
Abstract
Background
Digital technology has rapidly transformed how people communicate, learn, and perform professional activities. While technological advancements have improved access to information, productivity, and global connectivity, excessive reliance on digital devices has raised concerns regarding cognitive and behavioral health. Emerging evidence suggests that prolonged screen exposure, constant multitasking, and dependence on digital aids may contribute to cognitive symptoms resembling dementia, including impaired attention, memory difficulties, reduced problem-solving ability, and emotional disengagement. This phenomenon, often described as “virtual dementia” or “digital dementia,” has become an area of growing scientific and public health interest.
Summary
Current evidence indicates that excessive digital technology use may alter neural circuits involved in cognition, particularly within the prefrontal cortex, hippocampus, and the Default Mode Network. These changes may manifest as digital amnesia, attentional fragmentation, mental fatigue, reduced social engagement, and emotional blunting. Adolescents and young adults appear especially vulnerable due to ongoing neurodevelopment, although many of these changes may be reversible with behavioral modification. Unlike neurodegenerative disorders such as Alzheimer’s disease, virtual dementia is characterized by lifestyle-associated and potentially reversible cognitive dysfunction. At the same time, digital technologies also show therapeutic potential in cognitive monitoring, rehabilitation, and preventive interventions, highlighting their dual role in brain health.
Key Message
Virtual dementia represents a potentially reversible form of technology-associated cognitive impairment driven by maladaptive digital behaviours. Promoting digital hygiene, mindful technology use, cognitive training, and responsible technology policies may help protect cognitive health. Future longitudinal and mechanistic studies are needed to establish diagnostic criteria, clarify long-term neurological effects, and develop evidence-based prevention and intervention strategies.
Introduction
In recent years, the development of digital tools, including smartphones, social media platforms and artificial intelligence technology, has led to a substantial paradigm shift in how we interact with information. These gadgets have undoubtedly improved our lives by providing unprecedented ease, connectivity, speed and efficiency. 1 The introduction of smartphones, for example, has made access to information and communication extremely convenient, allowing us to easily acquire facts, connect with others and complete various tasks with a single tap on a touchscreen. Similarly, social media platforms have transformed the way we communicate and share information, allowing for more global connectivity and community building. Furthermore, AI solutions have automated many operations, improved workflows and increased productivity. 2 The consequences of digital tools on brain function and cognition are a complicated and sophisticated field of study, prompting substantial research by researchers and professionals. As we work to understand the effects of technology on our cognitive capacities, it is becoming increasingly difficult to distinguish between mere correlation and genuine causation due to our ongoing reliance on and use of digital tools. 3
Dementia is a global health problem. As reported by the World Health Organisation (WHO), more than 55 million people lived with dementia globally in 2021. Healthcare professionals and family caregivers must possess both expertise and empathy for individuals living with an illness, as emphasised by international and national legislation and research. 4 Dementia is an umbrella term used to refer to a range of degenerative neurological illnesses that lead to a decrease in cognitive function serious enough to interfere with daily life. 5 Dementia describes symptoms caused by brain injury that impair cognitive skills beyond the boundaries of natural ageing. This disorder impairs emotional regulation, behaviour and motivation while maintaining consciousness. Manfred Spitzer invented the phrase ‘digital dementia,’ referring to the cognitive decline linked with excessive reliance on digital technologies such as cell phones and Google, which may exacerbate attention-deficit hyperactivity disorder (ADHD) or memory loss. 6
The evolution of terminology describing technology-associated cognitive dysfunction, including concepts such as digital dementia and virtual dementia, is summarized in Table 1. The influence of digital media on the growing brain extends beyond motor skills to language and cognition. Excessive digital media usage among young individuals is associated with decreased cognitive empathy, which affects interpersonal understanding and facial recognition. Studies have linked strong reliance on web-based media to diminished white matter integrity, which is critical for language abilities. 7 Adolescents may be more prone to anxiety and false expectations as a result of excessive digital media use. Overuse of digital media has an impact on brain development, particularly cognitive and inhibitory control, attention, memory and reasoning, all of which are required for adaptive behaviour in dynamic situations. Early exposure to fast-paced media can decrease motor skills, spatial awareness, problem-solving abilities and language acquisition. Neuroimaging studies show that environmental influences such as screen time have an effect on brain networks that control social-emotional behaviour and executive functioning.
Emergence of Terms Such as ‘Digital Dementia’ and ‘Virtual Dementia’.
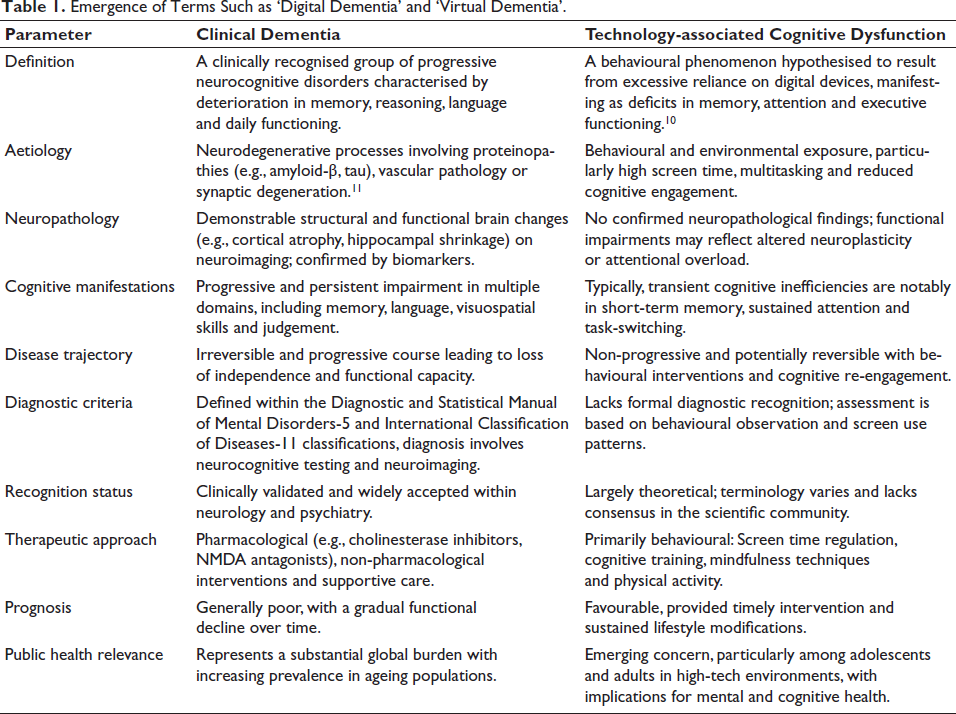
The rapid integration of digital technology into everyday life has given rise to new terminology such as ‘digital dementia’ and ‘virtual dementia’, which reflect growing concerns about the cognitive repercussions of excessive screen time. 12 Digital dementia, a term coined by German neuroscientist Manfred Spitzer in 2012, refers to the impairment of cognitive capacities such as memory and attention as a result of extended use of digital gadgets. The term has gained popularity as research has revealed the neurological and behavioural alterations related to digital multitasking and decreased physical-social connection, notably among adolescents. 13 Meanwhile, virtual dementia is gaining traction in settings where immersive digital environments, such as virtual reality (VR), are utilised to simulate cognitive deterioration for educational or therapeutic purposes. Though not clinically recognised, these phrases serve as metaphors for the changing environment of brain health in the digital age, generating both scientific investigation and popular debate.
Care for people with dementia is difficult and the majority of Alzheimer’s patients are supported in the primary care context, with primary care clinicians accounting for 85% of dementia diagnoses. Above age 65 is projected at 6.9 million and is expected to climb to 13.8 million by 2060, causing a strain for primary care providers and an estimated 11 million unpaid family caregivers. 14 The objective of this review is to examine the emerging concept of virtual dementia in the digital age by exploring how excessive digital dependence, prolonged screen exposure and reduced real-world cognitive engagement may contribute to dementia-like symptoms. It aims to analyse existing research on neurocognitive, psychological and social impacts of digital lifestyles, while also evaluating the dual role of technology as both a potential risk factor and a supportive tool for cognitive health. 15 The scope of the review extends across all age groups, with particular emphasis on adolescents, young adults and the elderly, highlighting the neurological, behavioural and public health dimensions of this growing concern. It further seeks to identify preventive and therapeutic strategies, ranging from lifestyle modifications and digital detox approaches to the integration of VR, AI and cognitive training tools, while also addressing gaps in current knowledge and proposing future directions for research and public health policy.
Understanding Virtual Dementia
Virtual dementia, often referred to as digital dementia, is not a formally recognised medical condition but a growing conceptual framework used to describe cognitive decline and dementia-like symptoms linked to overuse of digital technologies. 10 The term has gained attention in recent years as researchers, neurologists and public health experts observe parallels between excessive reliance on digital devices and impairments in memory, attention span and executive function. Unlike traditional dementia, which is primarily age-related and associated with neurodegenerative processes, virtual dementia highlights the lifestyle-induced risks of the digital era. 15 It reflects the possibility that constant screen exposure, multitasking, reduced physical activity and limited face-to-face social interaction may negatively impact brain regions such as the prefrontal cortex (PFC) and hippocampus, which are critical for memory, learning and emotional regulation. While it remains a debated and evolving concept rather than an established diagnosis, the growing discourse underscores its importance as a public health concern in the context of rapidly advancing digitalisation. 16
Virtual dementia, often termed digital dementia, is not a formally recognised medical condition, yet it is gaining growing attention in neuroscience and public health discourse. The concept describes dementia-like symptoms—such as memory lapses, reduced attention span and impaired cognitive processing—arising from excessive reliance on digital devices and screen-based activities. Although still debated, this emerging framework highlights the potential long-term impact of digital lifestyles on brain health and has sparked increasing concern among researchers, clinicians and policymakers.9, 13
Neurocognitive Effects of Digital Overuse
Attention and Focus
One of the most profound cognitive shifts linked to modern digital media use is the erosion of sustained attention and the rise of fragmented attention patterns. With Generation Z and Millennials engaging in near-constant digital connectivity, multitasking across multiple screens, such as simultaneously texting, streaming videos and browsing social media, has become a normalised mode of interaction. This multiscreen multitasking creates a continuous cycle of attentional disengagement and re-engagement, where each notification, app switch or incoming message triggers a shift in focus. These micro-interruptions gradually condition the brain to expect frequent novelty, lowering the threshold for distraction and diminishing the ability to remain deeply engaged with a single task.17, 18 From a neuroscientific standpoint, sustained attention relies on the coordinated activity of the dorsolateral prefrontal cortex (DLPFC), anterior cingulate cortex (ACC) and parietal attention networks. Excessive multitasking reduces the recruitment efficiency of these regions, as shown by neuroimaging studies that report reduced grey matter density in the anterior cingulate among heavy media multitaskers, weakened functional connectivity between prefrontal control regions and sensory processing areas, leading to slower re-focusing after distraction and impaired working memory performance caused by the cognitive toll of constant task-switching.
In adolescents, whose neural circuits for attention control are still maturing, such patterns may entrench maladaptive attentional habits that persist into adulthood. These effects manifest not only as transient lapses in focus but as cumulative changes: Shallow cognitive processing that favours breadth over depth, reduced tolerance for mental effort and compromised learning efficiency due to poor transfer of information into long-term memory. The prenatal and adolescent stages represent critical windows of heightened neuroplasticity during brain development (depicted in Figure 1).19, 20
Differences between a Healthy Brain and a Brain Affected by Digital Dementia.
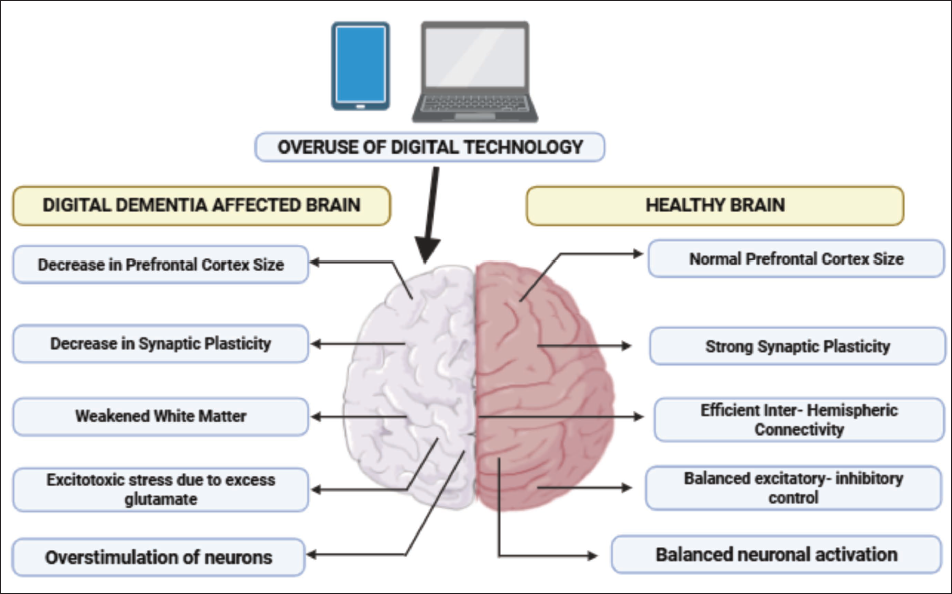
Dynamic brain networks that govern cognition, emotional regulation and executive functioning emerge early in life and become more interconnected during adolescence, with connectivity patterns predicting future cognitive health. Environmental factors such as early exposure to screens, childhood adversity and urban living can influence the maturation of these networks. 21 Research has shown that early television exposure correlates with later attentional deficits, with approximately 10% of children aged one to three displaying such issues by age seven. Among adolescents and young adults, frequent multitasking on digital devices, especially during study, is associated with poorer academic performance, diminished working memory and reduced executive functioning.
Excessive simultaneous engagement with multiple digital platforms, such as messaging while browsing or streaming, further compounds attentional fragmentation by repeatedly forcing the brain into rapid task-switching. This constant reallocation of cognitive resources not only increases mental load but also disrupts the ability to maintain a singular attentional set, fostering a chronic state of distraction. Over time, neural networks responsible for selective attention may become less efficient, undermining the capacity to prioritise relevant information. This shift mirrors features of a ‘virtual dementia’, where the brain adapts to rapid, shallow information sampling at the expense of deep, sustained engagement, ultimately affecting learning, memory retention and real-world task performance.22, 23
Frequent exposure to high-speed, highly stimulating digital environments such as fast-paced social media feeds, algorithm-driven video recommendations and instant messaging gradually conditions the brain to function in a rapid information-scanning mode. Instead of processing material in a slow, linear and deliberate manner, individuals begin to favour quick skimming and frequent content switching. This shift in cognitive processing style reduces attentional dwell time, the span of time the brain remains focused on a single stimulus before disengaging. 24 As a result, even in low-stimulation contexts such as reading a printed book or listening to a lecture, individuals may experience restlessness, mental wandering or a persistent urge to seek novel stimuli. Neurocognitively, shortened attention spans under these conditions are associated with heightened salience network reactivity to novel cues, making distractions disproportionately compelling; reduced activation stability in DLPFC, which undermines sustained, goal-directed attention; and altered dopamine regulation that biases the reward system toward novelty-seeking while eroding patience for slower, more effortful cognitive processing.
Over time, these adaptations create a baseline attentional state that is fragmented and transient, impairing the ability to engage in deep, uninterrupted concentration. 25 The risks are particularly significant during adolescence, a developmental stage marked by extensive synaptic pruning and myelination within attentional control regions. Persistent exposure to fragmented, high-intensity digital input during this period may recalibrate attentional norms toward brevity and novelty, setting long-term cognitive patterns that persist into adulthood. This neural tuning toward rapid, surface-level processing reinforces a preference for easily digestible information while reducing tolerance for slower-paced, cognitively demanding tasks. Consequently, individuals may find it increasingly difficult to sustain mental engagement across academic, professional and creative domains, mirroring early patterns of cognitive decline often described as ‘virtual dementia’.26, 27
Deep, sustained focus, often termed ‘deep work’, refers to the capacity to remain engaged with a single, cognitively demanding task for extended periods while actively filtering out irrelevant stimuli. This ability is supported by the coordinated activation of the PFC, ACC and parietal association areas, which work together to maintain goal-directed attention. At the same time, robust inhibitory control mechanisms suppress competing inputs from the environment, protecting working memory from distraction and preserving the continuity of thought. Persistent digital overuse gradually undermines these neural processes. Habitual interruptions from notifications, message alerts and frequent app-switching train the brain to expect constant novelty, eroding its tolerance for uninterrupted work. The repeated shifting between tasks carries measurable ‘cognitive switching costs’, meaning that every transition delays re-engagement and reduces overall cognitive efficiency.28, 29 Over time, this also weakens inhibitory control circuits, lowering the threshold for attentional disengagement and allowing even minor, irrelevant cues to intrude more easily into the mental workspace.
Behaviourally, these neural changes emerge as difficulty maintaining concentration on complex tasks for more than brief intervals, a growing preference for short, rapidly consumable content over sustained engagement with challenging material and a tendency to abandon tasks prematurely in favour of more immediately rewarding alternatives. Over extended periods, this shift diminishes the brain’s endurance for prolonged mental exertion, producing a form of attentional fatigue that parallels inefficiencies seen in early stages of neurocognitive decline. This has led researchers and commentators to describe the effect as a kind of ‘virtual dementia’ not implying irreversible neurodegeneration, but rather highlighting the functional similarity in how both conditions weaken the ability to sustain focused, high-quality work across academic, professional and creative domains.30–32
Memory Impairment
Digital amnesia refers to the tendency to forget information that is readily accessible through digital devices, a phenomenon that has become increasingly prevalent with the widespread use of smartphones, cloud storage and search engines. In cognitive neuroscience terms, it reflects a shift in how the brain encodes, stores and retrieves information. Normally, memory formation involves deep encoding through attention, elaboration and consolidation, processes that engage the hippocampus and interconnected cortical regions.33, 34 However, when individuals habitually rely on technology to store information, whether it be phone numbers, appointments or facts, there is less need for active rehearsal or retrieval practice. This reduces hippocampal engagement, leading to weaker memory traces and diminished long-term retention. The constant availability of information online promotes a form of ‘transactive memory’, where knowledge is distributed between the individual and the device. While this can be cognitively efficient in the short-term, it fosters dependency on external memory systems. 35 Over-reliance on reminders, notifications and search functions erodes the brain’s capacity for self-initiated recall, encouraging a reactive rather than proactive approach to memory.
Over time, this dependency may impair cognitive flexibility and resilience, as the neural circuits for encoding and retrieval become underutilised. Behaviourally, digital amnesia manifests as difficulty recalling details without device assistance, reduced confidence in one’s memory abilities and a preference for quickly re-searching information rather than committing it to memory. In the context of ‘virtual dementia’, this reliance on digital aids parallels early signs of neurocognitive impairment, where external supports compensate for declining internal memory functions. While digital amnesia is not pathological in itself, its cumulative impact, combined with other effects of digital overuse such as attentional fragmentation, may contribute to measurable cognitive inefficiencies over time. 33
Encoding is the process by which sensory input is transformed into a memory trace stored in neural networks, primarily involving the hippocampus, PFC and associated medial temporal lobe structures. Effective encoding requires sustained attention, deep processing and meaningful association with prior knowledge. Recall, in turn, depends on the reactivation of these memory traces via retrieval cues. Persistent digital overuse, especially in the form of rapid content switching, multitasking and frequent reliance on external information sources, interferes with both encoding and recall. Multitasking fragments attention, reducing the depth of processing and preventing information from being adequately consolidated into long-term memory. Instead of deep semantic encoding, the brain tends toward shallow, surface-level processing, optimised for short-term recognition rather than lasting recall. 36 This is particularly problematic because consolidation, which occurs during offline rest and sleep, is less effective for weakly encoded material.
Moreover, constant access to search engines and reminders fosters ‘cognitive offloading’, where the brain offshifts the responsibility for information storage to external devices. This reduces active retrieval practice, a critical mechanism for strengthening neural pathways associated with recall. Over time, diminished self-initiated retrieval weakens synaptic connections, making recall more effortful and error-prone. Neuroimaging studies have shown that habitual technology users often display reduced hippocampal activation during memory tasks and altered functional connectivity in networks related to attentional control and long-term memory. Behaviourally, this manifests as difficulty recalling details without prompts, a tendency to ‘look it up’ rather than rely on stored knowledge and a decline in confidence regarding one’s own memory abilities. In the broader framework of virtual dementia, these patterns parallel early-stage memory inefficiencies observed in mild cognitive impairment (MCI), though here they are functional and potentially reversible rather than degenerative. 37
The pervasive use of smartphones, wearable devices and digital assistants has introduced a shift in how individuals manage daily tasks, deadlines and personal information. While these tools provide convenience and efficiency, chronic dependence on them can inadvertently diminish intrinsic memory capabilities. This phenomenon is closely related to cognitive offloading, where the brain delegates memory functions such as remembering appointments, to-do lists or important events to external systems. In a healthy cognitive cycle, the PFC coordinates working memory and planning functions, while the hippocampus encodes and retrieves episodic details. Regular engagement in self-reminding and active recall strengthens these neural pathways, promoting long-term retention.38, 39 However, when notifications and reminders consistently take over this role, the brain receives fewer opportunities to engage in proactive retrieval processes. Over time, this reduces the efficiency of both prospective memory (remembering to perform intended actions in the future) and retrospective memory (recalling past events).
Research in the past decade has shown that heavy reliance on external cues can create a form of ‘passive attention’, where individuals respond reactively to prompts rather than engaging in self-directed cognitive planning. This not only impairs the encoding of event-related details—since the memory trace is never deeply processed—but can also erode time-management skills and self-monitoring abilities. Moreover, constant notifications fragment attention, making it harder to transition back into cognitively demanding tasks after interruption, a process known as the resumption lag.
In the framework of virtual dementia, over-reliance on digital reminders is functionally analogous to the use of external aids in early Alzheimer’s disease (AD) or MCI, where patients depend on calendars, sticky notes or voice recorders to compensate for weakened memory. The difference is that in digitally dependent individuals, the impairment is functional and environmentally induced, meaning it is potentially reversible through cognitive training and reduced reliance on external cues. 13
Emotional and Social Cognition
The digital era has replaced many spontaneous, in-person conversations with structured and often shallow digital exchanges such as texts, social media updates and short video clips, which, while efficient, often lack the emotional depth of real-time human interaction. This shift reduces exposure to the rich sensory experiences offered by face-to-face communication, eye contact, subtle facial expressions, body posture, gestures and tone modulation, all of which are vital for accurately interpreting emotions and intentions. Over time, the erosion of non-verbal cue recognition can weaken intuitive social understanding and diminish the ability to build trust and emotional closeness. Furthermore, reduced real-life interaction can foster feelings of isolation, social awkwardness and even anxiety in physical settings. This can create a self-reinforcing loop in which individuals feel more comfortable in curated digital environments, gradually avoiding in-person engagement and potentially impairing the development of long-term social skills and emotional resilience.40, 41
Constant scrolling, instant notifications and exposure to fast-paced content overstimulate the brain’s reward system, reducing tolerance for slower, deeper emotional exchanges and often making individuals more reactive or irritable in real-world interactions. Without regular practice in resolving face-to-face conflicts or interpreting subtle signs of emotional discomfort, emotional resilience may weaken, leading to difficulty in self-regulating during challenging interpersonal situations. Over time, empathy can also suffer, as online communication lacks the physical presence, shared environment and synchronised body language that naturally foster emotional connection. Additionally, the ‘highlight reel’ culture of social media encourages superficial engagement by prioritising image and curated perfection over authentic connection, ultimately diminishing the ability to genuinely understand and relate to others’ lived experiences.42, 43
Mirror neurons are specialised brain cells that activate not only when we perform an action but also when we observe another person performing the same action. They are integral to imitation, emotional understanding and the acquisition of social norms, essentially forming the neurological foundation for empathy and social learning. In early childhood, these neurons are especially active, as children learn by watching and mimicking caregivers, peers and other humans in their environment. However, when screen time dominates a child’s formative years, particularly if their primary ‘interaction’ is with animated characters, digital avatars or fast-changing visual stimuli rather than real human faces, the activation of mirror neurons may become less frequent and less effective. This reduced stimulation can hinder the development of skills that depend on real-time social feedback, such as reading subtle emotional cues, synchronising responses and building rapport. Over the long-term, this may manifest as delayed emotional recognition, diminished empathy, difficulty interpreting others’ intentions and weaker collaborative abilities. These deficits, if not addressed through increased real-world interaction and social engagement, can persist into adolescence and adulthood, potentially affecting personal relationships, workplace dynamics and overall emotional intelligence.44, 45
Brain Structure and Function: What the Research Says
Executive Control and the Prefrontal Cortex
Cross-sectional fMRI in youth with problematic internet/gaming often finds reduced activation and altered connectivity in PFC and cingulate regions during control/decision tasks—consistent with weaker top-down control. Newer reviews integrating social media neuroscience also highlight heightened sensitivity to social reward with immature PFC control, a mismatch that can bias habits toward screen-seeking. 46
Memory Systems and the Hippocampus
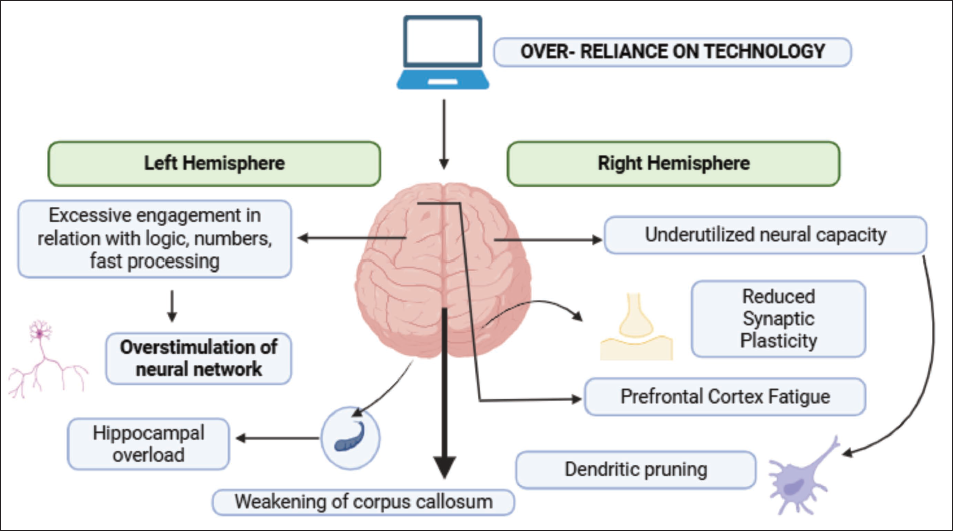
Meta-analytic work in adolescents/young adults with internet addiction reports decreased functional connectivity involving memory and control networks; some studies note resting hyperactivity with task-related hypo-connectivity that can impair encoding/recall. Importantly, large longitudinal cohorts so far show limited macrostructural changes (e.g., no robust global cortical or striatal volume effects over 2–3 years), suggesting functional dysregulation (depicted in Figure 2) may precede or outweigh gross structural change. 47
Structural and Functional Changes in the Brain Affected with Digital Dementia.
Intrinsic Connectivity and the Default Mode Network
Youth with high screen/media use or internet addiction show Default Mode Network (DMN) connectivity disruptions (often stronger DMN coupling with other networks at rest, but weaker task-positive integration), which correlates with mind-wandering and poorer goal-directed focus. Adolescent studies also identify distinct DMN profiles linked to internalising/externalising symptoms, implying DMN is a key vulnerability node during this developmental window. Evidence from adolescent and young adult populations. A 2024 PLOS Mental Health meta-analysis of 10–19-year-olds with internet addiction found network-wide functional alterations, especially in executive control and memory-related systems. Broad reviews and ABIDE/ABCD-style cohort papers converge on: Functional (connectivity/activation) changes in youth are common; structural changes are smaller/inconsistent at the population level over short follow-ups. 48
Reward Systems and Dopaminergic Circuitry
Behavioural addiction and internet addiction syntheses show altered reward processing (ventral striatum, orbitofrontal cortex), with reports of reduced striatal dopamine transporter availability and reward-cue hypersensitivity, a pattern that promotes cue-driven seeking and habit formation. In adolescents, this reward-control imbalance (strong mesolimbic drive, still maturing PFC) likely amplifies compulsive digital use and makes disengagement harder. The most consistent signals in youth are functional: Disrupted PFC control, DMN dysconnectivity and reward-circuit bias, a triad that can mimic ‘virtual dementia’ complaints (inattention, forgetfulness, executive lapses) without clear, uniform gross atrophy. Longitudinal cohorts caution against overclaiming structural harm, but they do not negate functional risks during sensitive developmental periods. 49
Risk Populations
Certain populations are especially vulnerable to ‘virtual dementia’-like effects of excessive digital media use because of the way their brains are developing or functioning. Adolescents (12–19 years) face the greatest risk since the PFC, which governs executive control, planning and inhibition, is still maturing. At the same time, their dopaminergic reward circuitry (ventral striatum, nucleus accumbens) is hyper-responsive, creating an imbalance that fuels impulsivity and compulsive engagement with digital platforms. 50 Young adults (20–25 years) remain susceptible because brain connectivity is still stabilising, particularly between the PFC and the DMN, making them prone to distraction and multitasking inefficiency in academic and social contexts. Children under 12 years are vulnerable due to the rapid development of the hippocampus and executive networks; heavy reliance on screens during this phase can interfere with memory consolidation and language learning, while also altering white matter integrity in attention pathways.
In addition to age-based groups, individuals with pre-existing vulnerabilities such as ADHD, anxiety, depression or learning disorders show heightened sensitivity, since their fronto-striatal circuits (responsible for attention and control) and DMN regulation are already atypical; digital overstimulation exacerbates these deficits. 51 Heavy gamers and social media users exhibit overactivation of the reward circuitry (ventral striatum, orbitofrontal cortex) and reduced dopamine transporter availability, reinforcing compulsive checking and craving behaviours. Among adults under high cognitive load—such as students, knowledge workers and caregivers—excessive multitasking weakens PFC function and disrupts hippocampal-dependent encoding, producing forgetfulness and disorganisation similar to early cognitive decline. Final, although less studied, the elderly may also be at risk; reliance on external reminders may reduce hippocampal engagement, potentially accelerating cognitive offloading in those with MCI.52, 53
In summary, children, adolescents and young adults are the highest-risk groups, with vulnerabilities linked to developmental changes in the PFC, hippocampus, DMN and reward pathways, while adults with cognitive vulnerabilities or high digital exposure show functional patterns that mimic dementia-like symptoms.
Comparison with Clinical Dementia
While ‘virtual dementia’ shares some functional similarities with clinical dementias such as AD, the underlying mechanisms differ substantially. In clinical dementia, especially in AD, Alzheimer’s, there is progressive neurodegeneration characterised by amyloid-β plaques, tau tangles, neuronal loss and hippocampal atrophy. 54 These structural changes lead to irreversible deficits in episodic memory, executive function and orientation, ultimately impairing daily functioning. In contrast, virtual dementia does not involve widespread cell death but rather reflects maladaptive neuroplasticity and functional dysregulation caused by chronic digital overstimulation. For instance, adolescents and young adults with heavy digital use often show reduced PFC activation, hippocampal dysconnectivity and DMN hyperactivity, which resemble the attentional lapses, forgetfulness and planning difficulties observed in early dementia. However, these changes are generally functional and potentially reversible, as shown by neuroimaging studies indicating partial recovery after digital detox or controlled use. 55
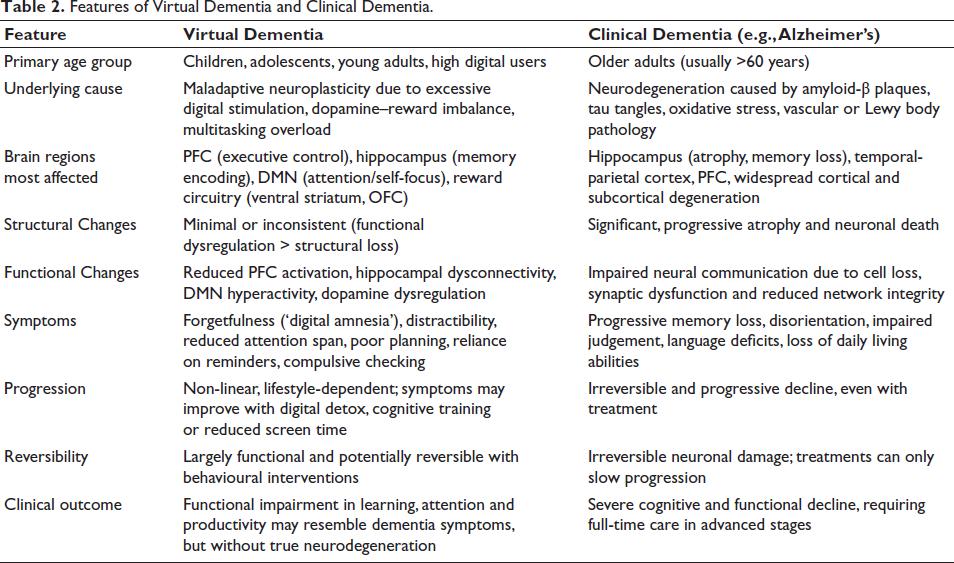
Another key distinction lies in progression. Clinical dementia worsens steadily and irreversibly over time, while virtual dementia-like symptoms may fluctuate depending on lifestyle, screen exposure and cognitive training. Moreover, clinical dementia affects older adults, whereas virtual dementia is most evident in children, adolescents and young adults, reflecting the vulnerability of developing brain circuits. Both conditions implicate the hippocampus (memory), PFC (executive control) and network-level changes in the DMN, but the root cause differs: Neurodegeneration in clinical dementia versus behavioural overuse and reward-circuit imbalance in virtual dementia. 56 A comparative overview of the clinical and neurocognitive features of virtual dementia and disorders such as Alzheimer’s disease is presented in Table 2.
Features of Virtual Dementia and Clinical Dementia.
Public Health Implications
There has been a rising dependency on digital technology, social media and screen-based activities, thus leading to growing concerns about their implications on the general public’s health across all age groups. Although digital technologies are a part of daily routine and have made lives convenient, their uncontrolled use has turned out to be a bane. As a result, virtual dementia is now an evident issue of this overexposure to digital activities. It significantly comprises neurodevelopmental and psychosocial-related cognitive impairments. 34 It is estimated that about 4.8 billion people use social media and about 210 million are termed to be dangerously addicted to social media. 57 Additionally, 36% of them are critically addicted to the internet. 58 Over-reliance on devices is leading to minimised or zero personal interaction and strong dependency on digital platforms. The negative effects include reduced focusing, disturbed mental clarity, impaired attention and memory retention, thus resulting in mental strain and altered thought process. Over time, this can lead to symptoms resembling those of dementia. 58 As per the 2024 report by the WHO, the usage of social media rose from 7% (in 2018) to 11% (in 2022) in Europe; about 12% of teenagers were found to be affected by gaming risks. 59
A 2024 report by State of Emotional Well-being highlighted that only 3% of employees manage to strike a digital life-work balance. 60 Studies have revealed that excessive use of social media and virtual platforms is linked with disturbed sleep cycle, depression, anxiety and other mental health issues in youth. 61 The extent of changes in the brain is marked in children due to their neural plasticity, making them more vulnerable to the harmful effects of digital overuse. 62 Continuous engagement in counterproductive digital activities may cause cognitive fatigue. Altered circadian rhythm, reduced physical activity and sedentary routine associated with excess digital use can affect the physiology and mental health drastically. Individuals tend to withdraw from real-time situations as they lack willpower, search for constant social validation and superficial engagement. The behavioural shift can be detrimental to the academic, occupational and social skills. 58 It could potentially lead to Alzheimer’s disease and related dementias over time; by 2060, these conditions could increase by up to 4–6 times. 63
Currently, there is a need for awareness and interventions to promote mindful digital media usage. Early interventions should be implemented during the initial years of childhood. There is a need for structured and integrated digital wellness modules to be implemented in academic curricula and workplaces. These programmes should create awareness about the ill effects of excessive digital activities. It should ensure the digital well-being of the students and employees, such that mental fatigue and digital burnout are prevented. Many key tech giants, such as Google and Apple, have incorporated digital wellness tools in their workplaces. This step has proven to be beneficial as part of the corporate wellness market. It covers access to telemedicine and virtual healthcare facilities at an affordable cost. It has improved the employees’ productivity, maximised the return on investment and ensured better employee retention.64, 65
Prevention and Intervention Strategies
Digital Hygiene Practices
Digital hygiene refers to a systematic approach in the utilisation and management of digital technology to maintain an optimal state of mental and emotional well-being. It can be considered a conscious step taken towards the prevention of virtual dementia and associated cognitive dysfunction. It consists of measures such as regulation of screen time, management of notifications, creation of tech-free zones/time and being mindful about the consumption of online content. There must be necessary measures to track the duration of screen time. Restriction of mobile or laptop usage an hour before bedtime should be followed rigorously. Initiatives such as digital detox can be employed during weekends or on holidays. Digital detox activities include minimal or no use of devices, practising mindful screen use, engaging in physical exercise, yoga, reading printed books and spending time in nature and with family. 66 These activities help in imbuing qualities such as self-confidence, willpower, stronger family bonds, digital literacy, parental guidance and mediation and a positive mindset in adolescents. These traits help them to go through digital spaces safely, thereby reducing psychological issues and harmful online behaviour. 59
Educational and Cognitive Interventions
Cognitive training and educational practices aimed at building attention, memory and mindfulness can serve as countermeasures to digital-induced cognitive decline. 67 Activities such as reading, solving puzzles, playing musical instruments and participating in physical activities stimulate different areas of the brain. 68 In schools and colleges, integrating digital wellness modules and encouraging sessions such as attention training, mindfulness sessions and meditation practices have also shown efficacy in reducing mental stress and improving focus. A study reported the positive impacts of digital app-based mindfulness therapy on students’ mental health. 69 A study showed that digital cognitive training could be adopted to prevent cognitive decline in hypertensive older adults, thus improving memory, mood and brain structure through adaptive exercises. Digital cognitive assessment platforms such as BrainCheck can aid in the early detection of subtle cognitive decline through structured, gamified tests that evaluate memory, executive function, attention and reaction time. These tools offer scalable, remote options for continuous monitoring of cognitive health in digitally exposed populations. 70 Digital screening tools such as MoCA Duo and digiDEM-SCREEN enable early detection and remote monitoring of cognitive decline. They improve access to care, especially in rural areas, support caregivers and aid research. 71
Role of Policy and Awareness
Policy-level interventions are key tools to create an environment that fosters responsible and timely digital use. The European Union’s Digital Competence Framework and DigCompEdu promote digital well-being by ensuring safe and inclusive digital environments and responsible digital use across Europe. 72 There is a need for a well-defined policy for digital wellness in our country. In India, 60% of children aged 9–17 spend over three hours daily on social media or gaming. WHO estimates 15% of adolescents face mental disorders, with excessive screen time linked to anxiety, depression and learning issues. 73 Governments and educational institutions should implement guidelines on screen exposure, especially for children under the age of five, with not more than one hour of screen time, as recommended by the WHO. 74 Digital literacy programmes, parental control tools, can educate families about the risks of unregulated digital usage and promote healthy digital behaviours. Workplaces should adopt digital wellness policies that encourage employees to take periodic breaks and avoid digital burnout. There is a need to implement the ‘Right to Disconnect’ in India to protect employees from work-related demands beyond their working hours. 75
Research Gaps and Future Directions
There is a need for longitudinal and cross-cultural studies to understand the cognitive decline in the population over a long period of time. Robust longitudinal studies are useful in determining and establishing the factors, mechanisms, adverse effects and changes induced in humans as digital dementia evolves. Cross-cultural studies are required to understand the relationship between the social, technological or economic background and the extent of digital overuse and their subsequential effect on mental health. Several studies have reported mixed results; digital overuse is directly associated with cognitive decline in youth, whereas digital use is linked with cognitive improvement in the older population. Thus, age is a critical determinant in understanding the effects of digital use on brain activity, the extent of changes in cognitive abilities, and associated neurological activities. 3
A major research gap lies in the area of standardised diagnostic tools to assess digital-related cognitive impairment symptoms. The global market size of MCI was estimated to be about USD 2.2 billion in 2024 and could cross the USD 4 billion mark by the end of 2037. 76 As of now, virtual dementia is clinically not diagnosable. Advanced diagnostic tools are crucial to assess digital-related cognitive symptoms and can be applied to virtual dementia. Relationship between existing biomarkers and pathophysiology can be employed to map the possible changes occurring in case of neurological alterations in case of virtual dementia. Changes in biomarkers such as cortisol or neuroinflammatory agents can indicate the changes induced by prolonged digital exposure. 77
Simultaneously, the emergence of digital therapeutics opens new avenues for intervention. Digital therapeutics refer to health software-based treatments designed to prevent, manage or treat cognitive impairments. 78 They include interactive tasks, behavioural therapy modules and neurofeedback-based systems to enhance cognitive resilience. FDA-approved digital therapeutics are available as Software as a Medical Device. 79 These platforms in clinical and educational settings can minimise the impact of digital overuse on brain function.
Conclusion
This review has explored the emerging concept of virtual dementia associated with overuse of digital technologies and exposure to online media. It is a growing concern in public health, particularly among adolescents and requires consideration for formal clinical characterisation in future research. The digital overuse affects attention, memory, emotional and social cognition; thus alters the brain structure and functions. These cognitive disruptions are prominent in the young population. Although digital dementia is distinct from clinical dementia, they share similar features. The public health implications are significant, with increased cognitive and mental health burdens caused by a lack of awareness and inadequate institutional policies. Despite growing interest, research gaps exist in standardised diagnostic interventions and preventive measures. A conscious and collective effort, from individuals and institutions, is required to protect cognitive health and mental well-being, along with the regulation of digital technology usage.
Footnotes
Abbreviations
ADHD: Attention-deficit hyperactivity disorder
ICD-11: International Classification of Diseases-11
DSM5: Diagnostic and Statistical Manual of Mental Disorders-5
VR: Virtual reality
DLPFC: Dorsolateral prefrontal cortex
ACC: Anterior cingulate cortex
MCI: Mild cognitive impairment
AD: Alzheimer’s disease
PFC: Prefrontal cortex
DMN: Default Mode Network
ADRD: Alzheimer’s disease and related dementias
SaMD: Software as Medical Device
AI: Artificial Intelligence
NMDA: N-methyl D-aspartate receptor
fMRI: functional magnetic resonance imaging
PLOS: Public library of science
FDA: Food and Drug Administration
Acknowledgement
All the authors of this manuscript are thankful to their respective departments and universities for the successful completion of this study.
Authors’ Contribution
All authors contributed to the study’s conception and design. All authors read and approved the final manuscript.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Patient consent was not required as no human participants were involved in this study.
Statement of Ethics
No ethical approval was required for this review, as it does not report any original research involving humans or animals.