studies in India (Shumayla et al., 2022).
Furthermore, it is interesting in this present study that all the lactating mothers had starchy staples on the previous day, but only about half of them consumed pulses, and a smaller number of mothers consumed vitamin A-rich fruits. This result is consistent with other studies, which discovered that women’s diets are especially deficient in non-staple food groups such as vitamin A-rich fruits and vegetables, dairy, eggs, and green leafy vegetables in India (Gupta et al., 2020). Another study from Karnataka, India, discovered similar results to the present study, where all women consumed starchy staples, comparatively less than that consumed pulses, and less than 5% consumed egg and meat in their diet (Shashikantha et al., 2016). Rajpal et al. (2021) made a study in the tribal-dominated district of Palghar in Maharashtra, India, and reported that three-fourths of lactating mothers during early lactation and 66.5% during late lactation did not consume fruits in the last 24 h, which was also evident in most of the lactating mothers of the present study. The same study also supports the present study’s finding, where the consumption of dairy products and eggs was also low, as the majority of lactating mothers did not have a meal that included dairy products and eggs on the previous day of the study. In Manipur, the consumption of dairy products, fruits, and fats and oils was found to be very low among the Meitei women of reproductive age (Loukrakpam et al., 2020), which may be the reason for vitamin A deficiency in children and mothers. Due to preexisting dietary patterns and limited access to dairy products, as domestication of animals for dairy needs was not observed in most of the tribes of North-East India, most adult women and older children did not consume dairy products (Priscilla et al., 2016), which is consistent with the present study on the Mishing community. Consumption of high-carbohydrate content food groups like rice, millets, roots, and tubers was high in all the age groups of the study mothers. A similar trend of food consumption rich in carbohydrates was also reported in the Khasi children from Meghalaya (Chyne et al., 2017), Meitei children and women from Manipur (Loukrakpam et al., 2020) in North-East India. The traditionally fermented and dried fish, along with smoked pork, were almost consumed frequently in the community of the present study, like other tribal communities of North-East India. Though preferences and food taboos exist in the Mishing community, these gendered food ideologies give cultural legitimacy to the dietary practices of young girls, pregnant women, breastfeeding mothers, and infants, which was also observed in other studies in the Indian context (Bhattacharya, 2023). These practices may place women in a structurally disadvantageous position, which could have serious consequences for both the women and their children.
Lactation is one of the most intricate and nutrient-demanding stages of the human life cycle. Since nutritional knowledge is the cornerstone for combating malnutrition at all levels of society and plays a significant role in influencing dietary practices that ensure that nutrient needs throughout the lifecycle are met, adequate nutrition knowledge during lactation plays a greater role in optimal nutrient balance and survival of the children (Pratt et al., 2014). According to studies, lactating mothers are particularly susceptible to malnutrition because of their reduced food intake and/or infrequency of meals and low nutritional knowledge. The present study revealed that about half of the lactating mothers had low knowledge of nutrition, and less than one-fourth had high nutrition knowledge. Additionally, nutritional knowledge of mothers was statistically associated with nutritional practices. It was apparent that the lactating mothers with high knowledge of nutrition were 6 times more likely to have adequate MDD intake than the mothers with no knowledge of nutrition. Similar studies done in Ethiopia (Tessema et al., 2020) and India (Sharma et al., 2020; Shumayla et al., 2022) showed that knowledge was a significantly associated factor in dietary diversity practice. This result was supported by the fact that good knowledge about basic nutrients and an adequate, well-balanced diet usually result in positive dietary practices, which are important determinants of optimum overall health throughout life. Inadequate dietary diversity was more likely to be present in lactating mothers with no or low nutrition knowledge, unlike their peers with good nutrition knowledge. This finding is consistent with research carried out by FAO and FHI 360 (2016), Shumayla et al. (2022), and Getacher et al. (2020). The reason for such a picture from the present study was that the lactating mothers who had medium/high nutrition knowledge had higher education, approached the health care providers during pregnancy in ANC visits, and understood the importance of a wide variety of foods, and were more likely to consume these foods for the better health of the growing fetus. The women’s increased understanding of the variety of food groups contributed to their appropriate intake and consumption. The results also revealed that mothers may benefit from varied dietary counseling and information when they visit a health center for ANC. Similar results were reported by Boke and Geremew (2018) among the lactating mothers in Angecha districts, Southern Ethiopia. Tilahun and Kebede (2021) revealed that among pregnant women of Southwest Ethiopia, mothers who received nutrition advice were 2.2 times more likely to fulfil the MDD than mothers who did not receive nutrition information.
The present study revealed a discernible gradient in the percentage of women with MDD across income brackets, with mothers from higher SES households showing a higher probability of dietary diversity, which was also reported from a study in the tribal-dominated district of Palghar in Maharashtra, India (Rajpal et al., 2021). According to a recent study based on NFHS 2015-2016 (IIPS), mothers’ education levels, not their poverty status, were substantially correlated with their consumption of legumes, nuts, meat-based foods, pumpkin, and carrots (Agrawal et al., 2019), whereas, like the present study, other studies reported an association between adequate MDD and SES in India (Pal et al., 2017). When compared to the adolescent and emerging adult (20–24 years), lactating mothers, young adult lactating mothers had considerably higher adequate MDD in the present study, which had been observed in other studies done across the globe (Gitagia et al., 2019; Shumayla et al., 2022). The reason for these differences may be that young adult mothers with low parity are more aware of the dietary possibilities available in their community than the adolescent primiparous mothers and acquire autonomy to choose and cook different food items available (Acharya et al., 2010). In Assam, the percentage of underweight and pregnant anemic women was reported to be 17.60% and 54.20%, respectively (IIPS & ICF, 2021)—pregnant women who are anemic. The POSHAN Abhiyaan, the Government of India’s flagship program, aims at improving nutritional outcomes among pregnant women, lactating mothers, and children by reducing the level of stunting, underweight, anemia, and low birth weight by 2022. The data has shown that the outlaid budget has been meagerly utilized by the North-Eastern states, except for Mizoram, which had utilized 65.12% as of 2019. Assam is suggested as the worst performer in improving education for women, reducing infant, child, and maternal mortality rates, undernutrition, and prevalence of anemia in pregnant women, according to the comparisons made between NFHS-4 and NFHS-5 (Tantri et al., 2022). One of the promising steps to ameliorate these adverse outcomes is to improve the MDD status so that, right from the beginning of growth and development, a female can get adequate nutrition in the form of dietary diversity, and optimal outcomes can be transmitted to the next generation.
Limitations and Strengths
The limitations were that, as it was a cross-sectional study, the causal relationship between independent and outcome variables could not be established. In addition to that, the determination of MDD was derived from recall responses, which were based on accuracy and memory of the participants; thus, there are possible errors, but utmost care has been taken with established criteria and practices to keep the errors at a minimum level. The strengths were that it is a community-based study done in Assam among a tribal community, which has its own unique dietary habits and diversity, and this may be one of the newest domains to be studied in this part of the country. There have been limited studies with such an in-depth analysis on MDD of lactating mothers who need immediate attention on health and nutrition adequacies in Assam. This study provides baseline evidence and highlights that ANC programs are quintessential in nutrition-specific intervention with this vital segment of the population.
Conclusion
This study attempted to determine the prevalence of MDD and the associated factors among the lactating mothers belonging to the Mishing tribal community inhabiting Upper Assam of North-East India. The study clearly revealed the importance of formal education and occupation of the mothers, SES, ANC visits, anemic conditions, current nutritional status, and nutritional knowledge in achieving the MDD and, thus, enhanced nutrient intake among lactating women. Slightly greater than half of lactating mothers had adequate recommended minimum dietary intake, but discovered that diets are especially deficient in non-staple food groups such as vitamin A-rich fruits, dairy, eggs, nuts, and seeds. Though a considerable number of lactating mothers were underweight and diagnosed with anemia, only half of them consumed an adequate dietary diversity. A small number of them were aware of tri-color foods in daily consumption in the present study because the tiranga bhojan approach is still to be spread in the communities in Assam by health care agencies. Here, the role of PHC and ANC utilization emerged as the most powerful game changer in combating malnutrition and anemia and in ensuring any nutrition-specific intervention among lactating mothers.
Footnotes
Declaration of Conflict of Interests
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Informed consent in written form was obtained from the participants, and ethical consent was taken from the Ethical Committee for Biomedical and Health Research (ECBHR), Dibrugarh University, Assam.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.