
Abstract
Background
Children with chronic kidney disease (CKD) are at risk of inferior neurocognitive outcomes. As the brain develops rapidly during the early years of life, we wanted to find out the impact of CKD on neurocognition when it occurs during this time and any disease-associated risk factors.
Methods
A cross-sectional case-control study was conducted in the Paediatric Nephrology Clinic, PGIMER, Chandigarh. After obtaining parental consent, 52 children with CKD Stage 3–5 and 52 age-matched case controls were enrolled in the study. Neurocognitive outcome was assessed by the Developmental Assessment Scales for Indian Infants (DASII). Proper statistical tests were used to analyse the data.
Results
Mean comparison revealed that CKD children performed significantly lower on mental functions, motor functions and developmental quotient of DASII. Neurocognitive functions declined with disease progression, with children of CKD Stage 5 scoring lowest. Further, there was a significant difference in weight, height/length and head circumference between those in Stage 3 and 5. Similarly, there are significant mean differences in Hb, MCH, and MCHC levels between Stage 3 and both Stage 4 and 5, but no significant difference between those in Stage 4 and 5.
Conclusion
CKD is a debilitating condition that can have a significant impact on the health and development of children. Neurocognitive outcome declines as the stage of CKD progresses, which worsens their overall outcomes.
Keywords
Introduction
Children with chronic kidney disease (CKD) are at increased risk of complications, such as anaemia, growth retardation, mineral bone disorder, cardiovascular complications, with impaired quality of life (QOL). 1 In addition to all these complications, a study on children aged 6–18 years showed that CKD decreases their cognitive and academic outcomes. 2 The increased risk of impairment of overall cognitive function may be related to the severity and duration of kidney disease. 3 End-stage kidney disease (ESKD) diagnosed during infancy has been previously associated with poor neurocognitive outcomes. 4 The spectrum of neurocognitive abnormalities in these children ranges from mild symptoms, such as simple defects in verbal abstraction abilities leading to poor scholastic performance, to severe symptoms such as intracerebral infarcts. 5
The development of the brain in the first 2 years of life is critical, and any insult to it during this period can have an impact on its development and growth. 6 Kidney function gradually deteriorates in the latter stages of CKD, with Stage 5 being the most severe. The accumulation of toxins that the kidneys would usually filter out increases the probability of neurocognitive dysfunction. There are limited studies on neurocognitive difficulties in younger children with CKD.2, 3, 5, 7 The factors known to affect neurocognitive function in children with CKD are disease severity, younger age at onset of disease, longer duration of disease, presence of hypertension, proteinuria, malnutrition, etc.2, 3, 7, 8 It is important to recognise the neurocognitive deficits early in children with CKD because prompt intervention can improve QOL and school performance.9–11 While most of the studies are retrospective and involved few patients, we wanted to study the neurological outcomes in children less than 30 months of age with CKD Stage 3–5 and tried to examine other disease variables responsible for any adverse outcome in a larger prospective cohort.
Material and Methods
Study Design
Cross-sectional case-control study.
Setting
The study was carried out in the Paediatric Nephrology Clinic, Advanced Paediatric Centre, PGIMER, Chandigarh.
Participants
There were 52 children in Stages 3–5 of CKD, as well as 52 age-matched controls. After receiving parental consent, study participants were enrolled.
Procedure
The Institutional Ethics Committee (INT/IEC/2018/000469) in Chandigarh approved the study, and all participants’ parents or legal guardians gave their assent after being given complete information about the study. Participants were recruited from the Paediatric Nephrology Clinic of PGIMER in Chandigarh, India, from June 2018 to December 2019. A minimum of 50 cases and 50 controls were expected, though the study was kept open-ended. We enrolled 52 children aged 3–30 months with CKD Stage 3 or higher over the course of 18 months; children with neurological problems were excluded. Fifty-two healthy children from a vaccination clinic who were matched for age comprised the control group.
The information was obtained using a standardised questionnaire for demographic details, medical and clinical history. Clinical details and examination were recorded in a predesigned case record form. Relevant investigations done routinely for cases were documented. No blood tests were done for controls. Developmental Assessment Scales for Indian Infants (DASII) was used to measure neurocognitive outcomes, and it was administered by trained psychologists who were unaware of the participant’s CKD status. The rationale to select DASII as our investigation tool was its proven sensitivity and specificity in Indian children. 12 Neurocognitive outcome was noted under three domains—motor quotient (MoQ), mental quotient (MeQ) and development quotient (DQ).
Statistical Analysis
The statistical analysis was carried out using IBM SPSS (Statistical Package for Social Sciences) statistical version 23. Normality of data was checked by the Kolmogorov-Smirnov test. For normally distributed data, mean was compared with respect to parametric inference. For not normally distributed data, median was compared using non-parametric inference. All quantitative variables were estimated using measures of central location (mean and median) and measures of dispersion (standard deviation). Mean was compared with respect to an independent t-test (for two groups) and One-way ANOVA for multiple comparisons (for more than two groups). Median is compared using the non-parametric inference Kruskal-Wallis Test (for more than two groups). For the relationship, we used Pearson’s correlation and the ROC curve for sensitivity and specificity. All statistical tests were seen at a two-tailed level of significance (p ≤ .01 and p ≤ .05).
Results
Baseline Characteristics of Participants
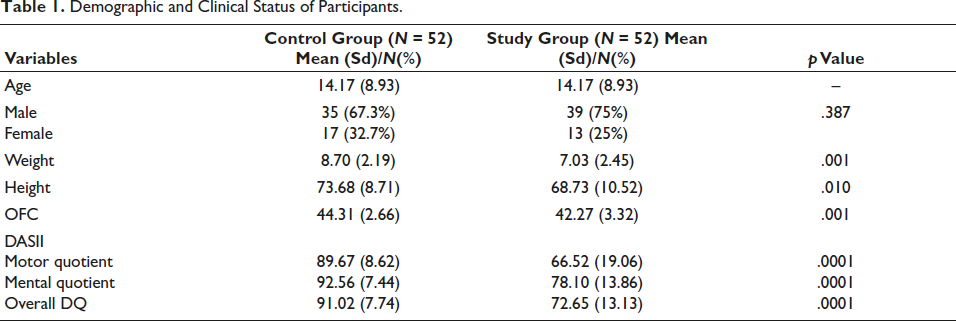
In this cross-sectional comparative study, 52 children with CKD Stage 3 and above, aged 3–30 months, were included in the study group. A similar number of healthy age and sex matched children were taken as controls. The mean age for both groups was 14.17 +/- 8.93 months. Gender-wise, there were more males in the study group 39 (75%) than in the control group 35 (67.3%). We found significant differences in weight (p = .001), height (p = .010) and OFC (p = .001) between the groups, with the study group having lower mean values than the control group for each of these parameters (Table 1).
Demographic and Clinical Status of Participants.
Clinical Characteristics of Study Group Participants
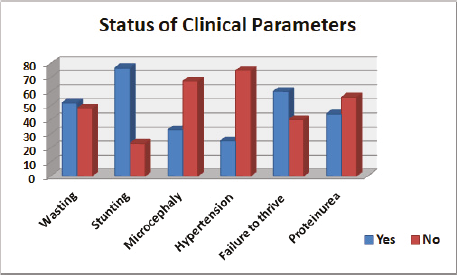
There were 23 (44%) children with CKD Stage 3, 23 (44%) in Stage 4 and 6 (11%) in Stage 5. Out of the 52 participants, 27 (52%) had wasting, 40 (77%) had stunting, 17 (33%) had microcephaly, and 13 (25%) had hypertension. About one third of study participants had cystic kidney disease (33%), followed by PUV (27%) (Figure 1). Proteinuria was present in 33% (though only 2% had nephrotic range).
Status of Clinical Parameters Among Study Participants.
Neurocognitive Functions of Study and Control Group Participants
DASII was used to assess the neurocognitive functions of the participants, and we observed that the study group performed considerably poorer than the control group in terms of MoQ, MeQ, and total developmental quotient (DQ). The mean MoQ in CKD children was 66.52 ± 19.06 compared to 89.67 ± 8.62 in the healthy group (p = .001). The mean MeQ was 78.10 ± 13.86 in CKD children compared to 92.56 ± 7.44 in the healthy group (p = .001). The mean DQ in CKD children was 72.63 ± 15.15, and in the healthy group was 91.03 ± 7.74, with p = .001 (Table 1).
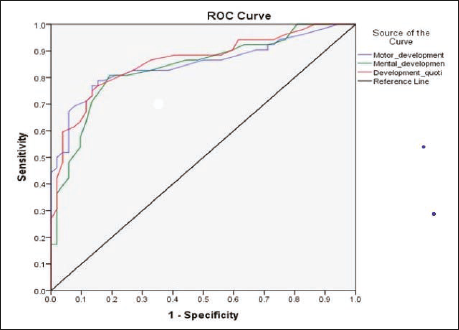
The ROC values demonstrate that the diagnostic accuracy of DASII is good at identifying children with developmental delay from those without. Developmental quotient: sensitivity 0.788; specificity 0.808; 95% CI: 0.789–0.933. Motor: sensitivity 0.788; specificity 0.846; 95% CI: 0.772–0.927. Mental: sensitivity 0.808; specificity 0.808; 95% CI: 0.760–0.916. This shows that for each test, the test accurately identified 81%–85% of healthy children as not having a significant developmental delay and 79%–81% of children who had a significant developmental delay. Each of the three tests has a ROC value more than 0.8, which suggests the tests are effective in differentiating between CKD children with developmental delay and healthy children (Figure 2).
Receiver Operating Characteristic (ROC) Curve for Predicting Developmental Status.
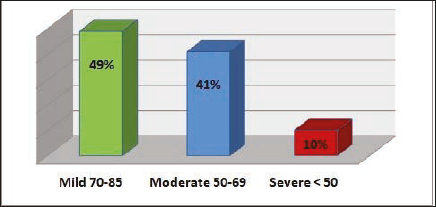
Based on DQ, neurocognitive delay can be further classified into mild (70–85), moderate (50–70) and severe (<50) delay. In our study, mild developmental delay was found in 49% of cases, 41% had moderate, and 10% had severe developmental delay. Disease-wise and group-wise developmental status has been presented in Figure 3.
Severity of Developmental Delay in the Study Group.
Stage-wise comparison revealed that, as compared to children with early stages of CKD, children with advanced CKD stages have poorer neurocognitive outcomes and clinical parameters, such as weight, height, head circumference, haemoglobin and metabolic acidosis.
The findings indicate that as CKD stage increases, weight, height, and head circumference all significantly decline. Compared to Stage 3, haemoglobin levels drastically drop in Stages 4 and 5. Compared to Stage 3, metabolic acidosis is more common in Stages 4 and 5 (Table 2).
Comparison of Clinical and Biochemical Parameters Across CKD Stages.
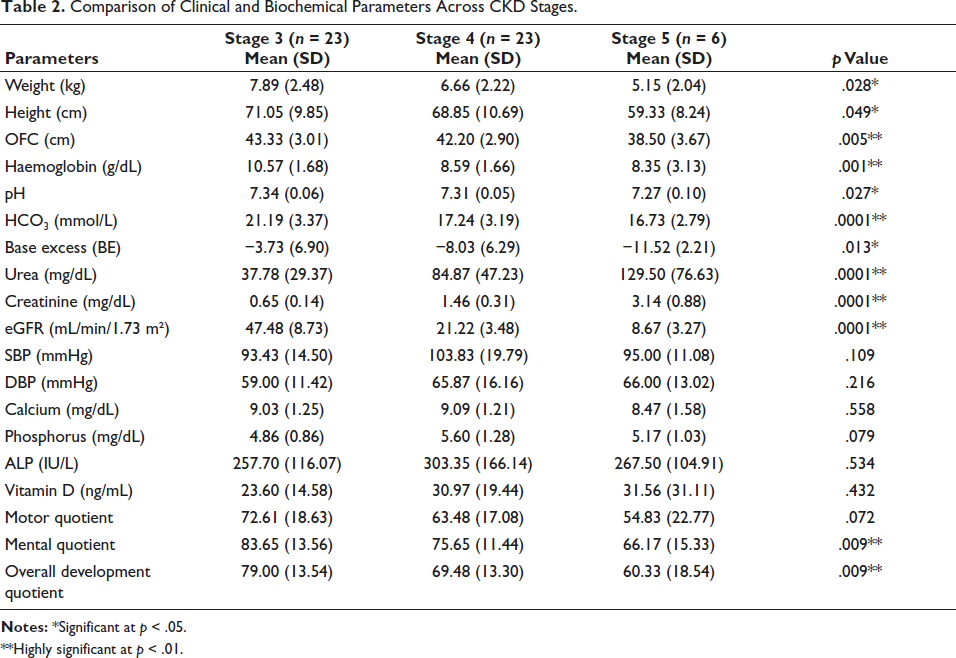
**Highly significant at p < .01.
Multiple comparison for growth (weight, height and OFC), haematological (Hb, MCH and MCHC), biochemical (pH, pCO2, HCO3, BE, urea, creatinine and eGFR) and developmental (MeDQ and overall DQ) parameters as dependent variables were compared across three CKD Stages (3, 4 and 5). Table 3 lists the mean difference between each pair of CKD Stages (I–J) for each dependent variable, as well as its standard error, p value for the comparison, and 95% confidence interval.
Multiple Comparisons of Growth, Haematological, Biochemical and Development Quotient Parameters Across CKD Stages.
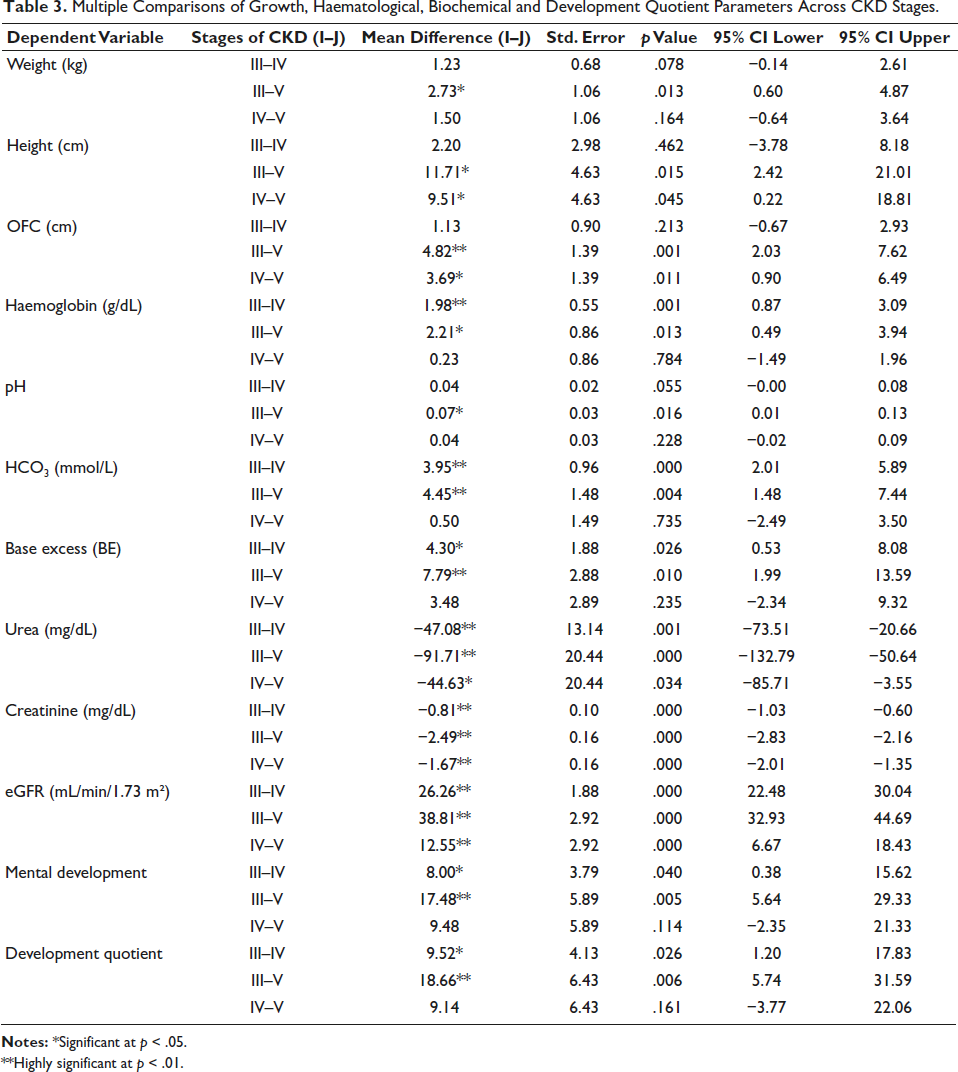
**Highly significant at p < .01.
There is no significant difference in any of the growth measures (weight, height and OFC) between Stages 3 and 4. However, Stage 3 and 5 differ significantly in terms of weight, with a p value of .013. Between Stage 3 and 5, there is a significant mean difference in height with a p value of .015, and between Stage 4 and 5, with a p value of .045. For OFC, there is a significant mean difference with a p value of .001, between Stage 3 and 5, and a difference with a p value of .011, between Stage 4 and 5.
In terms of mental development, Stages 3 and 5 differ significantly with 95% of CI (p = .040, CI 0.38–15.62). Detailed results are presented in Table 3.
Associations Between Clinical Parameters and Neurocognitive Functions
We observed that all three domains of DQ (motor, mental and total) show strong positive associations with weight, height, and head circumference (OFC). Additionally, all domains of DQ (MoDQ, MeDQ and overall DQ) showed a moderate to high positive association with metabolic acidosis and renal function. Besides, PTH indicated an adverse association with mental DQ, while platelet count, urea, and creatinine levels all showed negative relationships with both mental and overall DQ (Table 4).
Significant Association Among Clinical Variables and Developmental Status.
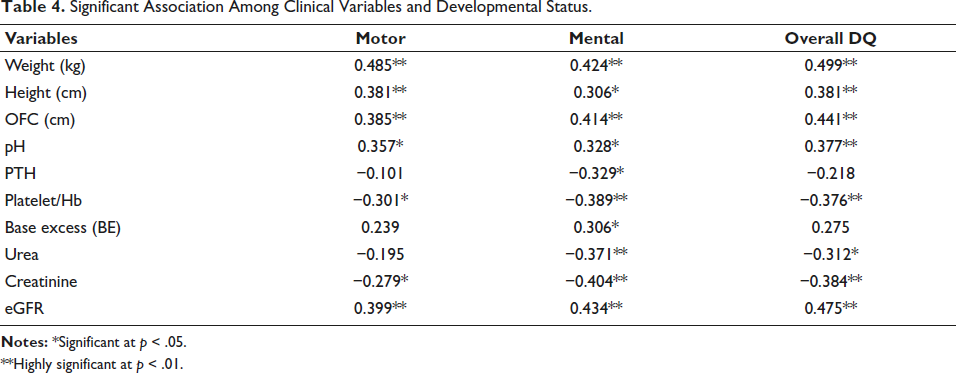
**Highly significant at p < .01.
Discussion
In our cross-sectional case-controlled study, we observed that neurocognitive outcome is worse in children with CKD compared to age and sex matched healthy controls. Further, this outcome is worsened with disease progression and severity. Developmental delay was found in 71% of the cases and was directly related to the stage of CKD. At baseline, when compared to controls, children with CKD Stage 3 to 5 had lower scores across all three domains of MoQ, MeQ and DQ.
Wasting and stunting were present in 27 (52%) and 40 (77%) of the cases. Failure to thrive can be a common presenting symptom in infants and children with CKD, especially if detected late. 13 Growth retardation in children with CKD has been attributed to multifactorial aetiology such as anaemia, poor appetite, metabolic acidosis, renal osteodystrophy and growth hormone resistance. 14
Growth failure in children with CKD has significant consequences and needs appropriate management to improve their development as well as their QOL. The findings from our study reemphasise that the incidence of wasting, stunting and microcephaly is directly proportional to the disease severity. Early implementation of nutritional and psychosocial support in addition to the standard treatment for CKD can improve neurological outcomes in young children with CKD.15–17
The underlying aetiology of CKD in the majority of our cohort was cystic kidney disease, followed by posterior urethral valves. As advanced stages of CKD at a young age was the inclusion criteria, the finding of cystic kidney disease. This was followed closely by posterior urethral valve, which is similar to the NAPRTCS data, where congenital causes were responsible for the majority of CKD in children.18–20
The neurocognitive development of CKD children in our cohort was low in all three domains, that is, MoQ, MeQ and DQ when compared to controls. There was a direct correlation between the uremic milieu and neurocognitive outcomes. The MeQ and DQ were inversely proportional to the stage of CKD. The duration of disease, in addition to the severity of disease, have been found to be associated with lower neurocognitive function in children with ESKD. 7 Low estimated glomerular filtration rate (eGFR) has also been implicated as an important risk factor for poor neurological outcome. 21 The direct toxic effect of the uremic milieu during the early stages of brain development, with a significant impact on neurocognitive delay in children with ESKD, is well documented in the literature.16, 21–23
The factors affecting the neurocognitive impairment in children with CKD are multifactorial. 3 Malnutrition has been implicated to have a direct correlation with low neurocognitive outcomes in children with protein-energy malnutrition (PEM).24, 25
Metabolic acidosis is responsible for poor physical growth in children with CKD. 13 However, its effect on neurocognitive development is not well established. In our study, metabolic acidosis was found in 52% of the cases, and a significant correlation of pH was found with all three domains of neurocognitive development assessed. It is possible that metabolic acidosis not only affects linear growth but also has a role in poor neurocognitive outcomes in children with CKD.
Hypertension is one of the independent risk factors contributing to neurocognitive dysfunction. The Chronic Kidney Disease in Children (CKiD) cohort found that higher blood pressure was independently associated with lower scores on Wechsler Abbreviated Scales of Intelligence (WASI) Performance IQ scores than those with normal BP in children with mild-to-moderate CKD. 26 In our study, 25% of the cases had hypertension, and among them, the majority (43%) of them were in CKD Stage 4. The incidence of hypertension was low in our cohort. This can be explained by the fact that hypertension is predominantly seen in children more than 5 years of age when the cause of CKD is due to glomerulonephritis. 27 We did not find any significant correlation of systolic or diastolic blood pressure with all three domains of neurocognitive function.
The median PTH levels were found to have a significant impact on each stage of CKD, with a negative correlation with MeQ. In infants with renal failure, it was observed that apart from uraemia, hypocalcaemia and hyperparathyroidism were the possible risk factors for poor neurological outcome. 22
Anaemia is another risk factor which has been postulated for poor neurocognitive outcomes in children with CKD. 28 The prevalence of anaemia in our cohort was 75%. However, there was no correlation between anaemia and neurocognitive parameters in our cohort. The CKiD cohort found that in pre-school children aged 12–68 months, lack of anaemia was associated with better neurocognitive outcome. 29
In our study, wasting, stunting, microcephaly, metabolic acidosis and hyperparathyroidism were found to be strongly associated with poor neurocognitive development. However, there was no association found with proteinuria, hypertension and anaemia with neurocognitive impairment in our study.
The strength of our study was that we focused on the neurocognitive aspect in the youngest age group between 3 and 30 months of children with CKD, which is usually the crucial age of brain growth and development. In addition, we use a single validated, time-tested tool to assess neurocognitive outcome.
The study had some limitations. Since it was a pilot study, the sample size was small. We were unable to follow up, and hence, we could not assess the long-term outcomes.
Conclusion
In children with CKD Stage 3 and above, low neurocognitive outcome was documented in all three parameters and with increasing stage of CKD, the mean MoQ, MeQ and DQ worsened when compared to healthy controls. All three parameters of physical growth, namely weight, height and OFC, were found to have an independent effect on the neurocognitive development of CKD children. Metabolic acidosis was found to be inversely proportional to the neurocognitive development in CKD children. Increasing PTH levels were found to correlate with poor MeQ in children with CKD. Early recognition of neurocognitive impairment in children with CKD can improve the QOL as well as school performance, as it is amenable to treatment. Management targeting growth, acidosis and slowing progression of CKD may be necessary to have a good neurocognitive outcome.
Clinical Implications
The results of this study have significant clinical practice ramifications since they highlight the importance of multidisciplinary care teams to handle the complicated physical and neurocognitive needs of children with CKD. Identification and treatment of CKD risk factors such as hydronephrosis, cystic kidney disease, hypertension, malnutrition and other clinical markers may be essential for preventing or postponing the development of CKD and its associated repercussions.
Footnotes
Acknowledgements
Any other identifying information related to the authors and/or their institutions, funders, approval committees, etc., that might compromise anonymity.
Authors’ Contribution
SV: Inception of idea, evaluation, Psychological assessment, writing initial draft, editing and revision of manuscript and final approval.
RS: Inception of idea, evaluation, Psychological assessment, editing and revision of manuscript and critical revision of the manuscript at all stages of production and final approval.
LS: Editing and revision of manuscript and critical revision of the manuscript at all stages of production and final approval
LD: Editing and revision of manuscript and critical revision of the manuscript at all stages of production and final approval
KT: Inception of idea, evaluation, writing initial draft, editing and revision of manuscript and critical revision of the manuscript at all stages of production and final approval.
Data Availability Statement
The data supporting the findings of this study are available upon request and can be obtained from the corresponding author.
Statement of Ethics
Ethical approval was obtained from the Institute Ethics Committee(INT/IEC/2018/000469)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Written informed consent was obtained from the participant for submission of the article to the journal.