
Abstract
Background
The COVID-19 pandemic has resulted in a significant increase in mental health issues, including depression, anxiety, post-traumatic stress disorder and sleep disturbances, particularly among recently hospitalised patients. Non-pharmacological interventions such as Yoga Nidra and Music Therapy offer cost-effective and accessible alternatives for improving psychological well-being and sleep quality in this population.
Purpose
This study aimed to investigate the effects of Yoga Nidra and Music Therapy on sleep quality, mental health and overall well-being among recently recovered, hospitalised COVID-19 patients.
Methods
This three-arm, parallel-group, randomised controlled trial (RCT) enrolled 90 adults recently discharged following COVID-19 hospitalisation. Participants were randomised in a 1:1:1 ratio into Yoga Nidra, Music Therapy or standard care groups. Both interventions were delivered online via Zoom for 30 min daily over 30 days. Sleep quality, mental health and well-being were assessed using the Pittsburgh Sleep Quality Index (PSQI), the Patient-Reported Outcomes Measurement Information System (PROMIS®) Global Health Scale and the World Health Organization Well-Being Index (WHO-5) at baseline day 0, day 15 and day 30. All outcomes were treated as exploratory.
Results
Both the Yoga Nidra and Music Therapy groups demonstrated significant improvements in PSQI, PROMIS and WHO-5 scores at day 15 and day 30 compared with the control group (p < .001 for all measures). Large effect sizes were observed across outcomes (partial η² = 0.195–0.795). Yoga Nidra showed greater improvements in overall well-being (WHO-5) and global health (PROMIS®), while Music Therapy demonstrated stronger effects on sleep quality (PSQI). No significant changes were observed in the control group. No adverse events were reported.
Conclusion
In this exploratory RCT, Yoga Nidra and Music Therapy were associated with significant improvements in sleep quality, mental health and overall well-being among post-COVID-19 hospitalised patients compared with standard care alone. These accessible, low-cost therapies may serve as valuable adjuncts to standard care for managing post-COVID psychological distress and sleep disturbances. Larger confirmatory trials are warranted.
Introduction
By the end of 2019, the appearance of the novel coronavirus disease (COVID-19) sparked widespread public fear. 1 A large number of individuals affected by COVID-19’s health and socio-economic impacts have developed mental health issues such as anxiety, depression and post-traumatic stress disorder. 2 Measures used during the pandemic to reduce the rate of transmission, like quarantine, are linked with a greater risk of developing mental health-related issues, especially in vulnerable groups like people with pre-existing mental health-related illnesses and frontline workers. 3 Various studies among normal subjects during the COVID-19 pandemic showed a higher level of anxiety-related disorders and preoccupation with the thought of COVID-19. 4 The first phase of the pandemic showed a 20% increase in patients with mental illness in India. 5 A link between the severity of depression and inflammatory markers like C-reactive protein levels indicates the role of inflammation and neuropsychiatric symptoms. 6 Sleep is essential for maintaining the immune system and contributes significantly to physical and mental health. Sleep disturbances, particularly insomnia, emerged as a significant public health concern during the COVID-19 pandemic, affecting approximately 40% of the adult population across various studies. 7 Various factors, including physical discomfort related to illness, lack of family members in the surroundings and other psychological factors like anxiety and depression, lead to sleep impairment. 6 The hypothalamic–pituitary–adrenal (HPA) axis becomes abnormally more active during stress, which makes it difficult to sleep. On the other hand, not being able to sleep makes the HPA axis even more active, which creates a vicious cycle of stress and insomnia. 8 Yoga Nidra (YN), also called ‘Yogic Sleep’, is an ancient relaxation technique, whose goal is to induce a state of relaxation with awareness of the surroundings.9, 10 The initial step in the preparation of the practice includes commitment towards the later action (Sankalpa), followed later by the spread of awareness to the other body parts, recall of various sensations and feelings and a restatement of Sankalpa, followed by the end of practice. 11 The principal action of YN therapy is to reduce sympathetic system activity. Its effect in mild to moderate hypertensive patients has resulted in simple, non-invasive and cost-effective practices to prevent stress. 12 Music Therapy (MT) is used in many community fields to help participants and others feel physically and mentally well. People who receive MT experience increased motivation, self-belief, pride, fullness and coping mechanisms. 13 Along with this, MT is documented to increase social engagement due to the recruitment of immersive and pleasurable elements. 14 Additionally, COVID-19 survivors have been shown to exhibit a high prevalence of anxiety and depression, with inflammatory and clinical factors playing a significant predictive role. 15 Since many post-COVID-19 patients demonstrated sleep and mental health-related issues as discussed above, and YN and MT are cost-effective, available and non-invasive methods, the question arises: ‘Does YN or music intervention significantly improve sleep quality and reduce mental stress levels compared to a control group among post-COVID patients?’ The objective of this study is to investigate the effect of YN and MT sessions on sleep quality, mental health and global well-being via comprehensive questionnaires. We hypothesised that YN and MT would improve sleep quality, mental health and overall well-being among post-COVID-19 patients.
Methods
Design
The study used a three-arm, parallel-group, randomised controlled trial (RCT) design. Participants eligible for the study were randomly allocated to one of three groups: control, YN or MT. Conducted at a tertiary care facility over six months from July to December 2022, the research was prospectively registered with the Clinical Trials Registry of India (CTRI/2021/07/034521). Ethical approval was secured from the Institutional Ethics Committee before the study’s commencement. Additionally, the paper adheres to the CONSORT guidelines for transparent reporting of RCTs.
Eligibility Criteria
The study population comprised adults aged 18 years and above with a documented history of laboratory-confirmed COVID-19. The reports need to be verified by reverse transcription polymerase chain reaction or rapid antigen testing. Patients who had been hospitalised for a minimum of five consecutive days due to COVID-19 and subsequently discharged within the six months before enrolment were considered eligible to ensure a clinically meaningful post-COVID population.
Participants with disturbed sleep and poor well-being, as measured by a Pittsburgh Sleep Quality Index (PSQI) score of five or higher and a World Health Organization Well-Being Index (WHO-5) score of 40 or lower, were considered eligible.16, 17 All participants were required to own a smartphone with reliable internet connectivity, as this was necessary for the online intervention giving. All eligible participants provided written informed consent before enrolment, in accordance with the Declaration of Helsinki. Participants were screened at baseline through self-reported medical history, based on which we excluded pre-existing sleep disorders (e.g., obstructive sleep apnoea and chronic insomnia) and major psychiatric illnesses. Where available, prior medical records were also reviewed. The study excluded people who already had sleep problems and were currently taking medications, were pregnant or had recently given birth, had serious complications from COVID, had cognitive difficulties or had taken part in other trials in the three months before this study. These exclusions were necessary to prevent confounding factors from affecting sleep and mental well-being assessments.
Sample Size and Randomisation
Since there was no prior data on the expected effects of YN and music interventions on mental stress in post-COVID patients, a formal sample size calculation was not performed. Instead, the sample size was determined based on feasibility and methodological considerations. Each of the three groups included 30 participants, a number commonly sufficient to approximate a normal distribution and enable parametric statistical analysis. Participants were recruited consecutively from the respective outpatient departments (OPDs). Participants were then randomly divided into three groups in a 1:1:1 ratio using a computer-generated randomisation sequence created by an independent third party not involved in the study. Allocation concealment was preserved using sequentially numbered, opaque, sealed envelopes lined with aluminium foil to prevent transparency. These envelopes were opened sequentially only after recording participant details, minimising potential selection bias.
Intervention
All eligible participants were allocated into three arms: YN, MT and a control group receiving routine standard care. All intervention sessions were conducted online via Zoom. The sessions were conducted under the supervision of trained and certified instructors from the Sri Sri Institute for Advanced Research (SSIAR), with a backup instructor available to ensure the intervention did not pause. YN: The instructor provided detailed instructions to participants before the sessions, including maintaining a comfortable supine position and following guided awareness of different body parts. To ensure standardisation and minimise intra-observer variability, a pre-recorded audio of guided YN, in the voice of Sri Sri Ravi Shankar (used with permission from SSIAR), was played during each session. This audio included verbal instructions for conscious relaxation and sequential rotation of awareness. Each session lasted 30 min and was conducted daily for 30 days. MT: The intervention consisted of a 30-min pre-recorded flute composition in Raag Lalit. The raag was rendered in a slow tempo to facilitate relaxation. Participants were instructed to listen passively and relax in the meantime. The same recording was used for all participants to maintain uniformity. Sessions were conducted daily for 30 days.
Sessions for both interventions were scheduled based on participants’ convenience within predefined morning and evening time windows. Adherence was monitored through online attendance tracking during sessions. The study team provided regular encouragement and follow-up to ensure compliance. The low burden and feasibility of the interventions contributed to complete retention, with no loss to follow-up. Participants were instructed to report any discomfort or adverse event experienced at any stage of the intervention period.
Outcome Assessment and Data Collection
Data collection was performed using a structured case report form. Standardised questionnaires assessing mental health, sleep quality and overall well-being were used to collect the data at baseline day 0, day 15 and day 30. Outcomes were evaluated pre- and post-intervention over the 30-day study period. In cases where a participant was admitted more than once during the study period, only data from the first admission was included in the analysis. All assessments were conducted by the principal investigator, who was blinded to group allocation to minimise assessment bias. Sleep quality was assessed using the PSQI; mental and global physical health were measured using the Patient-Reported Outcomes Measurement Information System (PROMIS®), Global Physical and Mental Health Scales and overall well-being was evaluated using the WHO-5 Well-Being Index.16–18
Data Analysis
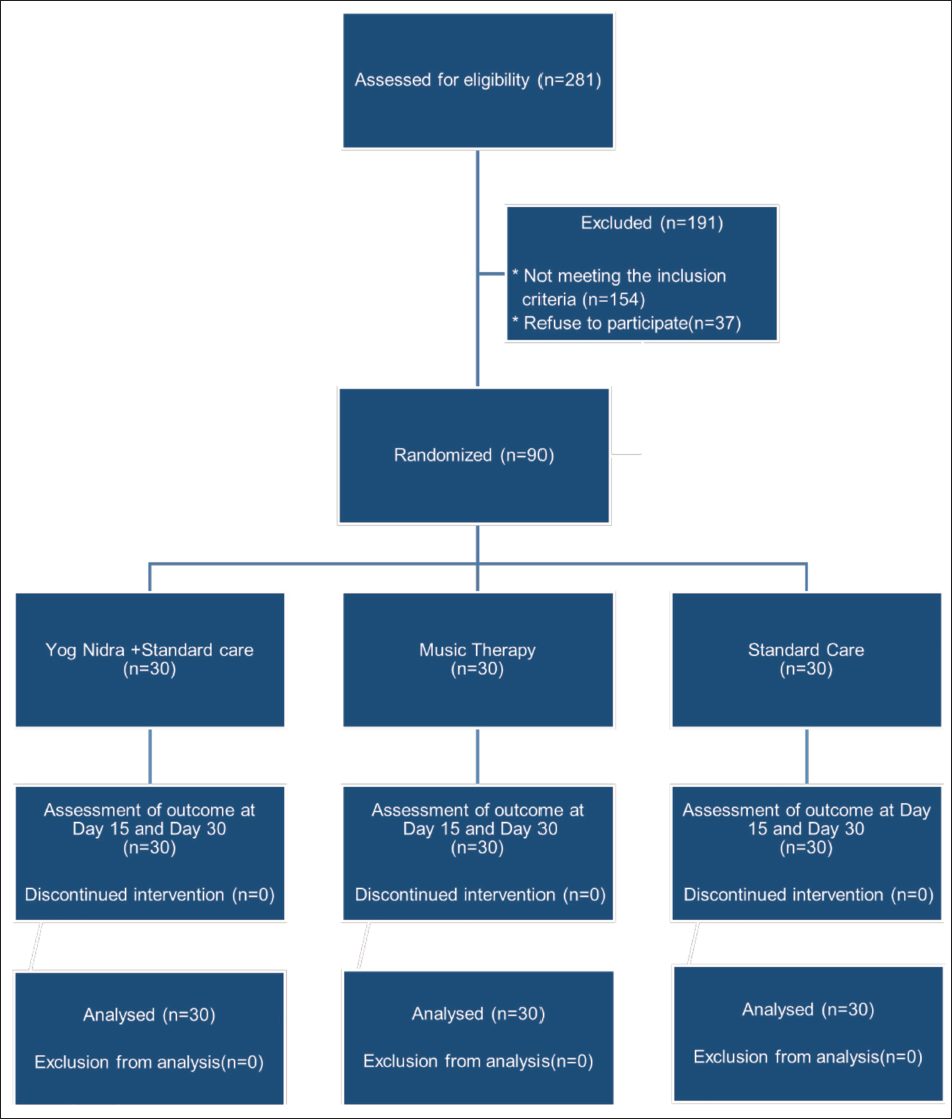
Outcome data collected at different time points were initially entered into Microsoft Excel 2016 and subsequently analysed using Microsoft Excel 2016 and SPSS version 20. A repeated-measures analysis of variance (ANOVA) was conducted to examine the effects of time, group and their interaction on the outcome variables. Mauchly’s test was used to assess sphericity; if the assumptions were violated, Greenhouse–Geisser corrections were applied. Post hoc pairwise comparisons were adjusted using Bonferroni correction. Effect sizes were reported as partial eta squared. An illustration of the participants’ flow through the study is shown in Figure 1.
CONSORT Flow Diagram of Participant Recruitment and Follow-up.
Results
Normality Assessment
The analysis started by checking the normality of the study variables using the Shapiro–Wilk test. Several variables, particularly the PSQI and WHO-5, showed deviations from normality (p < .05) across certain groups and time points. In contrast, PROMIS scores were largely normally distributed, with only minor violations. Given equal sample sizes across groups (n = 30 per group) and the established robustness of repeated-measures ANOVA to moderate violations of normality, parametric analyses were deemed suitable.
Baseline Comparisons
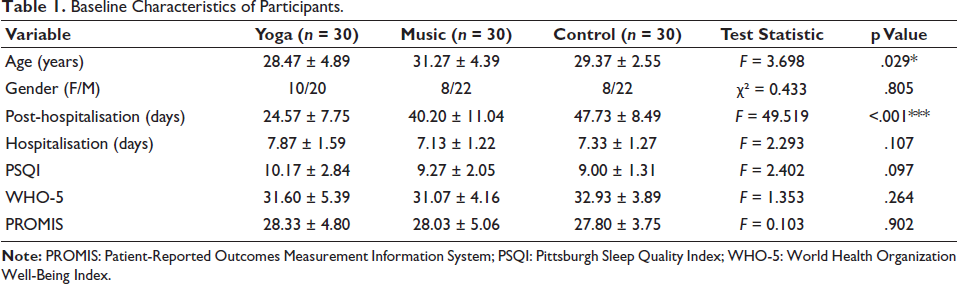
One-way ANOVA demonstrated that the three groups (Yoga, Music and Control) were comparable for most variables, including PSQI (p = .097), PROMIS (p = .902), WHO-5 (p = .264), and no of hospitalisation days (p = .107). Gender distribution was also comparable across groups (χ² = 0.433, p = .805). However, significant baseline differences were observed in age (p = .029) and post-hospitalisation scores (p < .001), indicating partial baseline imbalance despite randomisation (Table 1).
Baseline Characteristics of Participants.
Sleep Quality: Pittsburgh Sleep Quality Index
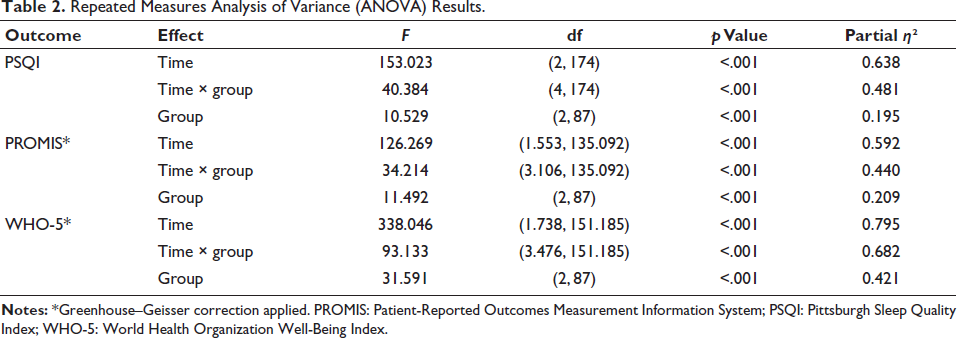
Mauchly’s test confirmed the sphericity assumption (W = 0.999, p = .959), so sphericity-assumed results are used. A significant main effect of time was found (F (2,174) = 153.02, p < .001, partial η² = 0.638), showing notable changes in sleep quality over time. The interaction between time and group was also significant (F (174) = 40.38, p < .001, partial η² = 0.481), suggesting different improvements across groups. Furthermore, a significant effect among groups was observed (F (2,87) = 10.53, p < .001, partial η² = 0.195) (Table 2).
Repeated Measures Analysis of Variance (ANOVA) Results.
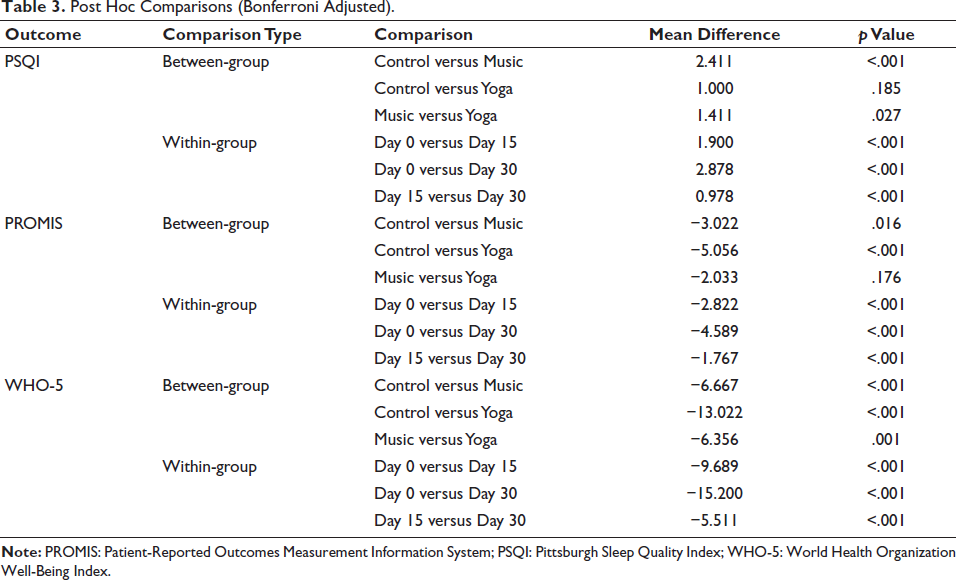
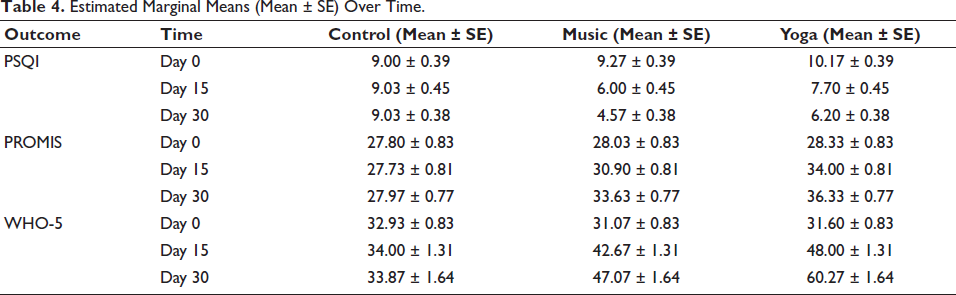
A post hoc analysis was conducted using Bonferroni-adjusted pairwise comparisons. In which the MT arm was found to significantly improve compared with the Control group (p < .001) and the Yoga group (p = .027). Whereas the difference between the Control and Yoga groups was not statistically significant (p = .185). Pairwise comparisons across time points indicated a significant improvement between all measurement intervals (p < .001) (Table 3). Descriptively, both Music and Yoga interventions improved sleep quality; however, the Music group demonstrated consistently greater reductions in PSQI scores over time than the Yoga group (Table 4).
Post Hoc Comparisons (Bonferroni Adjusted).
Estimated Marginal Means (Mean ± SE) Over Time.
Patient-Reported Outcomes Measurement Information System
While assessing sphericity with Mauchly’s test, a violation was found (W = 0.712, p < .001), so the Greenhouse–Geisser correction was used. There was a significant main effect of time (F (1.553, 135.092) = 126.269, p < .001, partial η² = 0.592), showing notable changes in PROMIS scores over time. A significant interaction between time and group was also detected (F (3.106, 135.092) = 34.214, p < .001, partial η² = 0.440), indicating different responses across groups. Additionally, the between-group effect was significant (F (2,87) = 11.49, p < .001, partial η² = 0.209) (Table 2).
Post hoc comparisons demonstrated that both the Music (p = .016) and Yoga (p < .001) groups differed significantly from the Control group, whereas no significant difference was observed between the Music and Yoga groups (p = .176). This indicates a comparable effectiveness of the two interventions (Table 3). The time-wise comparisons showed a significant change across all intervals (p < .001). Descriptive trends indicated that both intervention groups exhibited marked improvement, whereas the Control group showed minimal change over time (Table 4).
Well-being: World Health Organization Well-Being Index
The sphericity assumption, tested with Mauchly’s test, was violated (W = 0.849, p = .001), necessitating the use of the Greenhouse–Geisser correction in the results. A highly significant main effect of time was found (F (1.738, 151.185) = 338.05, p < .001, partial η² = 0.795), showing considerable improvement in well-being over time. The interaction between time and group was also significant (F (3.476, 151.185) = 93.13, p < .001, partial η² = 0.682), indicating varying degrees of improvement across groups. Additionally, a strong between-group effect was observed (F (2,87) = 31.59, p < .001, partial η² = 0.421) (Table 2).
The post hoc analysis revealed significant differences among all groups: Control versus Music (p < .001), Control versus Yoga (p < .001) and Music versus Yoga (p = .001) (Table 3). Time-wise comparisons indicated significant improvements across all time points (p < .00). Descriptively, the Yoga group showed the greatest improvement in well-being, followed by the Music group, with the Control group showing comparatively smaller changes (Table 4).
Overall Findings
The participants demonstrated high adherence rates, with means of 26.7 ± 2.29 and 26.03 ± 2.11 in the yoga and music groups, respectively. These corresponded to adherence rates of 89% and 86.8% in the yoga and music groups, respectively. No adverse events were reported. Across all outcome measures (PSQI, PROMIS and WHO-5), significant main effects of time and group, and a time × group interaction, were observed, indicating that both interventions produced meaningful improvements over time compared with the Control group (Table 2). The magnitude of these effects was large, particularly for WHO-5 (partial η² = 0.795), followed by PSQI (0.638) and PROMIS (0.592). Overall, Yoga demonstrated the most pronounced benefits in well-being, while Music showed stronger effects on sleep quality. For PROMIS outcomes, both interventions appeared equally effective.
Discussion
Systemic symptoms following COVID-19 infection can arise from both the immune response to the virus and environmental stressors, including social isolation and anxiety about severe or potentially fatal illness. A study of COVID-19 survivors found a high prevalence of psychiatric sequelae, with 55% of participants experiencing at least one disorder, most commonly PTSD, major depression and anxiety. 15 A meta-analysis combining data from 31 observational studies involving 5,153 COVID-19 patients reported prevalence rates of 47%, 45% and 34% for anxiety, depression and sleep disturbances, respectively. 19 YN, a form of guided meditation, is known to promote deep rest for the body and mind. Research examining the effects of YN and seated meditation on mental health demonstrated their efficacy in reducing anxiety and stress. 20 Jespersen et al. conducted a study that underscored the beneficial effects of MT on individuals with insomnia, concluding that it may improve sleep quality in this demographic. 21 However, very few studies have explored the effectiveness of non-pharmacological interventions specifically for COVID-19 patients. Notably, the YN (66.7%), MT (73.3%) and control groups (73.3%) had more males than females. This finding contrasts with a meta-analysis that reported a higher prevalence of post-COVID sleep-related issues in females (60%) than in males (40%). 22
This study found no significant difference in the mean duration of hospitalisation between the YN arm (7.87 days) and the MT arm (7.13 days) when compared to the control arm (7.33 days). van den Ende et al. reported in an observational study that patients hospitalised with COVID-19 were nearly five times more likely to have severely disturbed night sleep compared to the non-COVID-19 population. 23 Similarly, El Sayed et al. found a significant negative correlation between post-COVID-19 duration and sleep disorders, indicating that individuals in the early post-COVID-19 phase are at a greater risk for sleep disturbances due to the illness. Among a studied population of 500 individuals who had recovered from COVID-19, subthreshold insomnia was present in 59.2% of cases (n = 296), clinical insomnia (moderate severity) was found in 26.6% of cases (n = 133), and clinical insomnia (severe) was detected in 5.4% of cases (n = 27), highlighting the significant prevalence of post-COVID-19 sleep-related issues. 24
Becker noted that agents with anti-inflammatory properties, which are clinically used in psychiatry and sleep medicine, such as agomelatine, olanzapine, venlafaxine, mirtazapine and amitriptyline, can be effective in reducing the severity of COVID-19 and managing associated sleep disorders. 25 Our study aimed to identify a less costly and more accessible alternative to existing treatments. Participants in the control arm continued their regular treatment. The control group showed minimal changes in PSQI, PROMIS and WHO-5 scores over time, as evidenced by relatively stable estimated marginal means, indicating limited improvement in the absence of intervention. This may be attributed to a general lack of awareness regarding post-COVID psychological distress and the stigma surrounding the use of sedatives and hypnotics within the population. 26
YN influences and regulates the activity of the sympathetic nervous system, impacting essential parameters such as heart rate, systolic and diastolic blood pressure and brain electrical rhythms. It also modifies the levels of circulating stress hormones like adrenaline and cortisol, contributing to a reduction in sympathetic activity. 12 This effect has been well documented, as YN is part of various non-pharmacological interventions aimed at lowering blood pressure in individuals. These physiological effects make YN a suitable non-pharmacological intervention for stress-related conditions, including those arising in the post-COVID-19 recovery period.
Gulia and Sreedharan conducted a longitudinal study during the COVID-19 pandemic to examine the effects of yogic sleep on the sleep and well-being of postmenopausal subjects. The study revealed a marked improvement in the emotional state of the participants, indicating a positive impact on overall well-being. 27 In our study, we conducted daily YN sessions according to the previously mentioned protocol, utilising predefined questionnaires. We found a significant improvement over time in PSQI, PROMIS and WHO-5 scores (p value < .001). These findings suggest that the YN intervention demonstrated significant improvements in PROMIS and WHO-5 scores compared with the control group, particularly by day 30. YN was found to be effective in improving psychological well-being and global health outcomes, although the music arm showed comparatively greater improvement in sleep quality.
Vaishnav et al. implemented guided meditation, in the form of YN, among patients with end-stage renal disease undergoing maintenance haemodialysis for six weeks, resulting in statistically significant improvements (p value < .05) in quality of life and stress levels. 28 In the MT arm, music is widely recognised as a method for enhancing well-being and reducing stress, due to its direct physiological effects on the autonomic nervous system.29, 30 Our study found that post-COVID-19 patients had better sleep quality, mental health and overall well-being after treatment, as shown by improved scores on the PSQI, PROMIS and WHO-5 over time. Post hoc analysis revealed that the music group showed significantly greater improvements in sleep quality than both the yoga and control groups. This indicates that MT could play a role in enhancing sleep quality, mental and overall well-being. Liu et al. demonstrated the benefits of combining MT with mindfulness-based stress reduction on pain, sleep quality and anxiety in osteosarcoma patients over an eight-week duration, utilising the Wong-Baker FACES Pain Rating Scale, PSQI score and Hamilton Anxiety Rating Scale. Their results indicated that such interventions significantly alleviated symptoms. 31 Although this study provides strong evidence for the effectiveness of YN and MT in enhancing mental health after COVID-19, it is essential to acknowledge several limitations. A formal sample size calculation was not performed due to the absence of prior data on these specific treatments, which might limit the group’s ability to detect small differences. Additionally, no primary outcome was pre-specified, and therefore, the findings should be interpreted as exploratory rather than confirmatory. Despite randomisation, significant baseline differences in age and post-hospitalisation duration were observed across groups, which need to be considered when interpreting the results. Future research could benefit from pilot studies to inform more precise sample-size estimates. Additionally, even though providing services online made life easier for people during the pandemic, comparing the effectiveness of in-person and online interventions would provide valuable information, particularly regarding how people relate to therapy and the impact of disparities in technology access. Despite these issues, the internal validity of our findings is strengthened by the randomised, blinded design and the use of validated tools. This supports the incorporation of these non-pharmacological approaches into post-COVID care strategies.
Conclusion
Psychological distress following COVID-19 infection is a well-documented phenomenon, as highlighted in recent studies conducted during the pandemic. A simple, cost-effective non-pharmacological intervention could significantly benefit the general population experiencing such symptoms. This RCT addressed our research question, suggesting that YN and MT may enhance sleep quality, mental health and overall well-being among post-COVID-19 hospitalised patients compared with standard treatment alone.
Footnotes
Abbreviations
ANOVA: Analysis of variance; CONSORT: Consolidated standards of reporting trials; COVID-19: Coronavirus disease 2019; CRP: C-reactive protein; CTRI: Clinical Trials Registry of India; HAM-A: Hamilton Anxiety Rating Scale; HPA axis: Hypothalamic–pituitary–adrenal axis; MT: Music therapy; OPD: Outpatient department; PROMIS: Patient-Reported Outcomes Measurement Information System; PSQI: Pittsburgh Sleep Quality Index; RCT: Randomised controlled trial; RT-PCR: Reverse transcription polymerase chain reaction; SNOSE: Sequentially numbered, opaque, sealed envelopes; SPSS: Statistical Package for the Social Sciences; PTSD: Post-traumatic stress disorder; WBRS: Wong-Baker FACES Pain Rating Scale; WHO-5: World Health Organization Well-Being Index; YN: Yoga Nidra.
Acknowledgements
The authors sincerely acknowledge the support of the hospital and OPD staff for their invaluable assistance with patient recruitment, patient flow coordination and data collection during the study period. A heartfelt recognition goes to the instructor who intervened with the patients. The authors are also grateful to the clinical and research support staff who contributed to participant assessments and ensured smooth execution of the study procedures. The authors further extend our appreciation to all participants for their time, cooperation and willingness to participate in this research.
Author Contributions
The study was conceptualised by Dr Vikram Jain and Dr Monika Pathania. Dr Vikram Jain was primarily responsible for patient recruitment, interventions and data collection under the supervision of Dr Monika Pathania, who ensured proper execution of the study. Dr Prasan Panda and Dr Mahendra Singh assisted with OPD coordination and patient recruitment. Prateek Harsora was responsible for coordinating and providing intervention specialists to the patients throughout the study. Sumit Sharma analysed the data and contributed to the drafting and editing of the manuscript. All authors reviewed and approved the final manuscript.
Consent for Publication
This manuscript does not contain any individual person’s data, images, videos or other identifying information requiring consent for publication.
Consent to Participate
Written informed consent was obtained from all participants prior to enrolment in the study. Participants were provided with detailed information regarding the study objectives, procedures, potential benefits and risks, and informed of their right to withdraw at any time without affecting their standard of care.
CTRI Registration
The study was prospectively registered with the Clinical Trial Registry of India (CTRI Number: CTRI/2021/07/034521.
Data Availability
The data sets generated or analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient Consent
Prior to participation, written informed consent was voluntarily obtained from all individual subjects or their legally authorized representatives. Confidentiality and data privacy were maintained throughout the study.
Statement of Ethics
The study was conducted in accordance with institutional research procedures and the Declaration of Helsinki. The study received ethical approval from the Institutional Ethics Committee of All India Institute of Medical Sciences (Approval No. 165/IEC/PGM/2021 dated 15 May 2021).