
Abstract
Background
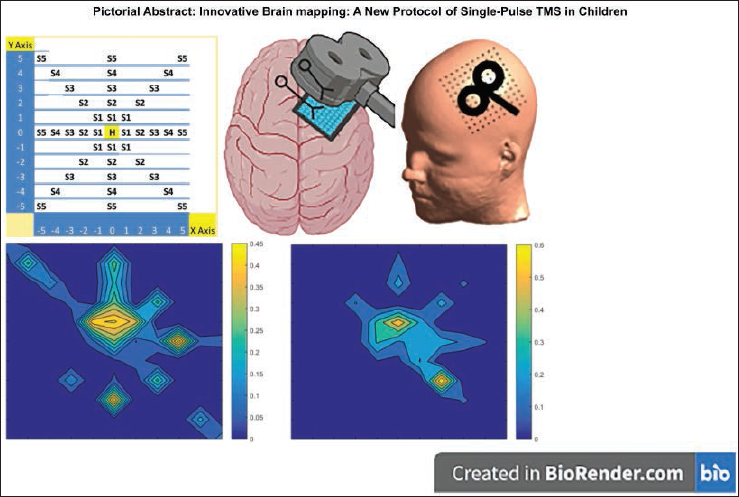
Single-pulse paradigms of transcranial magnetic stimulation (TMS) have been used to understand cortical excitability and reorganisation.
Purpose
This study aims to develop a protocol for mapping of the primary motor cortex (M1) using single-pulse TMS in children.
Methods
A 11×11 manual grid was created around the hotspot of abductor pollicis brevis (APB). Motor-evoked potential (MEP) amplitude was recorded from 41 sites around the hotspot of APB and analysed.
Results
Maximum MEP amplitude was recorded from the hotspot that reduced as distance increased. Heat maps generated were consistent among the participants.
Conclusion
In children, 41 single-pulse TMS stimulations with interstimulus interval of two seconds provide reliable information about motor maps. This procedure will aid in understanding cortical reorganisation in children with neurodevelopmental disorders.
Keywords
Introduction
The human brain’s intricacy is magnificent, coordinated circuitry that enables us to perform goal-directed fine-skilled movement and tasks. 1 The brain injury that occurs early in childhood affects the normal development of these brain networks and can even result in the modification of the brain’s architecture permanently. To better describe trauma-induced cortical alterations and underlying mechanisms, it is critical to integrate and analyse personalised somatotopy of the primary motor cortical areas, leading to targeted treatments and early diagnosis and prognosis of disease. 2 Cortical motor mapping is proposed to be a valuable neurophysiological metric for assessing the cortical topography and plasticity as well as motor function following brain injury, insult or skilled training.3, 4 In children, especially, use of non-invasive techniques like single-pulse transcranial magnetic stimulation (TMS) is desirable to unravel cortical remodelling in disorders of early childhood like cerebral palsy and autism, for the initiation of timely focussed treatments.
TMS, due to its clinical applications, is found to be an invaluable technique in the field of neurophysiology which is proved in many studies to be safe and well-bearable by participants.5, 6 This non-invasive technique in adults has been used for investigating alterations in the motor cortical representation of the body areas in various neurodegenerative disorders by analysing amplitudes of motor-evoked potentials (MEPs) recorded from the motor areas surrounding the target muscle hotspot.7–9 Both traditional manual grid and pseudorandom walk method have been shown to generate reliable motor maps; however, the number of stimuli given and stimulation sites were large, making it protracting for children.6, 8 Though TMS is a safe technique, a few studies have still raised questions on its safety in which it has been emphasised that there are possibilities of adverse events including seizures with longer sessions and greater stimulations.10, 11 Keeping this information in mind, this study aims to develop a new method for motor mapping in children using a limited number of stimulation sites that would be efficacious as well as safe for fragile patients.
Materials and Methods
Participant and Recruitment
Four healthy control male children participated in the study, aged 7–17 years, ambidextrous, from a well socioeconomic background belonging to upper middle class, scored between 16 and 25 according to the modified Kuppuswamy socioeconomic scale, 12 with at least one person, either father or mother, as main source of income in the family and a stable occupation, having their children enrolled at a school. Informed consent was taken from the parents of each participant before screening. The subjective data was collected to ensure no neurological condition, affecting the posture or sensorimotor functions of any of the extremities. Further, history was taken about neurorehabilitation, if any received previously.
Electromyography
Silver-silver chloride (Ag/AgCl) gelled surface electrodes were placed on the abductor pollicis brevis (APB; right hand) and were connected to the Neuro-MEP amplifier (Neurosoft, Ivanovo, Russia) to study the electrical signal acquisition using Neuro-MS/D (Neurosoft, Ivanovo, Russia). The participants were seated comfortably in the medical chair during the procedure. Baseline parameters including resting (RMT) and active (AMT) motor threshold were recorded with the help of a figure-of-8 coil placed on the scalp (primary motor cortex, dominant hand area) of the contralateral hemisphere. The minimum stimulus intensity required to elicit a MEP response of amplitude ≥50 and ≥100 µV in at least 5 out of 10 trials was considered as threshold for RMT and AMT respectively. The corresponding MEP amplitudes of RMT and AMT obtained in these five trials were taken as mean value. 13
Transcranial Magnetic Stimulation
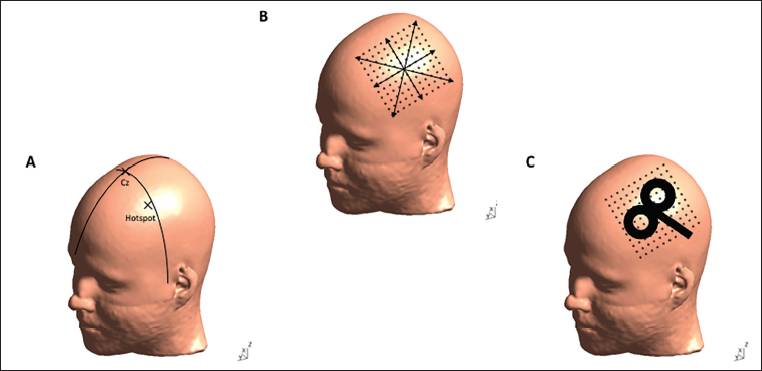
To map the primary motor cortex (M1), the hotspot of the APB was localised using the International 10-5 and 10-20 electroencephalography (EEG) system. 14 The identification of the required points (C1, C3h, C3) on the scalp was performed by two skilled and experienced researchers.
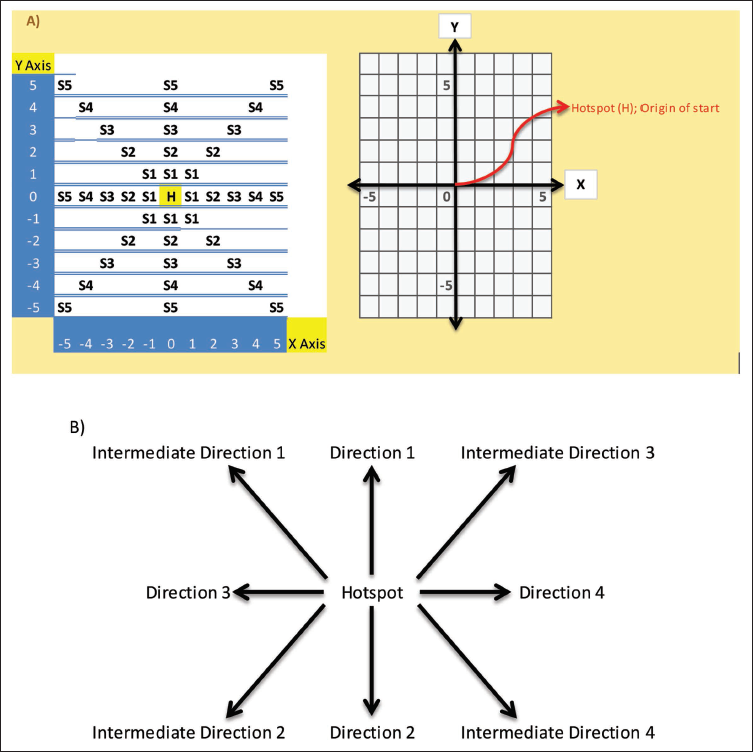
A manual grid of 11×11 dimensions was designed for brain mapping around the hotspot, on a customised scalp fitted cap, having a total of 41 stimulation sites marked on it. During the recordings, to ensure accurate placement of the coil at the same location, the subjects were made to wear this fitted cap. The grid was placed in relation to surface landmarks: vertex and inter-auricular line. The centre of the grid was considered as the location of the hotspot from where the coil was moved in total eight marked cardinal (4) and intercardinal (4) directions during the procedure in a chronological order, keeping the coil firmly at an angle of 45 degrees during the entire procedure. Every direction consisted of five stimulation sites each with 1 cm of spacing in between (Figure 1). The targeted locations were then stimulated sequentially (total 5 stimuli per marked site) with an interstimulus interval of two seconds with single-pulse TMS at an intensity of 120% RMT recorded at the baseline. Pre- and post-TMS recordings, the children with their parents were asked to fill in a questionnaire reporting adverse events.
The recorded MEP data was then plotted on a cartesian plane and converted into a matrix in MATLAB version R2022b (MathWorks, Inc., Natick, Massachusetts, United States) for generating the brain heat map. The defined hotspot is positioned in the centre of the matrix and was considered as the origin or start point while performing brain mapping procedure (Figure 2).
(A) Representation of the Aligned MEP Data According to the Stimulation Sites (Total 41 Sites) on the Manually Designed Grid Plotted on x-y Plane. H = Hotspot (Origin); S(n) = Stimulation Site, Where n Is an Integer. (B) Chronology of the Directions Followed in Which the TMS Coil Was Moved to Stimulate the Marked Sites in Part (A).
Data Collection
Neuro MEP.Net (V.4.5.1.2) was used for electromyographic data collection. The software was synchronised to the stimulator and the TMS coil to record MEP at baseline and during motor mapping.
Results
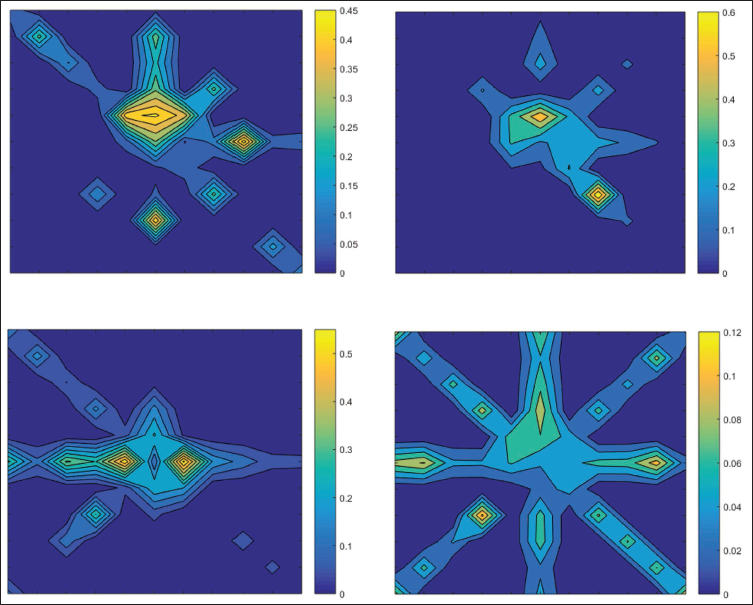
The participants successfully completed the study and reported no adverse events during the procedure further indicating the tolerability of the technique. Figure 3 depicts the generated cortical contour heat maps of all four participants, showing difference in the excitability of the region surrounding the hotspot (differential colours). The colours refer to the range of the MEP amplitudes recorded during the mapping procedure. This range goes from dark blue to light yellow, indicating the change in amplitude from having no or least values to the maximum.
Notably, around the hotspot region, the recorded MEP had larger amplitudes which reduced as we moved the coil farther away from the hotspot, confirming that most excitable region of the grey matter for APB in primary motor cortex is the hotspot area.
A Detailed 2D Contour Heat Map of the Four Participants. The Colour Ranges from Dark Blue to Light Yellow Indicate MEP Amplitude from Not Recordable or Least Values to Maximum.
The acquisition of the contour heat maps with different colours indicating differential excitability was followed by the empirical data that was quantified based on the MEP values ≥50 µV as shown by the colour bars. We computed the total area and volume of the excited regions in each map of each participant (Table 1). The area was approximated by considering the product of the sum of the number of excited grid points of the mapping data and grid spacing (1 cm2). 6
Mathematically,

Where variables i and j are the indexes of summation of values from 0.05 to the values of m × n matrix, where m is the number of rows and n is the number of columns on the grid.
Computed Total Area and Volume of the Excited Regions on the Contour Heat Maps of the Four Participants.
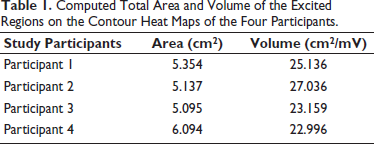
The volume (cm2/mV) was computed with help of the following formula
6
:

Table 1 shows uniformity among the four participants in the area and volume of the regions around the hotspot that were excited with varying shades of colours. The total average area of APB muscle as recorded by single-pulse TMS is 5.42 cm2 and volume is 24.58 cm2/mV.
Discussion
This study aimed to develop a new technique using single-pulse TMS cortical mapping with reduced number of stimuli in children, for application to unravel the somatotopy and cortical reorganisation under diseased conditions. We were successfully able to standardise the method of mapping APB region on M1, by recording MEP amplitudes. Highest amplitude of MEP was observed at the hotspot that also corresponded to the region that elicited least resting motor threshold, indicating presence of maximum number of motor neurons with utmost excitability innervating APB muscle in this region. As we proceeded in other cardinal directions and at farther distances from the hotspot, the amplitude reduced, suggesting presence of motor neurons with less excitability or having overlapping receptive fields with primary neurons. Thus, overall the heat maps generated provide information indirectly about the number and state (activated or inactivated) of the neurons surrounding the hotspot. Individual finger digits have been shown to be somatotopically organised in both primary motor and sensory cortices for sensorimotor integrations with thumb placed laterally. 15 The brain reorganisation process is generally adaptive, with the extent of changes determined by multiple factors like age, usage, needs, experience of an individual and during trauma, the extent and severity of damage.16, 17 Understanding of these plastic changes following injury may lead to better ways of facilitating reorganisations that are beneficial and preventing those with undesirable outcomes.
In healthy adults, both manual and robotic neural navigated methods have been used for mapping the motor cortex. In a study conducted by van de Ruit et al., 8 a two minutes protocol is proposed with minimum number of 63 stimuli and recommended at least 80 stimuli to be delivered to map the cortical area with interstimulus interval of 1–4 s. Though no adverse events were reported in the study, in fragile children, such as in patients with cerebral palsy or autism, stimulating the cortical regions based on the inter-participant variability may make them vulnerable to seizures (who may be more anxious or have lower seizure thresholds). We designed grid with reduced number of stimulation sites to 41, to attenuate the susceptibility and enable the researchers to map primary motor cortex without jeopardising the experimental population being studied. This reduction in stimuli is particularly advantageous for children, improving tolerability and safety while still yielding consistent motor maps, which is very imperative for researchers to comprehend. Further, map volume and hotspot magnitude are suggested to be the most reliable measures if mapping is done repeatedly at short- or long-time gaps in healthy participants.6, 18 The reduced number of stimuli along with recording of MEP amplitudes, generation of heat maps and their volume, enables noninvasive assessment of cortical reorganisation and plasticity with great tolerance, may also be advantageous to patients with other neurodevelopmental/neurological/neuromuscular disorders. We presume this simple technique will be helpful to understand the cortical alterations in paediatric population after trauma or in monitoring therapeutic efficacy of neuromodulatory interventions like neurorehabilitation/ transcranial magnetic stimulation that has the potential to modify neural plasticity in children.19, 20
The current brain mapping technique utilising MEP recordings holds significant clinical applications, particularly in neurorehabilitation. By integrating MEP-based assessments, healthcare providers can track patient progress over time, offering a quantitative measure of cortical excitability and plasticity. This may allow for a more personalised approach to treatment, where therapy plans can be adjusted based on real-time physiological responses. Such adaptability ensures that interventions remain effective and responsive to a patient’s evolving needs. Additionally, this quicker and safer technique can aid in early diagnosis and prognosis evaluation, helping clinicians determine the extent of motor cortex remodelling in conditions like cerebral palsy, autism and other neurodevelopmental disorders. This will provide guidance in the development of targeted rehabilitation strategies, enhance the precision and efficiency of neurorehabilitation, ensuring that treatments are optimised to improve motor function and overall quality of life (QoL) for children with neurological deficits. 21
The main limitation of the study is small sample size of only four participants and all males from similar socioeconomic status, as recruiting healthy children for brain stimulation study is a major challenge. Further, considering the paediatric population for the study protocol, motor mapping was done only for one target muscle (APB), mapping of other muscles and in both the cortices remains to be explored. We also did motor mapping manually, wherein the coil was moved gradually and precisely covering all the points on the designed grid, using a customised fitted cap placed on the scalp of each participant according to the International 10-20 EEG system. This was done as direct physical contact with the child helped in reducing the anxiety of both parents and child as well as head movements substantially during the procedure. 22 However, usage of neuronavigation system along with operator training may help in reducing the human errors, if any, while handling the coil.
Conclusion
We were able to successfully develop a new method for brain mapping with minimum number of stimulation sites to ensure safety and tolerability among the paediatric population. Single-pulse TMS brain mapping technique is a cost-effective strategy to map the cortical regions and can be very useful to understand the representations and alterations in the somatotopy of each hemisphere in health and disease. The developed technique is new and will add on to the evidence-based clinical practice for prognostic and therapeutic purposes in children. However, surplus research in this area is warranted to develop better and improved validated protocols that can be applicable for vast number of conditions and larger cohorts associated with brain injuries or atypical reorganisations. Furthermore, exploring the mapping of multiple muscle groups or larger cortical areas within a single session could determine the protocol’s scalability.
Abbreviations
S1: Primary somatosensory cortex (often referred to as somatosensory area 1)
RMT: Resting motor threshold
QoL: Quality of life
MEP: Motor evoked potentials
M1: Primary motor cortex (often referred to as motor area 1)
FDA: Food and Drug Administration
EEG: Electroencephalography
C3: Channel 3
C1: Channel 1
APB: Abductor pollicis brevis
AMT: Active motor threshold
Ag/AgCl: Silver-silver chloride
3D: Three-dimensional
2D: Two-dimensional
Footnotes
Acknowledgement
We thank Mr Sanjeev Kumar and Mr Praveen for providing administrative and technical support and assistance in the management and handling of young children during electrophysiological recordings. The pictorial abstract was created with the help of the BioRender app and the ![]() was created with the help of SimNIBS software (version 4.5.0).
was created with the help of SimNIBS software (version 4.5.0).
Authors’ Contribution
Suman Jain: contributed to conceptualisation, visualisation and project administration.
Rudraksh Banga: was involved in methodology.
Aliya Mufti and Suman Jain: helped in software.
Suman Jain and Sheffali Gulati: validated the study.
Rudraksh Banga, Aliya Mufti and Suman Jain: were involved in formal analysis, investigation and resources.
Sheffali Gulati, Sanjay Wadhwa, Kapil Sikka and Rohit Saxena: helped in data curation.
Rudraksh Banga and Aliya Mufti: helped in funding acquisition and writing—original draft preparation, and review and editing.
Sanjay Wadhwa, Kapil Sikka, Rohit Saxena, Md. Iqbal Alam, Kanwal Preet Kochhar: supervised the study.
All authors have read and agreed to the published version of the manuscript.
Statement of Ethics
The study approved by the Institutional Ethics Committee of AIIMS Delhi (IECPG-574/14.11.2018) and it was also conducted in accordance with the World Medical Association’s Declaration of Helsinki (2000).
Declaration of Conflicting Interests
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Funding
The financial support was provided by Indian Council of Medical Research (ICMR) Delhi Government of India.
Informed Consent
All of the subjects were informed about the nature and purpose of the study and provided written informed consent/assent, which was obtained from each participant or their legally authorised representative.