
Abstract
Background
Vaccination against COVID-19 infection became mandatory because of the field situation during the pandemic.
Purpose
Vaccine efficacy and safety need many field years of study; time constraints due to the pandemic limited the same. A hospital-based study was done in South India among patients who presented with immune-mediated disorders in temporal correlation with COVID-19 vaccination.
Methods
The study period was 20 months, from March 2020 to November 2021. There were a total of 3,235 patients with neurological issues seen in two tertiary institutions, catering predominantly to patients from lower socio-economic strata in South India. A total of 1,007 (31.12%) patients had received COVID-19 vaccination (single dose in 511 [50.7%] and both doses in 496 [49.3%]). The general prevalence of primary demyelinating disease was compared with the background of vaccine-induced demyelination. Chi-square test was utilised for determining the association between neurological sequelae and the type of vaccine administered.
Results
Eighteen patients had neurological sequelae, and 16 had a monophasic pattern. Recurrent autoimmunity was seen in two patients who took the Sputnik vaccine. Comparing the prevalence of primary multiple sclerosis (MS) versus vaccine-induced demyelination, there was a statistically significant difference (χ2 = 572.38; p < .001), which indicates a definite role of vaccination in these patients. The association between neurological manifestations of Covishield and Covaxin showed no statistically significant difference in neurological sequelae (χ2 = 0.0466; p = .8). The Sputnik vaccine was not considered, as the number was less than five. Anti-myelin oligodendrocyte glycoprotein-associated recurrent optic neuritis was seen in one patient, and tongue atrophy, pyramidal signs, ulcerative colitis and arthritis after 3 months, and C-ANCA positivity were seen following the Sputnik vaccine in one patient.
Conclusion
Vaccination is an effective public health intervention. However, in susceptible individuals, it can probably trigger a recurrent and multisystem event by immune dysregulation. The association is an observation-based postulate that needs a longer, larger follow-up. As per this study, it is non-fatal and remits permanently.
Introduction
By the end of 2019, the world faced the COVID-19 pandemic. The rapid development and global distribution of vaccines against SARS-CoV-2 were extraordinary public health activities, which significantly reduced the severity and mortality of coronavirus disease 2019 (COVID-19). 1 However, the unprecedented scale of this vaccination campaign has facilitated the detection of rare vaccine-related adverse events that were not detected in initial clinical trials. Post-market surveillance has documented a range of new-onset and relapsing autoimmune and autoinflammatory conditions temporally associated with vaccination, with a median time to onset of approximately 8 days after immunisation, 2 among which neurological sequelae have been identified as an important but rare potential adverse event that warrants careful pharmacovigilance. These include various central nervous system (CNS) disorders, such as transverse myelitis, acute disseminated encephalomyelitis (ADEM) and autoimmune encephalitis, as well as peripheral nervous system (PNS) involvement, with Guillain–Barré syndrome (GBS) being a common example; the pathophysiology is thought to involve an aberrant immune response in susceptible individuals due to mechanisms such as molecular mimicry between viral spike protein and neural antigens or non-specific bystander activation of autoreactive lymphocytes in a pro-inflammatory environment. 2 As global data are accumulating, the incidence, clinical phenotype, and risk factors for these sequelae remain poorly defined within this genetically and environmentally distinct Indian population, with India’s mass vaccination programme having used an adenovirus-vectored ChAdOx1-S/nCoV-19 vaccine (Covishield), which is associated internationally with specific neuro-immune events. 3 It has long been recognised that vaccines can trigger exacerbation of immune-mediated inflammatory disorders.4, 5 With these aspects in mind, we attempted to study the sequelae following the COVID-19 vaccination among people who presented to a tertiary care centre in South India.
We aim to study patients who presented with features of immune-mediated disorders after COVID-19 vaccination in two private tertiary hospitals (one a charitable hospital and the other a corporate one). Vaccines were developed using mRNA, and there were both viral vector vaccines and inactivated viral vaccines. 6 It is well known that immune-mediated inflammatory disorders carry a risk of exacerbation with vaccines. 7 Moreover, the efficacy of the vaccine itself can be altered in patients with co-existing immune-mediated disorders due to the disease, as well as the treatments the patient may be taking. 8 Pro-inflammatory and anti-inflammatory cytokines play a vital role in these responses. There is increased immune activation by mRNA vaccines due to pro-inflammatory cytokines. 9 Disease exacerbations are therefore expected with mRNA vaccines.
Patients and Methods
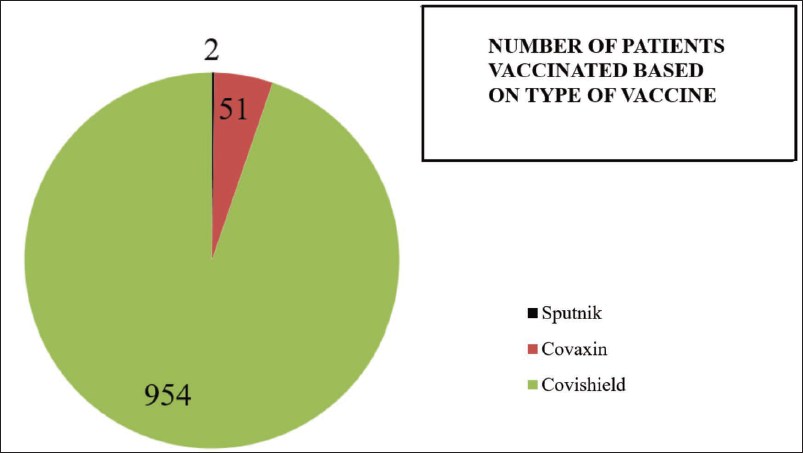
This is an observational descriptive study. Patients were recruited from among patients who had reported vaccination and, in varying periods after that, developed neurological complications in the absence of any other past illness. In the study period of 20 months, from March 2020 to November 2021, patients were evaluated in two tertiary centres in Thiruvananthapuram, Kerala state, catering to patients primarily belonging to lower socioeconomic strata. A total of 1,007 patients had taken the COVID-19 vaccine. It was observed that 511 (50.7%) patients had taken only a single dose and 496 (49.3%) had taken both doses. Two patients took the Sputnik vaccine, 51 patients took Covaxin, and all others took the Covishield vaccine (Figure 1). Those who had developed neurological sequelae following COVID-19 vaccination were evaluated in detail to identify the pattern of neurological illness, and appropriate treatment was initiated.
Distribution of Vaccine Taken is Depicted in the Pie Diagram.
Chi-square test was utilised for determining the association between neurological sequelae and the type of vaccine administered. Data were compared between Covaxin and Covishield vaccines, as only two patients had taken Sputnik. The patients were followed up by a single neurologist.
Results
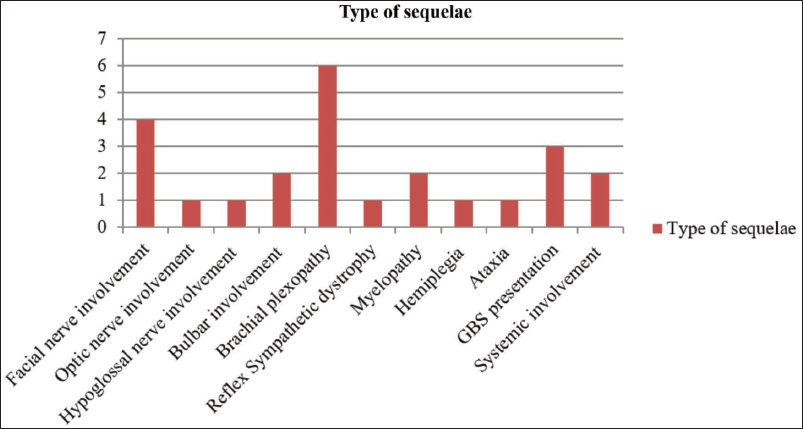
Out of 1,007 patients, 18 patients developed neurological sequelae, and 16 had a monophasic pattern of illness following vaccination, whereas a recurrent pattern of neurological illness was seen in only 2 patients (Figure 2). The various types of neurological sequelae observed post vaccination is depicted in Figure 2.
Bar Diagram Depicting the Distribution of the Following Neurological Sequelae in Patients Following Vaccination.
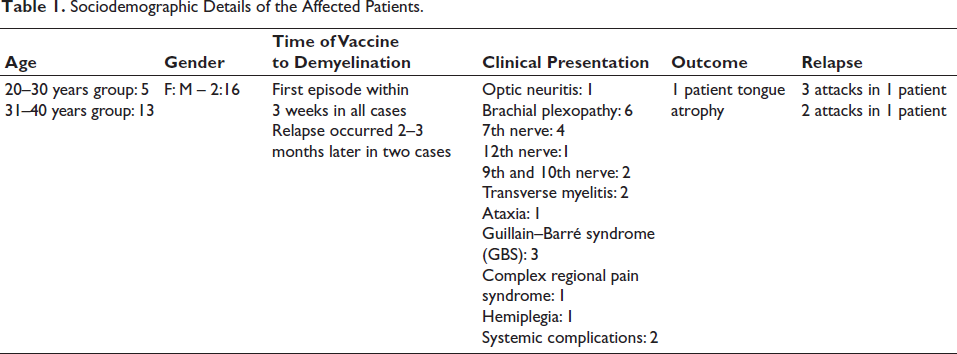
The majority of the patients in our study belonged to the 30–40 years age group, were male and had a predominantly acute presentation of neurological sequelae (Table 1). All the patients were treated with pulse methylprednisolone, 1 g in glucose saline for 5 days, with supportive measures and physiotherapy, followed by oral steroids tapered slowly over 3 months. The two patients who had recurrence were treated as follows. The patient who developed myelin oligodendrocyte glycoprotein (MOG)-positive optic neuritis was treated with a second parenteral pulse of methylprednisolone for 5 days and then shifted to oral steroids. The patient who had ulcerative colitis received oral steroids, 1 mg/kg, as advised by the gastroenterologist, and these were tapered off over 3 months. None in this group needed immunoglobulin or plasma exchange.
Sociodemographic Details of the Affected Patients.
Both subjects who took the Sputnik vaccine developed neurological sequelae. However, as the number of those who took the Sputnik vaccine was very small (<5), the association between vaccines and neurological deficits could not be analysed. Comparing the prevalence of primary multiple sclerosis (MS) versus vaccine-induced demyelination, there was a statistically significant difference (χ2 = 572.38; p < .001) in vaccinated patients. The association between neurological manifestations and indigenous vaccines (Covishield and Covaxin) was checked, and there was no significant association of neurological sequelae between these two vaccines (χ2 = 0.0466; p = .8). The vaccines did not differ in their risk of neurological sequelae.
MS has a prevalence of 35.9/100,000 people, a pooled incidence rate of 2.1/100,000 persons across data sets available from 75 countries, and a mean age of diagnosis of 32 years. MS affects women twice as frequently as it affects men. 10 However, in our study, out of 1,007 patients who received the vaccine, 18 had demyelination, and males dominated.
Anti-MOG associated CNS involvement was seen as a sequela in one patient, and another patient had associated C-ANCA positivity. One patient who died following a road traffic accident had recurrent myelitis following Covishield, and another one was lost to follow-up; hence, they were excluded from follow-up data. In our group of patients who had taken the vaccine, only two patients had taken the Sputnik vaccine. Both had recurrent demyelination. All other 16 patients had a monophasic illness with a single episode (Figure 2).
Discussion
This observational study of people who developed demyelination of the nervous system, as well as immunological problems of other systems in previously normal individuals, indicates that a small percentage of patients do develop complications after vaccination. However, unlike the other conditions associated with demyelination, these patients had a maximum of two relapses and no further relapses in the last 4 years. There were no fatal complications in this group of patients. With reference to individual vaccines, as there were very few patients in each category of vaccines, it is difficult to draw any conclusion.
It is well known that vaccines can trigger demyelination in some persons. Immune dysregulation is a situation in which the immune system is overactive, underactive or abnormally active, causing autoimmunity. Autoimmunity is usually triggered by known antibody formation with or without association with malignancy, vaccines or infections. It also occurs possibly due to unknown antibodies that trigger immune reactions due to molecular mimicry and biological misidentification, causing a variety of neurological manifestations, as per literature, after varying periods of different triggers, from a few days to several weeks. Recurrent demyelination is typically seen in association with conditions such as vasculitis, MS and rheumatoid arthritis, as the abnormal regulation is persistent. With vaccines, it is mostly monophasic. Associated factors are major histocompatibility complex (MHC), immunoglobulin heavy chain, T-cell antigen receptor and myelin basic protein loci.
In this study of COVID-19 vaccine-associated demyelination, none had any previous illness of relevance, and three of our patients showed recurrent demyelination, of which two involved the nervous system and one developed systemic autoimmune disease with P-ANCA positivity (Figure 2). He had taken the Sputnik vaccine. Now, after 4 years of follow-up, no further problems were seen in any of these patients, including those who had relapse. One patient was MOG positive, and the patient who had a trigger of systemic autoimmunity with P- ANCA positivity is not reported in the literature. However, there is no persistence of this immune dysregulation in any of these patients, indicating that the dysregulation is temporary and restricted to a small number of persons. Even persons who have recurrence have a good prognosis, unlike those with primary immune dysregulation syndromes. Vaccine-associated demyelination appears to have a varied prevalence and pattern and a gender difference, with male dominance in this study. Studies have also reported that among Asians, 3.3% had an acute neurological event following vaccination, and also only 2% of the individuals vaccinated in Singapore had a recurrence of their neurological symptoms after revaccinations, further showing the relative safety of vaccines.11, 12
With reference to MS, the pooled incidence rate across 75 reporting countries is 2.1 per 100,000 persons/year, and the mean age of diagnosis is 32 years. Females are affected twice than the males. 10 However, in this study, males dominated.
Few Case Reports of Patients with Neurological Sequelae
Patient 1
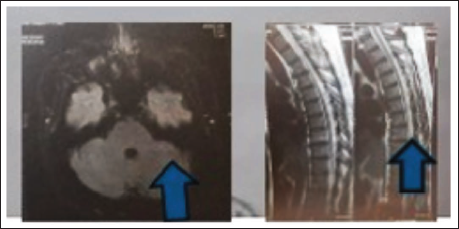
A 34-year-old Ayurvedic doctor working in Dubai took his first dose of the Sputnik vaccine on 8 July 2021 and had no complications. The second dose was taken on 21 July, and this was followed by high fever and body pain for 1 day. Two weeks after this, he developed a tingling sensation in his chest and was evaluated for heart disease. Then it extended to the neck, and he had a girdle sensation and numbness below the neck. By the first week of October, the symptoms worsened, he developed slurred speech and swallowing difficulty, and was he suspected to have motor neuron disease. Examination revealed left 7th, 10th, 11th and 12th nerve palsies with tongue fasciculations and atrophy (Video 1 in the supplementary material). He had bilateral pyramidal signs, and posterior column and cerebellar signs. His antinuclear antibody (ANA) profile, screening for malignancy and positron emission tomography-computed tomography (PET-CT) were negative. His magnetic resonance imaging (MRI) showed signal changes in the middle cerebellar peduncle and dorsal root sleeves (Figure 3). Cerebrospinal fluid (CSF) showed 11 cells, all lymphocytes. Infection markers were negative, which included TB GeneXpert, oligoclonal bands (OCBs), anti-aquaporin 4 antibody and anti-MOG. This patient had asymmetrical cranial nerve palsy, tongue atrophy with fasciculations on the right side and also had motor and sensory involvement of the spinal cord due to which motor neuron disease was considered unlikely. Demyelination was considered, and with treatment, he recovered except for tongue wasting. Later, while on tapering steroids, around 50 days after the pulse, while on 4 mg of methylprednisolone, he developed severe abdominal pain and blood in stools, and biopsy showed eosinophilic enterocolitis, and blood evaluation showed P-ANCA positivity. Steroids were increased again by the gastroenterologist. Steroids were tapered very slowly over 3 months, and the patient became symptom-free.
Signal Changes in the Middle Cerebellar Peduncle and Dorsal Root Sleeves (Magnetic Resonance Imaging [MRI] Images Enclosed with Arrows).
Patient 2
A medical student took Covishield and developed optic neuritis in the right eye 2 weeks after vaccination. His CSF showed anti-MOG antibody positivity. Other markers were negative. He was treated with parenteral steroids and recovered fully. Two months later, there was a recurrence in the left eye, but it improved completely and had no other neuraxial involvement or systemic complications. He also suffered a third relapse of optic neuritis a month later, with complete recovery.
Other Manifestations
A 45-year-old male developed transverse myelitis within a week of his first dose of the Covishield vaccine. His blood and CSF did not yield any antibody positivity. He improved partially with treatment at the end of 5 days and could walk without support but was slow and spastic. Unfortunately, this particular patient passed away on the day of discharge in a road accident, and we did not include him in this study.
Among the remaining 16 patients, the manifestations were as follows: optic nerve involvement in one, hypoglossal nerve involvement in two, bulbar palsy in two patients, brachial plexopathy in six, hemiplegia in one patient, reflex sympathetic dystrophy in one, myelopathy in two patients, ataxia in one, GBS in three patients and systemic involvement in one patient (Figure 2).
Three of our patients showed recurrent demyelination, two involving the nervous system and one involving eosinophilic enterocolitis with P-ANCA positivity. He had taken the Sputnik vaccine. Now, after 4 years of follow-up, no further problems were seen in any of these patients, including those who had cyclical relapses. The other patient was MOG positive. Anti-MOG associated recurrent optic neuritis and C-ANCA positive systemic auto immune disease are not so far reported in literature in this context. However, there was no persistence of this immune dysregulation in any of these patients, indicating that the dysregulation was temporary and restricted to a small number of persons. This is seen with all vaccines, and even persons who had recurrence have a good prognosis, unlike those with primary immune dysregulation syndromes.
The strengths of this study involve a large number of patients presenting to a tertiary centre in India, being evaluated and followed up by a single neurology team, and detailed evaluation of the pattern, progression and resolution of the neurological sequelae. The limitations include the absence of a control group of unvaccinated patients with demyelination and the descriptive nature of the study. We did not screen for asymptomatic predisposition to primary demyelinating disorders.
Conclusion
This observational study indicates that immune dysregulation can be triggered by COVID-19 vaccines. Mostly, they are non-fatal. They can be both neurological and non-neurological. The underlying pathological mechanisms need further study. Larger studies will give more insight into these observations. Vaccination is one of the most effective public health interventions, successfully controlling many serious infectious diseases and saving millions of lives globally each year. As all these patients were previously normal and symptoms were time-bound to vaccination, it is likely that, in susceptible individuals, it can probably trigger even a recurrent autoimmune syndrome. None of our patients needed intravenous immunoglobulin or plasmapheresis. None of our patients went on to have a regularly relapsing or progressive course unlike primary demyelinating diseases. There was no fatality in this series.
Footnotes
Acknowledgement
The authors acknowledge with gratitude the patients and their caregivers, who cooperated with the study, the hospital management and the Ethics Committee for facilitating and encouraging the study.
Authors’ Contribution
VA and SRC were associated with conception, design, acquisition, analysis, interpretation and final approval, TGI was associated with acquisition. Analysis and interpretation associated with acquisition. SRC (CA) is accountable for all aspects of the work.
Data Availability Statement
The data sets generated and/or analysed during the current study are not publicly available to ensure the privacy of the study participants. Data requests can be directed to the corresponding author, SRC.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Voluntary informed consent was obtained from all the participants.
Statement of Ethics
The study was approved by the Institutional Ethics Committee (IEC).
Supplementary Material
Supplementary material for this article is available online.